HIV INFECTION AND THE ACQUIRED IMMUNODEFICIENCY SYNDROME (AIDS)
90
HIV INFECTION AND THE ACQUIRED IMMUNODEFICIENCY SYNDROME (AIDS)
-
Upload
aleesha-richards -
Category
Documents
-
view
217 -
download
1
Transcript of HIV INFECTION AND THE ACQUIRED IMMUNODEFICIENCY SYNDROME (AIDS)
HIV INFECTIONAND THE
ACQUIRED IMMUNODEFICIENCY SYNDROME (AIDS)
HIV INFECTIONAND THE
ACQUIRED IMMUNODEFICIENCY SYNDROME (AIDS)
HISTORICAL PERSPECTIVES OF AIDSHISTORICAL PERSPECTIVES OF AIDS
1981
1982
1983
1984
1986
1981
1982
1983
1984
1986
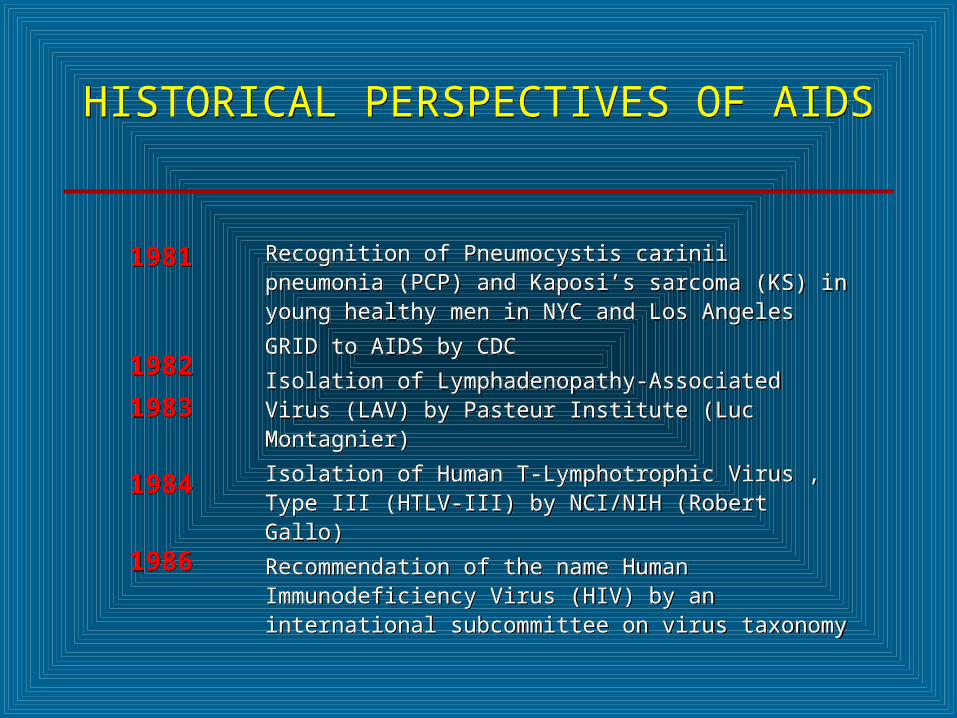
Recognition of Pneumocystis carinii pneumonia (PCP) and Kaposi’s sarcoma (KS) in young healthy men in NYC and Los Angeles
GRID to AIDS by CDC
Isolation of Lymphadenopathy-Associated Virus (LAV) by Pasteur Institute (Luc Montagnier)
Isolation of Human T-Lymphotrophic Virus , Type III (HTLV-III) by NCI/NIH (Robert Gallo)
Recommendation of the name Human Immunodeficiency Virus (HIV) by an international subcommittee on virus taxonomy
Recognition of Pneumocystis carinii pneumonia (PCP) and Kaposi’s sarcoma (KS) in young healthy men in NYC and Los Angeles
GRID to AIDS by CDC
Isolation of Lymphadenopathy-Associated Virus (LAV) by Pasteur Institute (Luc Montagnier)
Isolation of Human T-Lymphotrophic Virus , Type III (HTLV-III) by NCI/NIH (Robert Gallo)
Recommendation of the name Human Immunodeficiency Virus (HIV) by an international subcommittee on virus taxonomy


HUMAN IMMUNODEFICIENCY VIRUSES (HIV)
HUMAN IMMUNODEFICIENCY VIRUSES (HIV)
* Classification* Retroviridae (family) * Lentivirus (genus)
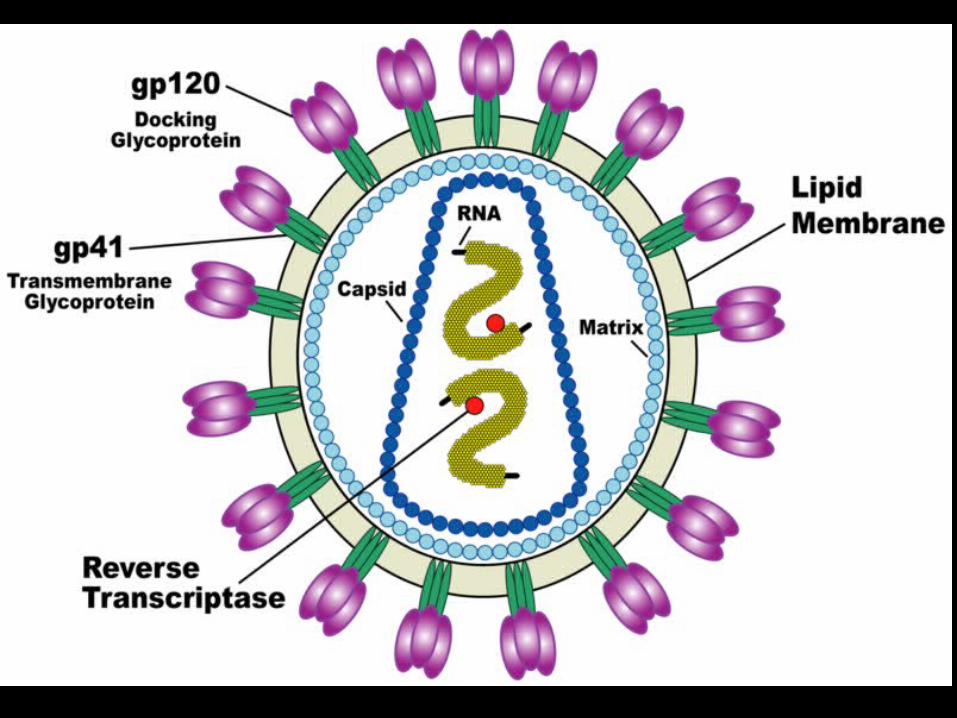
* Characteristics* 100 nm in diameter* Genome of 2 single strands of RNA
* Nine genes
* Reverse transcriptase* RNA-dependent DNA polymerase* Transcribes RNA into DNA
* Classification* Retroviridae (family) * Lentivirus (genus)
* Characteristics* 100 nm in diameter* Genome of 2 single strands of RNA
* Nine genes
* Reverse transcriptase* RNA-dependent DNA polymerase* Transcribes RNA into DNA

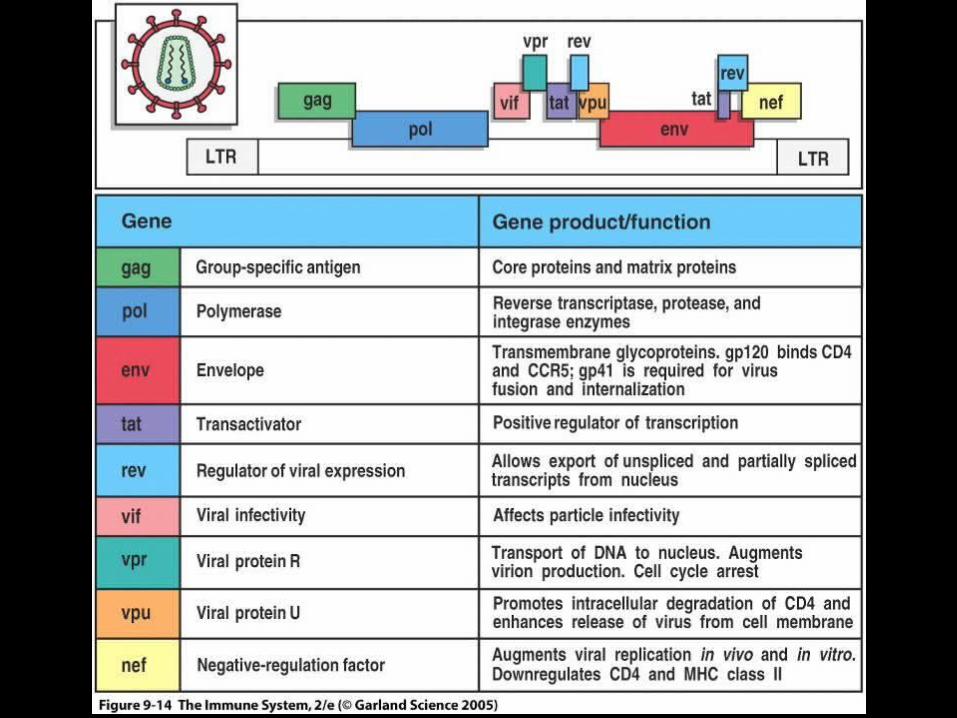
GENOME OF HIVGENOME OF HIV
* Contains 6 regulatory genes* Contains 3 structural genes
* Env (Envelope glycoproteins)* gp120 and gp41
* Gag (Core and matrix proteins)* p55, p40 and p24
* Pol (Enzymes)* Reverse transcriptase (p66, p51)* Protease (p11)* Integrase (p32)
* Contains 6 regulatory genes* Contains 3 structural genes
* Env (Envelope glycoproteins)* gp120 and gp41
* Gag (Core and matrix proteins)* p55, p40 and p24
* Pol (Enzymes)* Reverse transcriptase (p66, p51)* Protease (p11)* Integrase (p32)
HUMAN RETROVIRIDAE (EXOGENOUS RETROVIRUSES)
HUMAN RETROVIRIDAE (EXOGENOUS RETROVIRUSES)
* Seven genera* Alpha, Beta, Gamma, Delta, Epsilon, Lenti and Spuma
* Deltavirus* Human T-lymphotropic virus, type I (HTLV-1)
* Human T-lymphotropic virus, type II (HTLV-II)
* Lentivirus* Human immunodeficiency virus, type 1 (HIV-1)
* Human immunodeficiency virus, type 2 (HIV-2)
* Seven genera* Alpha, Beta, Gamma, Delta, Epsilon, Lenti and Spuma
* Deltavirus* Human T-lymphotropic virus, type I (HTLV-1)
* Human T-lymphotropic virus, type II (HTLV-II)
* Lentivirus* Human immunodeficiency virus, type 1 (HIV-1)
* Human immunodeficiency virus, type 2 (HIV-2)
CLASSIFICATION OF THE HUMAN IMMUNODEFICIENCY VIRUSES (HIV)
CLASSIFICATION OF THE HUMAN IMMUNODEFICIENCY VIRUSES (HIV)
* Types* Human immunodeficiency virus, type 1 (HIV-1)
* Human immunodeficiency virus, type 2 (HIV-2)
* HIV-1 is divided into groups* M (Major)
* N (New)
* O (Outlier)
* Group M is divided into * Subtypes (Clades)
* Circulating recombinant forms (CRF)
* Types* Human immunodeficiency virus, type 1 (HIV-1)
* Human immunodeficiency virus, type 2 (HIV-2)
* HIV-1 is divided into groups* M (Major)
* N (New)
* O (Outlier)
* Group M is divided into * Subtypes (Clades)
* Circulating recombinant forms (CRF)

CLASSIFICATION OF HIVCLASSIFICATION OF HIV
*HIV-1
*Group M
*Group N
*Group O
*A *B *C *D *F *G *H *J *K *CRFs
*HIV-2
ORIGIN OF HUMAN IMMUNODEFICIENCY VIRUSES
ORIGIN OF HUMAN IMMUNODEFICIENCY VIRUSES
* Existed as monkey virus in equatorial Africa* HIV-1
* Chimpanzee (Pan troglodytes troglodytes)
* HIV-2* Sooty Mangabey (Cercocebus atys)
* Transition from monkeys to humans * When - Circa 1908
* Molecular phylogenetics
* How – Hunter theory
* Existed as monkey virus in equatorial Africa* HIV-1
* Chimpanzee (Pan troglodytes troglodytes)
* HIV-2* Sooty Mangabey (Cercocebus atys)
* Transition from monkeys to humans * When - Circa 1908
* Molecular phylogenetics
* How – Hunter theory

MECHANISM OF PATHOGENICITY OF HIV
MECHANISM OF PATHOGENICITY OF HIV
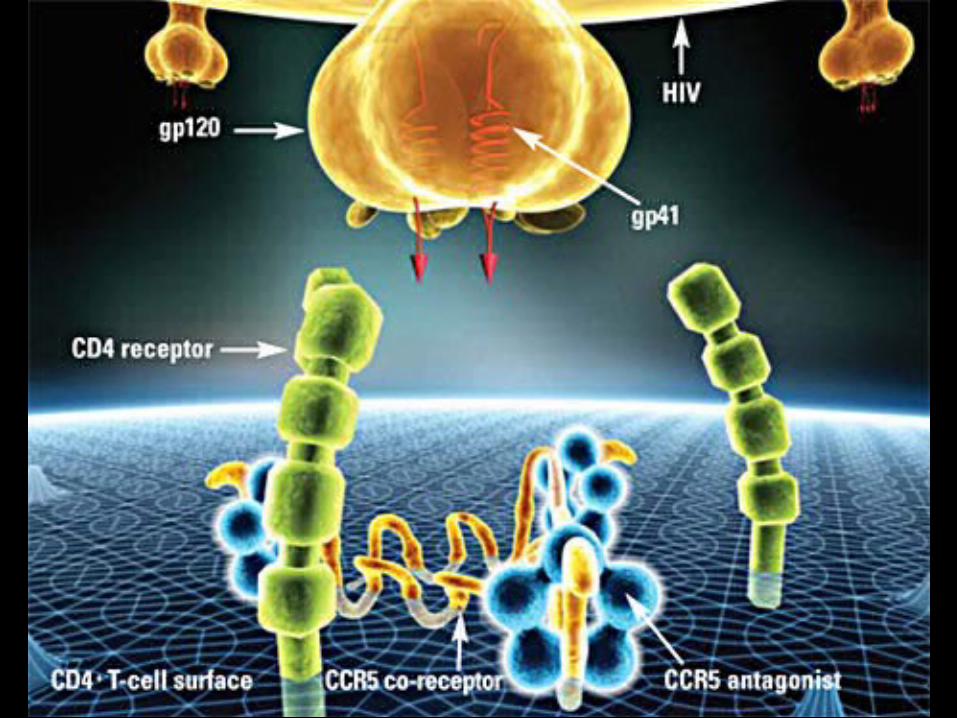
* Envelope protein (gp120) of HIV binds with CD-4 receptor on surface of* T-lymphocytes
* Macrophages
* Dendritic cells
* Microglial cells
* Coreceptors for attachment of HIV* CCR5 (T-cells, macrophages, dendritic cells, microglial
cells)
* CXCR4 (T-cells)
* Envelope protein (gp120) of HIV binds with CD-4 receptor on surface of* T-lymphocytes
* Macrophages
* Dendritic cells
* Microglial cells
* Coreceptors for attachment of HIV* CCR5 (T-cells, macrophages, dendritic cells, microglial
cells)
* CXCR4 (T-cells)
MECHANISM OF PATHOGENICITY OF HIV
MECHANISM OF PATHOGENICITY OF HIV
* Early infectionEarly infection* CCR5 coreceptor is used (R5 strains)CCR5 coreceptor is used (R5 strains)* Growth equal in monocytes and lymphocytesGrowth equal in monocytes and lymphocytes* Non syncytium-inducing (NSI)Non syncytium-inducing (NSI)
* Late infectionLate infection* CXCR4 coreceptor is used (X4 strains)CXCR4 coreceptor is used (X4 strains)* Growth in T cellsGrowth in T cells* Syncytium-inducing (SI)Syncytium-inducing (SI)
* Emergence of X4 strains associated with accelerated decline in CD4 T Emergence of X4 strains associated with accelerated decline in CD4 T cellscells* Cause or consequence?Cause or consequence?
* Early infectionEarly infection* CCR5 coreceptor is used (R5 strains)CCR5 coreceptor is used (R5 strains)* Growth equal in monocytes and lymphocytesGrowth equal in monocytes and lymphocytes* Non syncytium-inducing (NSI)Non syncytium-inducing (NSI)
* Late infectionLate infection* CXCR4 coreceptor is used (X4 strains)CXCR4 coreceptor is used (X4 strains)* Growth in T cellsGrowth in T cells* Syncytium-inducing (SI)Syncytium-inducing (SI)
* Emergence of X4 strains associated with accelerated decline in CD4 T Emergence of X4 strains associated with accelerated decline in CD4 T cellscells* Cause or consequence?Cause or consequence?

MECHANISM OF PATHOGENICITY OF HIV
MECHANISM OF PATHOGENICITY OF HIV
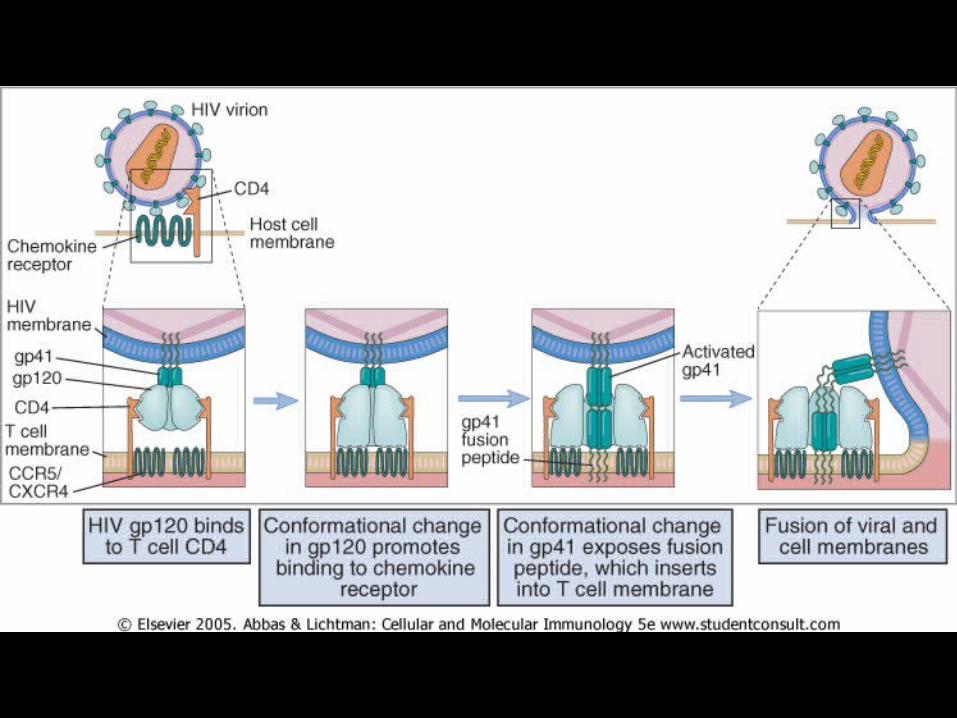
* Following attachment, virus enters cells and removes protein coat
* Viral RNA is transcribed into DNA by * Reverse transcriptase
* Viral DNA then integrated into host cell DNA* Integrase
* Integrated viral DNA * Referred to as “provirus”* Production of active infection
* Following attachment, virus enters cells and removes protein coat
* Viral RNA is transcribed into DNA by * Reverse transcriptase
* Viral DNA then integrated into host cell DNA* Integrase
* Integrated viral DNA * Referred to as “provirus”* Production of active infection

EPIDEMIOLOGY OF HIV INFECTION AND AIDS
EPIDEMIOLOGY OF HIV INFECTION AND AIDS
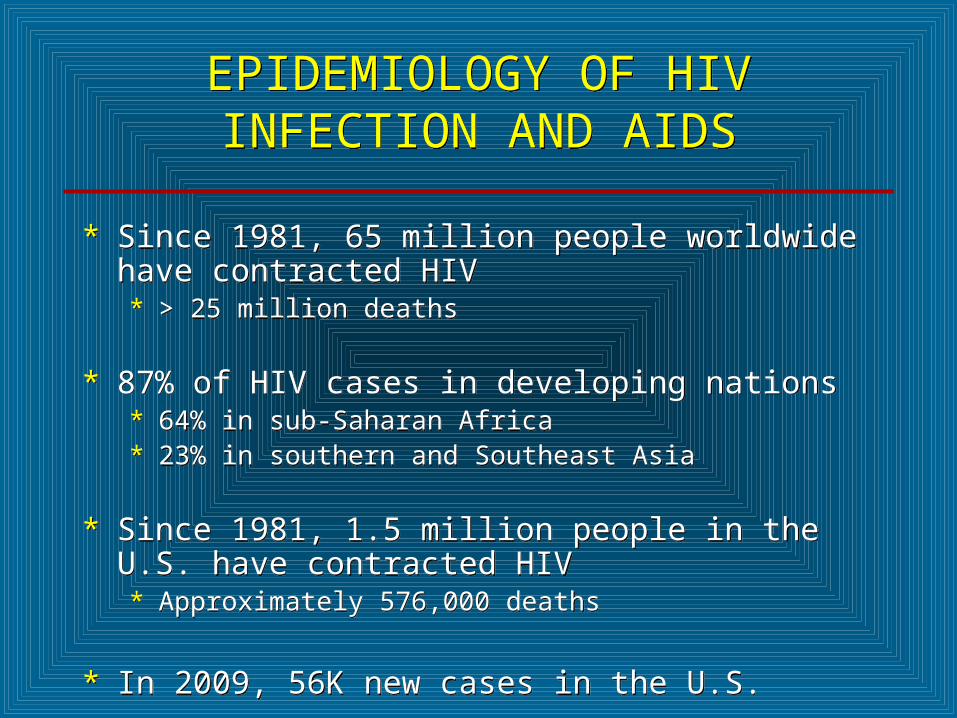
* Since 1981, 65 million people worldwide have contracted HIV* > 25 million deaths
* 87% of HIV cases in developing nations* 64% in sub-Saharan Africa* 23% in southern and Southeast Asia
* Since 1981, 1.5 million people in the U.S. have contracted HIV* Approximately 576,000 deaths
* In 2009, 56K new cases in the U.S.
* Since 1981, 65 million people worldwide have contracted HIV* > 25 million deaths
* 87% of HIV cases in developing nations* 64% in sub-Saharan Africa* 23% in southern and Southeast Asia
* Since 1981, 1.5 million people in the U.S. have contracted HIV* Approximately 576,000 deaths
* In 2009, 56K new cases in the U.S.


TRANSMISSION OF HIV INFECTION AND AIDS
TRANSMISSION OF HIV INFECTION AND AIDS
* Sexual intercourse with infected person* Homosexual (MSM)
* Heterosexual
* Bisexual
* Children born to infected mothers* Perinatal
* IV drug addicts sharing contaminated syringes/needles
* Transfusion of blood and blood products* Transfusion recipients
* Hemophiliacs
* Occupational exposure in health-care setting
* Sexual intercourse with infected person* Homosexual (MSM)
* Heterosexual
* Bisexual
* Children born to infected mothers* Perinatal
* IV drug addicts sharing contaminated syringes/needles
* Transfusion of blood and blood products* Transfusion recipients
* Hemophiliacs
* Occupational exposure in health-care setting
CDC CLASSIFICATION OF HIV INFECTION AND DISEASE IN ADULTS
AND ADOLESCENTS
CDC CLASSIFICATION OF HIV INFECTION AND DISEASE IN ADULTS
AND ADOLESCENTS
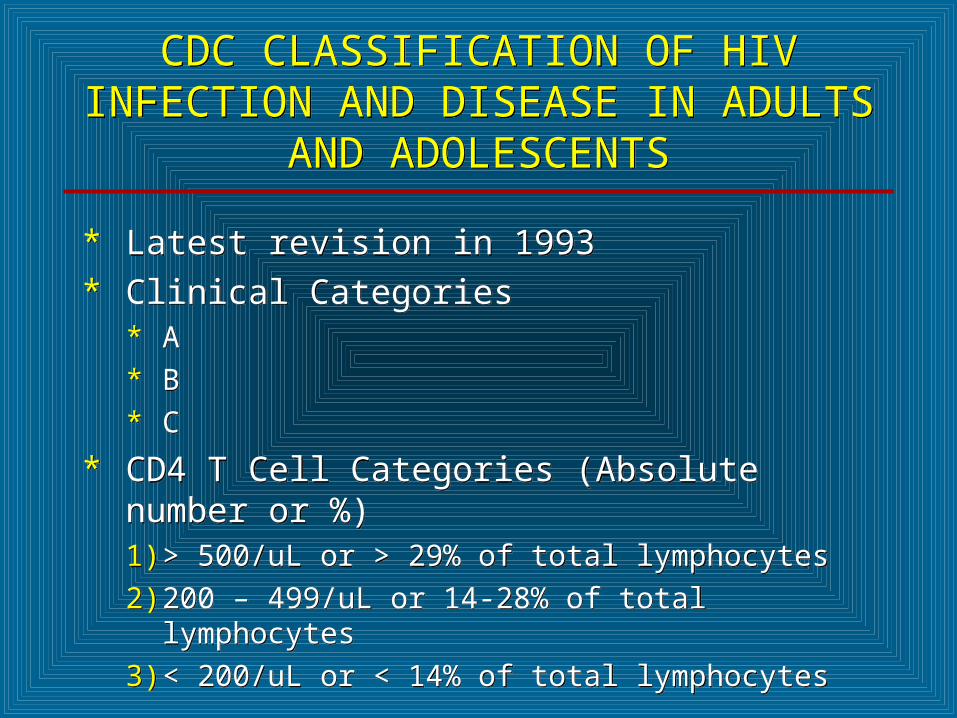
* Latest revision in 1993* Clinical Categories
* A
* B
* C
* CD4 T Cell Categories (Absolute number or %)1) > 500/uL or > 29% of total lymphocytes
2) 200 – 499/uL or 14-28% of total lymphocytes
3) < 200/uL or < 14% of total lymphocytes
* Latest revision in 1993* Clinical Categories
* A
* B
* C
* CD4 T Cell Categories (Absolute number or %)1) > 500/uL or > 29% of total lymphocytes
2) 200 – 499/uL or 14-28% of total lymphocytes
3) < 200/uL or < 14% of total lymphocytes
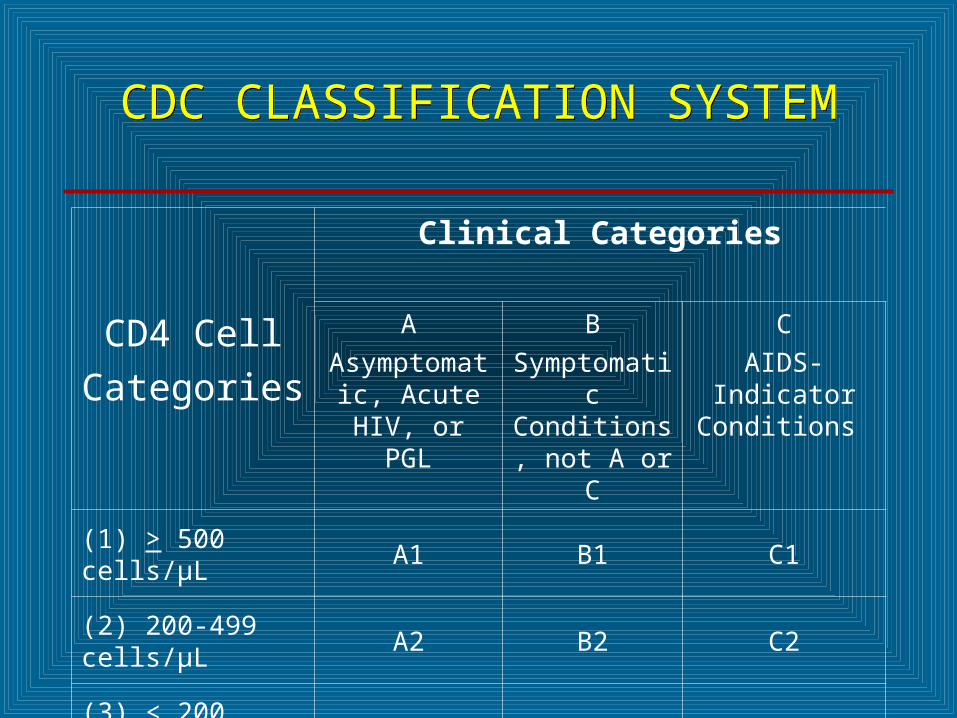
CDC CLASSIFICATION SYSTEMCDC CLASSIFICATION SYSTEM
CD4 Cell
Categories
Clinical Categories
A
Asymptomatic, Acute HIV, or
PGL
B
Symptomatic Conditions, not A or C
C
AIDS-Indicator Conditions
(1) > 500 cells/µL A1 B1 C1
(2) 200-499 cells/µL A2 B2 C2
(3) < 200 cells/µL A3 B3 C3


CDC CLASSIFICATION SYSTEM(CLINICAL CATEGORY A)
CDC CLASSIFICATION SYSTEM(CLINICAL CATEGORY A)
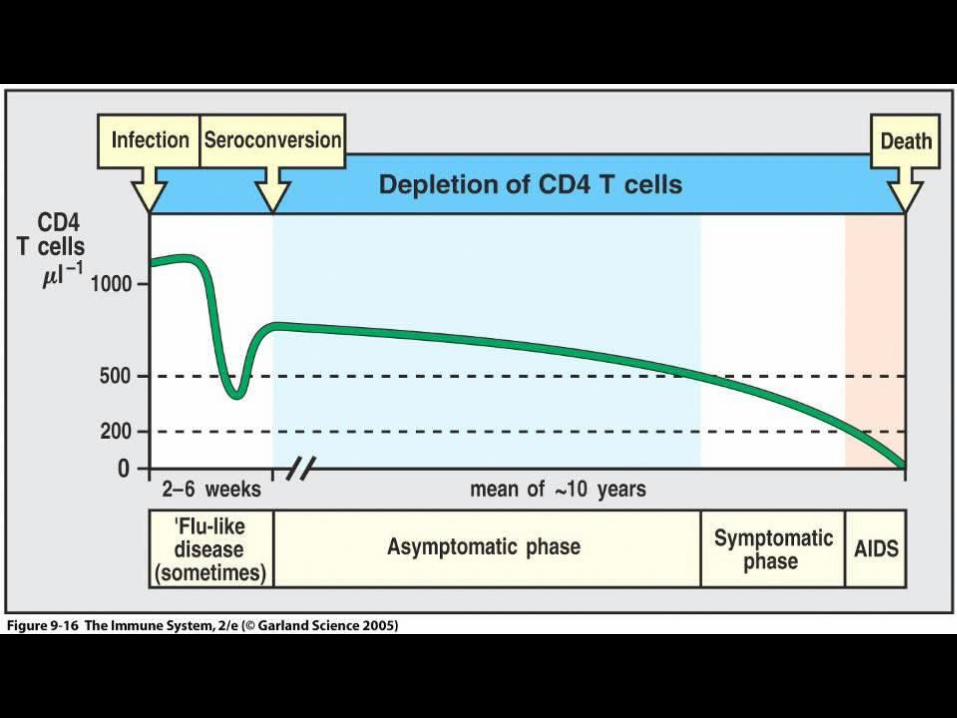
* Following initial infection * Asymptomatic * Acute Retroviral Syndrome
* Infectious mononucleosis-like or flu-like illness * 2 days to 4 weeks following infection* Clinical manifestations
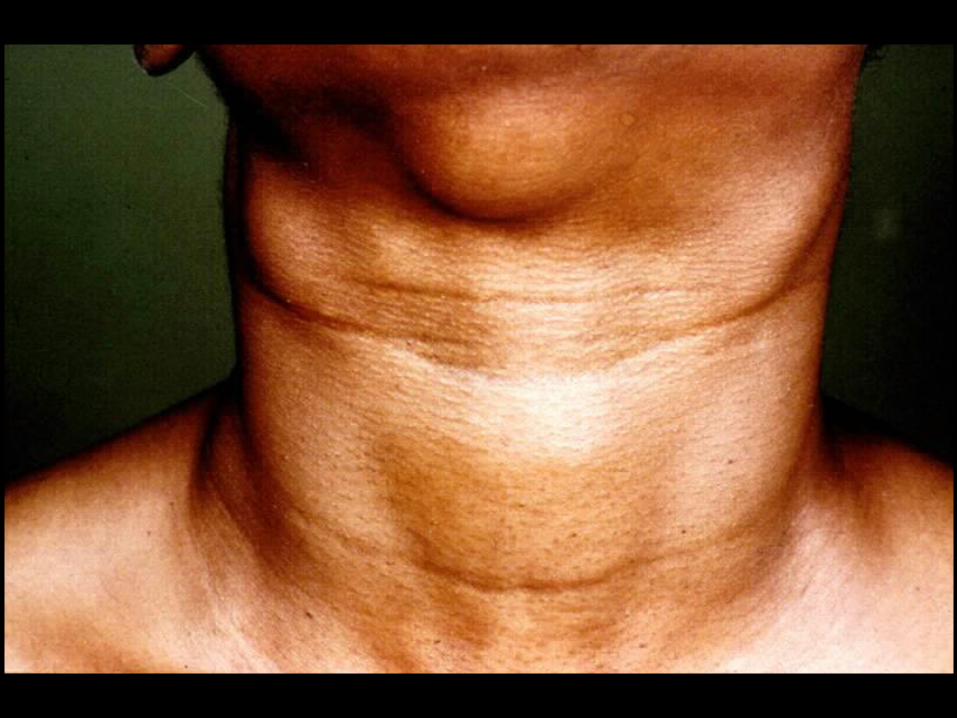
* Fever, headache, lethargy, pharyngitis, myalgias, photophobia, lymphadenopathy and a faint maculopapular rash
* Resolution within 30 days
* Persistent generalized lymphadenopathy (PGL)
* Following initial infection * Asymptomatic * Acute Retroviral Syndrome
* Infectious mononucleosis-like or flu-like illness * 2 days to 4 weeks following infection* Clinical manifestations
* Fever, headache, lethargy, pharyngitis, myalgias, photophobia, lymphadenopathy and a faint maculopapular rash
* Resolution within 30 days
* Persistent generalized lymphadenopathy (PGL)

CDC CLASSIFICATION SYSTEM (CLINICAL CATEGORY B)
CDC CLASSIFICATION SYSTEM (CLINICAL CATEGORY B)
* Symptomatic conditions not meeting conditions of clinical categories A or C* Herpes zoster (shingles)
* Oropharyngeal Candidiasis (thrush)* Candida albicans
* Vulvovaginal candidiasis
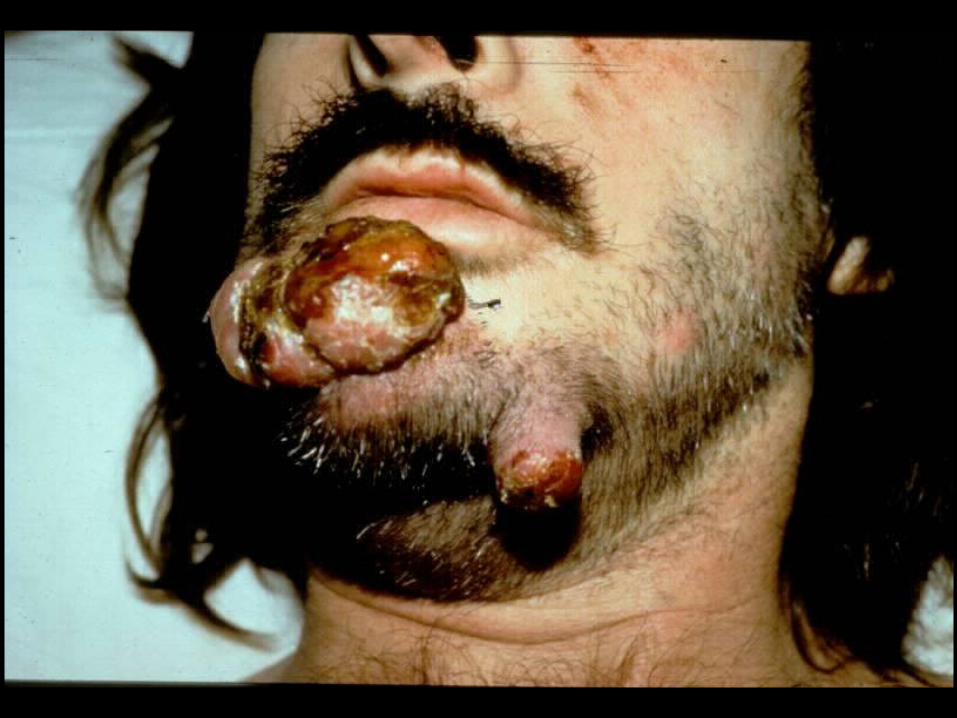
* Bacillary angiomatosis* Bartonella henselae
* Peripheral neuropathy
* Idiopathic thrombocytopenic purpura (ITP)
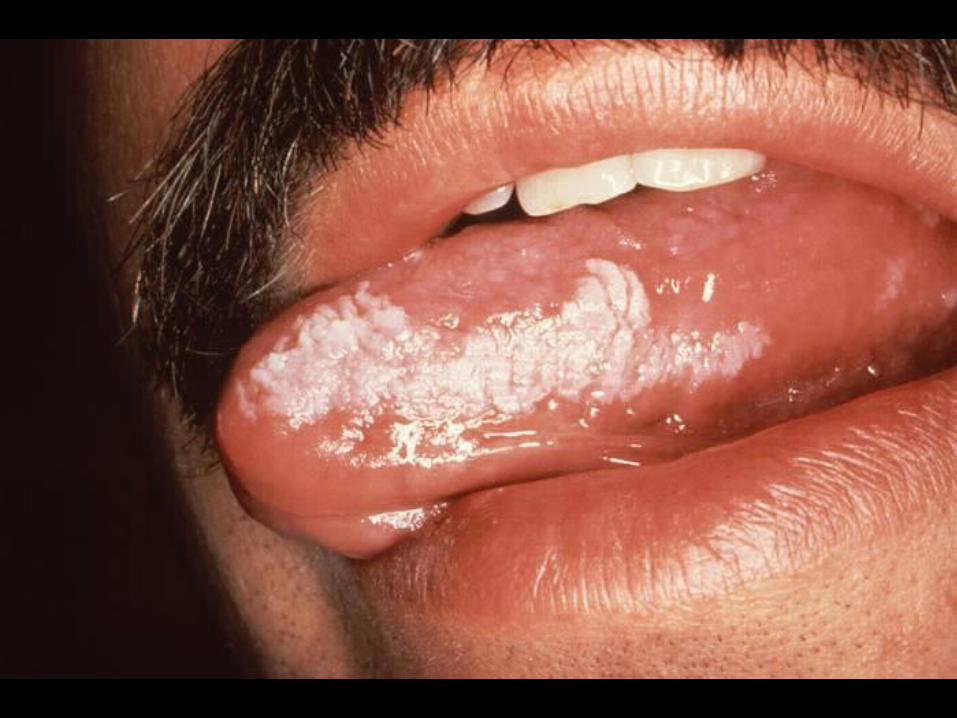
* Hairy leukoplakia (oral)
* Symptomatic conditions not meeting conditions of clinical categories A or C* Herpes zoster (shingles)
* Oropharyngeal Candidiasis (thrush)* Candida albicans
* Vulvovaginal candidiasis
* Bacillary angiomatosis* Bartonella henselae
* Peripheral neuropathy
* Idiopathic thrombocytopenic purpura (ITP)
* Hairy leukoplakia (oral)


CDC CLASSIFICATION SYSTEM (CLINICAL CATEGORY C)
CDC CLASSIFICATION SYSTEM (CLINICAL CATEGORY C)
* Acquired Immunodeficiency Syndrome (AIDS) Defining Conditions* Esophageal Candidiasis
* Cryptosporidiosis
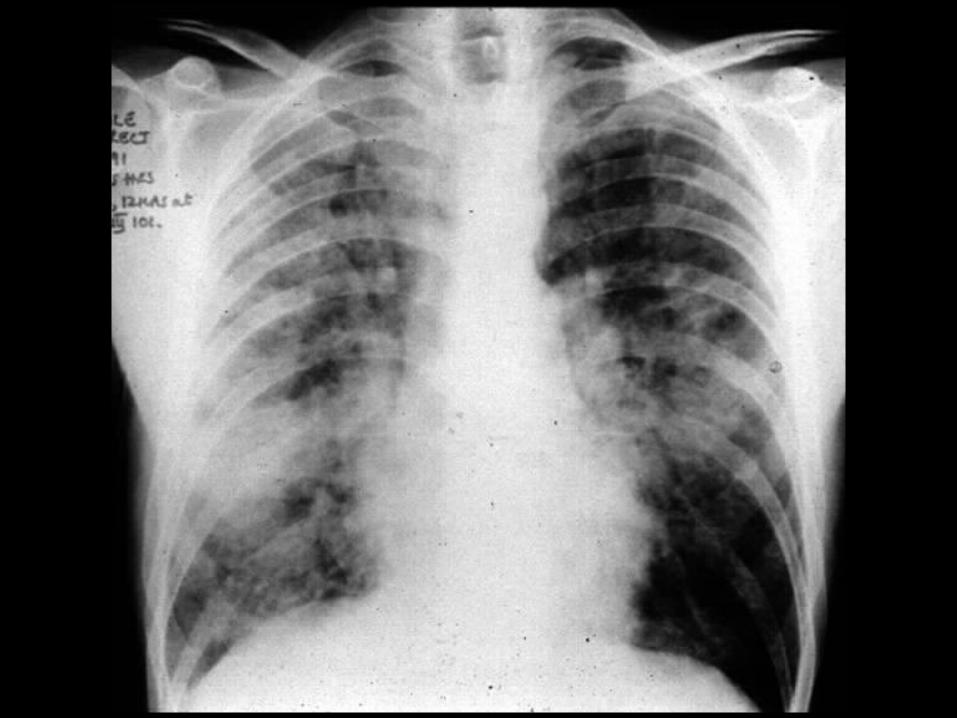
* Pneumocystis jiroveci (carinii) pneumonia
* Tuberculosis (pulmonary or extrapulmonary)
* Disseminated Mycobacterium avium complex (MAC) disease
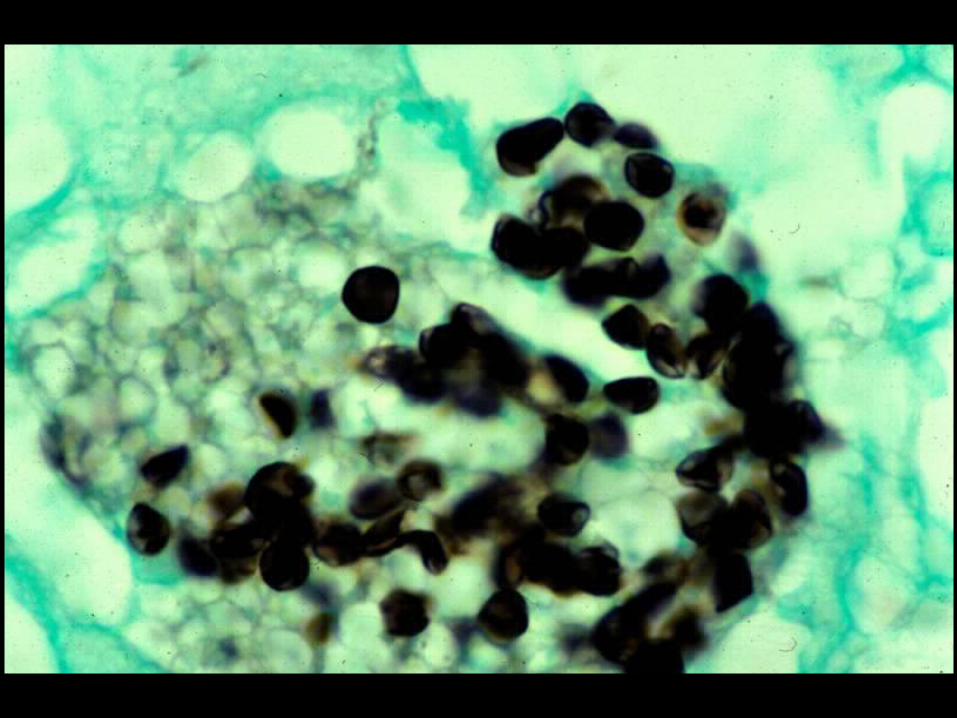
* Histoplasmosis (disseminated or extrapulmonary)
* Acquired Immunodeficiency Syndrome (AIDS) Defining Conditions* Esophageal Candidiasis
* Cryptosporidiosis
* Pneumocystis jiroveci (carinii) pneumonia
* Tuberculosis (pulmonary or extrapulmonary)
* Disseminated Mycobacterium avium complex (MAC) disease
* Histoplasmosis (disseminated or extrapulmonary)
HIV INFECTION IN ADULTS (CLINICAL CATEGORY C)
HIV INFECTION IN ADULTS (CLINICAL CATEGORY C)
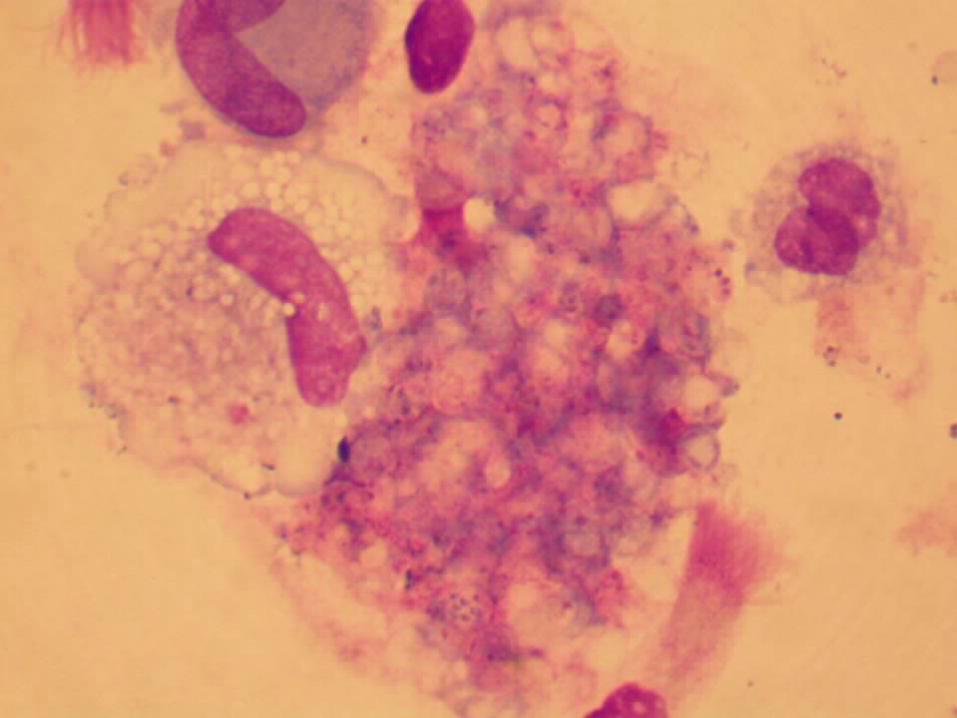
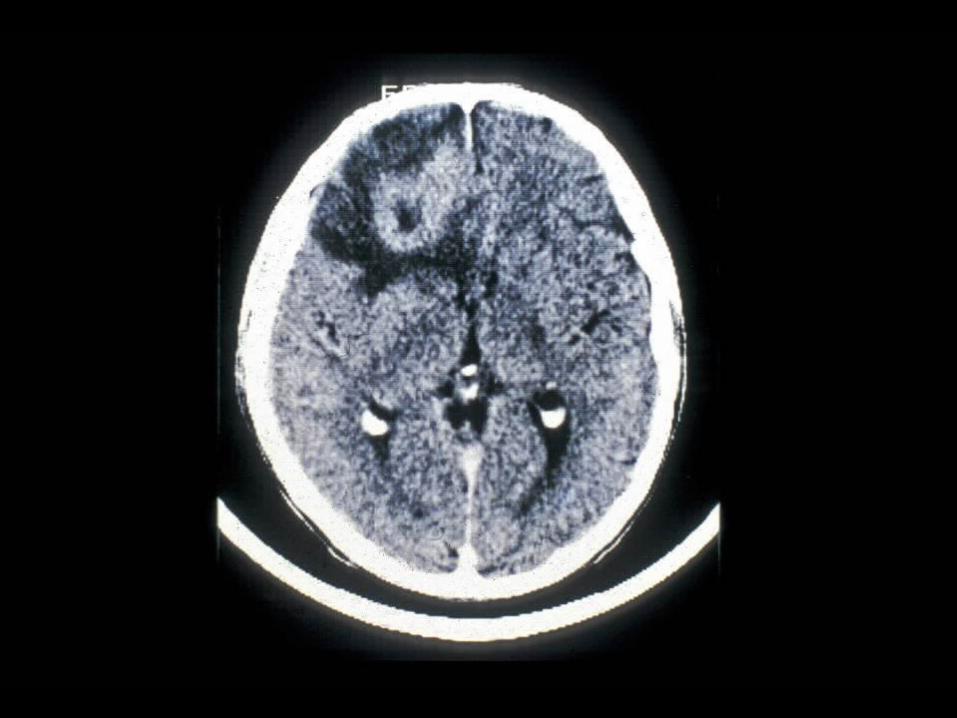
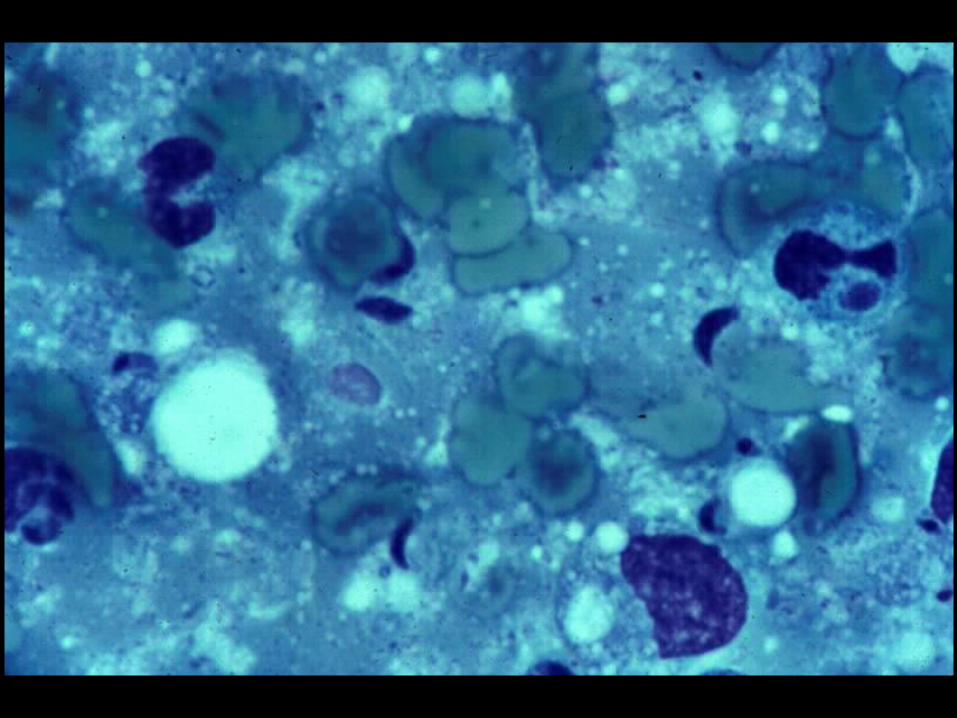
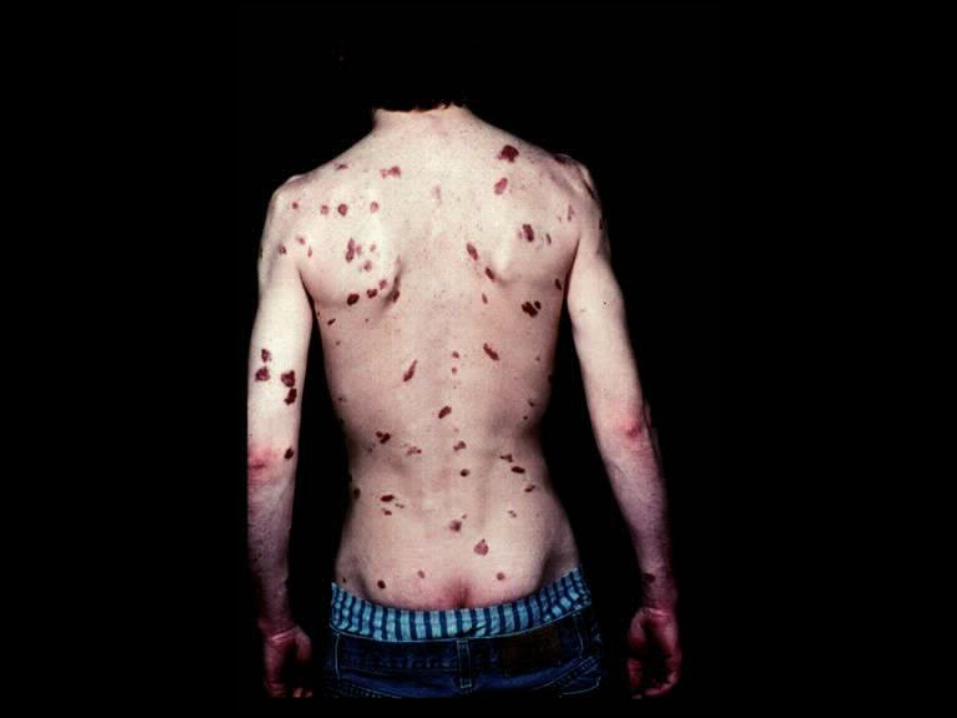
* Acquired Immunodeficiency Syndrome (AIDS) Defining Conditions* HIV wasting syndrome* Cryptococcal meningitis* Cytomegalovirus retinitis* Cerebral Toxoplasmosis* Progressive multifocal leukoencephalopathy (PML)
* JC virus
* Kaposi’s sarcoma* Human herpesvirus type 8 (HHV-8)
* Acquired Immunodeficiency Syndrome (AIDS) Defining Conditions* HIV wasting syndrome* Cryptococcal meningitis* Cytomegalovirus retinitis* Cerebral Toxoplasmosis* Progressive multifocal leukoencephalopathy (PML)
* JC virus
* Kaposi’s sarcoma* Human herpesvirus type 8 (HHV-8)





PROGNOSIS AND MONITORING OF HIV TREATMENT AND DISEASE
PROGNOSIS AND MONITORING OF HIV TREATMENT AND DISEASE
* CD4 T cell count (Immunological response)CD4 T cell count (Immunological response)* Absolute numberAbsolute number
* Best indicator for patients with counts < 200 cells/uLBest indicator for patients with counts < 200 cells/uL
* PercentPercent* Best indicator for patients with counts > 200 cells/uLBest indicator for patients with counts > 200 cells/uL
* HIV-1 RNA (Viral load) (Virological response)HIV-1 RNA (Viral load) (Virological response)
* Discordant immunological and virological responses existDiscordant immunological and virological responses exist
* CD4 T cell count (Immunological response)CD4 T cell count (Immunological response)* Absolute numberAbsolute number
* Best indicator for patients with counts < 200 cells/uLBest indicator for patients with counts < 200 cells/uL
* PercentPercent* Best indicator for patients with counts > 200 cells/uLBest indicator for patients with counts > 200 cells/uL
* HIV-1 RNA (Viral load) (Virological response)HIV-1 RNA (Viral load) (Virological response)
* Discordant immunological and virological responses existDiscordant immunological and virological responses exist
TREATMENT OF HIV INFECTION AND DISEASE
TREATMENT OF HIV INFECTION AND DISEASE
* Anti-retroviral drugs do not cure HIV infection or diseaseAnti-retroviral drugs do not cure HIV infection or disease* Suppression of virus to undetectable levelsSuppression of virus to undetectable levels
* Suppression of virusSuppression of virus* Drugs must be taken continuouslyDrugs must be taken continuously* Patients remain infectiousPatients remain infectious
* Mutation rate in HIV is high and resistance developsMutation rate in HIV is high and resistance develops
* Recommendation for combination therapyRecommendation for combination therapy* Combination of drugs from two or more classesCombination of drugs from two or more classes* Highly Active Anti-Retroviral Therapy (HAART)Highly Active Anti-Retroviral Therapy (HAART)
* Anti-retroviral drugs do not cure HIV infection or diseaseAnti-retroviral drugs do not cure HIV infection or disease* Suppression of virus to undetectable levelsSuppression of virus to undetectable levels
* Suppression of virusSuppression of virus* Drugs must be taken continuouslyDrugs must be taken continuously* Patients remain infectiousPatients remain infectious
* Mutation rate in HIV is high and resistance developsMutation rate in HIV is high and resistance develops
* Recommendation for combination therapyRecommendation for combination therapy* Combination of drugs from two or more classesCombination of drugs from two or more classes* Highly Active Anti-Retroviral Therapy (HAART)Highly Active Anti-Retroviral Therapy (HAART)

TREATMENT OF HIV INECTION AND DISEASE
TREATMENT OF HIV INECTION AND DISEASE
* Classes of anti-retroviral drugsClasses of anti-retroviral drugs* Reverse Transcriptase Inhibitors (RTI’s)Reverse Transcriptase Inhibitors (RTI’s)
* NucleosideNucleoside* NucleotideNucleotide* Non-nucleosideNon-nucleoside
* Protease Inhibitors (PIs)Protease Inhibitors (PIs)* Fusion or Entry Inhibitors Fusion or Entry Inhibitors
* Act on gp41 or CCR5 coreceptorAct on gp41 or CCR5 coreceptor
* Integrase InhibitorsIntegrase Inhibitors* Fixed dose combinationsFixed dose combinations
* Drugs from two or more classes into a single productDrugs from two or more classes into a single product
* Classes of anti-retroviral drugsClasses of anti-retroviral drugs* Reverse Transcriptase Inhibitors (RTI’s)Reverse Transcriptase Inhibitors (RTI’s)
* NucleosideNucleoside* NucleotideNucleotide* Non-nucleosideNon-nucleoside
* Protease Inhibitors (PIs)Protease Inhibitors (PIs)* Fusion or Entry Inhibitors Fusion or Entry Inhibitors
* Act on gp41 or CCR5 coreceptorAct on gp41 or CCR5 coreceptor
* Integrase InhibitorsIntegrase Inhibitors* Fixed dose combinationsFixed dose combinations
* Drugs from two or more classes into a single productDrugs from two or more classes into a single product
TREATMENT OF HIV INECTION AND DISEASE
TREATMENT OF HIV INECTION AND DISEASE
* Reverse transcriptase inhibitorsReverse transcriptase inhibitors* Nucleoside analog (NARTI, NRTI)Nucleoside analog (NARTI, NRTI)
* Converted into nucleotide Converted into nucleotide
* Incorporated into and stops viral DNA synthesisIncorporated into and stops viral DNA synthesis
* Zidovudine (Retrovir)Zidovudine (Retrovir)
* Nucleotide analog (NtARTI, NtRTI)Nucleotide analog (NtARTI, NtRTI)* Incorporated into and stops viral DNA synthesisIncorporated into and stops viral DNA synthesis
* Tenofir (Viread)Tenofir (Viread)
* Non-nucleoside (NNRTI)Non-nucleoside (NNRTI)* Not incorporated into viral DNANot incorporated into viral DNA
* Binds to enzyme and inhibits functionBinds to enzyme and inhibits function
* Nevirapine (Viramune)Nevirapine (Viramune)
* Reverse transcriptase inhibitorsReverse transcriptase inhibitors* Nucleoside analog (NARTI, NRTI)Nucleoside analog (NARTI, NRTI)
* Converted into nucleotide Converted into nucleotide
* Incorporated into and stops viral DNA synthesisIncorporated into and stops viral DNA synthesis
* Zidovudine (Retrovir)Zidovudine (Retrovir)
* Nucleotide analog (NtARTI, NtRTI)Nucleotide analog (NtARTI, NtRTI)* Incorporated into and stops viral DNA synthesisIncorporated into and stops viral DNA synthesis
* Tenofir (Viread)Tenofir (Viread)
* Non-nucleoside (NNRTI)Non-nucleoside (NNRTI)* Not incorporated into viral DNANot incorporated into viral DNA
* Binds to enzyme and inhibits functionBinds to enzyme and inhibits function
* Nevirapine (Viramune)Nevirapine (Viramune)
TREATMENT OF HIV INECTION AND DISEASE
TREATMENT OF HIV INECTION AND DISEASE
* Goals of HAARTGoals of HAART* Suppression of HIVSuppression of HIV
* Decrease viral load Decrease viral load
* Reduce potential for resistance to anti-viral agentsReduce potential for resistance to anti-viral agents* Immune system reconstitutionImmune system reconstitution
* Restore CD4 T cell populationRestore CD4 T cell population
* Immune system reconstitutionImmune system reconstitution* Most successful with high baseline CD4 count at HAART initiationMost successful with high baseline CD4 count at HAART initiation* Increase of 50 to 150 cells per yearIncrease of 50 to 150 cells per year
* Goals of HAARTGoals of HAART* Suppression of HIVSuppression of HIV
* Decrease viral load Decrease viral load
* Reduce potential for resistance to anti-viral agentsReduce potential for resistance to anti-viral agents* Immune system reconstitutionImmune system reconstitution
* Restore CD4 T cell populationRestore CD4 T cell population
* Immune system reconstitutionImmune system reconstitution* Most successful with high baseline CD4 count at HAART initiationMost successful with high baseline CD4 count at HAART initiation* Increase of 50 to 150 cells per yearIncrease of 50 to 150 cells per year
TREATMENT OF HIV INECTION AND DISEASE
TREATMENT OF HIV INECTION AND DISEASE
* HAART negativesHAART negatives* High cost, medication fatigue, adherence to complicated drug regimens, High cost, medication fatigue, adherence to complicated drug regimens,
adverse events, names for anti-retroviral drugsadverse events, names for anti-retroviral drugs
* HAART InterruptionHAART Interruption* Minimize negatives using structured treatment interruption (STI)Minimize negatives using structured treatment interruption (STI)
* 6 months of IL-2 without HAART 6 months of IL-2 without HAART
* Safety (unclear) and efficacy (inferior) Safety (unclear) and efficacy (inferior)
* HAART associated withHAART associated with* Immune reconstitution syndromeImmune reconstitution syndrome
* HAART negativesHAART negatives* High cost, medication fatigue, adherence to complicated drug regimens, High cost, medication fatigue, adherence to complicated drug regimens,
adverse events, names for anti-retroviral drugsadverse events, names for anti-retroviral drugs
* HAART InterruptionHAART Interruption* Minimize negatives using structured treatment interruption (STI)Minimize negatives using structured treatment interruption (STI)
* 6 months of IL-2 without HAART 6 months of IL-2 without HAART
* Safety (unclear) and efficacy (inferior) Safety (unclear) and efficacy (inferior)
* HAART associated withHAART associated with* Immune reconstitution syndromeImmune reconstitution syndrome
IMMUNE RECONSTITUTION SYNDROME (IRS)
IMMUNE RECONSTITUTION SYNDROME (IRS)
* Immune reconstitution inflammatory syndrome (IRIS)Immune reconstitution inflammatory syndrome (IRIS)* Strong response by recovering immune system to latent or active infectionsStrong response by recovering immune system to latent or active infections
* Risk factors for IRIS following HAART Risk factors for IRIS following HAART * CD4 percent of < 15%CD4 percent of < 15%* CD4 count of < 100 cell/uLCD4 count of < 100 cell/uL* High rate of increase of CD 4 count High rate of increase of CD 4 count
* Most commonly associated withMost commonly associated with* Pneumocystis pneumoniaPneumocystis pneumonia* Cytomegalovirus diseaseCytomegalovirus disease* Herpes zosterHerpes zoster* Mycobacterium avium complex (MAC) diseaseMycobacterium avium complex (MAC) disease
* Tuberculosis Tuberculosis
* Immune reconstitution inflammatory syndrome (IRIS)Immune reconstitution inflammatory syndrome (IRIS)* Strong response by recovering immune system to latent or active infectionsStrong response by recovering immune system to latent or active infections
* Risk factors for IRIS following HAART Risk factors for IRIS following HAART * CD4 percent of < 15%CD4 percent of < 15%* CD4 count of < 100 cell/uLCD4 count of < 100 cell/uL* High rate of increase of CD 4 count High rate of increase of CD 4 count
* Most commonly associated withMost commonly associated with* Pneumocystis pneumoniaPneumocystis pneumonia* Cytomegalovirus diseaseCytomegalovirus disease* Herpes zosterHerpes zoster* Mycobacterium avium complex (MAC) diseaseMycobacterium avium complex (MAC) disease
* Tuberculosis Tuberculosis
IMMUNE RECONSTITUTION SYNDROME
IMMUNE RECONSTITUTION SYNDROME
* Important to distinguish between IRIS and clinical failureImportant to distinguish between IRIS and clinical failure
* Clinical failureClinical failure* Disease progression with development of OI or malignancy when Disease progression with development of OI or malignancy when
drugs given for sufficient timedrugs given for sufficient time
* IRISIRIS* Seen within first several weeks of therapy when a latent or active Seen within first several weeks of therapy when a latent or active
infection is presentinfection is present
* Important to distinguish between IRIS and clinical failureImportant to distinguish between IRIS and clinical failure
* Clinical failureClinical failure* Disease progression with development of OI or malignancy when Disease progression with development of OI or malignancy when
drugs given for sufficient timedrugs given for sufficient time
* IRISIRIS* Seen within first several weeks of therapy when a latent or active Seen within first several weeks of therapy when a latent or active
infection is presentinfection is present
IMMUNE RECONSTITUTION SYNDROME
IMMUNE RECONSTITUTION SYNDROME
* Management optionsManagement options* Inflammatory reaction treated withInflammatory reaction treated with
* SteroidsSteroids* Non-steroidal anti-inflammatory drugs (NSAIDS)Non-steroidal anti-inflammatory drugs (NSAIDS)
* Antimicrobial agents directed at the infectious agentAntimicrobial agents directed at the infectious agent
* Antiretroviral therapyAntiretroviral therapy* Withhold or continue (?)Withhold or continue (?)
* Management optionsManagement options* Inflammatory reaction treated withInflammatory reaction treated with
* SteroidsSteroids* Non-steroidal anti-inflammatory drugs (NSAIDS)Non-steroidal anti-inflammatory drugs (NSAIDS)
* Antimicrobial agents directed at the infectious agentAntimicrobial agents directed at the infectious agent
* Antiretroviral therapyAntiretroviral therapy* Withhold or continue (?)Withhold or continue (?)

NAMING ANTI-RETROVIRAL DRUGS
NAMING ANTI-RETROVIRAL DRUGS
* Anti-retroviral drugs have at least 3 names Anti-retroviral drugs have at least 3 names * AbbreviationAbbreviation
* Research or chemical nameResearch or chemical name* Generic nameGeneric name
* Generic nameGeneric name* Trade nameTrade name
* ExampleExample* Abbreviation (Research/Chemical) AZT Abbreviation (Research/Chemical) AZT * Abbreviation (Generic name) ZDVAbbreviation (Generic name) ZDV* Generic ZidovudineGeneric Zidovudine* Trade RetrovirTrade Retrovir
* Anti-retroviral drugs have at least 3 names Anti-retroviral drugs have at least 3 names * AbbreviationAbbreviation
* Research or chemical nameResearch or chemical name* Generic nameGeneric name
* Generic nameGeneric name* Trade nameTrade name
* ExampleExample* Abbreviation (Research/Chemical) AZT Abbreviation (Research/Chemical) AZT * Abbreviation (Generic name) ZDVAbbreviation (Generic name) ZDV* Generic ZidovudineGeneric Zidovudine* Trade RetrovirTrade Retrovir
MARAVORIC (MVC / SELZENTRY)MARAVORIC (MVC / SELZENTRY)
* First in new class anti-retroviral drugFirst in new class anti-retroviral drug* CCR5 co-receptor antagonist (entry inhibitor)CCR5 co-receptor antagonist (entry inhibitor)
* Indicated for CCR5 tropic HIV-1 showing resistance to multiple anti-Indicated for CCR5 tropic HIV-1 showing resistance to multiple anti-retroviral drugsretroviral drugs
* Black box warningBlack box warning* HepatotoxicityHepatotoxicity* Systemic allergic reactionSystemic allergic reaction
* Pruritic rash, eosinophilia, elevated IgEPruritic rash, eosinophilia, elevated IgE
* FDA approval on August 8, 2007FDA approval on August 8, 2007* Requires tropism testingRequires tropism testing
* First in new class anti-retroviral drugFirst in new class anti-retroviral drug* CCR5 co-receptor antagonist (entry inhibitor)CCR5 co-receptor antagonist (entry inhibitor)
* Indicated for CCR5 tropic HIV-1 showing resistance to multiple anti-Indicated for CCR5 tropic HIV-1 showing resistance to multiple anti-retroviral drugsretroviral drugs
* Black box warningBlack box warning* HepatotoxicityHepatotoxicity* Systemic allergic reactionSystemic allergic reaction
* Pruritic rash, eosinophilia, elevated IgEPruritic rash, eosinophilia, elevated IgE
* FDA approval on August 8, 2007FDA approval on August 8, 2007* Requires tropism testingRequires tropism testing

HIV CO-RECEPTOR TROPISM ASSAYHIV CO-RECEPTOR TROPISM ASSAY
* Trofile ™ (Monogram Bioscience)Trofile ™ (Monogram Bioscience)* FDA approval on August 6, 2007FDA approval on August 6, 2007
* In vitro diagnostic assayIn vitro diagnostic assay* Determines tropism of patient’s HIVDetermines tropism of patient’s HIV
* CCR5 CCR5 * CXCR4CXCR4* D/M (dual / mixed)D/M (dual / mixed)
* Trofile ™ assayTrofile ™ assay* Specimen is EDTA plasmaSpecimen is EDTA plasma* Viral load of 1,000 copies/mLViral load of 1,000 copies/mL* TAT of 14 daysTAT of 14 days* Cost $$$$$Cost $$$$$
* Trofile ™ (Monogram Bioscience)Trofile ™ (Monogram Bioscience)* FDA approval on August 6, 2007FDA approval on August 6, 2007
* In vitro diagnostic assayIn vitro diagnostic assay* Determines tropism of patient’s HIVDetermines tropism of patient’s HIV
* CCR5 CCR5 * CXCR4CXCR4* D/M (dual / mixed)D/M (dual / mixed)
* Trofile ™ assayTrofile ™ assay* Specimen is EDTA plasmaSpecimen is EDTA plasma* Viral load of 1,000 copies/mLViral load of 1,000 copies/mL* TAT of 14 daysTAT of 14 days* Cost $$$$$Cost $$$$$

LABORATORY DIAGNOSIS OF HIV INFECTION
LABORATORY DIAGNOSIS OF HIV INFECTION
* Standard algorithm consists of using two tests for the detection of antibody to HIV-1/2* Screening
* Enzyme immunoassay (EIA) or
* Enzyme-linked Immunosorbent Assay (ELISA)
* High sensitivity
* Confirmation* Western blot (WB)
* High specificity
* Sensitivity is “positivity in disease”
* Specificity is “negativity in disease”
* Standard algorithm consists of using two tests for the detection of antibody to HIV-1/2* Screening
* Enzyme immunoassay (EIA) or
* Enzyme-linked Immunosorbent Assay (ELISA)
* High sensitivity
* Confirmation* Western blot (WB)
* High specificity
* Sensitivity is “positivity in disease”
* Specificity is “negativity in disease”
LABORATORY DIAGNOSIS OF HIV INFECTION (STANDARD ALGORITHM)
LABORATORY DIAGNOSIS OF HIV INFECTION (STANDARD ALGORITHM)
* Specimens “initially reactive” by EIA / ELISA are retested in duplicate* One or both repeat tests positive, specimens are considered “repeatedly reactive” for
antibody
* Specimens “repeatedly reactive” by EIA / ELISA then tested by Western Blot (WB) assay
* Specimens “reactive” for both EIA / ELISA and WB are considered “positive” for HIV infection
* Seroconversion * From infection to antibody
* Specimens “initially reactive” by EIA / ELISA are retested in duplicate* One or both repeat tests positive, specimens are considered “repeatedly reactive” for
antibody
* Specimens “repeatedly reactive” by EIA / ELISA then tested by Western Blot (WB) assay
* Specimens “reactive” for both EIA / ELISA and WB are considered “positive” for HIV infection
* Seroconversion * From infection to antibody
LABORATORY DIAGNOSIS OF HIV INFECTION
LABORATORY DIAGNOSIS OF HIV INFECTION
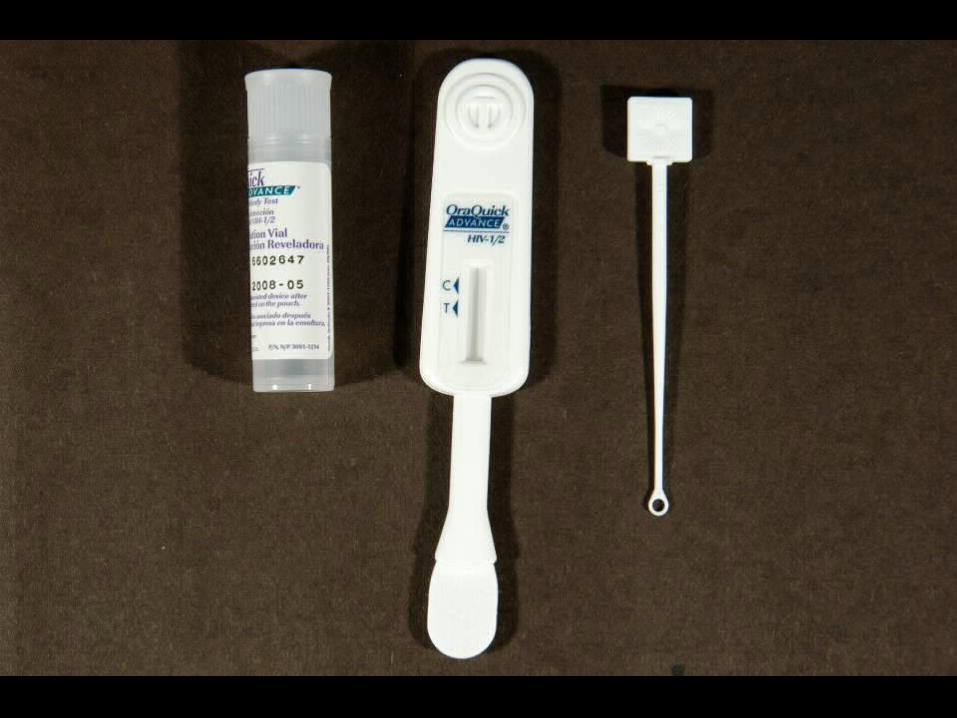
* Rapid detection of HIV-1/2 antibody
* OraQuick ® ADVANCE ™ Rapid HIV-1/2 Antibody* OraSure Technologies, Inc., PA
* Immunochromatographic assay (ICA)
* Analytical time of 25 minutes
* Sensitivity of 99.5% and specificity of 99.9%
* Specimens of Choice* Whole blood
* Fingerstick
* Venipuncture (EDTA)
* EDTA plasma
* Oral fluid (Oral mucosal transudate)
* Rapid detection of HIV-1/2 antibody
* OraQuick ® ADVANCE ™ Rapid HIV-1/2 Antibody* OraSure Technologies, Inc., PA
* Immunochromatographic assay (ICA)
* Analytical time of 25 minutes
* Sensitivity of 99.5% and specificity of 99.9%
* Specimens of Choice* Whole blood
* Fingerstick
* Venipuncture (EDTA)
* EDTA plasma
* Oral fluid (Oral mucosal transudate)


CLINICAL USE OF ORAQUICK ® RAPID HIV-1/2 ASSAY
CLINICAL USE OF ORAQUICK ® RAPID HIV-1/2 ASSAY
* Rapid screening* HCW with potential HIV exposure
* Pregnant females with unknown HIV status at time of delivery
* New HIV clinic patients
* Same day screening* All other patients
* Reporting of Results* Negative for HIV-1/2 Antibodies
* Preliminary Positive for HIV-1/2 Antibodies. Confirmation by Western Blot testing to follow.
* Rapid screening* HCW with potential HIV exposure
* Pregnant females with unknown HIV status at time of delivery
* New HIV clinic patients
* Same day screening* All other patients
* Reporting of Results* Negative for HIV-1/2 Antibodies
* Preliminary Positive for HIV-1/2 Antibodies. Confirmation by Western Blot testing to follow.




LABORATORY DIAGNOSIS OF HIV INFECTION
LABORATORY DIAGNOSIS OF HIV INFECTION
* Detection of HIV Core Antigen (p24)* Serum or CSF
* Methods* EIA or ELISA (Non-ICD)* EIA or ELISA (immune complex dissociation)* Positives confirmed by neutralization
* Clinical Use* Early diagnosis before antibody response* Monitor effectiveness of therapy* Marker of disease progression
* Detection of HIV Core Antigen (p24)* Serum or CSF
* Methods* EIA or ELISA (Non-ICD)* EIA or ELISA (immune complex dissociation)* Positives confirmed by neutralization
* Clinical Use* Early diagnosis before antibody response* Monitor effectiveness of therapy* Marker of disease progression

LABORATORY DIAGNOSIS OF HIV INFECTION
LABORATORY DIAGNOSIS OF HIV INFECTION
* Detection of proviral DNA* EDTA whole blood
* Method* Polymerase chain reaction (PCR)
* Clinical Use* Diagnosis of infection in neonates of HIV positive mothers* Early diagnosis before antibody response
* Detection of proviral DNA* EDTA whole blood
* Method* Polymerase chain reaction (PCR)
* Clinical Use* Diagnosis of infection in neonates of HIV positive mothers* Early diagnosis before antibody response
LABORATORY PROGNOSIS OF HIV INFECTION
LABORATORY PROGNOSIS OF HIV INFECTION
* Quantitation of HIV-1 RNA (Viral load)* EDTA plasma
* Methods * Reverse Transcriptase – PCR (RT-PCR)* Branched chain DNA (bDNA)
* Clinical Use* Determination of amount of free virus (Viral load)* Predicting progression and outcome of infection* Assessing efficacy of antiviral therapy
* Quantitation of HIV-1 RNA (Viral load)* EDTA plasma
* Methods * Reverse Transcriptase – PCR (RT-PCR)* Branched chain DNA (bDNA)
* Clinical Use* Determination of amount of free virus (Viral load)* Predicting progression and outcome of infection* Assessing efficacy of antiviral therapy

LABORATORY DIAGNOSIS OF HIV INFECTION BY ORAL FLUID TESTING
LABORATORY DIAGNOSIS OF HIV INFECTION BY ORAL FLUID TESTING
* OraQuick ® ADVANCE ™ Rapid HIV-1/2 Antibody Test* Pad on test device used to swab between upper and
lower outer gums and cheek
* Pad is stored in preservative vial and sent for ICA testing
* Advantages* Reduces occupational exposure
* Patient appeal
* OraQuick ® ADVANCE ™ Rapid HIV-1/2 Antibody Test* Pad on test device used to swab between upper and
lower outer gums and cheek
* Pad is stored in preservative vial and sent for ICA testing
* Advantages* Reduces occupational exposure
* Patient appeal

LABORATORY DIAGNOSIS OF HIV INFECTION BY URINE TESTING
LABORATORY DIAGNOSIS OF HIV INFECTION BY URINE TESTING
* Calypte HIV-1 Urine EIA (Calypte Biomedical, Berkeley, CA)* FDA approval for EIA (1996) and Western Blot (1998)
* Sensitivity and specificity * Lower compared to blood and oral fluid
* Question* IgG in urine
* Calypte ® Aware ™ HIV-1/2 Urine Rapid Test* Available outside US
* Advantages* Reduces occupational exposure* Patient appeal
* Calypte HIV-1 Urine EIA (Calypte Biomedical, Berkeley, CA)* FDA approval for EIA (1996) and Western Blot (1998)
* Sensitivity and specificity * Lower compared to blood and oral fluid
* Question* IgG in urine
* Calypte ® Aware ™ HIV-1/2 Urine Rapid Test* Available outside US
* Advantages* Reduces occupational exposure* Patient appeal
THE IMMUNOLOGY OF HIV INFECTION
THE IMMUNOLOGY OF HIV INFECTION
* Interactions between HIV and human immune system are extremely complex
* HIV subverts immune system by * Infecting CD4 T cells and inducing quantitative and qualitative
dysfunction
* Hyperactivating B cells with resulting hypergammaglobulinemia
* Inducing cytokine system to own replicative advantage
* There are no known correlates of protective immunity
* Interactions between HIV and human immune system are extremely complex
* HIV subverts immune system by * Infecting CD4 T cells and inducing quantitative and qualitative
dysfunction
* Hyperactivating B cells with resulting hypergammaglobulinemia
* Inducing cytokine system to own replicative advantage
* There are no known correlates of protective immunity

MECHANISMS OF CD4 T-CELL DEPLETION
MECHANISMS OF CD4 T-CELL DEPLETION
* Direct killing of infected T cellsDirect killing of infected T cells
* Increased rate of apoptosis in infected T cellsIncreased rate of apoptosis in infected T cells* Molecule associated with apoptosis (PD-1) is over-expressed in Molecule associated with apoptosis (PD-1) is over-expressed in
chronic viremiachronic viremia
* Syncytia formationSyncytia formation* Fusion of infected and non-infected T cellsFusion of infected and non-infected T cells
* Killing of infected CD4 cells by CD8 cellsKilling of infected CD4 cells by CD8 cells
* Direct killing of infected T cellsDirect killing of infected T cells
* Increased rate of apoptosis in infected T cellsIncreased rate of apoptosis in infected T cells* Molecule associated with apoptosis (PD-1) is over-expressed in Molecule associated with apoptosis (PD-1) is over-expressed in
chronic viremiachronic viremia
* Syncytia formationSyncytia formation* Fusion of infected and non-infected T cellsFusion of infected and non-infected T cells
* Killing of infected CD4 cells by CD8 cellsKilling of infected CD4 cells by CD8 cells
KILLING OF INFECTED CD4 CELLS BY CD8 CELLS – ALTERNATIVE VIEW
KILLING OF INFECTED CD4 CELLS BY CD8 CELLS – ALTERNATIVE VIEW
* Mechanism that keeps HIV in check in long term non-progressors Mechanism that keeps HIV in check in long term non-progressors (LTNPs)(LTNPs)
* Long term non-progressors (LTNPs)Long term non-progressors (LTNPs)* Carry the virus but do not get AIDSCarry the virus but do not get AIDS
* Have 20 times more CD8 T cells than progressorsHave 20 times more CD8 T cells than progressors
* Function of CD8 T cell surplusFunction of CD8 T cell surplus* Up-regulate production (2X rate of progressors) of 2 killer proteinsUp-regulate production (2X rate of progressors) of 2 killer proteins
* PerforinPerforin
* Granzyme BGranzyme B
* Mechanism that keeps HIV in check in long term non-progressors Mechanism that keeps HIV in check in long term non-progressors (LTNPs)(LTNPs)
* Long term non-progressors (LTNPs)Long term non-progressors (LTNPs)* Carry the virus but do not get AIDSCarry the virus but do not get AIDS
* Have 20 times more CD8 T cells than progressorsHave 20 times more CD8 T cells than progressors
* Function of CD8 T cell surplusFunction of CD8 T cell surplus* Up-regulate production (2X rate of progressors) of 2 killer proteinsUp-regulate production (2X rate of progressors) of 2 killer proteins
* PerforinPerforin
* Granzyme BGranzyme B


IMMUNE DYSFUNCTION DURING HIV INFECTION - SUMMARY
IMMUNE DYSFUNCTION DURING HIV INFECTION - SUMMARY
* HIV infection is multifactorial process capable of disarming immune system by direct and indirect mechanisms
* Certain chemokine receptors function as necessary coreceptors for entry of HIV into cells
* Central Paradox* Progression of HIV disease in setting of vigorous immune
response
* Lack of correlates of protective immunity are major obstacle to immunotherapy and vaccine development
* HIV infection is multifactorial process capable of disarming immune system by direct and indirect mechanisms
* Certain chemokine receptors function as necessary coreceptors for entry of HIV into cells
* Central Paradox* Progression of HIV disease in setting of vigorous immune
response
* Lack of correlates of protective immunity are major obstacle to immunotherapy and vaccine development