HIP ARTHROPLASTY: AVOIDING AND MANAGING PROBLEMS … · The modern, hybrid total hip arthroplasty...
6
54 CCJR SUPPLEMENT TO THE BONE & JOINT JOURNAL HIP ARTHROPLASTY: AVOIDING AND MANAGING PROBLEMS The modern, hybrid total hip arthroplasty for primary osteoarthritis at the Hospital for Special Surgery A. González Della Valle, N. Sharrock, M. Barlow, L. Caceres, G. Go, E. A. Salvati From The Hospital for Special Surgery, New York, United States A. González Della Valle, MD, Orthopaedic Surgeon, Professor of Clinical Orthopaedic Surgery N. Sharrock, MB, ChB, Attending Anaesthesiologist M. Barlow, PA, Physician Assistant L. Caceres, MD, Orthopaedic Surgeon E. A. Salvati, MD, Orthopaedic Surgeon, Professor of Clinical Orthopaedic Surgery G. Go, BS, Research Assistant Hospital for Special Surgery, 535 East 70th Street, New York, 20012, USA. Correspondence should be sent to Dr A. González Della Valle; e-mail: [email protected] ©2016 The British Editorial Society of Bone & Joint Surgery doi:10.1302/0301-620X.98B1. 36409 $2.00 Bone Joint J 2016;98-B(1 Suppl A):54–9. We describe our technique and rationale using hybrid fixation for primary total hip arthroplasty (THA) at the Hospital for Special Surgery. Modern uncemented acetabular components have few screw holes, or no holes, polished inner surfaces, improved locking mechanisms, and maximised thickness and shell-liner conformity. Uncemented sockets can be combined with highly cross-linked polyethylene liners, which have demonstrated very low wear and osteolysis rates after ten to 15 years of implantation. The results of cement fixation with a smooth or polished surface finished stem have been excellent, virtually eliminating complications seen with cementless fixation like peri-operative femoral fractures and thigh pain. Although mid-term results of modern cementless stems are encouraging, the long-term data do not show reduced revision rates for cementless stems compared with cemented smooth stems. In this paper we review the conduct of a hybrid THA, with emphasis on pre-operative planning, surgical technique, hypotensive epidural anaesthesia, and intra-operative physiology. Cite this article: Bone Joint J 2016;98-B(1 Suppl A):54–9. History and scientific background behind hybrid fixation for total hip arthroplasty Long-term results of cemented total hip arthro- plasty (THA) have revealed a progressive dete- rioration of acetabular fixation after the first decade in vivo. 1,2 While acetabular revision rates for aseptic loosening increase, the radio- graphic fixation and clinical survivorship of cemented femoral stems has remained excel- lent at a follow-up of three to four decades. 1,3 Coupled with advances in cementless acetabu- lar fixation, these observations have resulted in an increased used of hybrid fixation. 4 Long- term survivorship and a low incidence of com- plications reported in national registries sup- port the use of hybrid fixation. 4,5 Accordingly hybrid fixation continues to be our preferred method for primary THA. First generation cementless acetabular com- ponents exhibited low rates of loosening, 6 but were affected by complications related to defi- cient design, implantation technique and man- ufacturing processes. Suboptimal locking mechanisms permitted micromotion between the liner and the shell, with the subsequent generation of backside wear. 7 The lack of con- formity between the liner and the shell, and the roughness of the inner surface of the shell, compounded this problem. 7 In some of the early acetabular component designs, fatigue failure of the locking mechanism and displace- ment of the insert have been reported. 8 The presence of screw holes permitted debris to access the pelvic interface, which accompanied by the hydrodynamic pumping action of repeated hip loading, resulted in retro-acetabu- lar osteolysis. 9 Lastly, suboptimal sintering of the ingrowth surface enabled shedding of this material and third-body wear to ensue. 10,11 Understanding these modes of late failure, cou- pled with advancements in the manufacturing process, resulted in modern uncemented shells with fewer or no screw holes, polished inner surfaces, improved locking mechanisms, and maximised thickness and shell-liner conform- ity. 12 Contemporary cementless acetabular shells combined with highly cross-linked poly- ethylene liners have provided encouraging results with low wear and rates of osteoly- sis. 13,14 In a review of 60 patients who under- went primary, hybrid THA with conventional (gamma irradiated in nitrogen) or highly cross- linked polyethylene, at a mean follow-up of 11 years (7 to 15) the latter group exhibited signif- icantly lower annual wear rates (0.17 mm/year and 0.02 mm/year respectively, p < 0.001) and osteolysis (97% and 10% respectively, p < 0.001). 14 The satisfactory long-term results of cemented femoral stems support the use of cement for stem
Transcript of HIP ARTHROPLASTY: AVOIDING AND MANAGING PROBLEMS … · The modern, hybrid total hip arthroplasty...

54 CCJR SUPPLEMENT TO THE BONE & JOINT JOURNAL
HIP ARTHROPLASTY: AVOIDING AND MANAGING PROBLEMS
The modern, hybrid total hip arthroplasty for primary osteoarthritis at the Hospital for Special Surgery
A. González Della Valle,N. Sharrock,M. Barlow,L. Caceres,G. Go,E. A. Salvati
From The Hospital for Special Surgery, New York, United States
A. González Della Valle, MD, Orthopaedic Surgeon, Professor of Clinical Orthopaedic Surgery N. Sharrock, MB, ChB, Attending Anaesthesiologist M. Barlow, PA, Physician Assistant L. Caceres, MD, Orthopaedic Surgeon E. A. Salvati, MD, Orthopaedic Surgeon, Professor of Clinical Orthopaedic Surgery G. Go, BS, Research AssistantHospital for Special Surgery, 535 East 70th Street, New York, 20012, USA.
Correspondence should be sent to Dr A. González Della Valle; e-mail: [email protected]
©2016 The British Editorial Society of Bone & Joint Surgerydoi:10.1302/0301-620X.98B1. 36409 $2.00
Bone Joint J2016;98-B(1 Suppl A):54–9.
We describe our technique and rationale using hybrid fixation for primary total hip arthroplasty (THA) at the Hospital for Special Surgery. Modern uncemented acetabular components have few screw holes, or no holes, polished inner surfaces, improved locking mechanisms, and maximised thickness and shell-liner conformity. Uncemented sockets can be combined with highly cross-linked polyethylene liners, which have demonstrated very low wear and osteolysis rates after ten to 15 years of implantation. The results of cement fixation with a smooth or polished surface finished stem have been excellent, virtually eliminating complications seen with cementless fixation like peri-operative femoral fractures and thigh pain. Although mid-term results of modern cementless stems are encouraging, the long-term data do not show reduced revision rates for cementless stems compared with cemented smooth stems. In this paper we review the conduct of a hybrid THA, with emphasis on pre-operative planning, surgical technique, hypotensive epidural anaesthesia, and intra-operative physiology.
Cite this article: Bone Joint J 2016;98-B(1 Suppl A):54–9.
History and scientific background behind hybrid fixation for total hip arthroplastyLong-term results of cemented total hip arthro-plasty (THA) have revealed a progressive dete-rioration of acetabular fixation after the firstdecade in vivo.1,2 While acetabular revisionrates for aseptic loosening increase, the radio-graphic fixation and clinical survivorship ofcemented femoral stems has remained excel-lent at a follow-up of three to four decades.1,3
Coupled with advances in cementless acetabu-lar fixation, these observations have resulted inan increased used of hybrid fixation.4 Long-term survivorship and a low incidence of com-plications reported in national registries sup-port the use of hybrid fixation.4,5 Accordinglyhybrid fixation continues to be our preferredmethod for primary THA.
First generation cementless acetabular com-ponents exhibited low rates of loosening,6 butwere affected by complications related to defi-cient design, implantation technique and man-ufacturing processes. Suboptimal lockingmechanisms permitted micromotion betweenthe liner and the shell, with the subsequentgeneration of backside wear.7 The lack of con-formity between the liner and the shell, and theroughness of the inner surface of the shell,compounded this problem.7 In some of theearly acetabular component designs, fatigue
failure of the locking mechanism and displace-ment of the insert have been reported.8 Thepresence of screw holes permitted debris toaccess the pelvic interface, which accompaniedby the hydrodynamic pumping action ofrepeated hip loading, resulted in retro-acetabu-lar osteolysis.9 Lastly, suboptimal sintering ofthe ingrowth surface enabled shedding of thismaterial and third-body wear to ensue.10,11
Understanding these modes of late failure, cou-pled with advancements in the manufacturingprocess, resulted in modern uncemented shellswith fewer or no screw holes, polished innersurfaces, improved locking mechanisms, andmaximised thickness and shell-liner conform-ity.12 Contemporary cementless acetabularshells combined with highly cross-linked poly-ethylene liners have provided encouragingresults with low wear and rates of osteoly-sis.13,14 In a review of 60 patients who under-went primary, hybrid THA with conventional(gamma irradiated in nitrogen) or highly cross-linked polyethylene, at a mean follow-up of 11years (7 to 15) the latter group exhibited signif-icantly lower annual wear rates (0.17 mm/yearand 0.02 mm/year respectively, p < 0.001)and osteolysis (97% and 10% respectively,p < 0.001).14
The satisfactory long-term results of cementedfemoral stems support the use of cement for stem

THE MODERN, HYBRID TOTAL HIP ARTHROPLASTY FOR PRIMARY OSTEOARTHRITIS AT THE HOSPITAL FOR SPECIAL SURGERY 55
VOL. 98-B, No. 1, JANUARY 2016
fixation.1,2,15,16 The constituents of acrylic cement remainedvirtually unchanged since the 1960s and advancements inthe understanding of cement fixation, mixing techniques,application, pressurisation, stem materials and designresulted in predictable long-term fixation and clinicalresults.17 The improvements in cementing techniqueinclude: femoral preparation to diminish interface bleeding,pulsatile lavage, reduced cement porosity by vacuum mix-ing, the use of a cement restrictor, pre-heating the stem andpolymer,18 retrograde canal filling and pressurisation witha cement gun, stem centralisation and stem geometries thatincrease the intramedullary pressure, and intrusion of thecement into the bone.19,20 In contrast, certain changes incement fixation and the polymer itself were detrimental andwere abandoned.21-23
In recent years there has been a tendency towards anincreased use of cementless femoral fixation.24 The shift inthe choice of fixation followed the consistent, durable fixa-tion obtained with uncemented acetabular compo-nents,12,25 ease of implantation, and the poor results ofcemented fixation observed with rough and pre-coatedstems.21-23 Unlike cementless femoral fixation, cementedfixation has numerous advantages: it is versatile, durableand can be used regardless of the diagnosis, proximal fem-oral geometry, anteversion, and bone quality. It can also actas a local antibiotic delivery system. Intra-operative femo-ral fractures and post-operative thigh pain are rare with
cemented femoral fixation. Survivorship has not beensurpassed by uncemented femoral fixation4 and it contin-ues to be our preferred form of fixation.
Pre-operative templatingA standardised radiographic evaluation of the hip, includesan anteroposterior (AP) view of the pelvis centred over thepubic symphysis, and a flog-leg lateral view of the affectedhip.26,27 The AP view is obtained with the hips in 10° to 15°of internal rotation to ensure a true AP view of the femoralneck.
Assuming that the x-ray tube is at a distance of 1 metrefrom the tabletop, and the film is placed in a tray 5 cmbelow the table, the radiographic magnification willapproximate 20%. The magnification will increase in obesepatients and diminish in thin patients. If digital radiographyis used or if absolute measurements are required, a magni-fication marker is placed at the level of the hip.
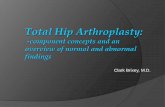
Our templating protocol has been developed by the sen-ior author (EAS) and has been in use for the last three dec-ades. It begins with drawing the inter-teardrop line as ahorizontal reference for acetabular inclination and leglength. The acetabular template is placed at 40° to 45° ofinclination with the inferomedial silhouette of the compo-nent approximating to the base of the teardrop and themedial border approximating to the ilioischial line. Theintended acetabular component should be sized to achievemaximum acetabular coverage with minimal removal ofsubchondral bone (Fig. 1). The implant size, the new centreof rotation, and the relative amount of uncoverage (if any)are recorded in the plan.
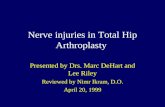
The goals of femoral templating are to achieve animplant with adequate alignment and fixation, restore fem-oral offset, and equalise leg length. The stem size should bethe one that allows for a 2 mm circumferential cement man-tle, which usually is marked on the template. The positionof the stem in the femoral canal should allow equalisationof limb length and restoration of offset (Fig. 1). The sur-geon should aim to use the mid-range of neck lengths inorder to allow adjustment to a shorter or longer modularhead during surgery. Once the position and offset of thestem are planned, the new centre of rotation of the pros-thetic head, and the level of the femoral neck osteotomy aremarked. The distance from the proximal corner of thelesser trochanter to the centre of rotation of the prosthetichead and the distance from the proximal corner of thelesser trochanter to the neck cut are then both measured.Measuring the distance from the calcar medial to themedial border of the templated stem at the neck cut helpsthe surgeon assess the alignment of the stem in the frontalplane (varus–valgus) intra-operatively (Fig. 2). The diame-ter of the distal centraliser, the plug size and depth of inser-tion are also recorded in the plan.
With careful templating, acetabular and femoral compo-nents for hybrid THA can be predicted to within one size in99.2% of cases.27 The predictability in component sizing
Fig. 1
Radiograph showing that the socketand stem are templated individually.The position of the centre of rotationof the head (black arrow) in relationto the centre of rotation of the socket(white arrow) is selected so thatlimb-length and offset are restored(template from Zimmer, Warsaw,Indiana).

56 A. GONZÁLEZ DELLA VALLE, N. SHARROCK, M. BARLOW, L. CACERES, G. GO, E. A. SALVATI
CCJR SUPPLEMENT TO THE BONE & JOINT JOURNAL
allows pre-heating of the intended stem (± 1 size) and havingthe remaining implants available in the operating theatre toexpedite surgery.
Intra-operative and anaesthetic factorsThere are three important intra-operative factors to con-sider: Firstly, the use of regional anaesthesia; secondly,intra-operative hypotensive anaesthesia; and thirdly, use ofmultimodal thromboprophylaxis.
Improved outcome has been shown when spinal or epiduralanaesthesia is used rather than general anaesthesia.28,29
Advantages include fewer respiratory complications, lessblood loss/transfusion, lower risk of thromboembolism and alower rate of post-operative mortality.
Intra-operative hypotensive anaesthesia results inimproved interdigitation of cement into cancellous bone.Secondly, a dry surgical field improves surgical exposureand finally, reduced blood loss results in less fluid adminis-tration and transfusion requirements.28
Multimodal thromboprophylaxis developed at the Hos-pital for Special Surgery, encompasses several strategiesbased on the peri-operative physiology which contributesto thrombogenesis. Firstly, femoral venous occlusion occursduring surgery on the femur when the femoral vein iskinked because of flexion and internal rotation of thefemur. In the mid-1990s, using rapid markers of thrombo-sis, it was determined that this is the moment when throm-bogenesis begins.30 Therefore, the period of potentialfemoral venous occlusion should be as brief as possible.31 Weadminister intravenous (IV) heparin (15 units/kg) before sur-gery on the femur.32-35 Administering a low intra-operativedose of IV unfractionated heparin demonstrated that throm-bogenesis during surgery is avoided.30,32 Lower extremity
blood flow is augmented with low dose IV epinephrine(1 mcg/min to 3 mcg/min), and post-operatively by footflexion/extension exercises, pneumatic compression devicesand early ambulation. This multimodal approach to throm-boprophylaxis enables aspirin to be used, which is both asafe and effective chemoprophylaxis agent in this setting.34
This results in a lower risk of bleeding than found withpowerful anticoagulants and is associated with an overalllower rate of post-operative mortality.36
General principles of surgical techniqueThe long-term success of THA is contingent upon the pre-cision and accuracy with which the components areimplanted. Adequate exposure to allow accurate bonypreparation and component implantation is encouraged.We favour the posterolateral approach because of its ana-tomical dissection and its extensile nature.
Acetabular preparationAfter acetabular exposure, the labrum must be com-pletely resected. Often a medial acetabular osteophyte ispresent which must be reamed until the true medial wallis encountered. Once the medial wall is reached, thereamer angle is changed to proceed in 40° of abductionand 20° to 25° of anteversion. Reaming to size is reachedwhen subchondral bone is exposed and healthy bleedingbone is visualised. The acetabular bed should beinspected for subchondral cysts which are curetted andpacked with autologous graft. Under-reaming by 2 mmhas been promoted as a way of enhancing initial compo-nent stability. A trial component can be used to assureadequate contact and stability. We currently use a porousshell with limited screw holes or no holes. If socket
Fig. 2
Radiograph showing how, after determining the position of the stem,the distance from the proximal corner of the lesser trochanter (P) tothe neck cut (NC) and to the centre of rotation of the prosthetic head(CH) is measured. The distance from the medial aspect of the calcar tothe medial aspect of the broach at the level of the neck cut (*) willguide stem centralisation avoiding varus or valgus malalignment.
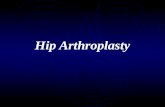
Fig. 3
Photograph showing how the femoral exposure is achieved by placinga “jaws” type retractor (JR) in the anteromedial aspect of the neck, anAufrank retractor (AR) medial to the neck, and a thin, bent Hohmannretractor lateral to the greater traochanter. Exposure should allow vis-ualisation of the neck cut, calcar and piriformis fossa (PF), while pro-tecting the gluteus medius tendon and muscle (GM) that canpotentially be injured during femoral work.

THE MODERN, HYBRID TOTAL HIP ARTHROPLASTY FOR PRIMARY OSTEOARTHRITIS AT THE HOSPITAL FOR SPECIAL SURGERY 57
VOL. 98-B, No. 1, JANUARY 2016
stability is questionable, supplementary screw fixationcan be used.37
If the acetabular component insertion is being obstructedby a dense sclerotic acetabular rim, expansion with thereamer 1 mm smaller than the component size is required.Any peripheral osteophytes are removed and the highlycross-linked polyethylene liner is inserted.
Complications related to press-fit sockets are rare but canarise owing to technical errors during preparation and inser-tion. Sharkey et al38 have reported acetabular fracture duringcementless socket insertion. The fractures can be the result ofundersized reaming. Care should be taken to avoid over-zeal-ous shell impaction in osteoporotic bone. While the routineuse of supplementary screws for fixation in primary THA isbecoming less common, neurovascular complications relatedto screw placement are best managed by avoidance of thedanger zones, described by Wasielewski et al.39
Femoral preparationStem and cement pre-heating. The pre-operative plan allowspre-heating the selected femoral stem and the next size smallerand larger to approximately 40 ºC to 44 ºC in an oven closeto the operating theatre. Pre-heating the stem and the cementpolymer reduces cement porosity, particularly at the cementmetal interface and polymerisation time by approximatelysix minutes, without affecting its mechanical properties.18,40
The surgical time is shortened at a critical time when thethrombogenesis is maximally activated and while the leg ismaintained in an extreme position, with the femoral veinkinked and occluded,41,42 causing venous stasis, and poten-tial endothelial injury. Reducing the time for polymerisationalso decreases the risk of an inadvertent displacement of thestem while the cement is curing.
Pre-heating of the stem and cement should be imple-mented cautiously only once an efficient surgical team isworking together, as a delay could result in prematurepolimerisation.Surgical technique for cemented femoral fixation. Surgicalexposure should allow a clear view of the proximal femoralopening and the proximal corner of the lesser trochanter,while protecting the soft-tissues around the proximal femur(Fig. 3). The surgeon should avoid muscular damage, par-ticularly to the gluteus medius muscle and tendon that mayresult in the formation of heterotopic ossification or post-operative limping. Immediately after exposure, any ante-rior osteophytes in the femoral neck are identified andresected.
The proximal femur can be opened with a box cuttingchisel. The point of insertion is generally posterior, in thevicinity of the piriformis fossa.43 Failure to determine thecorrect AP position of the proximal femoral opening canresult in a deficient cement mantle.43 A canal finder is intro-duced by hand to open the femoral canal.
The authors prefer only to use broaches for femoralpreparation. The broaches are designed with smooth teethto displace and compact intramedullary bone. Femoral
preparation is usually started with a broach that is two sizessmaller than the size of the templated stem. Progressivelylarger size broaches are used. The surgeon should not relyonly on the pre-operative plan for stem sizing. The tactilefeedback during broaching is important to select the stemsize, and to minimise cancellous bone loss and the risk offracture. Recognition of the compliance and strength of thebone during preparation is as important as the pre-operativeplan. We have demonstrated that as the femoral canal isinstrumented, intramedullary contents including fat marroware forced to the proximal femoral venous system, activatingthe clotting cascade.30 Removal of the intramedullary con-tents by frequent irrigation and aspiration reduces the loadof these procoagulants.
After the final broach is inserted, the calcar planer can beused to make final adjustments in the plane of femoral neckresection. A trial modular neck and head attached to thebroach can be used to measure the distance from the prox-imal corner of the lesser trochanter to the centre of rotationof the head and for trial reduction. Modular femoral headswith a skirt or those that expose the Morse taper diminish-ing the head-neck ratio, should be avoided.
The broach is then removed and the distal centralisermeasured selecting the largest diameter that can be easilyintroduced to the appropriate depth.
The cement restrictor is then inserted to the adequatedepth, which is usually 1 cm to 1.5 cm beyond the tip of thestem. The plug should be introduced at a slow pace in aclean and dry canal. Failure to aspirate the intramedullarycontents and/or a fast introduction of the plug can forceprocoagulants and air into the venous circulation causingcardiopulmonary complications and arrest.21 Once theplug is fully seated, the stability of the plug should be testedto ensure that the intramedullary canal is pressurised dur-ing cement injection and stem insertion without migrationof the plug. An unstable plug should be removed andreplaced with a bigger one.
The intramedullary canal should be clean and dry withrepeated pulsatile lavage and aspiration to remove loosedebris, blood clots, and marrow before cement injection. Thecanal remains bloodless if the leg is in an extreme position offlexion and internal rotation during cement insertion, partic-ularly in the presence of hypotensive anaesthesia.
Vacuum mixed, pre-heated cement is then injected andpressurised in the canal. The authors prefer to occlude theproximal femur with their thumb rather than with a rubberseal as it affords greater control over the pressure in the canalduring cement pressurisation. The surgeon should create ahigh and constant intramedullary pressure that allows theviscous cement to interdigitate in the cancellous bone.
The stem is inserted at a slow pace, without changes inrotation or alignment while the surgeon continues toocclude the proximal femoral opening with the thumb. It isduring stem insertion that the highest intramedullary pres-sures are achieved.19,20 We have shown that rarely, post-operative radiographs demonstrate cement filling the prox-

58 A. GONZÁLEZ DELLA VALLE, N. SHARROCK, M. BARLOW, L. CACERES, G. GO, E. A. SALVATI
CCJR SUPPLEMENT TO THE BONE & JOINT JOURNAL
imal femoral veins indicating high pressurisation has beenobtained.44 This radiographic finding is clinically benignand should not be misinterpreted as a femoral fracture.Tapered stems generate higher intramedullary pressuresduring insertion than cylindrical stems, as the formerreduce the proximal space for the cement throughout steminsertion.19,20
Once fully seated, gentle pressure should be appliedwithout changes in alignment or rotation until the cement ispolymerised. The modular femoral head should beimpacted onto a clean dry taper. A Morse taper contami-nated with blood or irrigation fluids can favour corrosion.
Preference for satin or highly polished cemented femoral stemsCement is not an adhesive and the fixation is achieved byinterdigitation. The cemented femoral stem acts as a com-posite structure, transmitting body weight through threelayers (metal, cement and bone) and through the two inter-faces between them (metal-cement and cement-bone).45
This load transfer is determined by the cement-to-metalsurface interaction, the cement-bone interface, the stemgeometry, the structural properties of the implant, and bythe patient weight and activity level.46 Surgeons implantfemoral stems with a wide variety of surface finishes andtextures which are supported by contrasting philosophiesof fixation.
In polished stems, bone cement acts as a structural grout-ing material. Load transfer occurs through compressionwith micromotion at the cement-metal interface in view ofthe non-adherent, smooth and polished interface.21,46 Thismicromotion may be protective of the bone-cement inter-face. Conversely, with the firm mechanical adhesion ofcement to the femoral stem with rough surfaces, the loadtransfer occurs through tension, shear and compressiondirectly to the cement-metal interface. The lack of micro-motion at this interface transfers all the loads to the bonecement interface.
Our experience with a rough, proximally textured, mod-ern cemented femoral stem has been disappointing. A seriesof 64 THAs with a rough Versys stem (Zimmer, Warsaw,Indiana) (μRa: 80 to 100 microinches) and 138 THAs witha satin Versys stem (μRa: 20 microinches) was followedclinically and radiographically for four to seven years. Alloperations were performed by the senior author (EAS) withthe same surgical technique, acetabular component, cementtype and cementing technique. In the rough group, sevenhips and none in the satin group developed aseptic loosen-ing (p < 0.001).22
Smooth stems tolerate micromotion at the cement-prosthesis interface without damaging the fixation. Con-versely, when a tight mechanical or chemical cement-pros-thesis bond is achieved with a rough or pre-coated stem, thetorsional and axial forces transmitted to the bone-cementinterface are higher and micromotion may initiate macro-motion with loosening at the bone-cement interface. The
literature supports the use of smooth or polished surfacefinish for cemented femoral components.21,45
Wound closure and rehabilitationWe strongly advocate the use of an enhanced soft-tissuerepair that includes capsule, short external rotators andquadratus femoris muscle. Finally, 3 g of tranexamic acid isapplied topically before would closure to avoid the use ofdrains.
Patients are mobilised promptly after surgery, bearingweight as tolerated with assistive devices as required. Exer-cises will avoid flexion greater than 90° and internal rota-tion for the initial five to six weeks following surgery.
The multimodal thromboprophylaxis is used for the firstsix post-operative weeks.28,34,35
Author contributions:N. Sharrock: Generated a structured draft, edited the draft, reviewed current lit-erature.A. González Della Valle: Generated a structured draft, edited the draft, reviewedcurrent literature.M. Barlow: Generated a structured draft, reviewed current literature, generatedillustrations.L. Caceres: Generated a structured draft, reviewed current literature, generatedillustrations.G. Go: Generated a structured draft, edited the draft, reviewed current literature.E. A. Salvati: Generated a structured draft, edited the draft, reviewed current lit-erature.
No benefits in any form have been received or will be received from a commer-cial party related directly or indirectly to the subject of this article.
This study was partially funded by the generous donation of Mr. G. Bergenfield,the Sidney Milton and Leoma Simon Foundation and by Mrs. M. Bayroff.
This article was primary edited by G. Scott.
This paper is based on a study which was presented at the 2014 CurrentConcepts in Joint Replacement® - The Journey Continues meeting held inIguassu Falls, Brazil, 17th-20th September.
References1. Wroblewski BM, Siney PD, Fleming PA. Charnley low-frictional torque arthro-
plasty: follow-up for 30 to 40 years. J Bone Joint Surg [Br] 2009;91-B:447–450.
2. Berry DJ, Harmsen WS, Cabanela ME, Morrey BF. Twenty-five-year survivorshipof two thousand consecutive primary Charnley total hip replacements: factors affect-ing survivorship of acetabular and femoral components. J Bone Joint Surg [Am]2002;84-A:171–177.
3. Berry DJ, Harmsen WS, Ilstrup DM. The natural history of debonding of the fem-oral component from the cement and its effect on long-term survival of Charnley totalhip replacements. J Bone Joint Surg [Am] 1998;80-A:715–721.
4. No authors listed. The Swedish Artroplasty Register: Annual Report, 2013. http://www.shpr.se/Libraries/Documents/AnnualReport_2013Eng.sflb.ashx (date lastaccessed 20 July 2015).
5. No authors listed. Annual Report 2014. The Australian Hip and Knee ArthroplastyRegister. https://aoanjrr.dmac.adelaide.edu.au/documents/10180/172286/Annual%20Report%202014 (date last accessed 30 July 2015).
6. Crowther JD, Lachiewicz PF. Survival and polyethylene wear of porous-coatedacetabular components in patients less than fifty years old: results at nine to fourteenyears. J Bone Joint Surg [Am] 2002;84-A:729–735.
7. Huk OL, Bansal M, Betts F, et al. Polyethylene and metal debris generated by non-articulating surfaces of modular acetabular components. J Bone Joint Surg [Br]1994;76-B:568–574.
8. González Della Valle A, Ruzo PS, Li S, et al. Dislodgment of polyethylene liners infirst and second-generation Harris-Galante acetabular components. A report of eight-een cases. J Bone Joint Surg [Am] 2001;83-A:553–559.
9. Bono JV, Sanford L, Toussaint JT. Severe polyethylene wear in total hip arthro-plasty. Observations from retrieved AML PLUS hip implants with an ACS polyethyleneliner. J Arthroplasty 1994;9:119–125.
10. Slullitel G, González Della Valle A, Buttaro M, Piccaluga F. Early bead shed-ding of the Vitalock acetabular cup--a report on 7 cases. Acta Orthop Scand2003;74:658–660.

THE MODERN, HYBRID TOTAL HIP ARTHROPLASTY FOR PRIMARY OSTEOARTHRITIS AT THE HOSPITAL FOR SPECIAL SURGERY 59
VOL. 98-B, No. 1, JANUARY 2016
11. Mayman DJ, González Della Valle A, Lambert E, et al. Late fiber metal sheddingof the Harris Galante Type II acetabular component. A report of 5 cases. J Arthroplasty2007;22:624–629.
12. González Della Valle A, Zoppi A, Peterson MG, Salvati EA. Clinical and radio-graphic results associated with a modern, cementless modular cup design in total hiparthroplasty. J Bone Joint Surg [Am] 2004;86-A:1998–2004.
13. Beksaç B, Salas AP, Gonzalez Della Valle A, Salvati EA. Wear is reduced intotal hip arthroplasties performed with highly cross–linked polyethylene. A matchpaired study of 82 hips at 5-year follow up. Clin Orthop Relat Res 2009;467:1765–1772.
14. Beksac B, Gonzalez Della Valle A, Salvati EA. Highly cross linked polyethylenesignificantly lowers wear and osteolysis following THA [abstract]. AAOS AnnualMeeting, 2015.
15. Ling RS, Charity J, Lee AJ, et al. The long-term results of the original Exeter pol-ished cemented femoral component: a follow-up report. J Arthroplasty 2009;24:511–517.
16. El Masri F, Kerboull L, Kerboull M, Courpied JP, Hamadouche M. Is the so-called 'French paradox' a reality? Long-term survival and migration of the Charnley-Kerboull stem cemented line-to-line. J Bone Joint Surg [Br] 2010;92-B:342–348.
17. Malchau H, Herberts P, Eisler T, Garellick G, Söderman P. The Swedish TotalHip Replacement Register. J Bone Joint Surg [Am] 2002;84-A (suppl 2):2–20.
18. Parks ML, Walsh HA, Salvati EA, Li S. Effect of increasing temperature on theproperties of four bone cements. Clin Orthop Relat Res 1998;355:238–248.
19. Churchill DL, Incavo SJ, Uroskie JA, Beynnon BD. Femoral stem insertion gen-erates high bone cement pressurization. Clin Orthop Relat Res 2001;393:335–344.
20. Dayton MR, Incavo SJ, Churchill DL, Uroskie JA, Beynnon BD. Effects of earlyand late stage cement intrusion into cancellous bone. Clin Orthop Relat Res2002;405:39–45.
21. Simesen-De Bielke H, González-Della Valle A, Salvati EA. Vástagos cementa-dos en la artroplastía de cadera: historia y evolución. Acta Ortop Mex 2011;25:323–333.
22. González Della Valle A, Zoppi A, Peterson MG, Salvati EA. A rough surface fin-ish adversely affects the survivorship of a cemented femoral stem. Clin Orthop RelatRes 2005;436:158–163.
23. Beksac B, Taveras NA, González Della Valle A, Salvati EA. Surface finishmechanics explain different clinical survivorship of cemented femoral stems for totalhip arthroplasty. J Long Term Eff Med Implants 2006;16:407–422.
24. Troelsen A, Malchau E, Sillesen N, Malchau H. A review of current fixation useand registry outcomes in total hip arthroplasty: the uncemented paradox. Clin OrthopRelat Res 2013;471:2052–2059.
25. González Della Valle A, Su E, Zoppi A, Sculco TP, Salvati EA. Wear and preva-lence of osteolysis in modular and non-modular acetabular cups. A match pairedstudy at a follow up of 5 to 8 years. J Arthroplasty 2004;19:972–977.
26. González Della Valle A, Padgett DE, Salvati EA. Preoperative planning for pri-mary total hip arthroplasty. J Am Acad Orthop Surg 2005;13:455–462.
27. González Della Valle A, Slullitel G, Piccaluga F, Salvati EA. The precision andusefulness of preoperative planning for cemented and hybrid primary total hip arthro-plasty. J Arthroplasty 2005;20:51–58.
28. Salvati E, Sharrock NE, Westrich G, et al. Nicholas Andry Award: three decadesof clinical, basic and applied research on thromboembolic disease after total hiparthroplasty. Clin Orthop Relat Res 2007;444:246–254.
29. Sharrock NE. Just do it! Commentary on an article by Mohammad A. Helwani, MD,et al: “Effects of regional versus general anesthesia on outcomes after total hiparthroplasty: a retrospective propensity-matched cohort study”. J Bone Joint Surg[Am] 2015;97-A:18.
30. Sharrock NE, Go G, Harpel PC, et al. The John Charnley Award. Thrombogenesisduring total hip arthroplasty. Clin Orthop Relat Res 1995;319:16–27.
31. Sharrock NE, Go G, Mayman D, Sculco TP. Decreases in pulmonary artery oxygensaturation during total hip arthroplasty variations using 2 leg positioning techniques.J Arthroplasty 2005;20:499–502.
32. Salvati EA, Pellegrini VD Jr, Sharrock NE, et al. Recent advances in venousthromboembolic prophylaxis during and after total hip replacement. J Bone Joint Surg[Am] 2000;82-A:252–270.
33. DiGiovanni C, Restrepo A, González Della Valle A, et al. The safety and efficacyof intraoperative heparin for primary total hip replacement. Clin Orthop Relat Res2000;379:178–185.
34. González Della Valle A, Serota A, Go G, et al. Venous thromboembolism is rareafter total hip arthroplasty with a multimodal prophylaxis protocol. Clin Orthop RelatRes 2006;443:146–153.
35. Vulcano E, Gesell M, Esposito A, et al. Multimodal thromboprophylaxis with pref-erential use of aspirin for elective hip and knee arthroplasty. Int Orthop2012;36:1995–2002.
36. Sharrock NE, González Della Valle A, Go G, Lyman S, Salvati EA. Potent anti-coagulants are associated with a higher all-cause mortality rate after hip and kneearthroplasty. Clin Orthop Relat Res 2008;466:714–721.
37. Padgett DE, González Della Valle A. The uncemented acetabular component. In:Barrack RL, Rosenberg AG, eds. Master Techniques in Orthopeadic Surgery. The Hip.Philadelphia: Lippincott Williams & Wilkins, 2006:283–294.
38. Sharkey PF, Hozack WJ, Callaghan JJ, et al. Acetabular fracture associated withcementless acetabular component insertion: a report of 13 cases. J Arthroplasty1999;14:426–431.
39. Wasielewski RC, Cooperstein LA, Kruger MP, Rubash HE. Acetabular anatomyand the transacetabular fixation of screws in total hip arthroplasty. J Bone Joint Surg[Am] 1990;72-A:501–508.
40. Iesaka K, Jaffe WL, Kummer FJ. Effects of preheating of hip prostheses on thestem-cement interface. J Bone Joint Surg [Am] 2003;85-A:421–427.
41. Binns M, Pho R. Femoral vein occlusion during hip arthroplasty. Clin Orthop RelatRes 1990;255:168–172.
42. Planès A, Vochelle N, Fagola M. Total hip replacement and deep vein thrombosis.A venographic and necropsy study. J Bone Joint Surg [Br] 1990;72-B:9–13.
43. Crawford RW, Psychoyios V, Gie G, Ling R, Murray D. Incomplete cement man-tles in the sagittal femoral plane: an anatomical explanation. Acta Orthop Scand1999;70:596–598.
44. González Della Valle A, Piccaluga F, Alfie V, Salvati EA. Polymethyl-mathacrylate venogram after total hip arthroplasty. A report of six cases and reviewof the literature. Hip Int 2003;13:184–188.
45. Comba F, González Della Valle A, Salvati EA. The role of surface finish on the sur-vivorship of cemented femoral stems for total hip arthroplasty. Minerva Ortop Trau-matol 2005;56:65–79.
46. Crowninshield RD, Jennings JD, Laurent ML, Maloney WJ. Cemented femoralcomponent surface finish mechanics. Clin Orthop Relat Res 1998;355:90–102.