
HISTOPATHOLOGICAL STUDY OF BREAST TUMOURS IN …
66
1 HISTOPATHOLOGICAL STUDY OF BREAST TUMOURS IN KANO: A TEN YEAR RETROSPECTIVE REVIEW (2001-2010) BEING A DISSERTATION SUBMITTED IN PARTIAL FULFILMENT OF REQUIREMENTS FOR THE FELLOWSHIP OF THE NATIONAL POSTGRADUATE MEDICAL COLLEGE OF NIGERIA IN PATHOLOGY BY: DR.MOHAMMED IBRAHIM IMAM AF/008/09/115/646 SUPERVISORS: COL. (DR.) YAWALE ILIYASU, MBBS, FMCPath, FICS, MIAC CONSULTANT PATHOLOGIST /SENIOR LECTURER, AHMADU BELLO UNIVERSITY TEACHING HOSPITAL/AHMADU BELLO UNIVERSITY, ZARIA. DR.AMINU ZAKARI MOHAMMED MBBS, FMCPath. CONSULTANT PATHOLOGIST/READER, DEPARTMENT OF PATHOLOGY, AMINU KANO TEACHING HOSPITAL/BAYERO UNIVERSITY, KANO.
Transcript of HISTOPATHOLOGICAL STUDY OF BREAST TUMOURS IN …
1
HISTOPATHOLOGICAL STUDY OF BREAST TUMOURS IN KANO:
A TEN YEAR RETROSPECTIVE REVIEW
(2001-2010)
BEING A DISSERTATION SUBMITTED IN PARTIAL FULFILMENT OF
REQUIREMENTS FOR THE FELLOWSHIP OF THE NATIONAL
POSTGRADUATE MEDICAL COLLEGE OF NIGERIA IN PATHOLOGY
BY:
DR.MOHAMMED IBRAHIM IMAM
AF/008/09/115/646
SUPERVISORS:
COL. (DR.) YAWALE ILIYASU, MBBS, FMCPath, FICS, MIAC
CONSULTANT PATHOLOGIST /SENIOR LECTURER,
AHMADU BELLO UNIVERSITY TEACHING HOSPITAL/AHMADU BELLO
UNIVERSITY, ZARIA.
DR.AMINU ZAKARI MOHAMMED MBBS, FMCPath.
CONSULTANT PATHOLOGIST/READER,
DEPARTMENT OF PATHOLOGY, AMINU KANO TEACHING
HOSPITAL/BAYERO UNIVERSITY, KANO.
2
CERTIFICATION
We hereby certify that the study in this dissertation: Histopathological Study of Breast
Tumours in Kano: A Ten year Retrospective Review (2001- 2010) was carried out in
the Department of Pathology, Aminu Kano Teaching Hospital, Kano under our
supervision.
__________________________________________
Signature
COL. (DR.) YAWALE ILIYASU, MBBS, FMCPath, FICS, MIAC
CONSULTANT PATHOLOGIST/ SENIOR LECTURER
DEPARTMENT OF PATHOLOGY
AHMADU BELLO UNIVERSITY TEACHING HOSPITAL/ AHMADU BELLO
UNIVERSITY, ZARIA.
___________________________________________
Signature
DR. AMINU ZAKARI MOHAMMED, MBBS, FMCPath
CONSULTANT PATHOLOGIST/ READER,
DEPARTMENT OF PATHOLOGY
AMINU KANO TEACHING HOSPITAL/ BAYERO UNIVERSITY, KANO.
3
DECLARATION
I hereby declare that this dissertation is an original work done by me and that, to the
best of my knowledge, it contains no material previously published by me nor has it
been presented to any college for the award of fellowship or any degree or diploma nor
has it been submitted elsewhere for publication.
________________________________________
DR. M. I. IMAM
1st June, 2012

4
DEDICATION
This work is dedicated to my parents, to whom credit belongs for who I am today, my
Tutors, for guiding me through the Residency training programme and to my wife and
children for enduring all the years of the training.

5
ACKNOWLEDGEMENT
I thank Almighty God for giving me the life, health and wisdom to reach this stage of
my life. My sincere gratitude and appreciation goes to Col. (Dr.) Yawale Iliyasu and
Dr. A. Z. Mohammed who guided me through successful completion of this
dissertation. I also wish to express my deepest regards to Drs Ochicha, Malami,
Atanda and Umar who are never tired of sharing their wealth of experience with me. I
also thank my dearest colleagues, Drs Yusuf and Adogu, Mrs. Atanda, Mallam Sani,
other members of pathology Department, AKTH, Kano and my nuclear and extended
family for their support and encouragement.

6
TABLE OF CONTENTS
Item Description Page
Title page i
Certification ii
Declaration iii
Dedication iv
Acknowledgement v
Table of contents vi
List of tables vii
List of figures viii
Abstract ix
Chapter One:
Introduction 1-2
Aims and Objectives 3
Chapter Two:
Literature review
Benign breast tumours 4-6
Breast cancer
Epidemiology 7-11
Histological subtypes of breast cancer 12-17
Histological grading of breast cancer 18-19
Prognostic factors 20-22
Chapter Three:
Materials and Methods 23
Exclusion Criteria 24
Limitations of Study 24
Chapter Four: Results 25-27
Tables 28-33
Figures 34-38
Chapter Five: Discussion 39-44
Conclusion 45

7
References 46-51
Appendix 52-55

8
LIST OF TABLES
Table Title Page
1. Histopathological Distribution of Benign Breast Tumours 28
2. Histopathological Distribution of Malignant Breast Tumours 28
3. Age Distribution of Benign Breast Tumours according to
Histological subtypes 29
4. Age Distribution of Malignant Breast Tumours According to
Histological Subtypes 30
5. Sex Distribution of Malignant Breast Tumours According to
Histological Types 31
6. Laterality of common Benign Breast Tumours 32
7. Laterality of common Malignant Breast Tumours 32
8. Nottingham Grading of Breast Cancer According to
Histological Types 33
9
LIST OF FIGURES
Figure Title Page
1. Pie chart showing histological distribution of malignant
breast tumours 34
2. Fibroadenoma 35
3. Fibrocystic change 35
4. Invasive ductal carcinoma (NST) 36
5. Medullary carcinoma 36
6. Adenoid cystic carcinoma 37
7. Invasive lobular carcinoma 37
8. Burkitt lymphoma 38

10
ABSTRACT
This ten year retrospective histopathological review was carried out to classify, grade
and to determine the changing pattern, frequency, age and sex distribution of breast
tumours received in the histopathology department of Aminu Kano Teaching Hospital,
(AKTH), Kano from 1st January, 2001 to 31st December, 2010.
The study comprised of all cases of breast tumours diagnosed over the 10 year review
period. Laboratory request forms and duplicate copies of histology reports were
retrieved and relevant clinical information such as age, sex, side and histologic types
of the tumours were extracted. Corresponding haematoxylin and eosin stained slides
were reviewed and evaluated. Special stains such as Periodic acid schiff (PAS) and
mucicarmine were used for some cases where necessary. The tumours were classified
according to WHO classification and graded using the Nottingham grading system and
the results analyzed using frequency tables and pie chart.
A total of 1566 breast tumours were received during the period under review and of
these 1035 (66.3%) were benign and 531 (33.7%) were malignant, with a benign to
malignant ratio of approximately 2:1. The malignant breast tumours accounted for
11.9% overall of all the malignant tumours while benign breast tumours accounted for
8.3% of all the benign tumours received in the Department from all sites during the
period. The age range of the benign tumours was 13 to 63 years with a mean age of 29
years. The frequency of benign tumours peaked in the 3rd decade accounting for 432
(41.7%) cases. The most common benign breast tumour was fibroadenoma (47.1%)
followed by fibrocystic change (25.4%). Laterality was documented in 984 benign
tumours out of which 541 (55.0%), 414 (42.1%) and 30 (2.9%) were right – sided, left
– sided and bilateral respectively.
The malignant breast tumours similarly had a wide age range of 15 to 80 years with a
mean age of 42 years. Invasive ductal carcinoma(NST) was the commonest malignant
breast tumour accounting for 316 (59.5%) cases followed by medullary carcinoma
with 61 (11.5%) cases, Invasive lobular and papillary carcinomas each with 37 (6.9%)
cases. Of the 1472 malignant breast tumours documented with laterality, 860 (58.4%),

11
581 (39.5%) and 32 (2.8%) were right – sided, left – sided and bilateral respectively.
The malignant breast tumours were graded according to Nottingham grading system.
Two hundred and thirty seven (44.6%) cases were classified as grade 1, grade 2
tumours accounted for 133 (25.0%) cases and grade 3 tumours are composed of 161
(30.4%) cases.
CHAPTER ONE
INTRODUCTION
The breast is an externally located organ which is phylogenetically considered as a modification
of sweat glands.1 It is a unique organ that is not fully developed at birth, undergoes cyclical
changes during reproductive life, and starts to involute along time before menopause.2
The breast remains rudimentary in adult males, but plays an important part in human sexual
behaviour being one of the most visible or obvious female secondary sex characteristics which is
a hallmark of pubertal development. It also serves a major role in enhancing a woman’s
confidence and personality. It is specialized for production of milk as natural nourishment of the
newborn and infants. Thus, the importance of the breast in ensuring that women successfully
play these roles cannot be overemphasized.3
Breast tumours are commonly seen in clinical practice worldwide amongst females of various
age groups and less frequently in men. Benign breast tumours usually outnumber the malignant
types by a wide margin.4
Breast cancer constitutes a major public health issue globally with over 1million new cases
diagnosed annually, resulting in over 400,000 annual deaths and about 4.4 million women living
with the disease. It is the commonest site specific malignancy affecting women and the most
common cause of cancer mortality in women world wide.5
Incidence rates are higher in the developed countries than in the developing countries, and are
also higher in urban areas than in the rural areas. In Africa, breast cancer has overtaken cervical
cancer as the commonest malignancy affecting women and the incidence rates appear to be rising
12
due to changes in the demography, socio-economic parameters, epidemiologic risk factors, better
reporting and awareness of the disease.6,7
The mortality rate is declining in the developed world (America, Australia and Western Europe)
as a result of breast cancer screening, early diagnosis and improved cancer treatment
programmes. The reverse is the case in the developing world as well as in eastern and central
Europe.8
Rationale for study:
Although breast cancer is by far the commonest female malignancy worldwide and is the major
reason for the interest in breast lumps in general, there have been relatively few studies of this
deadly scourge in northern Nigeria. Most Nigerian studies of breast tumours are from the south,
and given the differences in demography, lifestyle and possibly genetics, they may not be
reflective of the entire Nigerian populace. Being the most populous state in Nigeria (2006
census), Kano is particularly well placed to provide representative data for the north.
Over a decade ago two studies on breast tumours were carried out here in Kano. One focused on
benign breast lesions and the other on malignant conditions of the breast. The small sample sizes
of those initial studies from the then newly established pathology department render them less
statistically significant and less representative of today’s much larger breast tumour burden in
Kano.
Breast cancer was second to cervical cancer as the commonest female malignancy back then, but
recent studies and unpublished data from our cancer registry indicate that breast cancer is now
the indisputable premier malignancy in Kano. This evident surge in breast cancer prevalence
suggests a change in trend which needs to be investigated, hence the relevance of this study.
Also with the advent of current classification and new information in the International literature
on breast tumours which suggest an evolving pattern of histopathology of breast tumours further
motivated the need for this study.

13

14
AIMS AND OBJECTIVES
The study is aimed at achieving the following objectives:
1. To classify and grade the histopathological types of breast tumours seen in the Department of
Pathology, Aminu Kano Teaching Hospital, Kano over a period of 10 years (2001-2010)
using WHO classification of breast tumours (2002) and Nottingham grading system of breast
cancer respectively.
2. To determine the distribution, frequency and laterality of breast tumours in various sex and
age groups.
3. To compare the findings with studies in other parts of Nigeria, Africa and the rest of the
world.

15
CHAPTER TWO
LITERATURE REVIEW
BENIGN BREAST TUMOURS
Tumours of the breast are among the most common human neoplasms which occur worldwide. 9
The incidence and histological subtypes of these tumours vary from one region of the world to
the other.10
Increasing awareness of breast cancer has stimulated profound interest in benign breast diseases
since certain epithelial benign breast lesions have been associated with malignant
transformation.11 Benign breast tumours include fibroadenoma, granular cell tumours, intraductal
papillomas and benign phyllodes tumours.12 Generally, as with neoplasms of other organs, the
benign breast tumours occur more frequently than the malignant breast tumours in both sexes,
and worldwide fibroadenoma is the most common benign breast tumour.
Reports from Hong Kong and India by Cederquist and Onukak 13 on benign breast disorders in
nonwestern populations showed that fibroadenoma is the most common benign breast tumour
among young adolescent girls. A study among Afro-Caribbean populations in Jamaica14 showed
that fibroadenomas constituted 33% of all the benign breast diseases.
In Ghana15 out of a total of 65 breast specimens sampled, 31(48%) were fibroadenomas,
21(32%) cancers, and 13(20%) miscellaneous benign diseases. It also accounted for 70% of all
the benign breast lesions. A histopathologic review from Kenya16 showed that fibroadenomas
constituted 49% of all the benign breast lesions.
A study conducted in Zaria, Nigeria by Yusuf et al17 on breast masses, showed that benign breast
lesions constitute 71.3%, with fibroadenoma and fibrocystic change accounting for 24% and
15.2% of the cases respectively.
In a 7 year review of benign breast diseases in Ilesha, Nigeria by Adesukanmi and Agbakwuru,18
histopathologic analysis showed that fibroadenoma accounted for 46.2% of the entire benign
breast tumours. Similarly, a 10 year review of benign breast tumours among Igbos by Anyanwu19
showed that fibroadenoma was the commonest adolescent breast mass in Nigerian Igbos
accounting for 33% of the cases and appeared earlier than in industrialized regions. He attributed

16
the differences to hormonal imbalances. A survey by Mayun et al20 in Gombe on pattern of
histopathological diagnosis of breast lesions showed that 59.5% of the breast lesions are benign
and fibroadenoma was the commonest constituting 23.7% of cases.
A 5 year review of breast lesions in Eastern Nigeria by Anyikam et al,21 reported that 68.8% of
the cases are benign with 44% of them being fibroadenomas with a high prevalence among
nulliparous adolescent females. A 10- year study of breast diseases in Ife22 indicated that 79% of
the cases are benign and 48% of them fibroadenomas. Otu23 conducted a study in Calabar on
benign breast tumours and reported that out of 259 cases, 94% were fibroadenoma and
concluded that benign breast tumours were common in women of child bearing age.
An earlier study carried out at Aminu Kano Teaching Hospital a decade ago by Ochicha et al24
showed that benign breast lesions comprised 73% of all breast lumps with fibrocystic disease
being the commonest accounting for 34% of cases. Fibrocystic disease was also found to be the
commonest benign breast lesion in a study done in Ibadan25 and among Caucasians.2
HISTOLOGICAL TYPES OF BENIGN BREAST TUMOURS
Fibroadenoma-This is the most common benign tumour of the female breast.2 It can occur at
any age during reproductive life, even though most patients are between 15 to 30 years of age. It
is less common in postmenopausal women, is usually single, but in 20% of cases there are
multiple lesions in the same breast or bilaterally.2
Grossly, fibroadenoma is a sharply demarcated, firm mass, usually no more than 3cm in
diameter. Microscopically, fibroadenoma vary in appearance from case to case depending on the
relative amounts of glandular and connective tissue and are divided into intracanalicular and
pericanalicular variants. Morphologic variations in fibroadenoma include hyalinization,
calcification, prominent myxoid changes, haemorrhagic infarction, apocrine metaplasia,
squamous metaplasia and lactational changes.
Epidemiologic studies have concluded that fibroadenoma represents a low long-term risk of
0.1% of cases for breast carcinomas. This risk is increased in women with complex

17
fibroadenomas, ductal hyperplasia, or a family history of breast carcinoma. Sarcomatous
transformation of the stroma of a fibroadenoma is an even rarer phenomenon.26
Tubular adenoma-Tubular adenomas occur mainly in young females. They clinically resemble
fibroadenoma, rarely occur before menarche or after menopause and account for 0.13 to 1.7% of
benign breast lesions.
Grossly, it is usually a solitary, well-circumscribed, tan-yellow, firm tumour. On microscopic
examination, tubular adenomas are separated from the adjacent breast tissue by a pseudocapsule,
and are composed of a proliferation of uniform, small tubular structures with a scant amount of
intervening stroma. Because of their complexity and cellularity, they can be mistaken for
carcinoma.
Benign Phyllodes tumour-This is an uncommon tumour and the patients generally are over the
age of 40 years. Grossly, the typical phyllodes tumour is round, relatively well circumscribed,
firm and may be quite large. The cut surface is solid and gray-white and shows a characteristic
leaf-like pattern. Microscopically, the two key features of phyllodes tumour are stromal
hypercellularity and the presence of benign glandular elements. It is wise to consider most
phyllodes tumours as benign lesions that require adequate excision and local recurrence is said to
occur.
Lipomas- Lipomas consist of encapsulated nodules of mature adipose tissue. Although, true
lipomas occur in the breast, many lesions designated ‘lipoma’ probably represent foci of fatty
breast tissue without a true capsule.
Others-These include fibrocystic change, lactating adenoma, duct papilloma and duct adenoma.
Leiomyoma, neurofibroma, adenomyoepithelioma and granular cell tumour are generally
uncommon and only infrequently encountered in clinical practice.

18
BREAST CANCER
Epidemiology
Incidence Pattern-Breast cancer is reported to be the commonest female malignancy
worldwide. It is seen in about 2% of the total female population and nearly 10% of the female
population aged 65 years and older.27,28 It accounts for about 25 per cent of all female
malignancies and is the fifth most common cause of cancer death. Globally, the incidence of
breast cancer is on the increase and over 1.38 million new cases were diagnosed in 2008 (23% of
all cancers).29
The incidence rates vary substantially around the world and is found to be lowest in less-
developed countries and highest in the more-developed countries. The incidence rate is low in
Mozambique with about 3.9 cases per 100,000, and in Japan with 28.6 new cases annually per
100,000 women while it is 110 new cases annually per 100,000 women in the United States of
America and Northern Europe.30
Breast cancer is the commonest malignancy in North American women. In the United States,
aside from skin cancer, it is the most commonly diagnosed cancer in women, accounting for 32%
of all cancers in women (more than 1 in 4 cancer cases).31
In United Kingdom in 2007, there were 45,972 (75.4/100,000) new cases of breast cancer in
women and 314 new cases in men.32 Heidari et al33 found that according to the latest report by
Cancer Institute of Iran, breast cancer constitutes 25% of all cancers among Iranian women. The
Karachi Cancer Registry, which is the only population based cancer registry in Pakistan, shows
breast cancer to be the most common cancer (34.6% of cancer cases) among females.34
In a study done in South Africa on breast cancer incidence, it was also found out to be the
commonest female malignancy, and between 1993 and 1995, an annual average of 3,785 new
cases of breast cancer were reported with 1,572 deaths.35 The age-standardized incidence rate in
South Africa was 11.3 per 100,000, while that of Harare, Kampala and Gambia were 20.4, 16.4
and 3.4 per 100,000 respectively.36 Bjerregaard and Kung’u37 reported that cancer of the breast
accounted for 5% of all malignancies in Kenya, being second only to cancer of the cervix.

19
In Nigeria recent reports from tertiary centres indicate that breast cancer is rapidly increasing
among the populace and despite the steady rise, it is generally believed that the true prevalence is
under reported, as most of the studies are retrospective and hospital based with propensity for
underestimation and bias.38
It has been reported from the Ibadan cancer registry that the incidence has more than doubled
from 15 per 100,000, to 33 per 100,000 over a 16-year period,39 while Aghadiuno40 reported an
incidence of 63.3% at the same centre in 1979. In Ilorin,41 carcinoma of the breast accounted for
31.8% of breast specimens received from female patients. Oluwole42 in Ile-Ife reported an
incidence of 21% and at the University of Calabar Teaching Hospital, Otu43 reported an
incidence of 26.6%.
A 6-year retrospective study by Ihezue et al44 in Jos showed a hospital incidence of 13 new cases
annually, and 10.6 new cases a year was reported in South Eastern Nigeria by other observers.
The mortality rate in Nigeria is generally high (age standardized mortality rate of 19.6 per
100,000) due to late clinical presentation.44
Sex Distribution- A female preponderance has been reported by several Researchers in various
parts of the world. In developed countries breast cancer is 100 times more common in women
than in men, with male breast cancer accounting for about 1% of all breast cancer cases, 0.2 % of
all male cancers and 0.1% of cancer mortality in men.45 The worldwide variation of male breast
cancer resembles that of breast cancer in women, with higher rates in North America and Europe
and lower rates in Asia.46 Although the epidemiologic literature of female breast cancer is
extensive, little is known about the epidemiology of male breast cancer.
In Canada, about 180 men were estimated to be diagnosed with breast cancer in 2010. The
incidence of breast cancer in men has remained unchanged since 2009 and men with breast
cancer make up a little less than 1% of all cases.47
The female to male ratio of breast cancer in England, Scotland, Northern Ireland and Wales are
120:0.8, 132:0.3, 115:0.1 and 123:0.5 respectively.48
In Africa breast cancer is similarly much more common in females. The incidence rate of male
breast cancer in Kenya,49 Uganda,50 and Zambia51 were 12.5%, 5% and 15% respectively.

20
In Nigeria breast cancer in males is rare and accounts for between 2.2% to 8.0% of all breast
cancers.52,53 Differences in study group and period have been suggested as possible reasons for
such a variation. In Calabar, Nigeria, Otu43 reported a male: female ratio of 1:7 while the
incidence rate of male breast cancer in Zaria,17 Ile-Ife,28 Benin,52 Enugu,53 Ibadan,54 Jos,55 and
Ilorin56 were 5.2%, 1.9%, 2.2%, 8.0%, 3.4%, 8.6% and 6.1% respectively.
Age Distribution- It is evident that the incidence of breast cancer increases dramatically with
age and it is rarely found before the age of 25 years except in familial cases. The median age at
diagnosis of breast cancer in the United States is 64 years and 77% of the cases occur in women
over 50 years of age.2 In other parts of the world, where life expectancy is shorter, the median
age at which breast cancer develops is 10 to 15 years younger.41
In United Kingdom breast cancer risk is also strongly related to age, with 81% of cases occurring
in women aged 50 years and over, and nearly half (48%) of the cases are diagnosed in the 50-69
age group.
African women with breast cancer are more likely to be premenopausal and the incidence peaks
between 35 and 45 years which is almost 10-15 years earlier than the peak incidence for Western
countries.57,58 In Nigeria, there is wide variation in the reported age distribution with a range of
between 16 to 82 years depending on the series.27 The mean age is as low as 36.2 years in
Zaria,17 and 47.2 in Ilorin,41 while the mean age in Lagos,59 Ibadan,60 Eastern Nigeria61 and
Calabar43 are 37.1, 40.5, 44 and 42.7 years respectively.
The peak mean age of male breast cancer in Maiduguri62 was 45 years, while the mean age in
Zaria,63 Ibadan64 and Calabar65 are 55, 54 and 53.1 years respectively.
Laterality-Breast cancer affects the right breast more frequently than the left in Nigeria. This
has been confirmed by studies done in Benin,66 Kano,27 Ilorin41 and other Southern Nigerian
series, even though a left sided predilection has been reported in Zaria.67

21
Aetiology
The exact cause of breast cancer is unknown but it is known to be associated with several risk
factors.2 Its incidence varies substantially according to the presence or absence of these risk
factors. The variable geographical, racial and ethnic differences in parts of the world show that
the major risk factors for the development of breast cancer are hormonal, genetic, age, gender
and environmental factors.68
Genetic factors/Family history: Approximately one-third of women with breast cancer
have one or more first-degree relatives with breast cancer, and about 4 to 9 % are
considered to have hereditary breast cancer.69 Individuals with a first-degree relative with
a history of breast cancer have a substantially increased risk of developing breast cancer
compared to women without a family history.70 Familial breast cancer, however,
accounts for less than 10% of all breast cancers, and BRCA1- and BRCA2-related
familial breast cancers appear to be responsible for only two-thirds to three-quarters of
these cases.
In Nigerian women, a positive family history of breast cancer has not been consistently
demonstrated to be associated with increased breast cancer risk.71 This has been
attributed to lack of medical records and the fact that issues like cancer diagnosis are
rarely discussed, even among relatives, due to existing social norms and fear of
stigmatization.71
Endocrine and reproductive risk factor- Several studies suggest a strong link between
the female reproductive hormone oestrogen and the development of breast cancer. Breast
cancer is predominantly a disease of women and is rarely seen in males. Epidemiologic
studies have demonstrated repeatedly that the absence of full-term pregnancies is a risk
factor for breast cancer.72 Early onset of menarche and late onset of menopause have
been associated with an increased risk of breast cancer.73
In Nigerian women, age at first full-term pregnancy and breastfeeding have also been
shown to be associated with increased risk of breast cancer. Women in Nigeria tend to
have children at an earlier age, have more children and breastfeed their children longer
than women in Western countries. These behaviours might be responsible for the lower
incidence of breast cancer in Nigeria.74

22
Ethnicity-Different ethnic groups have widely divergent incidence rates of breast cancer.
Asian-Pacific groups have a much lower incidence of breast cancer, whereas groups of
Western European origin have the highest incidence.31 Studies have suggested that
Jewish women, especially those with a family history of breast cancer in a first-degree
relative, have a risk of breast cancer almost four times that of women in other ethnic
groups.75
Women in Sub Saharan Africa were found to have a low incidence of breast cancer. This
was partly explained by a large protective reproductive history, including late menarche,
early menopause, high parity and prolonged breast feeding. Limited financial resources
lead to suboptimal cancer data collection, delayed diagnosis and treatment causing high
mortality in many African breast cancer patients.76
Other risk factors-These include presence of some benign breast diseases like atypical
epithelial hyperplasia and sclerosing adenosis, dietary fat intake, exposure to ionizing
radiation, obesity, alcohol consumption, functional ovarian tumours and increased
exposure or use of tobacco products.

23
HISTOLOGICAL TYPES OF DUCTAL CARCINOMA IN SITU
Lobular carcinoma in situ (LCIS)-Lobular carcinoma in situ is mostly an incidental finding in a
biopsy performed for another reason. It is bilateral in 20% to 40% of women when both breasts
are biopsied, is more common in young women with 80% to 90% of cases occurring prior to
menopause. It is also generally uncommon being found in about 1% to 6% of all breast
carcinomas.
It is not associated with any grossly recognizable features. Microscopically, the lesion is located
within the terminal duct lobular unit and the lobular architecture is maintained. The acini of one
or more lobules are expanded to varying degrees by a monomorphic proliferation of loosely
cohesive, usually small cells, with uniform round nuclei, indistinct nucleoli, uniform chromatin
and indistinct cell margins with sparse cytoplasm. Necrosis and calcification are uncommon and
mitoses are infrequent.
The relative risk for subsequent development of invasive carcinoma among patients with LCIS
ranges from 6.9 to 12 times that expected in women without LCIS.
Ductal carcinoma in situ (DCIS) - Is also called Intraductal carcinoma and is characterised by
increased epithelial proliferation, with moderate to marked cellular atypia and an inherent but not
necessarily obligate tendency for progression to invasive breast cancer. DCIS is considered a
precursor lesion with a relative risk of 8-11 for the development of invasive breast cancer.
A striking increase in the detection of DCIS has been noted with the introduction of widespread
screening mammography and increasing awareness of breast cancer in the general population.

24
HISTOLOGICAL TYPES OF INVASIVE BREAST CANCER
Invasive Ductal Carcinoma, No Special Type (NST)
Invasive ductal carcinoma of no special type comprises the largest group of invasive breast
cancers. It is a heterogeneous group of tumours that fail to exhibit sufficient characteristics to
achieve classification as a specific histological type, such as lobular or tubular carcinoma.
It is the most common ‘type’ of invasive carcinoma of the breast comprising between 40% and
75% in published series.77 It accounted for 80.6% of the histopathological types in an earlier
study done in AKTH.27 Though the proportions are different Ihezue44 and Atoyebi59 reported
91% and 94% respectively.
The classical macroscopic appearance of invasive ductal carcinoma is that of a scirrhous
carcinoma, characterised by a firm, sometimes rock-hard mass that on cut section has a grey-
white, gritty surface which is due to the desmoplastic tumour stroma. Although most invasive
ductal cancers have a stellate or speculated contour with irregular margins, some lesions have
rounded, pushing margins and are grossly well circumscribed, and rarely they lack a significant
tumour stroma and are indistinct.
Architecturally the tumour cells may be arranged in cords, clusters and trabeculae whilst some
tumours are characterised by a predominantly solid or syncytial infiltrative pattern with little
associated stroma. The carcinoma cells also have a variable appearance. The cytoplasm is often
abundant and eosinophilic. Nuclei may be regular, uniform or highly pleomorphic with
prominent, often multiple, nucleoli, mitotic activity may be virtually absent or extensive. In up to
80% of cases foci of associated ductal carcinoma in situ will be present.
Prognosis is influenced profoundly by the classical prognostic variables of histological grade,
tumour size, lymph node status and vascular invasion, in addition to predictors of therapeutic
response such as oestrogen receptor and ERBB2 status.
Invasive lobular carcinoma
Invasive lobular carcinomas constitute the second most frequent type of invasive breast cancer.
In most series, these tumours account for approximately 5-10% of invasive breast carcinomas.78
Invasive lobular carcinomas appear to be more often bilateral than other types of invasive breast
cancer, although the reported range of bilaterality has been broad (6-47%).79 Approximately 70-
80% of cases of invasive lobular carcinoma contain foci of lobular carcinoma in situ.

25
Grossly, invasive lobular carcinoma frequently present as irregular and poorly delimited tumours
which can be difficult to define macroscopically because of the diffuse growth pattern of the cell
infiltrate. Microscopically the classical variant of invasive lobular carcinoma is predominantly
characterised by the presence of small and relatively uniform tumour cells growing singly, in an
Indian file pattern, and in a concentric (“pagetoid”) fashion around lobules. Gland formation is
not a feature of classic invasive carcinoma. The dense fibrous stroma is usually abundant and
mitosis is typically infrequent. In addition to this classical pattern other variants include solid,
alveolar and pleomorphic lobular types.
The classical variant of invasive lobular carcinoma is associated with a more favourable
prognosis than invasive ductal carcinoma.80
Medullary carcinoma
Medullary carcinomas account for less than 5-7% of all invasive breast cancers.81 The mean age
of women with medullary cancer ranges from 45 to 52 years and is said to be particularly
common in Japanese women. It is also said to be particularly common in carriers of BRCA1
mutations.
Grossly, these lesions are well circumscribed, soft, tan-brown to gray tumours. Areas of
haemorrhage, necrosis, or cystic degeneration may be present. It can be mistaken clinically and
grossly for a fibroadenoma, but it lacks the trabeculation or whorling of the latter.
Microscopically, the borders are always of the “pushing” type. Histological criteria required for
the diagnosis of medullary carcinoma include: (1) syncytial growth pattern of the tumour cells in
more than 75% of the tumour; (2) moderate to marked diffuse admixed lymphoplasmacytic
infiltrates; (3) microscopic circumscription; (4) moderate to marked nuclear pleomorphism; (5)
absence of glandular differentiation.

26
Other Histological Types
Tubular carcinoma
This is a special type of cancer that is typically associated with limited metastatic potential and
an excellent prognosis. The mean age at presentation for patients with tubular carcinoma is in the
early sixth decade (range 23-89 years). In pure tubular carcinoma, 90% of the tumour is
characterised by a proliferation of well formed glands or tubules formed by a single layer of
epithelial cells without a myoepithelial component.
Mucinous carcinoma
This is also called colloid carcinoma and is another special type of cancer that is associated with
a relatively favourable prognosis. Most studies have indicated that less than 5% of invasive
breast carcinomas have a mucinous component and of these less than half represent pure
mucinous carcinomas. The mean age at presentation for patients with mucinous carcinoma is in
the seventh decade in most studies.82 The hallmark of mucinous carcinoma is extracellular mucin
production. However, the extent of extracellular mucin varies from tumour to tumour. This
characteristic histology should comprise at least 90% of the tumour to qualify for the diagnosis
of mucinous carcinoma.
Invasive cribriform carcinoma
Invasive cribriform carcinoma is a well differentiated cancer that shares some morphologic
features with tubular carcinoma and is also associated with a favourable prognosis.
Approximately 5-6% of invasive breast cancers show at least a partial invasive cribriform
component. The majority of patients present in the sixth decade, and they are characterised by
tumour cells that invade the stroma in a cribriform or fenestrated growth pattern with low or
intermediate grade nuclear features. Significant nuclear pleomorphism is generally not present.
Invasive papillary carcinoma
Invasive papillary carcinomas comprise from <1% to 2% of invasive breast cancers and are
characterised by a relatively good prognosis. They are diagnosed predominantly in
postmenopausal patients.

27
Invasive papillary carcinoma is grossly circumscribed in most of the cases. Microscopically,
invasive papillary carcinomas are characteristically circumscribed, the cells typically show
amphophilic cytoplasm but may have apocrine features and also may exhibit apical ‘snouting’ of
cytoplasm similar to tubular carcinoma. Tumour stroma is not abundant in most cases and
occasional cases show prominent extracellular mucin production. Calcifications are commonly
seen histologically.
Metaplastic carcinoma
Metaplastic carcinomas are uncommon lesions, representing less than 5% of all breast cancers.
Grossly, it is not distinctive and these tumours can either be well circumscribed or show an
indistinct or irregular borders. Microscopically, most reports divide metaplastic carcinomas into
two broad categories: those that show squamous differentiation and those that feature
heterologous elements, such as cartilage, bone, muscle, adipose tissue, vascular elements, and
even melanocytes, among others.
Secretory carcinoma
Secretory carcinoma is an exceedingly rare form of invasive carcinoma that accounts for <0.01%
of all breast cancer. Although secretory carcinomas occur over a wide age range, with a median
age in the third decade, they account for a substantial number of primary breast cancers
diagnosed in childhood and have therefore also been referred to as ‘juvenile’ carcinomas. The
majority of reported cases have been in females but rare cases have occurred in males, and in
addition no increased incidence of a positive family history of breast cancer has been reported in
patients with secretory carcinoma.
Secretory carcinomas are typically grossly circumscribed. Histologically, these lesions are
characterised by a proliferation of relatively low-grade tumour cells that form glandular
structures and microcystic spaces filled with a vacuolated, lightly eosinophilic secretion.

28
SARCOMAS
Sarcomas are very uncommon cancers of the breast, representing about 0.5% of the mammary
tumours.83 They include all tumours originating in the mesenchymal stroma of the mammary
gland. Most lesions that resemble sarcomas are in fact metaplastic carcinomas, which should be
excluded before one diagnoses a mammary sarcoma. The most important sarcoma that occurs
primarily in the breast is angiosarcoma.9
LYMPHOMAS
Different types of lymphomas may be observed as primary tumours of the breast. Primary breast
lymphoma may appear at any age, but the majority of patients are postmenopausal women and it
is bilateral in approximately 10% of cases. The disease is exceedingly rare in men.
Microscopically, the majority of primary breast lymphomas are diffuse large B cell lymphomas,
according to the most recent WHO classification.9 A minor proportion of primary lymphomas of
the breast are Burkitt lymphoma, extranodular marginal-zone B cell lymphoma of mucosa
associated lymphoid tissue (MALT) type, follicular lymphoma, lymphoblastic lymphoma of
either B or T type and, extremely rarely, T-cell lymphomas of variable subtypes by the current
WHO classification.
EXTRAMAMMARY MALIGNANCIES METASTATIC TO THE BREAST
Secondary tumour deposits in the breast may emanate from the contralateral breast or from
virtually any nonmammary site. Metastases to the breast from nonmammary malignancies
comprise 1.2% of all malignancies diagnosed in the breast.84 Nonmammary malignancies can
mimic the features of usual or unusual types of primary breast tumour, so it can be very difficult
to distinguish between the two in a subset of cases, particularly when there is no history of a
prior nonmammary malignancy.
Metastatic tumours to the breast have a variable gross appearance, depending on the type of
metastasis. The histologic appearance of these neoplasms is related to the site of origin of the
primary tumour. Metastatic lesions most frequently seen in the breast include malignant
melanoma, lung carcinoma, prostate carcinoma and carcinoid tumours from a variety of primary
sites. Any carcinoma, sarcoma, or haematopoietic malignancy can involve the breast.85

29
Histological Grading of invasive breast carcinoma
Invasive ductal carcinomas and all other invasive tumours are routinely graded based on an
assessment of tubule/gland formation, nuclear pleomorphism and mitotic counts.
Many studies have demonstrated a significant association between histological grade and
survival in invasive carcinoma. It is now recognized as a powerful prognostic factor and should
be included as a component of the minimum data set for histological reporting of breast cancer.
Assessment of histological grade has become more objective with Nottingham histologic grading
system.86
Three tumour characteristics are evaluated; tubule formation as an expression of glandular
differentiation, nuclear pleomorphism and mitotic counts. A numerical scoring system of 1-3 is
used to ensure that each factor is assessed individually. When evaluating tubules and glandular
acini only structures exhibiting clear central lumina are counted; cut off points of 75% and 10%
of glandular/tumour area are used to allocate the score.
Nuclear pleomorphism is assessed by reference to the regularity of nuclear size and shape of
normal epithelial cells in adjacent breast tissue. Increasing irregularity of nuclear outlines and the
number and size of nucleoli are useful additional features in allocating scores for pleomorphism.
Evaluation of mitotic figures requires care and observers must count only defined mitotic figures.
The total number of mitoses per 10 high power fields is counted and the field selection is by
random through the chosen area. Only fields with a representative tumour cell burden should be
assessed.
The three values are added together to produce scores of 3 to 9, to which the grade is assigned as
follows:
Grade 1- well differentiated: 3-5 points
Grade 2- moderately differentiated: 6-7 points
Grade 3- poorly differentiated: 8-9 points

30
NOTTINGHAM HISTOLOGIC GRADING SYSTEM OF BREAST CANCER86
Components of the grade Score
Tubules
>75% of tumour composed of tubules 1 point
10-75% of tumour composed of tubules 2 points
<10% of tumour composed of tubules 3 points
Nuclear grade
Nuclei small and uniform 1 point
Moderate variation in nuclear size/shape 2 points
Marked nuclear pleomorphism 3 points
Mitotic rate
Dependent on microscope field area 1-3 points

31
PROGNOSTIC FACTORS
The prognosis for primary breast cancer varies considerably from patient to patient. While some
women have the same life expectancy as women without breast cancer, others have only 13%
chance of being alive in 5 years. Except for the few women (<10%) with distant metastases at
presentation or with inflammatory carcinoma, prognosis is determined by the pathologic
examination of the primary carcinoma and the axillary lymph nodes. This information is
important for counseling patients about the likely outcome of their disease and for selecting
appropriate treatment modalities.
MAJOR PROGNOSTIC FACTORS.
The major prognostic factors are the strongest predictors of death from breast cancer. These
include:
1. Axillary lymph node metastasis- Involvement of the ipsilateral axillary lymph node is
still the most reliable and reproducible prognostic indicator for primary breast cancer.87 In
general, 50 to 70% of patients with positive lymph nodes have a relapse, whereas only 20 to 45%
of patients with all lymph nodes negative for metastatic disease have a relapse after locoregional
treatment only. Although axillary lymph node status is still the most powerful prognostic
indicator, 15 to 45% of patients whose lymph nodes do not contain metastases still experience a
recurrence and die.
2. Distant metastases- Once distant metastases are present, cure is unlikely, although long-
term remissions and palliation can be achieved, especially in women with hormonally responsive
tumours. The tumour type influences the timing and location of metastases.88
3. Tumour size- In addition to being a determinant for optimal local therapy, tumour size
has prognostic significance in the determination of additional therapy. As the size of the tumour
increases, the risk of recurrence or metastasis also increases for both lymph node- negative and
node-positive tumours. Approximately 25 to 30% of patients with negative lymph nodes and a
primary tumour less than 2cm in diameter will experience a recurrence within 20 years of follow
up. Patients with tumours 1 cm or less in diameter have an excellent prognosis, with fewer than
15% recurring at 10 years.
4. Locally advanced disease- Carcinomas invading into skin or skeletal muscle are usually
large and may be difficult to treat surgically. With increased awareness of breast cancer

32
detection, such cases have fortunately decreased in frequency and are now rare at initial
presentation in developed Countries. Unfortunately many patients in developing Countries are
still seen with locally advanced disease.
5. Inflammatory carcinoma- Breast cancer presenting with breast swelling and skin
thickening due to dermal lymphatic involvement has a particularly poor prognosis. The 3-year
survival rate is only 3% to 10%.
MINOR PROGNOSTIC FACTORS
1. Histological subtype- Several histological variables have been reported to have
prognostic significance. Breast cancers with favourable prognosis include tubular carcinoma,
mucinous or colloid carcinoma, papillary carcinoma, and all noninvasive breast cancers. These
cancers have substantially better prognoses, especially when found in a node-negative stage.
2. Histological grade- The most commonly used grading system, the Nottingham
histological score (also referred to as Scarff-Bloom-Richardson), combines nuclear grade, tubule
formation, and mitotic rate to classify invasive carcinomas into three groups that are highly
correlated with survival.
3. Oestrogen and progesterone receptors- Currently assays use immunohistochemistry to
detect nuclear hormone receptors, a finding that is correlated with a better outcome and is an
important predictor of response to hormonal therapy. Eighty percent of carcinomas that are
oestrogen(ER) and progesterone (PR) positive respond to hormonal manipulation, whereas only
about 40% of those with either ER or PR alone respond. ER positive cancers are less likely to
respond to chemotherapy. Cancers that fail to express either ER or PR have a less than 10%
likelihood of responding to hormonal therapy but are more likely to respond to chemotherapy.
4. HER2/neu- Overexpression of HER2/neu is a very good predictor of response to
Herceptin, but not a very good predictor or response to chemotherapy or overall survival. In
terms of relationship with tumour types, HER2/neu overexpression is found in nearly all cases of
high-grade ductal carcinoma in situ, in 20% to 30% of invasive ductal carcinomas, and in a
smaller percentage of invasive lobular carcinomas.

33
5. Lymphovascular invasion- Tumour cells are present within vascular spaces in about
half of all invasive carcinomas. This is strongly associated with the presence of lymph node
metastasis. It is a poor prognostic factor for overall survival in women without lymph node
metastases and a risk factor for local recurrence.
6. Proliferative rate- Proliferation can be measured by mitotic counts, by
immunohistochemical detection of cellular proteins produced during the cell cycle, by flow
cytometry, or by thymidine labeling index. Carcinomas with high proliferation rates have a
poorer prognosis but may respond better to chemotherapy.
7. DNA content- The amount of DNA per tumour cell can be determined by flow-
cytometric analysis or by image analysis of tissue sections. Tumours with a DNA index of 1
have the same total amount of DNA as normal diploid cells, although marked karyotypic
changes may be present.

34
CHAPTER THREE
MATERIALS AND METHODS
This is a retrospective study of all breast tumours that were histologically diagnosed in the
pathology department of Aminu Kano Teaching Hospital over a ten-year period, from 1st
January, 2001 to 31st December, 2010.
AKTH is the major tertiary health institution offering histopathology services to the entire Kano
state as well as parts of the neighbouring states of Jigawa, Katsina and Bauchi. Kano state is in
North-western Nigeria and has a population of over 9 million people (2006 census).
The laboratory request forms and duplicate copies of histology reports of all cases were retrieved
and relevant clinical information such as age, sex, and laterality were extracted.
The corresponding slides were also retrieved and in few cases of faded and missing slides, fresh
sections were cut from archival paraffin tissue blocks and routinely stained with Haematoxylin
and Eosin (H&E). Special stains including periodic acid-schiff and mucicarmine stains were
deployed where necessary.
The slides were then reviewed by me and then with the supervising Consultant Pathologists. The
tumours were then classified into the histogenetic groups according to the WHO International
Classification of breast tumours,9 and the Nottingham system was used for histological grading.86
The results were then analyzed and presented using relative frequency tables and pie charts with
photomicrographs of some of the tumours taken.

35
INCLUSION CRITERIA
1. All histologically diagnosed benign and malignant breast tumours through incision and
core needle biopsies, lumpectomies and mastectomies. In mastectomy patients who had
previous incision biopsies, only the mastectomy result was used.
2. Fibrocytic changes.
3. Gynaecomastia
EXCLUSION CRITERIA
1. All cases where both the slides and tissue blocks were missing were excluded from the
study.
2. All histologically diagnosed inflammatory breast diseases, proliferative breast disorders
and duct ectasia.
LIMITATIONS
1. Review of gross specimens and re-sampling of some cases where indicated was not
possible because most of the original specimens have been discarded.
2. Unavailability of immunohistochemistry for proper categorization of breast cancer cases.
Immunohistochemistry was only recently introduced in our laboratory and was not
available for most of the study period (2001-2010). Immunohistochemistry on archival
paraffin blocks was not practical because of the prohibitive cost, as well as the fact that
strict time guidelines on the formalin fixation for breast immunohistochemistry could not
be guaranteed for archival specimens.

36
CHAPTER FOUR
RESULTS
A total of 2470 surgical breast specimens were received in the department of Histopathology,
AKTH Kano over the ten year period (2001 – 2010) covered by this retrospective study. Out of
this number, 1566 (63% of the cases) were diagnosed as breast tumours (benign and malignant),
897 were found on histological examination to be inflammatory and intraepithelial breast lesions
and 7 cases had inconclusive diagnoses. Of the 1566 breast tumours, 1035 were benign
representing 66.3% and 531 (33.7%) were malignant with a benign to malignant ratio of
approximately 2:1. The classification of breast tumours into benign and malignant histologic
groups is shown in Tables 1 and 2 respectively.
Benign breast tumours accounted for 8.3% of all the benign tumours received in the department
during the period under review. The age range of the benign breast tumours was 13 to 63 years
with a mean of 29 years. The benign tumours were predominantly seen in the 21 to 30 years age
group, and the frequency peaked in the 3rd decade with 432 cases (41.7%), while no cases was
seen in the 1st decade and only four in the 7th decade as demonstrated in table 3. Fibroadenoma
was the most common benign tumour, accounting for 487(47.1%) of the benign cases seen. It
also represented 31.1% of all breast tumour cases seen, making it the most common histologic
type of breast tumour in the study. Majority, 275 (56.5%) of cases of fibroadenoma were seen in
the 21 to 30 year age group (Table 3).
Fibrocystic change was the second most common benign lesion seen, accounting for 263
(25.4%) of the benign cases. The frequency peaked in the 4th decade with 127 (48.3%) cases and
no case was recorded in the 1st and 8th decades. Other important histological types of benign
breast tumours which include Lactating adenoma, Tubular adenoma and Benign phyllodes
tumour accounted for 58 (5.6%), 62 (6.0%) and 50 (4.8%) of the benign cases respectively. The
least frequently diagnosed benign breast tumours were granular cell tumour, adenomyoepithelial
adenosis, lipoma and schwanoma each accounting for 9 (0.9%), 8(0.8%), 7(0.7%) and 5(0.5%)
cases respectively (Table1).
Gynaecomastia, which was the only benign tumour in males, constituted, 14(1.4%) of the benign
breast tumours.

37
Laterality was documented in 984 benign cases, amongst which 541 (55.0%) were right sided,
414 (42.1%) were left sided and 30 (2.9%) were bilateral.
Fibroadenoma accounted for 463 (47.1%) cases of all the benign breast tumours with laterality,
and was observed to occur more on the right breast (64%) than the left (31%). The same right-
sided preponderance was found in lactating adenoma (59%), benign phyllodes (55%) and
gynaecomastia (57%). Fibrocystic change, sclerosing adenosis and tubular adenoma were
observed to have left-sided predominance occurring in 52%, 62% and 80% cases respectively.
Fibroadenoma was the most frequent benign breast tumour with bilaterality, accounting for 23
(80%) out of the 30 bilateral benign breast cases. Other benign tumours with least frequent
bilateral cases are fibrocystic change (6.7%), lactating adenoma (3.3%), tubular adenoma (6.7%)
and gynaecomastia (3.3%).
Malignant breast tumours accounted for 11.9% overall of all malignant tumours with a wide age
range of 15 to 80 years and a mean age of 42 years.
A total of 531 malignant breast tumours were diagnosed, 35 (6.6%) cases in males and 496
(93.4%) cases in females giving a female to male ratio of 14.2:1 (Table 5).
Invasive ductal carcinoma (NST) was also the most common malignant breast tumour
accounting for 316(59.5%) cases as shown in Table 2. Twenty one (6.6%) cases were in males
and 295 (93.4%) cases were in females with a female to male ratio of 14.0:1. The 4th-6th decades
of life had the highest frequency of 235(74.4%) cases, while the lowest frequency of 3 (0.9%)
cases occurred in the 2nd decade.
Medullary carcinoma was the second most common malignant breast tumour accounting for 61
(11.5%) cases, all of which were diagnosed in females. The peak age range for this tumour was
in the 4th and 5th decades accounting together for 36(59.0%) cases. One (1.6%) case occurred in
the 8th decade.
Of the 37(6.9%) cases of Invasive lobular carcinoma, all were found in females and the highest
frequency of 13 (35.1%) cases was recorded in the 4th decade (Table 4).

38
Thirty seven cases of Invasive papillary carcinoma were also diagnosed representing 6.9% of all
breast malignancies seen. Of this number 4, (10.8%) cases were seen in males and 33 (89.2%)
cases in females, which represent 11.2% and 6.7% of all the malignant breast tumours seen in
males and females respectively. The female to male ratio was 8.3:1. The 31 - 40 year age group
had the highest frequency with no case recorded below the age of 21 years. The least frequently
diagnosed malignant breast tumours are Invasive cribriform carcinoma, Neuroendocrine
carcinoma, Sebaceous carcinoma and Burkitt lymphoma each accounting for a single case
(0.2%), as depicted in Table 2. No case of these tumours was recorded in males. The single case
of Burkitt Lymphoma occurred in the 2nd decade.
Of the 488 cases of malignant breast tumours with laterality, 319(65.4%) were right sided, 167
(34.2%) were left sided and 2 (0.4%) cases bilateral. Invasive ductal carcinoma(NST)
accounted for 301 of the cases, 193 (64%) cases were right sided, 108 (36%) cases left sided
with no case of bilateral involvement. Invasive lobular carcinoma demonstrated 33 cases with
laterality, 25 (76%) right sided, 7 (21%) left sided and 1(3%) case was bilateral. Laterality was
recorded in 58 cases of medullary carcinoma, 53 (91%) right sided, 5 (9%) left sided and no case
was bilateral. Invasive papillary carcinoma showed 34 cases with laterality, 17 (50%) right sided,
16 (47%) left sided and 1 (3%) case bilateral.
Thirteen cases of Apocrine carcinoma were documented with laterality, 6 (46%) cases right
sided, 7 (54%) cases left sided and no bilateral case documented. Other malignant breast tumours
showed 49 cases with laterality 25 (51%) cases right sided, 24 (49%) cases left sided and no
bilateral case.
The malignant breast tumours were graded according to Nottingham grading system. Two
hundred and thirty seven (44.6%) cases were classified as grade 1 (Table 8). Grade 2 tumours
accounted for 133 (25.0%) cases and grade 3 tumours are composed of 161 (30.4%) cases.

39
TABLE 1
Histopathologic Distribution of Benign Breast Tumours
TUMOUR TYPE FREQUENCY %
Fibroadenoma 487 47.1
Fibrocystic change
Tubular adenoma
263
62
25.4
6.0
Lactating adenoma
Benign phyllodes
58
50
5.6
4.8
Sclerosing adenoma
Blunt duct adenoma
34
26
3.3
2.5
Gynaecomastia
Ductal papilloma
Granular cell tumour
14
12
9
1.4
1.0
0.9
Adenomyoepithelial adenosis 8 0.8
Lipoma 7 0.7
Schwannoma 5 0.5
TOTAL 1035 100.0
TABLE 2
Histopathologic Distribution of Malignant Breast Tumours
TUMOUR TYPE FREQUENCY %
Invasive ductal carcinoma 316 59.5
Medullary carcinoma 61 11.5
Invasive lobular carcinoma 37 6.9
Invasive papillary carcinoma 37 6.9
Apocrine carcinoma 19 3.6
Metaplastic carcinoma 15 2.8
Mucinous carcinoma 14 2.6
Ductal carcinoma in situ 9 1.8
Malignant phyllodes tumour 7 1.3
Secretory carcinoma 5 0.9
Adenoid cystic carcinoma 4 0.8
Tubular carcinoma 3 0.6
Sebaceous carcinoma 1 0.2
Invasive cribriform carcinoma 1 0.2
Neuroendocrine carcinoma
Burkitt lymphoma
1
1
0.2
0.2
TOTAL 531 100.0

40
KEY: FA – Fibroadenoma, CYS – Fibrocystic change, TA- Tubular adenoma, LA – Lactating
adenoma, BP – Benign phyllodes, SA – Sclerosing adenosis, BDA – Blunt duct adenosis, GYN-
Gynaecomastia, DP – Ductal papillomas.
TABLE 3
Age Distribution of Benign Breast Tumours according to Histopathological Subtype
AGE
TUMOUR TYPE 0-
10
11-
20
21 -
30
31 –
40
41 -
50
51-
60
61 -
70
71-
80
unspecified TOTAL
(%)
FA - 148 275 54 2 1 - - 7 487(47.1)
CYS - 7 44 127 65 12 3 - 5 263(25.4)
TA - 21 12 11 10 4 - - 4 62(5.9)
LA - 8 43 5 - - - - 2 58(5.6)
BP - 5 22 9 11 1 - - 2 50(4.8)
SA - 2 13 17 1 - - - 1 34(3.3)
BDA - 5 11 9 1 - - - - 26(2.5)
GYN - - - 3 9 2 - - - 14(1.4)
DP - 2 2 3 - 2 - - 3 12(1.2)
OTHERS - 4 10 3 5 4 1 - 2 29(2.8)
TOTAL 0 202 432 241 104 26 4 0 26 1035(100.)

41
KEY: IDC - Invasive ductal carcinoma(NST), MC – Medullary carcinoma, ILC -Invasive
lobular carcinoma, IPC – Invasive papillary carcinoma, AC- Apocrine carcinoma, MET-
Metaplastic carcinoma, MUC – Mucinous carcinoma.
TABLE 4
Age Distribution of Malignant Breast Tumours according to Histopathological Subtype
AGE
TUMOUR
TYPE
0-
10
11-
20
21 -
30
31 -
40
41 -
50
51 -
60
61-
70
71-
80
unspecified TOTAL
(%)
IDC - 3 28 92 74 69 40 6 4 316(59.5)
MC - - 10 19 17 9 3 1 2 61(11.5)
ILC - - 4 13 10 3 4 2 1 37(6.9)
IPC - - 3 12 10 6 3 2 1 37(6.9)
AC - - - 4 3 10 1 - 1 19(3.6)
MET - - 1 2 3 7 - 1 1 15(2.8)
MUC - - 3 1 4 2 3 1 - 14(2.6)
OTHERS - 1 4 10 8 5 1 2 1 32(6.0)
TOTAL 0 4 53 153 129 111 55 15 11 531(100.0)

42
TABLE 5
Sex Distribution of Malignant Breast Tumours according to Histological Type
SEX
TUMOUR TYPE MALES(%) FEMALES(%) TOTAL(%)
IDC 21(7%) 295(93%) 316(100%)
MC - 61(100%) 61(100%)
ILC - 37(89%) 37(100%)
IPC 4(11%) 33(100%) 37(100%)
AC 3(16%) 16(84%) 19(100%)
MET 1(7%) 14(93%) 15(100%)
MUC 1(7%) 13(93%) 14(100%)
DCIS 1(11%) 8(89%) 9(100%)
MPT - 7(100%) 7(100%)
SEC - 5(100%) 5(100%)
ACC 1(25%) 3(75%) 4(100%)
TC - 3(100%) 3(100%)
SEB - 1(100%) 1(100%)
ICC - 1(100%) 1(100%)
NEC - 1(100%) 1(100%)
BL - 1(100%) 1(100%)
TOTAL(%) 35 (6.6%) 496 (93.4%) 531(100.0%)
KEY: IDC - Invasive ductal carcinoma, ILC -Invasive lobular carcinoma, TC –
Tubular carcinoma, ICC - Invasive cribriform carcinoma, MC - Medullary carcinoma, MUC -
Mucinous carcinoma, NEC – Neuroendocrine carcinoma, IPC – Invasive papillary carcinoma,
AC – Apocrine carcinoma, MET – Metaplastic carcinoma, SEC – Secretory carcinoma, ACC –
Adenoid cystic carcinoma, SEB – Sebaceous carcinoma, DCIS - Ductal carcinoma in situ, MPT -
Malignant phyllodes tumour, BL – Burkitt lymphoma.

43
TABLE 6
Laterality of common Benign Breast Tumours
TUMOUR
TYPE
No. with
laterality
Right
sided(%)
Left
sided(%)
Bilateral(%)
Total
FA 463 296(64%) 144(31%) 23(5%) 463(100%)
CYS 255 120(47%) 133(52%) 2(1%) 255(100%)
TA 59 10(17%) 47(80%) 2(3%) 59(100%)
LA 51 30(59%) 20(39%) 1(2%) 51(100%)
BP
SA
48
30
26(55%)
11(38%)
22(45%)
19(62%)
-
-
48(100%)
30(100%)
GYN 14 8(57%) 5(36%) 1(7%) 14(100%)
OTHERS 64 40(62%) 24(38%) - 64(100%)
TOTAL 984 541(55.0%) 414(42.1%) 30 (2.9%) 984(100%)
KEY: FA – Fibroadenoma, CYS – Fibrocystic change, LA – Lactating adenoma, SA –
Sclerosing adenosis, TA- Tubular adenoma, BP – Benign Phyllodes, GYN –
Gynaecomastia
TABLE 7
Laterality of common Malignant Breast Tumours
TUMOUR
TYPE
No. with
laterality
Right
sided(%)
Left
sided(%)
Bilateral(%)
Total
IDC 301 193(64%) 108(36%) - 301(100%)
MC 58 53(91%) 5(9%) - 58(100%)
IPC 34 17(50%) 16(47%) 1(3%) 34(100%)
ILC 33 25(76%) 7(21%) 1(3%) 33(100%)
AC 13 6(46%) 7(54%) - 13(100%)
OTHERS 49 25(51%) 24(49%) - 49(100%)
TOTAL 488 319(65.4%) 167(34.2%) 2(0.4%) 488(100%)

44
TABLE 8
Nottingham Grading of Breast Cancer according to Histological Types
GRADES
TUMOUR TYPE 1 2 3 TOTAL
IDC 151 (47.8%) 64 (20.3%) 101 (31.9%) 316
MC 26 (42.6%) 24 (39.3%) 11 (18.1%) 61
ILC 18 (48.6%) 11 (29.7%) 8 (21.7%) 37
IPC 15 (40.5%) 10 (27.0%) 12 (32.5%) 37
AC 9 (47.4%) 6 (31.6%) 4 (21.0%) 19
MET 6 (40.0%) 7 (46.7%) 2 (13.3%) 15
MUC 6 (42.9%) 3 (21.4%) 5 (35.7%) 14
DCIS 1 (11.1%) 2 (22.2%) 6 (66.7%) 9
MPT - - 3 (42.9%) 4 (57.1%) 7
SEC 2 (40.0%) 1 (20.0%) 2 (40.0%) 5
ACC - - 1 (25.0%) 3 (75.0%) 4
TC 2 (66.7%) - - 1 (33.3%) 3
ICC 1 (100.0%) - - - - 1
NEC - 1 (100.0%) - 1
TOTAL 237 (59.5%) 133 (33.4%) 28 (7.1%) 398(100.0%)
KEY: IDC - Invasive ductal carcinoma(NST), ILC -Invasive lobular carcinoma, TC -Tubular
carcinoma, ICC - Invasive cribriform carcinoma, MC - Medullary carcinoma, MUC – Mucinous
carcinoma, NEC – Neuroendocrine carcinoma, IPC – Invasive papillary carcinoma, AC –
Apocrine carcinoma, MET – Metaplastic carcinoma, SEC – Secretory carcinoma, ACC –
Adenoid cystic carcinoma, DCIS - Ductal carcinoma in situ, MPT - Malignant phyllodes tumour.
45
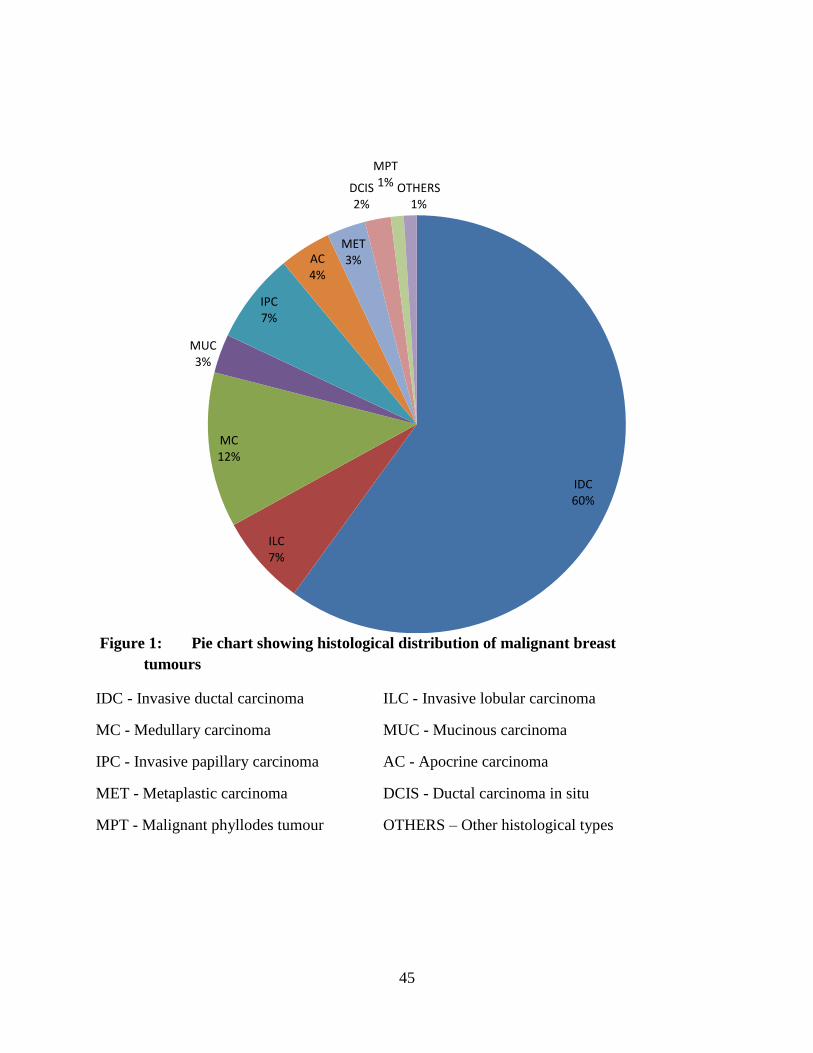
Figure 1: Pie chart showing histological distribution of malignant breast
tumours
IDC - Invasive ductal carcinoma ILC - Invasive lobular carcinoma
MC - Medullary carcinoma MUC - Mucinous carcinoma
IPC - Invasive papillary carcinoma AC - Apocrine carcinoma
MET - Metaplastic carcinoma DCIS - Ductal carcinoma in situ
MPT - Malignant phyllodes tumour OTHERS – Other histological types
IDC60%
ILC7%
MC12%
MUC3%
IPC7%
AC4%
MET3%
DCIS2%
MPT1% OTHERS
1%

46
Figure 2: Fibroadenoma, intracanalicular type showing compressed ducts disposed in a
curvilinear pattern within a fibromyxoid stroma… (H&E)X20
Figure 3: Fibrocystic change showing dilated cysts lined by cells altered by apocrine
metaplasia….. (H&E)X20.

47
Figure 4: Invasive ductal carcinoma (NST) showing nests of malignant ductal epithelial
cells and comedonecrosis within a desmoplastic stroma….. (H&E)X20.
Figure 5: Medullary carcinoma showing syncytial sheets of malignant cells
andLymphoplasmacytic infiltrates within the tumour….(H&E)X20.

48
Figure 6: Adenoid cystic carcinoma showing tumour cells in a cribriform pattern….
(H&E)X20.
Figure 7: Invasive lobular carcinoma showing single regular small malignant cells
arranged in an Indian file pattern… (H&E)X20.

49
Figure 8: Burkitt lymphoma showing sheets of uniform medium size malignant lymphoid
cells, tingible body macrophages and several mitoses…. (H&E)X20.
50
CHAPTER FIVE
DISCUSSION
Tumours of the breast are common and occur worldwide.2 The incidence and types of breast
tumours have been documented to vary from one part of the world to another.9 As in most
studies within and outside Nigeria, the frequency of benign breast tumours overwhelmingly out
number that of malignancies.24 The proportions however vary, as most breast lumps are likely to
be benign and approximately one out of ten breast biopsies turns out to be malignant.89 In this
study benign breast tumours which accounted for 66.3% of all the breast tumours were more
common than the malignant types (33.7% of cases) with a benign to malignant ratio of 2:1. This
is lower than the 73% reported in our centre a decade ago.24 The observed preponderance of
benign tumours over malignant varieties is in consonance with findings from Hong Kong13
where 89.1% of breast tumours were reported to be benign. Studies from the Afro-Caribbean14
and Ghana15 have also indicated that benign tumours are common representing 80% and 48% of
all breast tumours received. The findings of this study is also comparable with reports from
Zaria,17 Gombe,20 Ife,22 Calabar23 and Benin11 where 71.3%, 59.5%, 79%, 73.4% and 90% of the
cases were benign respectively.
The mean age of patients seen with benign tumours in this study was 29 years and 65.0% of
them were in the age group 21 – 40 years with peak incidence (41.7%) in age group 21 – 30
years. These results are consistent with the study by Otu et al23 in which majority of the patients
were below the age of 30 years. Reports from Zaria,17 Ilesha,18 and Gombe20 in Nigeria also
found the highest proportion of cases being below the age of 40 years.
Of the benign tumours fibroadenoma was found to be the most common variant accounting for
487 (47.1 %) cases and was most commonly seen (56.5%) in patients within the 3rd decade of
life. Similar preponderance of fibroadenoma amongst benign tumours of the breast was also
reported in other studies from Ghana15 and Kenya.16 This finding is also similar to reports from
Zaria,17 Ilesha,18 Gombe,20 Ife22 and Calabar23 but contrasts with the findings in Ibadan25 and
amongst Caucasians2 where fibrocystic change was reported to be the commonest benign breast
lesion. In a previous study carried out in Aminu Kano Teaching Hospital about a decade ago

51
fibrocystic change was reported as the commonest benign histological lesion comprising of
34.3% of all cases. This therefore shows a change in pattern even though the reason for the
change is not known. Fibroadenoma of the male breast is extremely rare and no case was found
in this study.
Fibrocystic change was the second most common benign breast lesion (25.4%) seen in this study
and the vast majority of the patients (48.3%) with fibrocystic change were in the 4th decade. This
is in consonance with several studies done in Saudi Arabia,90 India,91 Nepal,92 Kenya,16 and
Benin11 where fibrocystic change was found to be second in frequency to fibroadenoma. This
pattern is the reverse of what has been found in United States of America93 and Pakistan94 where
fibrocystic change was commoner than fibroadenoma. This has been explained as resulting from
differences in reproductive patterns in the different races.
Fibrocystic change is an important breast lesion because of its high frequency (second to
fibroadenoma in this study) and the ability of some of its subtypes to mimic the clinical and
radiographic appearance of carcinoma. Hormones also play a role in its development but the
exact pathogenesis still remains to be established.
Phyllodes tumours are said to be rare fibro-epithelial tumours which account for less than 1% of
all breast neoplasms.9 This study however found it to account for 4.8% of the breast biopsies
performed.
The benign breast tumours were more frequently unilateral than bilateral in this study with a
right sided preponderance of 55.0%, while 42.1% were left sided and 2.9% bilateral. This agrees
with the universal pattern and also with a study done in Ife22 but is at variance with earlier
findings by Oluwole et al95 where the incidence of benign breast lesions was higher in the left
breast.
Duct papilloma was seen in only 1.0% of cases in this study. Khanzada et al96 reported 4.7%
frequency within 3 years in Pakistan, while Mc Farlane14 in Jamaica reported 6.7% over a 2-year
period. This finding is comparable to 0.6% in Ibadan25 but is lower than 1.7% and 2.8% reported
in Ife22 and Makurdi97 respectively. Lactating adenoma which occurred in 5.6% of the patients
clustered around the reproductive age group and is comparable to 5.2% and 3.3% reported in
Makurdi97 and Ife22 respectively, but is higher than 1.6% documented in Zaria.17
52
Gynaecomastia was the only benign breast tumour recorded in males in this study. It constituted
1.4% of all the benign tumours demonstrating a decline in frequency when compared to 6%
reported a decade ago in our centre.24 This finding is lower than 4.9%, 1.9%, 2.4% and 3.4%
recorded in Zaria,17 Ibadan,25 Makurdi97 and Ife22 respectively. The incidence of this disease in
Nigerian male patients compares well with the 1% quoted in Caucasian series14 but is lower than
the 12% reported in Uganda.50 The mean age of 42 years found in our study is slightly at
variance with most published reviews, which report a bimodal age distribution at puberty /
adolescence and in the elderly. This study also found only 3 cases of adolescents with
gynaecomastia which may be attributed to the fact that this is a referral hospital based study and
figures quoted may not be a true reflection of relative incidence of gynaecomastia in adolescents
in our environment.
The study found 62(6.0%) cases of tubular adenoma, which is comparable to the finding in Ife22
but is higher than 2.4% recorded in Zaria.17 Sclerosing adenosis accounted for 34(3.3%) cases
which is lower than 4.5% reported in Ibadan25 and is higher than 1.4% documented in Zaria.17
Lipoma constituted 0.7% of all the benign cases seen, which is consistent with 1% and 0.6%
seen in Afro-Caribbean14 and Ibadan25 respectively. Other rare benign breast tumours observed
include granular cell tumour (0.9%) and schwannoma (0.5%).
In this study, cancer of the breast accounted for 11.9% overall of all malignant tumours. This
finding is similar to reports from Ghana15 but contrasts with the findings from Pakistan34 who
recorded higher figures of 34%. This finding is much higher than the 5% recorded in Kenya.37
Breast cancer was diagnosed in 34.2% of all breast specimens received in this study which is
higher than 26.6% reported by Otu et al43 in Calabar and 21% by Oluwole et al42 in Ife, but is
similar to 31.8% reported by Adeniji et al41 in Ilorin. The mean age at diagnosis of breast cancer
in this study was 42 years, which is relatively lower than 46.5 years obtained in an earlier study
conducted in our centre.27
African women with breast cancer are more likely to be premenopausal and the incidence peaks
between 35 and 45 years which is in agreement with our findings, and with the observation that
carcinoma of the female breast predominantly occurs a decade earlier in developing countries
than in Caucasians.57 The mean age of female breast cancer patients in United States of America
is 64 years and 77% of the cases occur in women over 50 years of age.2

53
This mean age also compares favourably with that of other parts of Nigeria. In Calabar,61
Ilorin,41 Jos,44 Ibadan,10 Ife,28 Gombe20 and Lagos59 the mean ages are within the 4th decade,
where as in Zaria17 the mean age is within the 3rd decade of life. In this series, breast cancer
occurred most commonly in age range of 31 to 40 years, followed by the age range of 41 to 51
years. This observed age range in which the bulk of the malignant tumours are found in this
study is comparable to 31 – 40 years also reported by Atoyebi et al59 at the Lagos University
Teaching Hospital and the 36 – 45 years documented by Ihekwaba60 at the University College
Hospital, Ibadan.
It however contrasts with the study by Adeniji et al41 in Ilorin where they reported a peak age
range between 40 – 49 years. These lower age ranges may be a reflection of the changing pattern
of carcinoma of the breast with increasing occurrence in younger women in our environment.
This may be based on the fact that in our society younger people are more educated, earn more
money and are more likely to go to hospitals than older people. Above all, younger people are
becoming aware of the deficiencies of alternative medicine practitioners.
Invasive ductal carcinoma (NST) is the commonest histologic type of breast cancer worldwide
accounting for about 40 – 75% of breast cancer in published series.77 It accounted for 59.5% of
the histopathological types in this study. Though the proportions are different, this is comparable
to 65.8% in Zaria,17 but is at variance with findings from Lagos (94%),59 Jos (91%),44 Ilorin
(78%),41 Ibadan (49.2%),60 Ife (97.3%),28 Gombe (68.6%)20 and 80.6% in an earlier study done in
our centre a decade ago.27 This decline in relative proportion of invasive ductal carcinoma may
be due to the fact that this is a referral hospital based study and the figures found may not be a
true reflection of relative incidence of invasive ductal carcinoma in our environment.
Medullary carcinoma was the second most common histologic type in this study accounting for
11.5% of cases, which agrees with earlier finding from our centre.27 Similarly high incidence of
medullary carcinoma has been reported from Saudi Arabia98 (13.4%) and Kenya37 but is at
variance with findings from Ilorin,41 Zaria17 and Ibadan60 where anaplastic carcinoma was found
to be second most common while in Ife28 ductal carcinoma in situ and papillary carcinomas
were the second and third most common cancers. Differences in the distribution of
histopathological types may be associated with different diagnostic criteria among the

54
pathologists. Medullary, mucinous, tubular and papillary carcinomas are associated with better
prognosis than invasive ductal and invasive lobular carcinomas.
Thirty seven (6.9%) cases of invasive lobular carcinoma were recorded in this study which is
higher than 2.8% and 0.6% reported in Ilorin41 and Ibadan60 respectively but is lower than 13.8%
found in Zaria.17
Male breast carcinomas constituted 6.6% of the cases in this study as against the 2.2% earlier
recorded in the study done in Kano27 and is more than the 1% found in developed countries.99
High incidence rate was also documented in some countries like Kenya (12.5%),49 Uganda
(5%),50 and Zambia (15%).51 Our figure is also higher than 2.2%, 5.2%, 3.4%, 6.1% and 1.9%
documented in Benin,52 Zaria,17 Ibadan,54 Ilorin,56 and Ife28 respectively, but is lower than 8.0%
and 8.6% recorded in Enugu53 and Jos55 respectively. This suggests that environmental factors
may be responsible for these variations in addition to liver diseases that result in
hyperoestrogenaemia which have also been suggested as possible factors leading to a greater
number of male breast cancers in our environment compared to the western world.
Most of the studies conducted in western world show high female to male ratio of breast cancers
as reports from England, Scotland, Northern Ireland and Wales showed 120:0.8, 132:0.3, 115:0.1
and 123:0.5 ratios respectively.48 The female to male ratio found in this study was 14.2:1.0
which compares favourably with 19.5:1 from Zaria17 but is higher than 7:1 in Calabar.43
In this study, breast carcinoma was found to occur more in the right breast (65.4%) than the left
(34.2%), and only 2 (0.4%) cases were bilateral. The right sided predilection in this review is
higher than that in Benin (53.5%)66 and Ilorin (52.9%).41 Other centres with right sided
predilection are Ife,28 Lagos59 and Kano27 and these are at variance from left sided predilection in
Zaria.67 However, apart from apocrine carcinoma which tends to occur more on the left breast
(54%) other histological types were similarly found to be more frequently affecting the right
breast with invasive lobular carcinoma accounting for 25(76%) cases as the most predominant.
This compares favourably with reports from Benin66 where most of the histologic types were
also on the right with medullary carcinoma, 17(43%) been more common. There is no clear cut
reason for the predilection of the right breast to the left because other studies have shown breast
cancer occurring more frequently in the left breast than the right.56 Only 2(0.4%) cases occurred

55
bilaterally which is lower than 2.4%, 2.2%, 0.8% and 4% documented in Ilorin,41 Ife,28 Benin66
and Lagos.59 Although the two tumours might have developed synchronously, it is possible that
one was a metastasis of the other. It is known that bilaterality and multicentricity are more
common with invasive lobular carcinoma79 which accounted for one of the two bilateral cases in
this study.
The tumour grade which is the summation of tubular pattern, nuclear pleomorphism and mitotic
figure tends to determine the level of differentiation and prognosis of the tumour. In this study
malignant breast tumours were graded and 237(44.6%) cases were grade 1, 133(25.0%) grade 2
and 161(30.4%) were grade 3. This contrasts with the study done in Port Harcourt100 where 21%
fall in grade 1, 26% in grade 2 and 53% in grade 3

56
CONCLUSION
This ten year retrospective study of breast tumours in AKTH, Kano has shown that these
tumours are quite common and are seen in both sexes with a striking female preponderance. The
findings are generally similar to most previous studies from Nigeria and Africa with minimal
variations. The benign tumours which accounted for 66.3% of all the breast tumours were more
common than the malignant types (33.7%) with a benign to malignant ratio of 2:1. Overall the
benign and malignant tumours were predominantly seen in the 3rd to 4th decades and are found to
be more common on the right side than on the left.
Fibroadenoma was the predominant type of benign breast tumour seen in our centre which
differs from most international studies that report fibrocystic disease to be more common but is
however similar to most other Nigerian studies which indicate a preponderance of the tumour
over other benign breast tumours. Gynaecomastia, the only benign breast tumour in males
constituted 1.4% of all the benign tumours which is relatively low compared to most other
Nigerian and African studies.
Invasive ductal carcinoma(NST) was the predominant type of malignant breast tumour seen in
our centre which is similar to other International and Nigerian studies. Other rare malignant
breast tumours such as neuroendocrine carcinoma, adenoid cystic carcinoma, sebaceous
carcinoma and Burkitt lymphoma were also infrequently documented in this study. There is also
declining mean age of breast cancer in our study compared with previous studies, the reason is
unknown.
Immunohistochemistry for the routine breast cancer markers – oestrogen receptor, progesterone
receptor and Her-2 was only recently introduced in our laboratory and was not available in most
of the study period for proper categorization of breast cancer cases, which is one of the major
limitations of the study.
It is hoped that the findings of this study will pave way for more comprehensive multicentre
studies on breast tumours.

57
REFERENCES
1. Ihezue CH, Anele AA. Breast cancer prevention and detection. J Med Res 2002; 2: 26-28.
2. Lester SC. The breast. In: Kumar V, Abbas AK, Fausto N. Robbins and Cotran pathologic
basis of disease. 8th ed. Philadelphia: Elsevier. 2010. p. 1066-1093.
3. Barrett KE, Barman SM, Boitano S, Brooks HL. The gonads: development and function of
the reproduction system. In: Ganong. Review of medical physiology. 23rd ed. Norwalk:
Lange; 2010. p. 426-27.
4. Veronesi U, Boyle P, Goldhirsch A, Orecchia R, Viale G. Breast cancer. Lancet 2005; 365
(9472): 1727-41.
5. Parkin DM, Bray F, Ferlay J, Pisani DM. Global cancer statistics, 2005. CA Cancer J Clin
2005; 55(2): 74-108.
6. Vorobiof DA, Sitas F, Vorobiaf G. Breast cancer incidence in South Africa. J Clin Oncol
2001; 19(18): 125-7.
7. Omar S, Khaled H, Gaafar R, Zekry AR, Eissa S, El-Khatib O, et al. Breast cancer in Egypt :
a review of disease presentation and detection strategies. Eastern Med Health J 2003; 9(3):
448-63.
8. Adesunkanmi AR, Lawal OO, Adelusola KA, Durosimi MA. The severity, outcome and
challenges of breast cancer in Nigeria. Breast 2006; 15(3): 399-409.
9. Ellis IO, Schnitt SJ, Bussolati G, Tavassoli FA, Mukai K, Tabar L, et al. Tumours of the
breast including histological classification In: Fattaneh A, Tavassoli A, Peter D. (eds).
Pathology and genetics of tumours of the breast and female genital organs. World Health
Organization classification of breast tumours. Lyon (France): IARC Press; 2005. p.9-110.
10. Ihekwaba C. Breast cancer in Nigerian women. Br J Surg 1992; 79: 771-5.
11. Okobia MN, Osime UA. A clinicopathological study of benign breast diseases in Benin City,
Nigeria. Nig J Surg 1998; 5: 64-68.
12. Harsh M. The breast. In: Textbook of Pathology. 5th ed. New Delhi: Jaypee Brothers; 2006.
p.780-791.

58
13. Cederquist RA, Onukak EE. Benign breast disorders in nonwestern populations. World J
Surg 1989; 13(6): 750-2.
14. McFarlane ME. Benign breast diseases in an Afro-Caribbean population. East Afr Med J
2001; 78(7): 358-359.
15. Chhanda B. Fibroadenoma in women in Ghana. Pan Afr Med J 2009; 2: 11-15.
16. Bjerregaard B, Kung’u A. Benign breast lesions in Kenya: a histopathological study. East Afr
Med J 1992; 69(5): 231-235.
17. Yusuf LMD, Odigie VI, Mohammed A: Breast masses in Zaria, Nigeria. Annals Afr Med
2003; 2: 13-16.
18. Adesunkanmi AR, Agbakwuru EA. Benign breast diseases at Wesley Guild Hospital, Ilesha,
Nigeria. West Afr Med J 2001; 20(2): 146-51.
19. Anyanwu SN. Fibroadenoma of the breast in Nigerian Igbos. S Afr Med J 2000; 90(12):
1223-6.
20. Mayun AA, Pindiga UH, Babayo UD. Pattern of histological diagnosis of breast lesions in
Gombe. Nig J Med 2008; 17(2): 159-62.
21. Anyikam A, Nzegwu MA, Ozumba BC, Okoye I, Olusina DB. Benign breast lesions in
Eastern Nigeria. Saudi Med J 2008; 29(2): 241-4.
22. Oluwole SF, Fadiran OA, Odesanmi WO. Diseases of the breast in Nigeria. Br J Surg 1987;
74(7): 582-5.
23. Otu AA. Benign breast tumours in an African population in South East. J R Coll Surg Edinb
1990; 35(6): 373-5.
24. Ochicha O, Edino ST, Mohammed AZ. Benign breast lesions in Kano. Nig J Surg Res 2002;
4: 1-5.
25. Ajayi OO, Adekunle O. Non-malignant breast masses in an African population. Br J Surg
1973; 60: 465-8.
26. Rosai J, editor. Breast. In: Ackerman’s surgical pathology. 9th ed. Philadelphia: Mosby;
2004. p. 1763-1839.
27. Edino ST, Ochicha O, Alhassan S, Mohammed AZ, Ajayi OO. A
Clinicopathological review of breast cancer in Kano. Nig J Surg 2000;
7(2): 70-75.

59
28. Adelusola KA, Fadiran OA, Adesunkanmi AR, Odesanmi WO. Breast cancer in Nigerian
women in Ile-Ife. Nig Med Pract 1996; 13: 17-2.
29. Ferlay J, Shin HR, Bray F, Forman D, Mathers C, Parkin DM. Estimates of worldwide
burden of cancer in 2008: Globocan 2008. Int J Cancer 2010; 127(12):2893-917.
30. Ries LAG, Eisner MP, Kosary CL. SEER cancer statistics review, 1973-1999, Bethesda:
National Cancer Institute; 2002.
31. Jemal A, Murray T, Samuel A. Cancer Statistics, 2007. Cancer J Clin 2003; 53: 5-26.
32. Cancer Research UK 2009.
33. Heidari Z, Mahmoud HR, Sakhavar N. Breast Cancer Screening Knowledge and Practice
among women in Southeast of Iran. Acta Medica Iranica 2008; 46(4): 321-28.
34. Ahmed F, Mahmud S, Hatcher J, Khan SM. Knowledge of breast cancer risk factors among
nurses in teaching hospitals of Karachi, Pakistan: a cross-sectional study. BMC Nurs 2006; 5:
6-10.
35. Sitas F, Madhoo J, Wessie J. Incidence of histologically diagnosed cancer in South Africa,
1993-1995. National Cancer Registry, South African Institute for Medical Research,
Johannesburg, 1998.
36. Daniel AV, Freddy S, Gabriel V. Breast cancer incidence in Africa. J Clin Onc 2001;
19(18): 125-27.
37. Bjerregaard B, Kung’u A. Breast cancer in Kenya. A Histopathological and Epidemiologic
study. East Afr Med J 1992; 54: 47-56.
38. Visvanathan R. Breast carcinoma in Nigerian women. Br J Surg 1993; 80: 126.
39. Adebamawo CA, Adekunle OO. Case controlled study of the epidemiological risk factors for
breast cancer in Nigeria. Br J Surg 1999; 86: 665-68.
40. Aghadiuno PU. Pathology of breast cancer. M.D. Thesis. Glasgow 1979.
41. Adeniji KA. Pathological appraisal of carcinoma of the female breast in Ilorin, Nigeria. Nig
postgrad Med J 1999; 6(2): 56-59.
42. Oluwole SF, Fadiran OA, Odesanmi WO. Diseases of the breast in Nigeria. Br J Surg 1987;
74: 582-806.
43. Otu AA, Ekanem IA, Khalil MI, Ekpo MD, Attah EB. Characterisation of breast cancer
subgroups in an African population. Br J Surg 1989; 76: 182-84.
44. Ihezue CH, Ugwu BT, Nwana EJ. Breast cancer in highlanders. Nig J Surg Sci 1994; 4: 1-4.
45. Weiss JR, Moysich KB, Swede H. Epidemiology of male breast cancer. Cancer
Epidemiology, Biomarkers and Prevention 2005; 14(1): 20-26.
46. Ravandi-Kashani F, Hayes TG. Male breast cancer: a review of the literature. Eur J Cancer
1998; 34: 1341-7.
47. Leong SP, Shen ZZ, Liu TJ, Tajima T. Breast cancer in Asian and Western Countries. World
J Surg 2010; 34(10): 2308-24.
48. Joli RW, Kristen BM, Heleh S. Epidemiology of male breast cancer. Cancer Epidemiol
Biomarkers Prev 2005; 14: 20-24.

60
49. Amir H, Makwanya CK, Moshiro AC, Kwesigabo G. Carcinoma of the male breast : A
sexually transmitted disease? East Afr Med J 1996; 73: 187-190.
50. Ojara EA. Carcinoma of male breast in Mulago Hospital, Kampala. East Afr Med J 1978; 5:
489-491.
51. Bhagwandin S. Carcinoma of the male breast in Zambia. East Afr Med J 1972; 49: 176-199.
52. Iribhogbe PE, Ohanaka EC. Male breast cancer in Benin City. Nig J Surg 2003; 9: 7-10.
53. Ihezue CH, Ojukwu JO, Mbonu OO: Male breast carcinoma in Eastern Nigeria. A 13 year
study. West Afr J Med 1992; 11: 203-210.
54. Aghadiuno PU: Male breast cancer. Analysis of forty three cases in Ibadan. Afr J Med Sc
1987; 16: 16-26.
55. Kidmas AT, Ugwu BT, Manasseh AN, Iya D, Opaluwa AS. Male breast malignancy in Jos
University Teaching Hospital. West Afr J Med 2005; 24(1): 36-40.
56. Adeniji KA, Anjorin AS. Diseases of the male breast in Ilorin, Nigeria. Nig Qt J Hosp Med
1999; 9(1): 8-10.
57. Fregene A, Newman LA. Breast cancer in sub-Saharan Africa: How it relates to breast
cancer in African- American women. Cancer 2005; 103: 1540-1550.
58. Abimiku BA, Mukhtar AU. The pattern of cancer in Federal Capital Territory of Nigeria.
Sahel Med J 2002; 5(3): 152-155.
59. Atoyebi OA, Atimomo CE, Adesanya AA, Beredugo BK. An appraisal of 100 patients with
breast cancer seen at the Lagos University Teaching Hospital. Nig Qt J Hosp Med 1997; 7(2):
104-108.
60. Ihekwaba FN. Breast cancer in Nigerian women at the University College Hospital, Ibadan.
Br J Surg 1992; 79: 771-775.
61. Stanley N, Anyanwu C. Breast cancer in Eastern Nigeria: A ten year review. West Afr Med J
2000; 21: 120-125.
62. Dogo D, Gali BM, Ali N, Nggada HA. Male breast cancer in north eastern Nigeria. Nig J
Clin Pract 2006; 9: 139-141.
63. Hassan I, Mabogunje OA. Cancer of the male breast in Zaria, Nigeria. East Afr Med J 1995;
72: 457-458.
64. Ihekwaba FN. Breast cancer in men in black Africa: a report of 73 cases. J R Coll Surg Edinb
1994; 39: 344-347.
65. Umoh MS, Asuquo ME, Otu AA, Imaobong E. Male breast cancer in Calabar, Nigeria. A
twenty year experience (1983-2002). Global J Com Med 2009; 2(1): 21-25.
66. Chiedozi LC. Breast cancer in Nigeria. Cancer 1985; 55: 653-657.
67. Hassan I, Onusk EE, Mabogunje OA. Breast Cancer in Zaria, Nigeria. J R Coll Surg Edinb
1992; 37: 159-161.
68. Colditz GA, Willett WC, Hunter DJ. Family history, age, and risk of breast cancer.
Prospective data from the Nurses’ Health Study. JAMA 1993; 270: 338-43.
69. Lynch HT, Lynch JF. Breast cancer genetics in an oncology clinic: 328 consecutive patients.
Cancer Genet Cyto-genet 1986; 22: 369-71.

61
70. Lindblom A. Familial breast cancer and genes involved in breast carcinogenesis. Breast
cancer Res Treat 1995; 34: 171-83.
71. Adebamawo CA, Ogundiran TO, Adenipekun AA, Oyesegun RA, Campbell OB, Akang EU
et al. Obesity and Height in Urban Nigerian Women with Breast Cancer. Ann Epidemiol
2003; 13; 455-461.
72. Hoskins KF, Stopfer JE, Calzone KA. Assessment and counseling for women with a family
history of breast cancer. A guide for clinicians. JAMA 1995; 273: 577-85.
73. Henderson BE, Ross RK, Judd HL. Do regular ovulatory cycles increase breast cancer risk?
Cancer 1985; 56: 1206-8.
74. Okobia M, Bunker C, Zmuda J, Kammere C, Vogel V, Uche E et al. Case-control study of
risk factors for breast cancer in Nigerian women. Intl J Cancer 2006; 119: 2179-2185.
75. Egan KM, Newcomb PA, Longnecker MP. Jewish religion and risk of breast cancer. Lancet
1996; 347: 1645-6.
76. Fregene A, Newman LA. Breast cancer in sub-saharan Africa: how does it relate to breast
cancer in African American women? Cancer 2005; 103(8): 1540-1550.
77. Elston CW, Ellis IO. Classification of malignant breast disease. In: Elston CW, Ellis IO. The
breast. 3rd ed. Edinburgh: Churchill Livingstone; 1998. p. 239-247.
78. Simpson JF. Predictive utility of the histopathologic analysis of carcinoma of the breast. Adv
Pathol Lab Med 1994; 7: 107-111.
79. Fisher ER, Gregorio RM, Fisher B. The pathology of invasive breast cancer. Cancer 1975;
36: 1-85.
80. Silverstein MJ, Lewinsky BS, Waisman JR. Infiltrating lobular carcinoma. Is it different
from infiltrating duct carcinoma? Cancer 1994; 73(6): 1673-1677.
81. Rosen PP, Oberman HA. Tumours of the mammary gland. Washington, DC: Armed Forces
Institute of Pathology; 1993.
82. Norrris HJ, Taylor HB. Prognosis of mucinous carcinoma of the breast. Cancer 1965; 18:
879-883.
83. Norris HJ, Taylor HB. Sarcomas and related mesenchymal tumours of the breast. Cancer
1968; 22(1): 22-28.
84. McCrea ES, Johnston C, Haney PJ. Metastases to the breast. AJR 1992; 141(4): 685-690.
85. Cangiavella J, Symmans WF, Cohen JM. Malignant melanoma metastatic to the breast.
Cancer 1998; 84(3): 160-162.
86. Elston CW, Ellis IO. Assessment of histologic grade. In: Elston CW, Ellis IO. The breast. 5th
ed. Edinburgh: Churchill Livingstone; 2006. p. 365-384.
87. Rosen PP, Saigo PE, Braun DW. Axillary micro- and macrometastases in breast cancer.
Prognostic significance of tumour size. Ann Surg 1981; 194: 585-91.
88. Luck AA. The influence of basal phenotype on the metastatic pattern of breast cancer. Clin
Oncol 2008; 20: 40-47.
89. Deane K, Degner L. Information needs uncertainty anxiety in women who had a breast
biopsy with benign outcome. Cancer Nursing 1998; 21: 117-26.

62
90. Chiedozi LC, El-Haq IA, Kollur SM. Breast diseases in the Northern region of Saudi Arabia.
Saudi Med J 2003; 24: 623-7.
91. Chaudhuri M, Sen S, Sengupta J. Breast lumps: A study of 10 years. J India Med Assoc
1995; 93: 455-7.
92. Khan S, Kapoor AK, Khan IU. Prospective study of pattern of breast disease at Nepalgunj
Medical college, Nepal. Kathmandu Uni Med J 2003; 1: 95-100.
93. Schnitt SJ. Benign breast diseases and breast cancer risk, morphology and beyond. Am J Surg
Path 2003; 27: 836-41.
94. Memon A, Parveen S, Malik MA. Changing pattern of benign breast lumps in young
females. World J Med Sci 2007; 2(1): 21-24.
95. Oluwole SF, Freemen HP. Analysis of benign breast lesions in blacks. Amer J Surg 1979;
137: 786-89.
96. Khanzada WT,Samad A, Sushel C. Spectrum of benign breast diseases. Pak J Med Sci 2009;
25(2): 265-68.
97. Echejoh G, Dzuachi D, Jenrola A. Histopathologic analysis of benign breast diseases in
Makurdi, North Central Nigeria. Int J Med Sci 2011; 3(5): 125-128.
98. Anim JT, Sohaibani MO, Grant CS, Dale T. Breast cancer as seen in King Fahad University
Hospital Al-kbobar. J R Coll Surg 1989; 34: 201-204. Fentiman IS, Fourquet A, Hortobagyi
GN. Male breast cancer. Lancet 2006; 367(9510): 595-604.
99. Fentiman IS, Fourquet A, Hortobagyi GN. Male breast cancer. Lancet 2006; 367(9510): 595-
604.
100. Gogo-Abite M, Nwosu SO. Histopathological characteristics of female breast carcinomas
seen at the University of Port Harcourt Teaching Hospital, Nigeria. Niger J Med 2005; 14(1):
72-76.

63
APPENDIX
WHO Histological Classification of Breast Tumours 200221
1. Epithelial tumours
Invasive ductal carcinoma, not otherwise specified
Mixed type carcinoma
Pleomorphic carcinoma
Carcinoma with osteoclastic giant cells
Carcinoma with choriocarcinomatous features
Carcinoma with melanotic features
Invasive lobular carcinoma
Tubular carcinoma
Invasive cribriform carcinoma
Medullary carcinoma
Mucinous carcinoma and other tumours with abundant mucin
Mucinous carcinoma
Cystadenocarcinoma and columnar cell mucinous carcinoma
Signet ring cell carcinoma
Neuroendocrine tumours
Solid neuroendocrine carcinoma
Atypical carcinoid tumour
Small cell/ oat cell carcinoma
Large cell neuroendocrine carcinoma
Invasive papillary carcinoma
Invasive micropapillary carcinoma
Apocrine carcinoma
Metaplastic carcinomas
Pure epithelial metaplastic carcinomas
Squamous cell carcinoma
Adenocarcinoma with spindle cell metaplasia
Adenosquamous carcinoma
Mucoepidermoid carcinoma

64
Mixed epithelial/mesenchymal metaplastic carcinomas
Lipid-rich carcinoma
Secretory carcinoma
Oncocytic carcinoma
Adenoid cystic carcinoma
Acinic cell carcinoma
Glycogen-rich clear cell carcinoma
Sebaceous carcinoma
Inflammatory carcinoma
Micro invasive carcinoma
Lobular neoplasm
Lobular carcinoma in situ
Intraductal proliferative lesions
Usual ductal hyperplasia
Flat epithelial atypia
Atypical ductal hyperplasia
Ductal carcinoma in situ
Intraductal papillary neoplasms
Central papillomas
Peripheral papillomas
Atypical papillomas
Intraductal papillary carcinoma
Intracystic papillary carcinoma
Benign epithelial proliferations
Adenosis including variants
Sclerosing adenosis
Apocrine adenosis
Blunt duct adenosis
Microgladular adenosis
Adenomyoepithelial adenosis
Radial scar/complex sclerosing lesion

65
Adenomas
Tubular adenoma
Lactating adenoma
Apocrine adenoma
Pleomorphic adenoma
Ductal adenoma
Benign Nonproliferative changes
Duct ectasia
Cyst
Apocrine change
2. Myoepithelial lesions
Myoepitheliosis
Adenomyoepithelial adenosis
Adenomyoepithelioma
Malignant myoepithelioma
3. Mesenchymal tumours
Haemangioma
Angiomatosis
Haemangiopericytoma
Pseudoangiomatous stromal hyperplasia
Myofibroblastoma
Fibromatosis
Inflammatory myofibroblastic tumour
Lipoma
Granular cell tumour
Neurofibroma
Schwannoma
Leiomyoma
Angiosarcoma

66
Liposarcoma
Rhabdomyosarcoma
Osteosarcoma
Leiomyosarcoma
4. Fibroepithelial tumour
Fibroadenoma
Phyllodes tumour
Benign
Borderline
Malignant
Mammary hamartoma
Periductal stromal sarcoma
5. Tumours of the nipple
Nipple adenoma
Syringomatous adenoma
Pagets disease of the nipple
6. Malignant lymphoma
Diffuse large B-cell lymphoma
Burkitt lymphoma
Extranodal marginal-zone B-cell lymphoma of MALT type
Follicular lymphoma
7. Male breast tumours
Gynaecomastia
Carcinoma
Invasive
In situ
8. Metastatic tumours


















