
HISTOLOGICAL PATTERN OF LIVER DISEASES IN JOS …
77
HISTOLOGICAL PATTERN OF LIVER DISEASES IN JOS UNIVERSITY TEACHING HOSPITAL, JOS: A TEN YEAR RETROSPECTIVE STUDY (2000-2009) BY VHRITERHIRE AKPOBOME RAYMOND (MBBS) DISSERTATION SUBMITTED IN PARTIAL FULFILMENT OF THE REQUIREMENTS FOR THE AWARD OF THE FELLOWSHIP OF THE NATIONAL POSTGRADUATE MEDICAL COLLEGE OF NIGERIA IN PATHOLOGY MAY, 2013
Transcript of HISTOLOGICAL PATTERN OF LIVER DISEASES IN JOS …

HISTOLOGICAL PATTERN OF LIVER DISEASES IN JOS
UNIVERSITY TEACHING HOSPITAL, JOS:
A TEN YEAR RETROSPECTIVE STUDY (2000-2009)
BY
VHRITERHIRE AKPOBOME RAYMOND (MBBS)
DISSERTATION SUBMITTED IN PARTIAL FULFILMENT OF THE
REQUIREMENTS FOR THE AWARD OF THE FELLOWSHIP OF THE
NATIONAL POSTGRADUATE MEDICAL COLLEGE OF NIGERIA IN
PATHOLOGY
MAY, 2013

ii

iii

iv

v
CONTENTS
Title page i
Supervisors ii
Certification iii
Declaration iv
Table of Contents v
Dedication vi
Acknowledgement vii
Abstract viii
Introduction 1
Aims and Objectives 4
Literature Review 5
Methodology 17
Results 19
Tables and Figures 27
Discussion 49
References 56
Appendix A: WHO histological classification of tumours of the liver and
intra-hepatic bile ducts 63
Appendix B: Knodell scoring system 66
Appendix C: Ethical clearance 67

vi
DEDICATION
To all those who expend their days seeking cures to diseases and end to all causes
of human suffering; truly, they are angels on earth, whose beautiful minds bear
immortal seeds of boundless hope.
To Benita, my little lovely daughter whose curiosity never fails to amuse me.

vii
ACKNOWLEDGEMENT
I wish to appreciate the dedicated tutorship by Professor B M Mandong and the
other consultants in the department.
Professor Mandong, Professor Abdulkareem and Dr Echejoh are the giants upon
whose shoulders I stood to see; and whose previous research work guided me
through the initially shadowy path of this project.
I also wish to thank the other resident doctors in the department and friends who
provided helpful suggestions and assistance during the course of this work.
The other staff in the laboratory have been very helpful and supportive most
especially Pastor Steve, Mrs Rifkat Bot, Kizito, Eno, Ju and Madame Mary. Mrs Bot
was ever available to skilfully section and stain the tissue specimens.

viii
ABSTRACT
Background: Liver disease is among the common causes of hospital visitation and
admission in most of tropical Africa. Among the liver diseases, viral hepatitis and
other stigmata of chronic liver disease are the commonest reasons for admission. In
most medical wards, patients with liver cirrhosis and hepatocellular carcinoma
constitute a significant proportion of admissions.
Objective of this study: This study was undertaken to document the histological
appearances of diseases in liver biopsies in Jos.
Methods: All documented cases of liver biopsies over a period of ten years were
reviewed.
Results: There were a total of 374 histologically diagnosed liver biopsy specimens
during the ten-year period of review (2000-2009). Liver diseases were found to be
more common in males than in females with male female ratio of 1.9:1. Most cases
occurred within the 31-40 years age bracket. Chronic viral hepatitis was the most
common diagnosis (61%) followed by hepatocellular carcinoma (20.3%) and
cirrhosis (7.8%). Chronic viral hepatitis and cirrhosis occurred most frequently in the
fourth decade while hepatocellular carcinoma peaked a decade later. More than half
of the cases of chronic hepatitis (51.1%) had Knodell scores between the range of
5-8 points while in cirrhosis more than half (51.7%) scored 13-18 points. Analysis of
variance (ANOVA) of these scores in both conditions failed to demonstrate any
statistically significant difference between males and females (P-value = 0.63).
There was poor correlation between age and Knodell scores (Pearson’s r = 0.0067).

ix
The patterns of hepatocellular carcinoma observed included trabecular (71.1%),
acinar/pseudoglandular (13.2%), clear cell (6.6%) and fibrolamellar (1.3%).
Conclusion: This study has demonstrated that there is a high frequency of
occurrence of histologically diagnosed chronic hepatitis and hepatocellular carcinoma
in Jos.
Keywords: liver, hepatitis, Knodell score, hepatocellular carcinoma.

1
CHAPTER ONE
INTRODUCTION
The liver weighing between 1.4 - 1.6 Kg is the second largest organ in the body. It is
roughly triangular and located mainly in the right upper quadrant of the abdomen
inferior to the diaphragm. As seen under the light microscope, cords of polyhedrally
shaped hepatocytes are organised into hexagonal lobules with a central vein and
portal tracts at the corners. The vascular sinusoids separate these cords, lined by
fenestrated flattened endothelial cells. Kupffer cells are attached to the luminal
border of the endothelial cells.1
Histological examination following a liver biopsy is the traditional gold standard for
the evaluation of liver diseases. Liver biopsy was first described by Ehrlich in 1883
but it gained wider acceptance after Menghini again described the procedure in
1958.2
The last 50 years has witnessed a dramatic change in the indications for performing
a liver biopsy because of better understanding of liver diseases, newer disease
entities and the availability of newer and advanced radiological, immunological,
biochemical and genetic markers.3
The common indications for requesting a liver biopsy include abnormal liver function
tests, fever of unknown origin, evaluation of chronic liver disease for diagnosis,
grading, staging and assessment of therapy, evaluation of cholestatic disorders,
tumours, unexplained hepatomegaly, evaluation of a potential living donor for liver
transplantation, drug reactions and non-alcoholic steatohepatitis (NASH).2

2
The approaches for obtaining liver tissue are percutaneous, transjugular,
laparoscopic and intra-operative. The percutaneous liver biopsy technique is the
most commonly used. It may be a blind procedure or guided by ultrasound or
computed tomography scan. Liver tissue may also be obtained during an autopsy.4
The needles for percutaneous liver biopsy are grouped into three categories: suction
needles (Menghini, Klatskin, Jamshidi), cutting needles (Vim-Silverman, Tru-cut),
and spring-loaded cutting needles that have a built-in triggering mechanism.2
Disposable Tru-cut needles are now used in many centres. The adequacy of the
specimen size is of concern to pathologists. A biopsy length of not less than 1.0 cm
to 1.5 cm is generally considered adequate for the evaluation of parenchymal liver
diseases. Some authors recommend larger biopsy sizes up to 2.5 cm in length.2 The
tissue is fixed in 10% formalin, processed and stained using standard methods.
There are concerns about cost, post-biopsy complications and inter-observer
variation in the interpretation of liver biopsy specimens, but it has remained the
procedure of choice for diagnosis and monitoring of patients with liver disorders.5,6
The wide range of morphological changes which occur following injury to
hepatocytes in disease conditions include degeneration, intracellular accumulation,
necrosis, apoptosis, inflammation, regeneration, and fibrosis.1
A systematic approach to the evaluation of liver biopsy is essential in order to ensure
that important diagnostic findings are not overlooked. The slide is first of all scanned
under low magnification to assess the entire architecture. In the portal tracts, the
portal veins, hepatic arteries, bile ducts and lymphatics are examined. The limiting
plate, periportal hepatocytes, sinusoids, pericentral hepatocytes and terminal hepatic

3
venules are next observed for changes. Focal lesions are studied carefully. Findings
are correlated with clinical information.
At least six stains including haematoxylin and eosin (H&E), and histochemical stains
are employed. These include periodic acid Schiff (PAS), Perls’ Prussian blue,
trichrome (or Van Gieson), reticulin and Victoria blue stains. Fibrosis, even in the
early stages is highlighted by reticulin silver impregnation. The trichrome stain
highlights Mallory hyaline and megamitochondria in alcoholic liver disease. Victoria
blue, Orcein and Gomori aldehyde fuchsin stains detect hepatitis B surface antigen
and elastic fibres which are abundant in cirrhosis.4
Other techniques include immunohistochemistry, molecular studies (in situ
hybridization, polymerase chain reaction), electron microscopy and metal assays
(Wilson disease, genetic haemochromatosis). Non-invasive techniques of estimation
of the stage and grade of liver disease include the use of fibroscan, aspartate
aminotransferase to platelet ratio index (APRI).7,8 Serology and imaging studies are
also used in the investigation of liver diseases.4
Although there is an increasing use of these non-invasive methods, proper
diagnostic evaluation still requires histological examination of liver biopsy specimens.
This study examined the pattern of liver diseases on biopsy specimens submitted at
the histopathology laboratory over a period of ten years. This study will contribute to
the existing pool of information on the morphological pattern of histologically
diagnosed liver diseases in our environment.

4
CHAPTER TWO
AIMS AND OBJECTIVES
Aim
The aim of this study is to describe the histological pattern of liver diseases
diagnosed in Jos University Teaching Hospital, Jos, during the period of study.
Objectives
1. To determine the specific histological diagnosis of all the cases;
2. To determine the histological activity index in cases of hepatitis and cirrhosis
using the Knodell scoring system;
3. To determine the sex and age distribution of the various histological
diagnoses;
4. To compare results with observations in similar research done in other
centres.

5
CHAPTER THREE
LITERATURE REVIEW
1. CHRONIC VIRAL HEPATITIS
Chronic hepatitis is a symptomatic, biochemical or serological evidence of continuing
or relapsing hepatic disease for more than six months with histologically documented
inflammation and necrosis.1 Aetiological agents of chronic hepatitis include hepatitis
B, C, and D, drugs, autoimmune and genetic disorders. It is a precursor lesion for
cirrhosis and hepatocellular carcinoma. The clinical features are extremely variable
and are not predictive of outcome.1
Chronic hepatitis formed 31.7% of liver biopsies reported in Jos .9 Previously,
Osuafor et al had found chronic active hepatitis to constitute only 6.5% of a series of
154 liver biopsies histologically analysed at Enugu.10 In a similar study in Kano,
chronic hepatitis was the commonest histological diagnosis (40.5%). Minimal necro-
inflammation without fibrosis was present in 24.4% of these cases. Minimal necro-
inflammation with fibrosis occurred in 3 (8.1%) but severe necro-inflammation with
or without fibrosis and periportal inflammation were seen in only 1 (2.7%) of the
patients.11
Lesi and colleagues in Lagos found chronic hepatitis to be histologically confirmed in
39 (53%) out of a total of 97 patients with clinical and sonographic evidence of
probable chronic liver disease.12
Ndububa et al studied seventy chronic hepatitis patients at Ibadan and observed 57
(75.7%) to be symptomatic while 24.3% were asymptomatic. The asymptomatic

6
cases were found during tests before blood transfusion or routine medical tests.
They were all positive for hepatitis B surface antigen (HBsAg) and negative for anti-
hepatitis C virus (HCV) antibody. Only one of the six symptomatic patients tested
positive for anti-HCV. All of the asymptomatic cases studied had a Knodell
histological grade of ≤ 8 and none with fibrosis. On the other hand, 56.6% of the 53
symptomatic patients with a histological grade of ≥ 9 had stage 3 or 4 fibrosis.
Severe necro-inflammation (HAI score ≥ 14) was found in 11 (20.8%) of the
symptomatic patients.13 This shows that the presence of symptoms may represent a
more severe disease.
The high prevalence of HBV infection in Nigeria was demonstrated by Olubuyide et
al in another study conducted at Ibadan in which 59.3% of hepatocellular carcinoma
patients were HbsAg positive. 14 An investigation into the association between
chronic HBV infection and hepatocellular carcinoma in Maiduguri revealed 86.8% of
114 HCC patients to be positive for HBsAg. 15 This was a significantly higher figure
than was found at Ibadan.
There is a low prevalence of hepatitis C virus infection in most of Africa. The
literature, however, displays an interesting pattern. Nwokedi et al observed HCV
seroprevalence rate of 6.2% in 1007 patients tested at Aminu Kano University
Teaching Hospital, Kano, over a period of three years.16 A slightly higher figure of
9.3% was observed in cirrhotic patients studied in The Gambia.17
However, Egypt has been reported to have the highest country wide prevalence of
HCV infection where eight to ten million of the 68 million population is estimated to
be infected18. Strickland et al studied the correlates of HCV in Egypt in a case control

7
study of 237 patients with liver disease. Anti-HCV antibody positive patients formed
58.2%. This high figure was linked to previous injection treatment for
schistosomiasis in 65.9% of the patients.18
The histological features of mild chronic hepatitis consist of inflammation limited to
the portal tracts and liver architecture remains well preserved. In HCV infection
there are lymphoid aggregates and focal steatosis. As the disease progresses,
interface hepatitis and bridging necrosis increase leading to fibrosis and invariably
cirrhosis.
The definitive diagnosis of chronic hepatitis, monitoring of response to therapy and
the progress of the disease rely heavily on liver biopsy.
2. GRANULOMATOUS HEPATITIS
Granulomas are aggregates of macrophages, often admixed with other inflammatory
cells, which usually result from chronic antigen presentation. Hepatic granulomas are
reportedly present in 2 - 10% of all liver biopsy specimens.19 Tuberculosis,
sarcoidosis, primary biliary cirrhosis, drugs and several infectious agents have been
implicated as causative agents. Primary biliary cirrhosis is the most common cause in
the western world.20
Granulomatous hepatitis was reported as the most common diagnosis among
patients who died of HIV/AIDS in Jos, accounting for 34% of the cases. Fourteen per
cent were non-specific aggregates of epithelioid cells.21 Four cases of granulomas
were also reported in another study of 227 liver biopsies in Jos. Two of these were

8
tuberculoid with caseous necrosis and one was a case of schistosomiasis. The
remaining one was a non-specific aggregate of epithelioid cells.9 Osuafor et al
documented granulomatous hepatitis comprising 1.3% of 154 liver biopsy cases at
Enugu.10
Muthuphei analysed 72 liver biopsies from children in Ga-Rankuwa Hospital, South
Africa and found schistosomiasis in 7 (9.7%) and tuberculosis in 2 (2.8%).22
Schistosomiasis is the leading cause of hepatic granulomas in Saudi Arabia
accounting for 54% of cases in one study.20 Amarapurkar et al studied the livers of
60 HIV positive autopsies in Mumbai, India. On histological examination of the livers,
tubercular granulomas were seen in 19 (31.6%) cases of disseminated tuberculosis.
Granulomas were typical caseating epithelioid cell type in 14 (73.6%) and in 5 cases,
granulomas were not typical. Acid fast bacilli were demonstrated in 4 (6.6%) cases,
all of which showed presence of granulomas.23
3. ALCOHOLIC LIVER DISEASE
The clinical spectrum of alcoholic liver disease consists of fatty change, hepatitis and
cirrhosis. Alcohol is the leading cause of liver cirrhosis in the developed countries
while infection with hepatitis B and or C is mainly responsible for progressive liver
disease in most of Africa.24
Ndububa et al investigated the contribution of alcohol to chronic liver disease at Ile-
Ife and reported that alcoholic liver disease made up 6 (14.4%) of the 145 patients
studied. Three of these alcoholic liver disease patients had cirrhosis while the other
three had hepatitis. Histologically, these patients’ liver biopsies showed the

9
characteristic features of centrilobular polymorphonuclear infiltrates, centrilobular
hepatocyte swelling, ballooning degeneration, macrovesicular steatosis and Mallory
bodies (hyaline bodies).25
4. NON ALCOHOLIC FATTY LIVER DISEASE (NAFLD)
Non-alcoholic fatty liver disease (NAFLD) is an increasingly recognised condition
which may progress into end stage liver disease. The pathological picture resembles
that of alcohol induced injury but it occurs in patients who do not abuse alcohol. It is
a spectrum of liver damage ranging from steatosis to steatohepatitis, advanced
fibrosis and cirrhosis. Non-alcoholic fatty liver disease is frequently found in patients
undergoing liver biopsy for an unexplained abnormal liver function studies. It has
been associated with obesity, type 2 diabetes, hyperlipidaemia, hyperinsulinemia and
insulin resistance. Some children with type 1 diabetes mellitus have been found with
NAFLD.26
Ndububa et al in Ile-Ife, reported 2 (1.4%) histologically diagnosed cases of non-
alcoholic fatty liver disease in their study.25 The liver biopsy features include
steatosis, mixed inflammatory cell infiltrate, hepatocyte ballooning and necrosis,
glycogen nuclei, Mallory’s hyaline, and fibrosis.26
5. LIVER CIRRHOSIS
Cirrhosis is a diffuse bridging fibrosis with on-going necroinflammation and attempt
at regeneration with nodule formation.1 Cirrhosis is often asymptomatic or
associated with only mild clinical symptoms. It is the final common pathway for most

10
liver diseases. Although cirrhotic persons can lead relatively normal lives for several
years, they are at a high risk for liver decompensation and progression to
hepatocellular carcinoma.1
It is the eighth leading cause of death in adults worldwide, responsible for 382, 000
deaths in the year 2002 according to the World Health organisation 2003 world
health report.27 Abdulkareem et al reported 17.7% cirrhosis in 345 liver biopsy
specimens examined in Lagos.28 Similar studies in Jos and Ife showed cirrhosis
accounting for 28% and 41.38% respectively25,29.
Similarly, Adeniji et al studied 251 liver biopsy specimens at Ilorin and found that
cirrhosis constituted 35 (13.9%) of the total. Forty per cent were macronodular
cirrhosis while 11.4% were micronodular.30 This figure is lower than the reports from
Lagos and Jos.
In terms of ranking of diagnostic entities, the findings from Lagos and Jos are similar
because cirrhosis ranked third after hepatocellular carcinoma and chronic hepatitis in
both locations.
Liver cirrhosis which has progressed to hepatocellular carcinoma is depicted by the
presence of the two conditions on biopsies from the same patient. Echejoh et al
found cirrhosis co-existing with hepatocellular carcinoma in 27.4% of 53 cases of
cirrhosis studied. The other 72.6% consisted of cirrhosis alone.29
Other disease conditions may also be seen on biopsy from cirrhotic patients. Falaiye
et al reported a case of a 45 years old farm worker who presented at Lagos
University Teaching Hospital with hepatomegaly. Investigation showed amoebic liver

11
abscess. Furthermore, biopsy revealed cirrhosis with patchy destruction of the liver
parenchyma separated by bands of fibrosis.31
6. BENIGN NEOPLASMS
Benign epithelial tumours of the liver include liver cell adenoma, bile duct adenoma,
bile duct cystadenoma and biliary papillomatosis. The non-epithelial tumours include
haemangioma and angiomyolipoma. Tumour–like lesions which occur in the liver are
cysts, focal nodular hyperplasia, nodular regenerative hyperplasia and peliosis.
Benign tumours of the liver are rare and not commonly found compared with the
malignant ones. Only one (0.6%) each of bile duct adenoma,
haemangioendothelioma and cavernous haemangioma were reported in a study in
Jos.9
6.1. HEPATIC ADENOMA
Hepatic adenoma is histologically composed of benign appearing hepatocytes
arranged in plates of one or two cells in thickness and they are most frequently
found in premenopausal women who have used oral contraceptives.1 Hepatic
adenomas have rarely been seen in men who have been on steroids or diagnosed
with glycogen storage diseases type I or III. Three cases of hepatic adenoma
occurring in males were reported from New Zealand.32 Nine cases of hepatic
adenoma were reported in Korea between 1987 and 2001. Interestingly, six of these
patients were males and three, females.33

12
7. MALIGNANT NEOPLASMS
Liver cancers occur worldwide and contribute immensely to morbidity and mortality.
Malignant tumours of the liver may be primary or metastatic.
Mandong et al reported cancer of the liver as the fourth most common of all
malignant tumours in Jos between 1985 and 1994 but it dropped to become the fifth
in the next study period of 1995 – 2002. The most common cancers were those of
the breast followed by cervix and prostate.34 From Sokoto, Malami and colleagues
reported a low figure of 9 (2.2%) liver cancers in males and none in females out of a
total of 298 cancers diagnosed from 1999 to 2004.35
7.1. HEPATOCELLULAR CARCINOMA (HCC)
Hepatocellular carcinoma which is the most common form of primary liver cell
carcinoma represents the fifth most common cancer in the world and the third most
frequent cause of mortality among cancer patients.36 According to global cancer
statistics, it was responsible for more than 500,000 deaths and more than 600,000
new cases worldwide. This tumour has the highest occurrence in South East Asia
and sub-Saharan Africa (120/100,000) and lowest in the USA (1.8/100, 000).36,37,38
One of the earliest papers on hepatocellular carcinoma in Nigeria emerged from
Ibadan in 1967 and was published in the British Journal of Cancer. It was a report
by Williams and colleagues, of four cases of childhood hepatocellular carcinoma seen
at the University College Hospital (UCH).39
A study of 227 liver biopsy specimens in Jos within a ten-year period (1995-2004)
showed a frequency of 71 (31.3%) hepatocellular carcinoma. There were 25

13
(40.4%) females and 46 (27.9%) males. The highest numbers of patients (29.6%)
were between the age ranges of 41-50 years.9 Similarly, primary liver cell carcinoma
was seen in 27% of liver biopsies examined in Kano.11
A prospective study of 100 histologically confirmed cases of HCC in Maiduguri, north
eastern Nigeria showed the highest prevalence among those aged 40-58 years and a
male to female ratio of 4:1.40 Osuafor et al found hepatocellular carcinoma to
constitute 38 (24.6%) of 154 liver biopsies. This was the most common histologically
diagnosed liver pathology at Enugu.10
Malignant tumours of the liver accounted for 105 (14.7%) of 713 malignant tumours
of gastroenterological organs studied in Lagos by Abdulkareem et al. Hepatocellular
carcinoma constituted 75% of these 105 cases.41 In a study aimed at evaluating the
temporal and biological trends in liver cancers in south western Nigeria, Otegbayo et
al analysed 1234 cases of histologically confirmed liver cancers seen at Ibadan for a
period of over two decades. Hepatocellular carcinoma accounted for 92% of these
cases demonstrating that it is the predominant liver cancer in the south west. The
peak age incidence occurred in the fifth decade and the male /female ratio was
2.5:1 42 similar to the findings in Jos.43
Adeniji et al noted hepatocellular carcinoma to be the most common malignant
tumour of the liver at Ilorin because it constituted 63.7% of all malignant tumours of
the liver in a series of 251 biopsy specimens.44 A similar study done by Seleye-
Fubara and colleagues in Port Harcourt showed HCC making up 3.6% of 2105
malignancies. The highest frequency occurred in the age range 40-49 years and a
male to female ratio of 2:1 similar to previous observations. The trabecular pattern

14
was the most common histological type (49.3%) followed by the
pseudoglandular/acinar pattern (28%).45
Four major aetiological factors associated with HCC have been established. These
are chronic viral infection (HBV, HCV), chronic alcoholism, non-alcoholic
steatohepatitis (NASH) and food contaminants (primarily aflatoxins).1 Benvegnu et al
investigated the pattern of hepatocellular carcinoma development in hepatitis B virus
and hepatitis C virus related cirrhosis in Italy. Four hundred and one patients with
cirrhosis were followed up for 14 – 189 months. Eight (16%) out of 50 HBsAg
positive and 53 (18.7%) out of 284 anti-HCV positive patients developed HCC during
follow-up. On the basis of ultrasound or computed tomography scans, two
morphologic patterns were observed in this study. HCC developed as a nodular type
in 81.8% while an infiltrating mass was found in 18.2% of the patients. Older age,
longer duration and more advanced stage of cirrhosis were all significantly
associated with increased risk of developing nodular but not infiltrating HCC. On the
other hand, male sex, HBsAg positivity and dual HBsAg and anti-HCV positivity were
significant risk factors for development of infiltrating but not nodular HCC.46
The National Cancer Institute Pathology Registry in Egypt shows that HCC make up
11.75% of the malignancies of all digestive organs and 1.68% of total malignancies.
The report of El Zayadi’s study of 2005 shows a rising incidence of HCC in Egypt
which has been explained by the increasing prevalence of the risk factors such as
the emergence of HCV, HBV, improvements in screening programs and diagnostic
tools. The increased survival of cirrhotic patients giving time for progression to HCC
was also noted.47

15
The carcinogenic effect of aflatoxin on hepatocytes following chronic exposure is well
documented by the International Agency for Research on Cancer (IARC).48 Kuniholm
et al reported that moderate and high lifetime groundnut consumption in The
Gambia was associated with 2-fold and 3-fold increase in the risk of cirrhosis and by
extension, an increased risk of acquiring hepatocellular carcinoma.17 In Nigeria,
33% of maize samples from different agro-ecological zones were observed to be
contaminated with aflatoxin49.
Aflatoxin B1 is metabolised by cytochrome p450 enzymes to its reactive form, AFB1-
5-9-oxide. It binds covalently with DNA at the N7 position of guanine causing G:C
>> T:A transversion in codon 249ser of p53 gene. This results in the amino acid
substitution of arginine with serine. This p53 mutation is more frequent in countries
where there is also increased exposure to HBV suggesting a synergism between
AFB1 and HBV in the aetiology of HCC.50
Igetei et al in a pioneering study of p53 codon 249 mutations in HCC patients in
south western Nigeria used cell-free DNA. Evaluation of the 79 plasma samples from
the HCC patients through restriction fragment length polymorphism revealed
mutation in 7.6% of them. This figure is lower than what is reported from Asia and
other sub-Saharan countries. The authors attributed this to the staple food of this
region that is based mainly on tubers. Perhaps a higher figure will be obtained from
the northern part of the country where the diet consists mainly of groundnuts and
grains. This study also revealed a younger age (34.5±11.64 years) of the patients
with p53 mutations.51 This is similar to observations in Asia and The Gambia
suggesting synergism with HBV.52,53

16
7.2. HEPATOBLASTOMA
Hepatoblastoma accounts for 0.2-5.8% of malignancies in childhood but 25 -45% of
all primary liver cell tumours, and forms about 50% of those that are malignant.
Eighty three to 92% occur before the age of five and 66% are seen within the first
two years of life.54 Otegbayo et al42 reported a 0.24% frequency of hepatoblastoma
at Ibadan, while 0.9% was recorded in Jos.9
7.3. CHOLANGIOCARCINOMA
Cholangiocarcinoma is a much less common cancer arising from the common bile
duct cells.
Cholangiocarcinoma formed 1.9% of 154 liver biopsies at Enugu. In that same
study, hepatocellular carcinoma constituted 24.6%.10 At Ibadan, cholangiocarcinoma
constituted 15 (1.2%) compared with 1136 (92%) hepatocellular carcinoma out of
1234 liver cancers.42 Other rare cancers reported in the Ibadan study include
lymphoma (0.16%) and hepatoblastoma (0.24%).42
7.4. METASTATIC TUMOURS
Three (4.8%) females and 6 (3.6%) males out of 227 liver biopsies in Jos were
found to have metastatic adenocarcinomas. One metastatic nephroblastoma was
seen in this study.9 Metastatic carcinoma accounted for 12 (54.5%) males and 10
(45.5%) females of 1,234 liver cancer cases studied at Ibadan.42

17
CHAPTER FOUR
METHODOLOGY
This study is retrospective and hospital based. In this study, the archival records and
materials of liver biopsy specimens accessioned in the Histopathology laboratory of
Jos University Teaching Hospital were analysed. The hospital receives close to 2,500
specimens annually.
Materials and Methods
The materials for this study consisted of the archival records of liver biopsy
specimens submitted at the Department of Histopathology, Jos University Teaching
Hospital, from January 2000 to December 2009.
The age, sex, diagnoses and other relevant information were obtained from the
records. Serological test results for hepatitis B surface antigen were obtained from
the clinical records. In diagnosed cases where additional information was needed,
like in the cases of chronic hepatitis and cirrhosis without staging and grading, the
tissue blocks were retrieved, re-sectioned and stained with haematoxylin and eosin.
Special stains such as Masson’s trichrome, Gordon and Sweet’s silver impregnation
and Perls’ Prussian blue were also employed.
World Health Organisation histological classification of tumours of the liver and
intra-hepatic bile ducts (2000) was used in this study50 (Appendix A). The
histological activity in hepatitis and cirrhosis was assessed with the Knodell scoring
system (Appendix B).

18
Statistical Analysis
Descriptive data obtained in this research were expressed as number, proportion,
and mean ± SD (standard deviation). The results of analysis of the different
diagnostic entities were presented on age and sex distribution tables. One way
analysis of variance (ANOVA) was computed to ascertain if there was any statistically
significant gender differences in the Knodell scores in chronic hepatitis and cirrhosis
based on assumptions of normality of distribution and parametric statistics.
Pearson’s correlation analysis was performed to determine the relationship between
age and Knodell scores obtained in chronic hepatitis. All statistical computations
were performed using Microsoft Excel (2007 version).
Inclusion Criteria
All available records of specimens submitted and reported at the department of
histopathology, Jos University Teaching Hospital, from January 2000 to December
2009 inclusive were used.
Exclusion Criteria
The entries of liver biopsy specimens not showing the complete records were
excluded in this analysis. Liver fine needle aspiration biopsy and cytology records
were also not used because they could not be scored or graded.
Ethical Clearance
The Ethical Committee of the Jos University Teaching Hospital granted ethical
clearance for this study.

19
CHAPTER FIVE
RESULTS
Annual Distribution of Liver Biopsy histological Diagnoses
There were three hundred and ninety one liver biopsy specimens accessioned in Jos
University Teaching Hospital from January 2000 to December 2009. Seventeen of
them were assessed to be inadequate and were not included in this analysis. These
included specimens which were necrotic, not properly fixed or processed, or with
less than five portal regions. Therefore, three hundred and seventy-four specimens
were analysed in this study.
As shown in figure 1, there was an increasing trend from 16 specimens in 2000 to
56 in 2005. A sudden decline occurred in 2006 before rising to a plateau between
2007 and 2008 with 78 and 79 specimens respectively. A sudden decrease was
again noted in 2009.
Liver diseases were generally observed to be more common in males than females.
There were a total of 245 (65.5%) males and 129 (34.5%) females with a male to
female ratio of 1.9:1.
The biopsy specimens were from patients with ages ranging from 4 months to 81
years. Most of the cases occurred within the 31 – 40 years age bracket. Seventy-
seven males and 47 females seen in this age group gave a total of 124 which
accounted for 33.2% of the total number of liver specimens. This was closely
followed by the preceding decade (21-30 years age group) which had 104 (27.8%).
Liver diseases occurred more in males (73) than in females (31) within this age

20
group. Next, the 41-50 years age group had 47 males and 20 females which
altogether formed 17.9%. Eight (2.1%) children between 0 – 10 years old had liver
diseases. However, at the other extreme of age, only a male older than 80 years
was found (table 1). Analysis of the various histologically diagnosed liver diseases
demonstrated that chronic hepatitis, hepatocellular carcinoma and cirrhosis occurred
frequently (table 2).
The most frequently diagnosed liver disease was chronic viral hepatitis with 228
(61%) out of the total of 374 liver disease specimens. Hepatocellular carcinoma
occurred about three times less frequently than chronic viral hepatitis. There were
76 (20.3%) cases of this malignant tumour.
Cirrhosis was significantly noted to be much less frequent with 29 (7.8%) cases seen
during this ten year period.
Other less frequent observations include liver with normal histology (4%) and
steatosis (1.9%). Figure 3 shows a case of hepatic steatosis. There were four cases
(1.1%) each of hepatoblastoma and metastatic adenocarcinoma to the liver.
Cholangiocarcinoma, non-alcoholic fatty liver disease, polycystic liver disease and
schistosomiasis were each diagnosed twice (0.5%). Conditions with only a single
case (0.3%) reported include capillary haemangioma, cavernous haemangioma,
focal nodular hyperplasia, haemangioendothelioma and tuberculosis (table 2).

21
Chronic hepatitis
Chronic hepatitis occurred most frequently in the fourth decade with 87 (38.2%) out
of 228 biopsies from patients within this age group. Chronic hepatitis occurred
predominantly in males with a male: female ratio of 1.9:1. The peak occurrence was
in the 31-40 years age group (table 3).
Hepatitis B virus (HBV) infection was responsible for 219 (96.1%) cases of chronic
hepatitis. All the hepatitis B virus cases were also positive for hepatitis B surface
antigen on serological testing. This information was obtained from the clinical
records. Figure 4 shows a case of chronic hepatitis due to hepatitis B virus infection.
There were five cases of hepatitis C viral infection while co-infection with hepatitis B
virus was present in four (1.8%).
Distribution of Knodell scores in chronic hepatitis.
The histological activity index in chronic hepatitis and cirrhosis was assessed using
the Knodell scoring system. The age and sex distribution of the Knodell scores
obtained in the slides diagnosed with hepatitis B virus infection is presented on
Table 4. The scores were arbitrarily grouped into 1-4, 5-8, 9-12, 13-18 and 19-22
points based on previous studies 13,55. The highest frequency (51.1%) was obtained
in those cases with scores between the ranges of 5-8 points. This was followed by
Knodell scores of 1-4 points, constituting 29.2%. Only two (0.9%) out of the 219
histologically diagnosed cases of chronic hepatitis B virus infection were scored 13-
18 points.

22
Cirrhosis
There were 29 cases of liver cirrhosis and their peak incidence paralleled that of
chronic hepatitis. Fourteen (48.3%) of them occurred within the 31-40 age bracket
and this was followed by the third decade (20.7%) similar to what was observed in
chronic hepatitis (Table 5). Figures 5, 6, and 7 show cases of liver cirrhosis.
Distribution of Knodell scores in cirrhosis
Slightly more than half (51.7%) of the cirrhosis cases had Knodell scores between
13 to 18 points. Thirty-four point five per cent were scored 9-13 points while 13.8%
were scored 5-8 points. In this study, there was no case of cirrhosis with a Knodell
score beyond 18 points (Table 6). Higher scores were obtained in the cases of
cirrhosis with a mean of 13.7±3.2 when compared with non-cirrhotic cases which
had a mean of 6.6±2.6.
Analysis of effect of gender on Knodell Scores in chronic hepatitis and
cirrhosis
The Knodell scores in males with chronic hepatitis B virus infection averaged 6.6 ±
2.5. There was a slightly higher mean of 6.8 ± 2.6 in females. Similarly, males had
lower mean scores (13.0 ± 3.4 S.D.) than females (15.3 ± 2.3) in cirrhosis (Table
7).

23
One-way analysis of variance (ANOVA) was performed to determine if there was a
statistically significant effect of gender on necro-inflammation and fibrosis, based on
the Knodell scores obtained, in chronic hepatitis and cirrhosis.
In chronic hepatitis B infection, the calculated variance ratio, F (0.23) was less than
the critical F value (6.75). In addition, the p-value computed, 0.63 is more than the
significance level for alpha (α), 0.01. Hence, the null hypothesis (Ho: µ male Knodell
scores = µ female Knodell scores) was not rejected. Therefore, there was no
statistically significant difference between the male and female scores in chronic
hepatitis B viral infection (Table 8).
Similarly, in cirrhosis, the calculated variance ratio, F (0.99), was less than the
critical F value (7.68) and the p-value, 0.033, is more than the alpha level of
significance (α) of 0.01. Hence, the null hypothesis (Ho: µ male Knodell scores = µ
female Knodell scores) was not rejected. Therefore, there was no statistically
significant difference between the male and female scores in cirrhosis (Table 8).
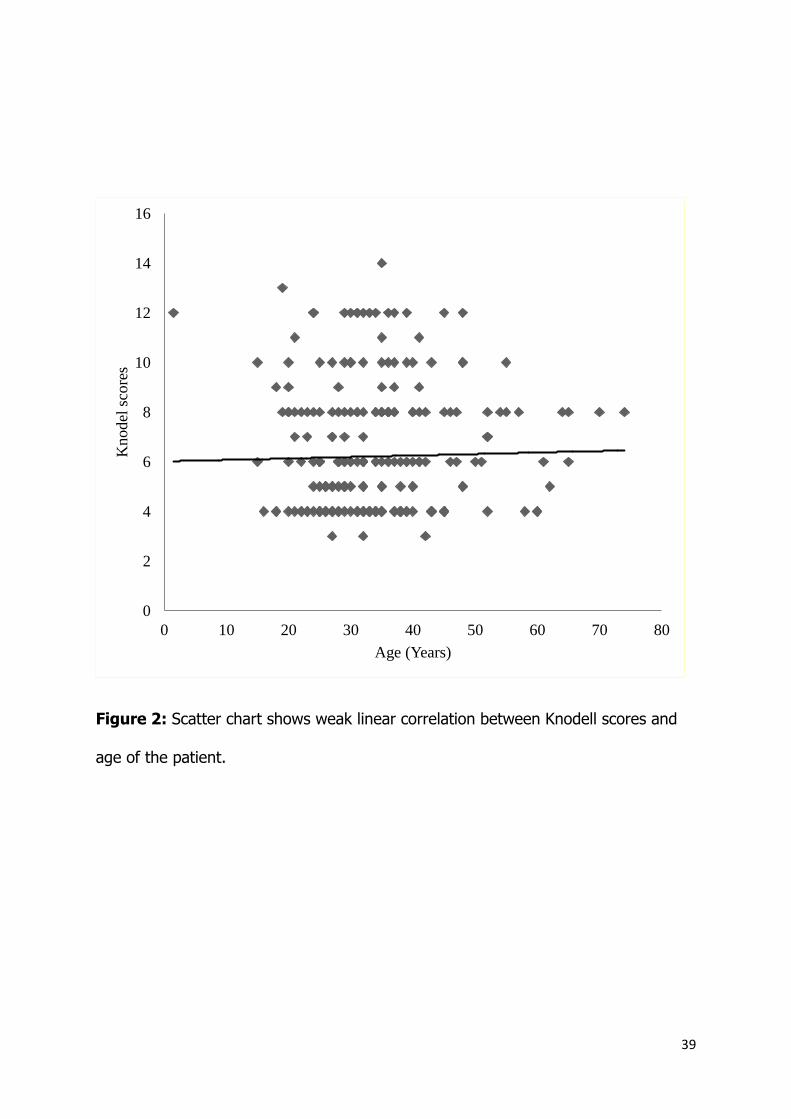
Correlation analysis of Knodell scores and age in chronic hepatitis
Pearson’s correlation analysis of age and all the Knodell scores in chronic hepatitis B
viral infection returned the value, r = 0.0067. With a degree of freedom (df) of 217,
there was a two tailed P-value of 0.9218 and one-tailed value of 0.4609. Pearson’s r
value is much less than both the two-tailed and one-tailed P-values. Therefore, there
was a weak positive linear correlation between the age of the patient and the degree

24
of liver damage. The scatter chart below illustrates this weak relationship between
the Knodell scores and the age of the patients (Figure 2).
Benign and malignant tumours
The benign tumours seen in this study included a case each of capillary
haemangioma, cavernous haemangioma, focal nodular hyperplasia; and two cases
of polycystic liver disease. They all make up 1.3% of the total biopsy specimens.
Eighty-eight malignant tumours were present, constituting 22.5% of the 391 total
number of biopsy specimens. Hepatocellular carcinoma was the most common and
made up 86.4% of the malignant tumours. This was followed by metastatic cancer
(5.7%), hepatoblastoma (4.5%), cholangiocarcinoma (2.3%) and
haemangioendothelioma (1.1%) (Table 9).
Hepatocellular carcinoma
There were 76 cases of hepatocellular carcinoma, 50 males and 26 females giving a
male to female ratio of 1.9:1 similar with the observation in chronic hepatitis B virus
infection. These have an average age of 46.2 ±13.9 years. The peak frequency
(30.3%) occurred in the 41-50 year age group with 17 males and 6 females (Table
10). Figures 8, 9 and 10 show cases of hepatocellular carcinoma.

25
Morphological patterns of hepatocellular carcinoma
The distribution of the various histological patterns of hepatocellular carcinoma
showed a preponderance of the trabecular pattern, which constituted 71.1% of the
total 76 cases of hepatocellular carcinoma studied. The proportion of males (4.7%)
with this pattern is more than twice that in females (22.4%). In addition, most of
them are males within the fifth decade. The next common pattern is the
acinar/pseudoglandular occurring in 13.2% of the cases. There was combined
occurrence of trabecular and acinar pattern in 7.9% of the cases. Other variants
include the clear cell (6.6%), and fibrolamellar (1.3%). There was only one case of
fibrolamellar pattern occurring in a 43 years old male. Overall, most of the
hepatocellular carcinoma cases were trabecular patterns in males within the fifth and
sixth decade (table 10).
Co-existence of hepatocellular carcinoma with other disease conditions
Hepatocellular carcinoma may co-exist with other conditions. In this study, 18
(23.7%) were cases of this cancer arising on a background of cirrhosis. However, a
larger proportion (75%) existed in isolation without observable combination with any
other disease condition. The males within this group alone made up half of the total
cases of this cancer (Table 11).
Cholangiocarcinoma
There were two cases of cholangiocarcinoma in 15 and 64 years old males, both of
which made up 0.5% of the total liver biopsy specimens.

26
Hepatoblastoma
The four cases of hepatoblastoma observed occurred in children between the ages
of 7 and 9 years with a mean of 8.3 ± 0.96 years. There was a nine years old
female and the remaining were males.
Metastases
Five cases of metastases were seen, four males and one female all constituting
1.1% of the total biopsies. The age range was 32-81 years. They were all cases of
metastatic adenocarcinoma. Figure 11 shows a case of metastatic adenocarcinoma.

27
Table 1: Age and sex distribution of liver biopsies
Age (Years) Male Female Total
Percentage
(%)
0-10 5 3 8 2.1
11-20 9 8 17 4.5
21-30 73 31 104 27.8
31-40 77 47 124 33.2
41-50 47 20 67 17.9
51-60 19 14 33 8.8
61-70 10 5 15 4.0
71-80 4 1 5 1.3
81-90 1 0 1 0.3
Total
245
(65.5%)
129
(34.5%) 374 100.0

28
Table 2: Sex distribution of liver diseases diagnosed by histology
Diagnosis Male Female Total Percentage (%)
Normal Liver 9 6 15 4.0
Inflammatory Diseases
Chronic Viral Hepatitis 149 79 228 61.0
Tuberculosis 1 0 1 0.3
Schistosomiasis 1 1 2 0.5
Metabolic Diseases
Steatosis 5 2 7 1.9
Other Conditions
Liver Cirrhosis 20 9 29 7.8
Benign Tumours and Tumour-like Conditions
Polycystic Liver Disease 0 2 2 0.5
Focal Nodular Hyperplasia 0 1 1 0.3
Capillary Haemangioma 0 1 1 0.3
Cavernous Haemangioma 1 0 1 0.3
Primary Malignant Tumours
Hepatocellular Carcinoma 50 26 76 20.3
Cholangiocarcinoma 2 0 2 0.5
Hepatoblastoma 3 1 4 1.1
Haemangioendothelioma 1 0 1 0.3
Metastatic Tumours
Adenocarcinoma 3 1 4 1.1
Total (Percentage) 245 (65.5%) 129 (34.5%) 374 100.0

29
Table 3: Age and sex distribution of chronic hepatitis
Age (Years) Male Female Total Percentage (%)
0-10 1 0 1 0.4
11-20 8 6 14 6.1
21-30 51 22 73 32.0
31-40 56 31 87 38.2
41-50 23 10 33 14.5
51-60 6 7 13 5.7
61-70 4 3 7 3.1
Total 149 79 228 100.0

30
Table 4: Age and sex distribution of Knodell scores in chronic hepatitis B virus
(HBV) infection
Age (Years)
Knodell Scores
Total Percentage (%) 1-4 5-8 9-12 13-18
M F M F M F M F
0-10 0 0 0 0 1 0 0 0 1 0.5
11-20 3 1 1 4 3 1 1 0 14 6.4
21-30 16 5 28 12 6 5 0 0 72 32.9
31-40 19 8 24 15 11 6 1 0 84 38.4
41-50 4 4 12 2 4 3 0 0 29 13.2
51-60 1 3 3 4 1 0 0 0 12 5.5
61-70 0 0 3 3 0 0 0 0 6 2.7
71-80 0 0 1 0 0 0 0 0 1 0.5
Total 43 21 72 40 26 15 2 0 219 100.0
M: male, F: female

31
Table 5: Age and sex distribution of liver cirrhosis
Age (Years) Male Female Total Percentage
11-20 0 1 1 3.4
21-30 5 1 6 20.7
31-40 11 3 14 48.3
41-50 3 2 5 17.2
51-60 0 2 2 6.9
61-70 1 0 1 3.4
TOTAL 20 (69%) 9 (31%) 29 100.0

32
Table 6: Age and sex distribution of Knodell scores in cirrhosis
Knodell scores
1-4 5-8 9-12 13-18
Age (Years) M F M F M F M F Total Per cent (%)
0-10 0 0 0 0 0 0 0 0 0 0.0
11-20 0 0 0 0 0 1 0 0 1 3.4
21-30 0 0 2 0 1 0 2 1 6 20.7
31-40 0 0 0 1 6 1 4 2 14 48.3
41-50 0 0 0 1 1 0 1 2 5 17.2
51-60 0 0 0 0 0 0 0 2 2 6.9
61-70 0 0 0 0 0 0 1 0 1 3.4
71-80 0 0 0 0 0 0 0 0 0 0.0
Total 0 0 2 2 8 2 8 7 29 100.0
M: male, F: female

33
Table 7: Knodell scores mean and standard deviation in chronic hepatitis B viral
infection and cirrhosis.
Sex
Hepatitis B Virus Infection Cirrhosis
Mean Score S.D. Mean Score S.D.
Male 6.6 2.5 13.0 3.4
Female 6.8 2.6 15.3 2.3

34
Table 8: Analysis of variance (ANOVA) tables for male and female Knodell scores
from chronic hepatitis and cirrhosis
Chronic hepatitis B infection
ANOVA
Source of
Variation SS Df MS F P-value F crit
Between Groups 1.52 1 1.52 0.23 0.63 6.75
Within Groups 1417.48 217 6.53
Total 1419.00 218
Cirrhosis
ANOVA
Source of
Variation SS Df MS F P-value F crit
Between Groups 108.91 1.00 108.91 0.99 0.33 7.68
Within Groups 2985.09 27.00 110.56
Total 3094 28
SS: sum of squares; df: degree of freedom; MS: mean sum of squares; F: F value;
P-value: calculated probability value; F crit: tabulated critical F value.

35
Table 9: Frequency of distribution of liver cancer types by sex
Diagnosis
Sex
Total Percentage (%) Males Females
Hepatocellular Carcinoma 50 26 76 86.4
Cholangiocarcinoma 2 0 2 2.3
Hepatoblastoma 3 1 4 4.5
Haemangioendothelioma 1 0 1 1.1
Metastases 4 1 5 5.7
Total 60 28 88 100.0

36
Table 10: Age and sex distribution of the patterns of hepatocellular carcinoma
Trabecular Acinar Trabecular and
Acinar
Clear Cell Fibrolamellar Total
Age M F M F M F M F M F Sum %
<10 0 1 0 0 0 0 0 0 0 0 1 1.3
11-20 0 0 0 0 0 0 0 0 0 0 0 0.0
21-30 5 2 2 0 0 0 0 2 0 0 11 14.5
31-40 4 5 2 1 0 1 0 1 0 0 14 18.4
41-50 12 4 2 1 1 1 1 0 1 0 23 30.3
51-60 10 3 1 0 1 2 0 0 0 0 17 22.4
61-70 3 2 0 0 0 0 1 0 0 0 6 7.9
71-80 3 0 1 0 0 0 0 0 0 0 4 5.3
Total 37 17 8 2 2 4 2 3 1 0 76 100

37
Table 11: Distribution of hepatocellular carcinoma (HCC) co-existing with cirrhosis
Diagnosis Male % Female % Total Cases Percentage
HCC alone 39 51.3 19 25 58 76.3
HCC and Cirrhosis 11 14.5 7 9.2 18 23.7
Total 50 65.8 26 34.2 76 100

38
Figure 1: Histogram showing the annual distribution of the number of liver biopsy
specimens in Jos University Teaching Hospital from January 2000 to December 2009.
The percentages indicated represent the proportion of the total number of liver
specimens (374) analysed in this study.
16(4.3%) 11(2.9%)
23(6.1%) 19(5.1%)
32(8.6%)
56(15%)
31(8.3%)
78(20.9%) 79(21.1%)
29(7.8%)
0
10
20
30
40
50
60
70
80
90
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009
Num
ber
of
bio
psi
es
Year
39
Figure 2: Scatter chart shows weak linear correlation between Knodell scores and
age of the patient.
0
2
4
6
8
10
12
14
16
0 10 20 30 40 50 60 70 80
Knodel
sco
res
Age (Years)

40
Figure 3: Photomicrograph of fatty liver in a 42 years old male. Many of the
hepatocytes have cytoplasmic microvesicles. These have coalesced in some of the
cells to form large fat vacuoles appearing as round clear spaces pushing the nuclei
peripherally (H & E, X 20).

41
Figure 4: Photomicrograph of hepatitis B virus infection exhibiting portal
inflammation, piecemeal necrosis, ballooning of hepatocytes with inflammatory cells
extending into the parenchyma (H & E, X10).
Inset: Some of the hepatocytes have pale, eosinophilic relatively finely granular
cytoplasm (ground glass appearance) and eosinophilic granules in the nuclei (sanded
nuclei). Lymphocytes are seen on the right infiltrating the liver parenchyma from a
portal region (H & E, X 40).

42
Figure 5: Photomicrograph of liver cirrhosis showing thick fibrous bands
surrounding nodules of regenerated hepatocytes (H & E, X 4).

43
Figure 6: Photomicrograph of liver cirrhosis. Abnormal deposition of reticulin fibres
and irregularity of hepatocyte plates is demonstrated in this reticulin silver
impregnation stain (Gordon and Sweet, X 10).

44
Figure 7: Photomicrograph of liver cirrhosis. This is a trichrome stain showing an
increased deposits of collagen within the fibrous bands separating lobules of
hepatocytes (Masson's trichrome, X 10)

45
Figure 8: Photomicrograph of hepatocellular carcinoma arising on a background of
cirrhosis. A vascularised fibrous band is present in the middle of the field. The
neoplastic cells are in sheets and irregular cords which are several cells thick. The
cells have increased nucleo-cytoplasmic ratio and striking pleomorphism. Most of the
cells have vesicular nuclei with prominent nucleoli (H & E, X40)

46
Figure 9: Photomicrograph of hepatocellular carcinoma, trabecular pattern. The
malignant cells are arranged in thick irregular trabecula (H & E, X 20).

47
Figure 10: Photomicrograph of hepatocellular carcinoma, acinar/pseudoglandular
pattern. These malignant cells are forming gland-like structures (H & E, X 40).

48
Figure 11: Photomicrograph showing metastatic adenocarcinoma in a 65 years
male (H & E, X 40).

49
CHAPTER SIX
DISCUSSION
The liver biopsy specimens used in this study cut across the different age groups, in
both sexes. The ratio of adults to children is 49:1. This is higher than the finding in
previous liver biopsy reports both in Jos, Enugu and Lagos10, 28, 29.
The incidence of liver diseases in males has been noted to be higher than in
females. In this study, the male to female ratio is 1.9:1. This ratio compares
favourably with the observations of Ndububa et al and Abdulkareem et al who both
reported 1.8:1 and it is significantly less than 3:1 reported by Osuafor and
colleagues10, 13, 28.
The most common diagnoses were chronic hepatitis, followed by hepatocellular
carcinoma and cirrhosis. A similar finding was reported in Kano11. Meanwhile, in the
east and south west, hepatocellular carcinoma consistently occurred most frequently
in different studies10,28,30.
The peak incidence of chronic hepatitis occurred in the 31-40 years age group in Jos.
This observation is consistent with reports by other workers9, 28. Most of the patients
are males and had Knodell scores ranging from five to eight points signifying mild
necro-inflammatory activity (Table 5). The older patients did not demonstrate a
greater degree of liver damage and Pearson correlation analysis returned a weak
linear correlation between Knodell scores and age. Perhaps, a further study with a
larger sample size, correlating the scores and duration of illness will give a significant
statistical result and computing with the duration of infection may predictably yield

50
the strongest positive correlation. Poynard et al found acceleration of fibrosis with
increasing age in a series of 4,852 patients with chronic liver diseases56. Older age at
diagnosis appears to be an important determinant of progression to cirrhosis and
hepatocellular carcinoma. This may be caused by the aging of the immune system
which can no longer contain the disease or because of the longer duration of
infection57.
Fibrosis appears to progress more slowly in females than in males with chronic
hepatitis B infection, suggesting that oestrogens have a protective effect on
fibrogenesis56. Rigamonti and colleagues demonstrated the effect of gender on
necro-inflammation. They conducted a univariate and multivariate analysis of the
prognostic variables in chronic hepatitis C and found that gender modulates the
progression of chronic hepatitis C only in younger patients. Women ≤ 50 years
showed lower necro-inflammatory and fibrosis scores than men of comparable age
while men and women >50 years did not exhibit any difference in the severity of the
disease58. In contrast to the observations of these researchers, the analysis of
variance (ANOVA) of the scores obtained from males and females with chronic
hepatitis B, in this study, failed to demonstrate a significant statistical difference
suggesting an insignificant influence of gender on histological activity index. There
has actually been contrasting data on the influence of gender on the risk of
progression of chronic hepatitis57.
The peak incidence of cirrhosis occurred in the fourth decade. This is lower than the
fifth decade reported in Jos and Lagos, and sixth decade observed at Illorin28, 30.

51
The occurrence of hepatocellular carcinoma found in this study (19.4%) is less than
previous observations in Jos (31.3%), Kano (27%), Lagos (33%), and Enugu
(24.6%)10,11,28,43.
The peak occurrence of hepatocellular carcinoma was in the 41-50 years age group,
a decade later than chronic hepatitis and cirrhosis. This concurs with findings in
Lagos, Ibadan, Enugu, Jos and Maiduguri 15, 42, 43, 60, 61.
The predominance of males with hepatocellular carcinoma is confirmed in this study.
This tumour was more common in males (50, 65.8%) than females (26, 34.2%)
giving a male female ratio of 1.9:1. This figure, however, is less than the
observations in Lagos (2.6:1), Maiduguri (2.5:1), Enugu (2.3:1) and Port Harcourt
(2:1)15, 45, 60, 61.
The aetiological factors implicated in hepatocellular carcinoma include viral hepatitis,
chronic alcoholism and aflatoxin exposure, with cirrhosis as the final common
pathway for most of the liver diseases. The significantly low frequency of cirrhosis
(7.8%) compared with chronic viral hepatitis (61%) and hepatocellular carcinoma
(20.3%) portends certain implications. Perhaps, most cases of viral hepatitis in this
region remained asymptomatic until progression to hepatocellular carcinoma. This
observation probably also demonstrates the important role played by other factors
such as aflatoxin in the aetiopathogenesis of hepatocellular carcinoma in our
environment where grains are abundantly consumed and there are no adequate
storage facilities. Synergism between aflatoxin and hepatitis B virus infection in
rapidity of progression to cancer has been previously reported52. In the case control
study conducted by Igetei and colleagues in the south west, all the hepatocellular

52
carcinoma patients who were positive for p53 codon 249 mutation were also positive
for hepatitis B surface antigen (HBsAg) but slightly more than half of the those
negative for this mutation were HBsAg positive suggesting synergism51. Certainly,
more comprehensive information on the contribution of aflatoxin B1 toxicity to liver
disease in this environment will be made available if a study similar to theirs is
performed in other regions of the country.
Cirrhosis was found in this study, to be most common a decade before
hepatocellular carcinoma peak occurrence. Hepatocellular carcinoma occurred in
23.7% of the cases, on a background of cirrhosis. The inference is that the process
leading to the cancer began as an inflammatory condition or otherwise, which
caused diffuse fibrosis with regeneration, a fertile ground for dysplasia and
eventually malignant transformation.
The architectural patterns of hepatocellular carcinoma observed in this study are the
trabecular, pseudoglandular/acinar, acinar and trabecular combined, clear cell and
fibrolamellar. The trabecular pattern, in which the tumour cells grow in cords
separated by sinusoidal blood spaces, was the most common, making up to 71.1%
of the hepatocellular carcinoma cases. Seleye-Fubara and colleagues have reported
the predominance of this histological pattern in Port Harcourt45. They reported
49.3% of 75 hepatocellular carcinoma cases to be of the trabecular pattern, which is
a much lower figure than observed in this study. Similar to the findings in Port
Harcourt, the next common variant is the acinar/pseudoglandular pattern (13.2%).
However, over 50% of the hepatocellular carcinoma cases in Lagos were reported to
be pseudoglandular in pattern60.

53
Other histological patterns of hepatocellular carcinoma not found in this study
include the compact, scirrhous and undifferentiated.
Immunostains distinguish hepatocellular carcinoma from other focal lesions or
malignancies especially cholangiocarcinoma and metastatic adenocarcinoma.
Hepatocellular carcinoma gives a positive result with alpha-fetoprotein, pCEA, Hep-
Par1, glypican 3 and cytokeratin 8-18; and gives negative results with cytokeratin 7,
19 and 20. By contrast, cholangiocarcinoma is positive to cytokeratin 7, 19 and 20,
while metastatic adenocarcinoma is positive only to cytokeratin 20 and negative to
the other immunohistochemical markers61.
The frequency of occurrence of hepatoblastoma (4.5%) is similar to previous reports
in Jos and higher than 2.4% reported at Ibadan by Otegbayo et al and 2% reported
at Lagos by Abdulkareem et al9, 42, 60.
The metastatic tumours observed in this study were all adenocarcinomas and
represented only 1.1% of all the liver biopsies and 5.7% of the malignant
neoplasms. This figure is less than 10% recorded in Lagos and 22% at Ibadan but
higher than 2.6% previously reported in Jos9, 42, 60.
Conclusion
This analysis of 374 histologically diagnosed liver biopsy specimens in Jos
demonstrated that there is high frequency of occurrence of chronic hepatitis and
hepatocellular carcinoma in the north central region of Nigeria. This study showed
an insignificant modulating effect of gender on necro-inflammatory activity and

54
fibrosis progression in chronic hepatitis. However, a weak positive correlation was
observed between disease progression and age. Hepatocellular carcinoma occurred
three times less than chronic hepatitis and the trabecular pattern was found to be
the most common. Despite the increasing popularity of non-invasive modalities of
liver evaluation, liver biopsy will remain, in a long time to come, the most effective
means of evaluation of liver disease especially in a resource-depleted setting.
Recommendations
I wish to make the following recommendations based on the findings of this study
and general observations during the course of this research.
1. There should be an increase in public awareness campaigns to enlighten the
public on the risks of transmission of hepatitis B virus. Health care workers
should adhere strictly to blood handling guidelines.
2. There should be a two pronged approach to the long term prevention of
hepatocellular carcinoma. There should be education of farmers on proper
preservation of food products and implementation of government policy on
provision of storage facilities. This will complement efforts being made
towards vaccination against hepatitis B virus infection.
3. There should be improvement in the synergism between surgeons,
physicians, radiologists and pathologists in the management of patients with
liver diseases. I believe this will increase the diagnostic yield of liver biopsies
and minimise instances of specimen inadequacy and incompletely or
incorrectly filled laboratory request forms.

55
4. Provision of facilities for immunohistochemistry in the histopathology
laboratory of the Jos University Teaching Hospital will greatly enhance
diagnostic accuracy of liver specimens.
5. A future study involving a morphometric correlation of necro-inflammation
and fibrosis with non-invasive markers (liver enzymes, telomere length, etc.,)
will aid in developing a model for accurate prognostication of disease
progression in patients from whom a liver biopsy cannot be obtained.

56
REFERENCES
1. Crawford JM, Liu C. Liver and biliary tract. In: Kumar V, Abbas AK, Fausto N, Aster
JC. Robbin and Cotran Pathologic basis of disease. 8th ed. Philadelphia: Elsevier;
2010.p. 833-890.
2. Sheela H, Seela W, Caldwell C, Boyer JL, Jain D. Liver biopsy: evolving role in the
new millennium. J Clin Gastroenterol 2005; 39:603-610.
3. Siegel CA, Silas AM, Suriawinata AA, Van-Leeuwen DJ. Liver biopsy 2005: when and
how? Cleveland Clin J Med 2005; 72(3):199-224.
4. Geller SA, Pitman MB, Nichols WS. Cellular molecular diagnostic techniques. In: Burt
AD, Portmann BC, Ferrell LD. MacSween’s Pathology of the liver. 5th ed. Philadelphia
(PA), USA: Elsevier; 2007. p. 120-128.
5. Friedman LS. Controversies in liver biopsy: who, where, when, how, why? Current
Gastroenterol Rep 2009; 6:30-36.
6. Piccino T, Sagnelli E, Pasquale G, Giusti G. Complications following percutaneous
liver biopsy. A multicentre retrospective study on 68, 276 biopsies. J Hepatol 1986;
2:165-173.
7. Streinu-Cercel A, Preoţescu L, Streinu-Cercel A, Călin R, Budulac A, Streinu-Cercel O.
Correlations between non-invasive explorations and liver biopsy in the determination
of liver fibrosis in chronic viral hepatitis C. Therap Pharmacol Clin Toxicol
2009;13(3):281-286.
8. Loaeza-del-Castillo A, Paz-Pineda F, Oviedo-Cárdenas E, Sánchez-Ávila F, Vargas-
Vorácková F. AST to platelet ratio index (APRI) for the non-invasive evaluation of
liver fibrosis. Ann Hepatol 2008; 7(4):350-357.

57
9. Echejoh GO, Tanko N M, Manasseh A N, Mandong BM, Ogala-Echejoh SE, Ladep GN
et al. Clinico-pathologic correlation of liver biopsy in Jos, central Nigeria. J Chinese
Clin Med 2007; 2(10):557-562.
10. Osuafor TO, Ikerionwu SE, Ukabam SO. Liver biopsy: experience at Enugu, eastern
Nigeria. Scand J Gastroenterol 1986; 124 Suppl:107S-112S.
11. Samaila AA, Mohammed AZ, Borodo MM, Tijjani BM. Histopathological findings in
liver biopsies and clinical correlation at Kano, Nigeria. Sahel Med J 2008; 11(1):20-
23.
12. Lesi OA, Kehinde MO, Anomneze EE, Wali SS. Hepatitis C infection and risk of chronic
liver disease in Lagos. Nig Q J Hosp Med 2002; 12(1-4):1-5.
13. Ndububa DA, Ojo OS, Adetiloye VA, Durosinmi MA, Olasode BJ, Famurewa OC et al.
Chronic hepatitis in Nigerian patients: a study of 70 biopsy proven cases. West Afr J
Med 2005; 24(2):107-111.
14. Olubuyide IO, Aliyu B, Olaleye OA, Ola SO, Olawuyi F, Malabu UH, et al. Hepatitis B
and C virus and hepatocellular carcinoma. Trans R Soc Trop Med Hyg 1997;91:38-41
15. Ajayi BB, Nggada HA, Moses AE. Hepatocellular carcinoma among patients diagnosed
with and without hepatitis B surface antigenaemia in a Nigerian tertiary hospital. Afr
J Microbiol Res 2007 Dec.1:121-124.
16. Nwokedi EE, Ilyasu Z, Emokpae MA, Dutse AI, Taura AA. Hepatitis C virus infection
among teaching hospital patients in Kano, Nigeria: a retrospective study. Ann Afr
Med 2006; 5(4):185-187.

58
17. Kuniholm MH, Lesi OA, Mendy M, Akano A, Sam O, Hall AJ, et al. Aflatoxin exposure
and viral hepatitis in the etiology of liver cirrhosis in the Gambia, West Africa. Env
Health Perpect 2008; 116(11):1553-57.
18. Strickland GT, Elhefni H, Salman T, Waked I, Abdel-Hamid M, Mikhail NN, et al. Role
of hepatitis C infection in chronic liver disease in Egypt. Am J Trop Med Hyg 2002;
67(4):436-42.
19. Lamps L W. Hepatic granulomas, with an emphasis on infectious causes. Adv Anat
Pathol 2008; 15:309–318.
20. Wainwright H. Hepatic granulomas. Eur J Gastroenterol Hepatol 2007;19:93–95
21. Echejoh GO, Mandong BM, Tanko MN, Manasseh AN, Okeke EN, Agaba EI. Hepatic
histopathological findings in HIV patients at post-mortem in Jos university teaching
hospital, Nigeria. Trop Doct 2006; 36: 228-231.
22. Muthuphei M N. Childhood liver diseases in Ga-Rankuwa hospital, South Africa. East
Afr Med J 2000; 77(9):508-509.
23. Amarapurkar A, Sangle NA. Histological spectrum of liver in HIV - autopsy study. Ann
Hepatol 2005; 4(1):47-51.
24. Mitra AK. Hepatitis C-related hepatocellular carcinoma: Prevalence around the world,
factors interacting, and role of genotypes. Epidemiol Rev 1999; 21(2):180-187.
25. Ndububa DA, Ojo OS, Adetiloye VA, Aladegbaiye AO, Adebayo RA, Adekunle O. The
contribution of alcohol to chronic liver disease in patients from south west Nigeria.
Nig J Clin Pract 2010; 13(4):360-364.
26. Angulo P. Non-alcoholic fatty liver disease. New Engl J Med 2002; 346(16):1221-
1231.

59
27. World Health Organisation. The world health report 2003. Geneva. World Health
Organisation; 2003.p.17. Available from: www.who.int\whr\2003\en\index.html
[accessed on 2rd March, 2011].
28. Abdulkareem FB, Banjo AA, Elesha SO, Daramola AO. Histopathological study of liver
diseases at Lagos University Teaching Hospital, Nigeria (1989-2000). Nig Postgrad
Med J 2006; 13(1):41-6.
29. Echejoh GO, Tanko MN, Manasseh AN, Silas AO, Ogala-Echejoh S, Mandong BM.
Liver cirrhosis in Jos, north central Nigeria. Jos J Med 2008; 3(1):26-29.
30. Adeniji KA, Anjorin AS. Histopathological assessment of the pattern liver cirrhosis in a
tropical population. Afr J Med Med Sci 2002; 31:367-369.
31. Falaiye JM, Okeke GCE, Fregene AO. Amoebic abscess in the cirrhotic liver. Gut
1980; 21:161-163.
32. Ronald M, Woofield J, McCall J, Koea J. Hepatic adenomas in male patients. HPB
2004; 6(1):25-27. DOI: 10.1080/13651 8203 10020846
33. Kim DH, Kim SU, Nam DH, Choi YJ, Park SM, Lee CK, Kim DY. A case of
hepatocellular carcinoma within hepatocellular adenoma in a non-cirrhotic male. Kor
J Int Med 2009; 24(2):147-152. DOI: 10.3904/kjim.2009.24.2.147
34. Mandong BM, Madaki AKJ, Manasseh AN. Malignant diseases in Jos: a follow up. Ann
Afr Med 2003; 2(2):49-53.
35. Malami SA, Pindiga UH, Abimiku BA, Mungadi IA, Abdullahi AD, Dauda A et al. A
descriptive retrospective study of the pattern of malignant diseases in Sokoto, north
western Nigeria (1999-2004). J Med Sci 2007; 7(6):1033-1038.

60
36. Bosch FX, Ribes J, Cleries R, Diaz M. Epidemiology of hepatocellular carcinoma. Clin
Liver Dis 2005; 9:191-211.
37. Parkin DM, Bray F, Ferley J, Pisani P. Global cancer statistics 2000. CA Cancer J Clin
2005; 55:74-108.
38. Stefaniuk P, Cianciara J, Wiercinska-Drapalo A. Present and future possibilities for
early diagnosis of hepatocellular carcinoma. World J Gastroenterol 2010 28;
16(4):418-424.
39. Williams AO, Edington GM, Obakponovwe PC. Hepatocellular carcinoma in infancy
and childhood. Br J Cancer 1967; 21(3):474-482.
40. Mustapha SK, Bolori MT, Ajayi NA, Ngadda HA, Pindiga UH, Gashau W et al.
hepatocellular carcinoma in north-eastern Nigeria: a prospective clinical study of 100
cases. Internet J Gastroenterol 2007;6(1)
41. Abdulkareem FB, Faduyile FA, Daramola A O, Rotimi O, Banjo AAF, Elesha SO, et al.
Malignant Gastrointestinal Tumours in South Western Nigeria: A Histopathologic
Analysis of 713 Cases. West Afr J Med 2009; 28(3):173-176.
42. Otegbayo JA, Oluwasola OA, Akere A, Ogunbiyi JO. Temporal and biological trends in
liver cancers at a university hospital in southwest Nigeria. Trop Doct 2006; 36:28-30.
43. Echejoh GO, Tanko MN, Manasseh AN, Ogala-Echejoh S, Ugoya SO, Mandong BM.
Hepatocellular carcinoma in Jos, Nigeria. Nig J Med 2008; 17(2):210-213.
44. Adeniji KA, Anjorin AS. The pattern of malignant tumours of the liver in a tertiary
institution in Nigeria. Afr J Med Med Sci 2004; 33:27-30.
45. Seleye-Fubara D, Jebbin NJ. Hepatocellular carcinoma in Port Harcourt, Nigeria:
Clinico-pathologic study of 75 cases. Ann Afr Med 2007; 6(2):54-57.

61
46. Benvegnu L, Alberti A. Pattern of hepatocellular carcinoma development in hepatitis
B virus and hepatitis C virus related cirrhosis. Antivir Res 2001; 52:199-207.
47. Wagida AA, Khaled HM, Amra HA, El-Nezami H, Loffredo C. Changing pattern of
hepatocellular carcinoma and its risk factors in Egypt: possibilities for prevention.
Mutat Res 2008; 659:176-184.
48. International Agency for Research on Cancer. Aflatoxins. IARC monographs
evaluating carcinogenic risks in humans. 1993; 56:245-395.
http://monographs.iarc.fr/ENG/Monographs/vol82/mono82.pdf [accessed 2nd March,
2011].
49. Udoh JM, Cardwel KF, Ikotun T. Storage structures and aflatoxin content of maize in
five agro-ecological zones of Nigeria. J Stored Products Res 2000; 36:187-201.
50. Hirohashi S, Ishak KG, Kojiro M, Wanless IR, Theis ND et al. Tumours of the liver and
intrahepatic bile ducts. In: Hamilton SR, Aaltonen LA [editors]. Pathology and
genetics of tumours of the digestive system. Lyon (France): IARC press; 2000.p.159-
172.
51. Igetei R, Otegbayo JA, Ndububa DA, Lesi OA, Anumudu CI, Hainaut P, Gormally E.
Detection of p53 codon 249 mutation in Nigerian patients with hepatocellular
carcinoma using novel evaluation of cell-free DNA. Ann Hepatol 2008; 7(4):339-344.
52. Kew MC. Synergistic interaction between aflatoxin B1 and hepatitis B virus in
hepatocellular carcinogenesis. Liver Int 2003; 23:405-409.
53. Turner PC, Mendy M, Whittle H, Fortuin M, Hall AJ, Wild CP. Hepatitis B infection and
aflatoxin biomarker levels in Gambian children. Trop Med Int Health 2000; 5:837-
841.

62
54. Anthony PP. Tumours of the hepatobiliary system. In: Fletcher CDM [editor].
Diagnostic histopathology of tumours. Vol 1. 2nd ed. London: Churchill Livingstone;
2000. p. 411-450.
55. Datta GS. Histopathological scoring of chronic viral hepatitis. Hep B Annual 2004;
1:92-112.
56. Poynard T, Mathurin P, Lai C, Guyader D, Poupon R, Tainturier M et al. A comparison
of fibrosis progression in chronic liver disease. J Hepatol 2003; 38:257-265.
57. Fattovich G, Zagni I, Scattolini C. Natural history of hepatitis B and prognostic factors
of disease progression. In: Marcellin P, editor. Management of patients with viral
hepatitis. Paris: Association pour l'amélioration de la prise en charge des malades
atteints d'hépatite virale (APMAHV); 2004.p.203-220.
58. Rigamonti C, Andorno S, Maduli E, Capelli F, Boldorini R, Sartori M. Gender and liver
fibrosis. Aliment Pharmacol Ther 2005; 21:1445-1451.
59. Kim SU, Han KH, Ahn SH. Non-invasive assessment of liver fibrosis: the gap between
ideal and real. J Gastroenterol Hepatol 2011; 26:937-942.
60. Abdulkareem FB, Banjo AF, Elesha SO. Hepatic neoplasms in Lagos: a ten-year
review of surgical biopsies (1989-1998). Nig Postgrad Med J 199; 6(3):126-129.
61. Nwokediuko SC, Ijoma UN, Obienu O. Liver cancer in Enugu, south east Nigeria.
Insight bioinformatics 2011; 1(1):1-5.
62. Yeh MM, Swanson PE. Hepatobiliary system. In: Gattuso P, Reddy VB, David O, Spitz
D, Haber MH. Differential diagnosis in surgical pathology. 2nd ed. Philadelphia.
Saunders-Elsevier; 2010.p.428-430.

63
APPENDIX A
WHO HISTOLOGICAL CLASSIFICATION OF TUMOURS OF THE LIVER AND
INTRAHEPATIC BILE DUCTS (2000)
1. Epithelial tumours
1.1. Benign:
1.1.1. Hepatocellular adenoma
1.1.2. Focal nodular hyperplasia
1.1.3. Intrahepatic bile duct adenoma
1.1.4. Intrahepatic bile duct cystadenoma
1.1.5. Biliary papillomatosis
1.2. Malignant:
1.2.1. Hepatocellular carcinoma (liver cell carcinoma)
1.2.2. Intrahepatic cholangiocarcinoma (peripheral bile duct adenoma)
1.2.3. Bile duct cystadenocarcinoma
1.2.4. Combined hepatocellular and cholangiocarcinoma
1.2.5. Hepatoblastoma
1.2.6. Undifferentiated carcinoma
2. Non-epithelial tumours
2.1. Benign:
2.1.1. Angiomyolipoma
2.1.2. Lymphangioma and lymphangiomatosis
2.1.3. Haemangioma
2.1.4. Infantile haemangioendothelioma
64
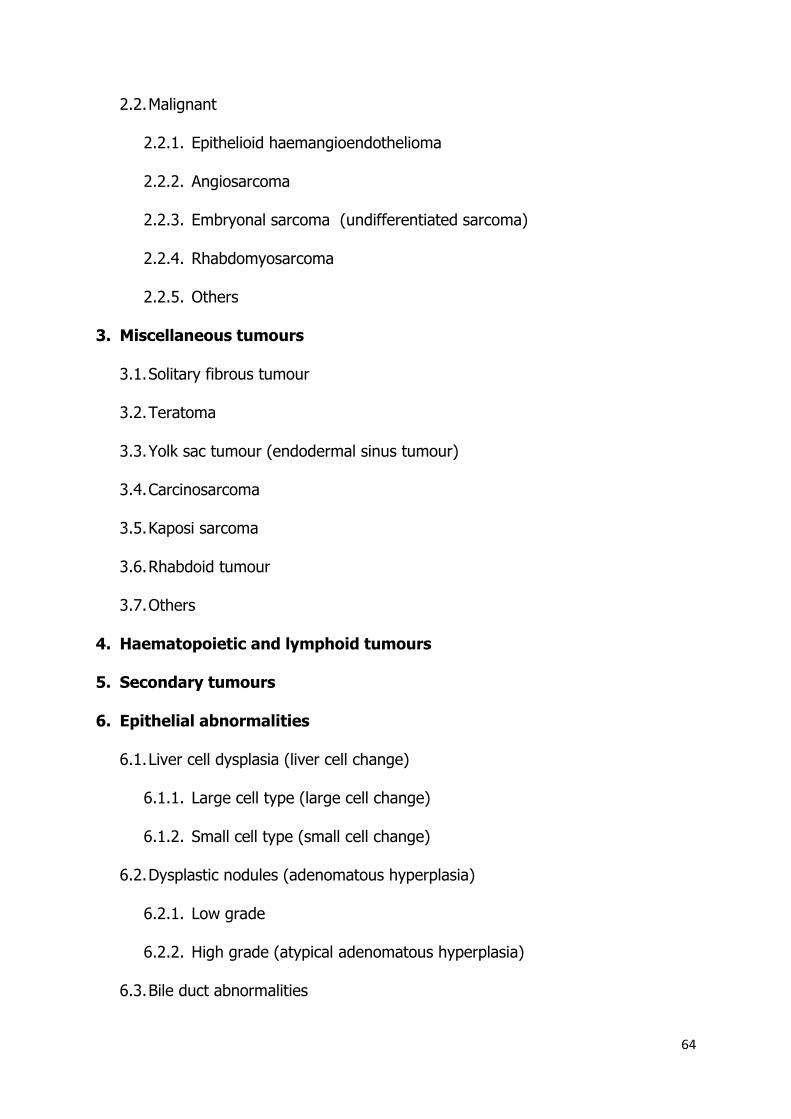
2.2. Malignant
2.2.1. Epithelioid haemangioendothelioma
2.2.2. Angiosarcoma
2.2.3. Embryonal sarcoma (undifferentiated sarcoma)
2.2.4. Rhabdomyosarcoma
2.2.5. Others
3. Miscellaneous tumours
3.1. Solitary fibrous tumour
3.2. Teratoma
3.3. Yolk sac tumour (endodermal sinus tumour)
3.4. Carcinosarcoma
3.5. Kaposi sarcoma
3.6. Rhabdoid tumour
3.7. Others
4. Haematopoietic and lymphoid tumours
5. Secondary tumours
6. Epithelial abnormalities
6.1. Liver cell dysplasia (liver cell change)
6.1.1. Large cell type (large cell change)
6.1.2. Small cell type (small cell change)
6.2. Dysplastic nodules (adenomatous hyperplasia)
6.2.1. Low grade
6.2.2. High grade (atypical adenomatous hyperplasia)
6.3. Bile duct abnormalities

65
6.3.1. Hyperplasia
6.3.2. Dysplasia (bile duct epithelium and peribiliary glands)
6.3.3. Intraepithelial carcinoma (carcinoma in situ)
7. Miscellaneous lesions
7.1. Mesenchymal hamartoma
7.2. Nodular transformation (nodular regenerative hyperplasia)
7.3. Inflammatory pseudotumour

66
APPENDIX B
KNODELL’S SCORING SYSTEM
Score
Periportal ± bridging necrosis
None 0
Mild piece meal necrosis (PMN) 1
Moderate PMN (<1/2 circumference) 3
Marked PMN (>1/2 circumference) 4
Moderate PMN + bridging necrosis 5
Marked PMN + bridging necrosis 6
Multilobular necrosis 10
Intralobular degeneration and focal
necrosis
None 0
Mild (<1/3 of lobules or nodules) 1
Moderate (1/3-2/3 of lobules or nodules) 3
Marked (>2/3 of lobules or nodules) 4
Portal inflammation
None 0
Mild (<1/3 of portal tract) 1
Moderate (1/3-2/3 of portal tract) 3
Marked (2/3 of portal tracts) 4
Fibrosis
None 0
Fibrous portal expansion 1
Bridging fibrosis (P-P) or (P-C) 3
Cirrhosis 4

67

68


















