
HIV cure research update - UKCAB€¦ · HIV$aaches$to$any$cell$with$certain$receptors$on$its$...
29
HIV HIV cure research
-
Upload
truongdung -
Category
Documents
-
view
218 -
download
5
Transcript of HIV cure research update - UKCAB€¦ · HIV$aaches$to$any$cell$with$certain$receptors$on$its$...

HIV
HIV cure research

Summary of talk
• The immune system • HIV • HIV treatment • HIV cure?

The role of the immune system
• Danger signal and recognise and remove abnormal cells
• Check for cancer cells iden:fy sick cells • Remove invaders • Kill the bad cells • Ignore “self”

Cells of the immune system

HIV virus

HIV aBaches to any cell with certain receptors on its surface and inserts virus gene:c material into the cells
own DNA

What happens to the person living with HIV?
• Virus infects usually through mucosal surfaces-‐ genital or gut
• Passes to local lymphoid :ssue • Spreads all round the body • Kills CD4 –cells and rests in “sleeping” cells of the immune system to form a latent pool of invisible and inaccessible cells

Treatment works!!treatment (ART) works!!


The success of ART
Gap report130
Where the criminalization of behaviours that affect key populations exists, access to testing and treatment must not be linked to criminal prosecution or other punitive consequences. A combination of approaches is needed in order to reach a greater number of people. Confidential and voluntary HIV testing options should include clinic-based testing, mobile testing, community-based testing, door-to-door testing and home-based testing kits with linkages to clinic- or community-based confirmation testing for positive results.
Innovative testing and service delivery models include multi disease, community health campaigns and service delivery (32). New technologies such as self-testing encourage a high uptake of HIV testing (33).
Projected impact of highly active antiretroviral therapy on expected survival of a 20-year-old person living with HIV in a high-income country
Source: Adapted from Lohse et al, 2007; Hoog et al, 2008, May et al, 2011 & Hogg et al, 2013.
+8years
+36years
+45years
+51years
+55years
HIV+1995–1996
HIV+2000–2002
HIV+2003–2006
HIV+2006–2007
HIV+2010
Pote
ntia
l sur
viva
l gai
ns (y
ears
)
Era before highly active antiretroviral therapy
(mono- and dual therapy)
Era of highly active antiretroviral therapy (triple therapy)
+60years
HIV- negative
+30
+40
+50
+60
+70
+80
+20
Source: UNAIDS, gap report. Adapted from Lohse et al, 2007; Hoog et al. 2008; May et al, 2011; Hogg et al. 2013
Expected survival of a 20-‐year-‐old person living with HIV in a high income country
Era before ART Era of ART
Gap report130
Where the criminalization of behaviours that affect key populations exists, access to testing and treatment must not be linked to criminal prosecution or other punitive consequences. A combination of approaches is needed in order to reach a greater number of people. Confidential and voluntary HIV testing options should include clinic-based testing, mobile testing, community-based testing, door-to-door testing and home-based testing kits with linkages to clinic- or community-based confirmation testing for positive results.
Innovative testing and service delivery models include multi disease, community health campaigns and service delivery (32). New technologies such as self-testing encourage a high uptake of HIV testing (33).
Projected impact of highly active antiretroviral therapy on expected survival of a 20-year-old person living with HIV in a high-income country
Source: Adapted from Lohse et al, 2007; Hoog et al, 2008, May et al, 2011 & Hogg et al, 2013.
+8years
+36years
+45years
+51years
+55years
HIV+1995–1996
HIV+2000–2002
HIV+2003–2006
HIV+2006–2007
HIV+2010
Pote
ntia
l sur
viva
l gai
ns (y
ears
)
Era before highly active antiretroviral therapy
(mono- and dual therapy)
Era of highly active antiretroviral therapy (triple therapy)
+60years
HIV- negative
+30
+40
+50
+60
+70
+80
+20
Gap report130
Where the criminalization of behaviours that affect key populations exists, access to testing and treatment must not be linked to criminal prosecution or other punitive consequences. A combination of approaches is needed in order to reach a greater number of people. Confidential and voluntary HIV testing options should include clinic-based testing, mobile testing, community-based testing, door-to-door testing and home-based testing kits with linkages to clinic- or community-based confirmation testing for positive results.
Innovative testing and service delivery models include multi disease, community health campaigns and service delivery (32). New technologies such as self-testing encourage a high uptake of HIV testing (33).
Projected impact of highly active antiretroviral therapy on expected survival of a 20-year-old person living with HIV in a high-income country
Source: Adapted from Lohse et al, 2007; Hoog et al, 2008, May et al, 2011 & Hogg et al, 2013.
+8years
+36years
+45years
+51years
+55years
HIV+1995–1996
HIV+2000–2002
HIV+2003–2006
HIV+2006–2007
HIV+2010
Pote
ntia
l sur
viva
l gai
ns (y
ears
)
Era before highly active antiretroviral therapy
(mono- and dual therapy)
Era of highly active antiretroviral therapy (triple therapy)
+60years
HIV- negative
+30
+40
+50
+60
+70
+80
+20

Why do we need a cure?


Circula:
ng viru
s
Time
HIV persists during ART
ART does not eradicate HIV
ART

Why can’t ART cure HIV?

Barriers to an HIV cure
HIV persistence in :ssues
Latently infected cells are rare and undis:nguishable
from uninfected cells
Latently infected cells are diverse
EradicaHon strategy should reach Hssues
EradicaHon strategy should be specific
EradicaHon strategy should target all infected
cells

TW Chun et al. J Infect Dis 2008; S. Yukl et al. J Infect Dis 2010; M. Churchill et al. Annals Neur 2010; C. Fletcher et al. PNAS 2014; M. Perreau et al. J Exp Med 2013
Where does HIV hide?

Two types of cure
• “Sterilizing” cure
• “Func:onal” cure

What is the difference between the two types of Cure?
FuncHonal cure • Absence of ongoing viral
replica:on in the absence of an:retroviral therapy
• Detectable viral DNA but no/liBle evidence of viral transcrip:on or replica:on
• No risk of onward transmission
• No ongoing immunological damage
Sterilising Cure • No detectable virus DNA
AND RNA • No detectable viral
reservoir • No detectable viral
transcrip:on • Timothy Brown

1 man in the world has been Cured
• Was it the stem cell transplant alone? – 2 recent reports of “no detectable virus” following allogeneic transplanta:on
with con:nuous ART (IAS 2013) • Was it the CCR5Δ32 transplant? • Was it GVHD? • Was it EVERYTHING

Cure strategies
To reduce the size of the reservoir

Approach 1: Treat EARLY Impact of early ART on HIV persistence (RV254)
J. Ananworanich et al. Plos One 2012; J. Ananworanich et al. Journal of Viral Eradica:on 2015; C. Vandergeeten, in prepara:on.
Very early ART (<2-‐3 weeks aPer infecHon) dramaHcally reduces the frequency of cells carrying integrated genomes
0 20 40 60 80 1000.1
1
10
100
1000
10000
Time (weeks)
Inte
grat
ed H
IV D
NA
(cop
ies/
106
PBM
Cs)
FIFIIIChronic (Search 011)
ART started: during chronic infec:on
<17 days ajer infec:on <25 days ajer infec:on

Approach 2: Render uninfected cells resistant to HIV
SB-‐728 vector (CCR5 disrup:on Zn Finger)
CD4 T cells enrichment
leukapheresis
Adapted from P. Tebas et al. New. Engl. J. Med. 2014
infusion
expansion

Approach 3: Flush out the latent reservoir (Shock and kill)
“Latency reversing agent”
Cytopathic effect Immune response
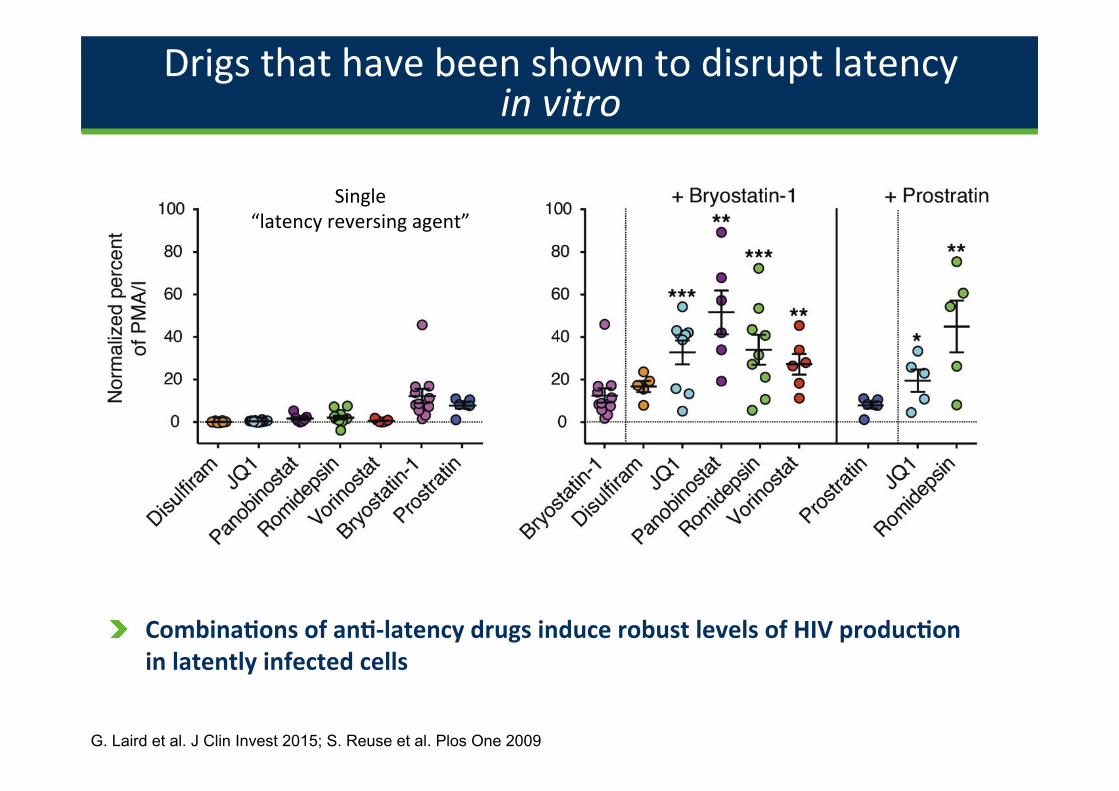
Drigs that have been shown to disrupt latency in vitro
G. Laird et al. J Clin Invest 2015; S. Reuse et al. Plos One 2009
CombinaHons of anH-‐latency drugs induce robust levels of HIV producHon in latently infected cells
Single “latency reversing agent”

Approach 4: (plus 3?) Help the immune system Immune checkpoints and HIV persistence
Immune checkpoints are expressed at the surface of infected cells and inhibit viral reacHvaHon from latency
R. Fromen:n et al. in prepara:on.
• Immune checkpoints (PD-‐1, LAG-‐3, TIGIT, CTLA-‐4) nega:vely regulate (switch off) T cell responses and contribute to immune exhaus:on
• These molecules can be blocked by an:bodies to restore HIV-‐specific immunity
0
3
6
9
12
Rel
ativ
e en
richm
ent i
n in
tegr
ated
HIV
DN
A Number of immune checkpoints
123
0
Number of immune checkpoints
0 1 2 3
0
20
40
60
80
100
Cell-
free
HIV
RNA
(% o
f CD3
/CD2
8)
CD3/CD28PD-L1
--
+-
++
Ac:va:on Ac:va:on + PD-‐1
engagement
No Ac:va:on
HIV prod
uc:o
n
+
-‐ +
PD-‐1

Protocol Overview A two-‐arm (proof of concept) randomised phase II trial


Summary
• New ideas to cure HIV • Block viral replica:on with ART • Add in drugs that ac:vate virus from the latently infected pool
• Wake up the immune system to kill these virus expressing cells
• Will people get re-‐infected though? • Are the drugs toxic • How much will this cost?

IS PHI the best :me to move towards an HIV cure?
Thanks Community of people living with HIV and Simon Collins, Damien Kelly CHERUB collabora:on John Frater Nicholas Chomont RIVER trial management team Funders: MRC, NIHR BRC, AmFAR, Industry partners (MSD, GSK)


















