
High Risk Pregnancy HB Tranx
12
SUBJECT: ObstetricsandGynecology Transcriber:MilesFernandez TOPIC:HighRiskPregnancy/Antepartum Editor:SarahSy-Santos andIntrapartumAssessment Lecturer:JennyLynnY.Vidanes,MD,DPOGS,FPSMFM NumberofPages:11 Legend: @ Things she stressed na most likely lalabas High Risk Pregnancy Description: - Pregnancies where there is an increased risk of maternal of fetal morbidity and mortality - Perinatal events have significant role in infant mortality - Fetal deaths may occur during antepartum and intrrapartum Attributed by: 30% Asphyxia (IUGR, Prolonged Gestation) 30% Maternal Complications 15% Congenital Anomalies 20% UNKNOWN etiology 5% Infection High Risk Factors A. Maternal Factors - Maternal Age o Age is less than 18 years old à Lack of physical or emotional maturity for pregnancy o Multipara > 35 years old à Greater exposure to infections/diseases; increased risk for developmental abnormalties o Woman greater than or equal to 35 years of age had a 2 fold greater risk for fetal death (Fretts, et al.) o Fetal deaths are highest in teenagers (< 18 years old) and women (> 35 years old) (Denmark data) - Maternal Height o 60 inches (153 cm) or less à Increased risk for cephalo pelvic disprop ortion o Increased rate for birth trauma, caesarean section, congenital anomalies, and prematurity o 42% contracted pelvis - Maternal Weight o Obesity/Abnormal BMI causes: § Increased fetal growth § Medical Complications (hypertension and diabetes mellitus) § Increased need for operative delivery § Increased still birth and neonatal death § Obesity increases propensity for cardiovascular disease - Social Factors o Smoking à Teratogenic § Intrauterine Growth Restrictions § It would induce vascular damage, leading to placental insufficiency o Drugs § Opium, Barbiturates, Amphetamines, and Methadone: Low birth weight § Tetracyclinw: Brownish staining of deciduous teeth § Chloramphenicol: Gray's Syndrome à Ash gray cyanosis of baby due to vascular collapse; RDS § Streptomycin: Congenital Deafness o Alcohol à Fetal mental retardation § Delerium Tremens § Craniofacial defect § Limb defects Cardiovascular defects B. Obstetric History - Multiparity (>5) - Abruptio Placen ta - Placenta Previa à displacement of placenta anterior to fetal head; the placenta "blocks" the birth canal - Postpartum Haemorrhage - Uterine Rupture - Twinning - Dysfunctional Labor - Congenital anomalies C. PROM and Preterm Birth - Cord prolapsed - Intrauterine amniotic infection - Respiratory distress syndrome - Intraventricular haemorrhage à preterm - Necrotizing enterocolitis à preterm D. Fetal Growth Disorders - IUGR o Prematurity, Death - Fetal Macrosomia o Asphyxia o Fetal distress o Trauma o Vaginal lacerations o Uterine atony à decreased contractions due to over stretched uterus E. Amniotic fluid abnormalities - Polyhydramnios (> 24 cm) - Oligohydramnios (< 5 cm) F. Post-term pregnancy - Sharp rise in both fetal and neonatal mortality - Fetal injury from fetopelvic disproportion - Asphyxial dama ge from fetal distress wi th increased chanc e of mental subnormality and neurologic deficit G. Maternal Medical Conditions - Renal diseases à increased risk for fetal pulmonary edema - Diabetes Mellitus à macrosomic baby - Thyroid disorders o Hyperthyroidism à tachycardia, hepatosplenomegaly, IUGR, craniosyntosis o Hypothyroidismà Neurologic abnormalities, respiratory difficulty, dysmorphic facies, hypotonia - Cardiovascular disorders à predisposition to eclampsia - Respiratory disorders - Hematologic disorders - Anemia - Malnutritionà LBW infant
-
Upload
angeliquepastrana -
Category
Documents
-
view
226 -
download
0
Transcript of High Risk Pregnancy HB Tranx
7/28/2019 High Risk Pregnancy HB Tranx
http://slidepdf.com/reader/full/high-risk-pregnancy-hb-tranx 1/11
SUBJECT:ObstetricsandGynecology Transcriber:MilesFernandezTOPIC:HighRiskPregnancy/Antepartum Editor:SarahSy-SantosandIntrapartumAssessment
Lecturer:JennyLynnY.Vidanes,MD,DPOGS,FPSMFM NumberofPages:11
Legend: @ Things she stressed na most likely lalabas
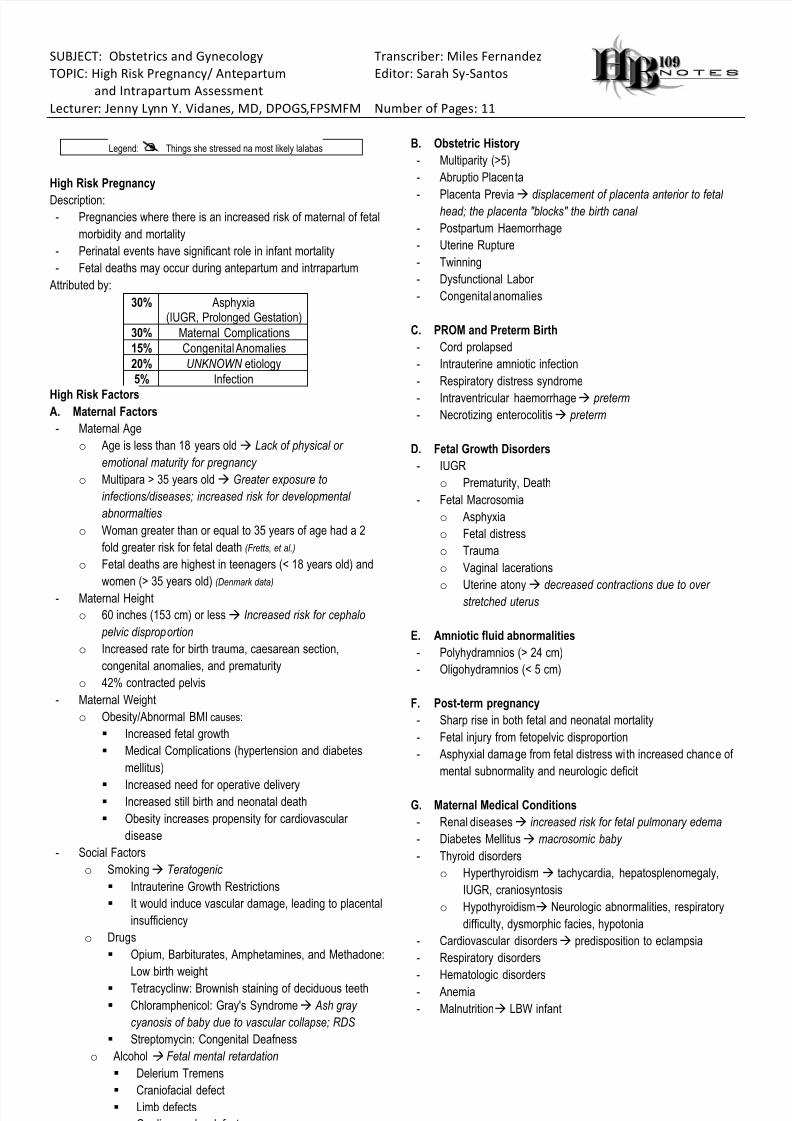
High Risk Pregnancy
Description:- Pregnancies where there is an increased risk of maternal of fetal
morbidity and mortality
- Perinatal events have significant role in infant mortality
- Fetal deaths may occur during antepartum and intrrapartum
Attributed by:
30% Asphyxia(IUGR, Prolonged Gestation)
30% Maternal Complications
15% Congenital Anomalies
20% UNKNOWN etiology
5% Infection
High Risk Factors A. Maternal Factors
- Maternal Age
o Age is less than 18 years old à Lack of physical or
emotional maturity for pregnancy
o Multipara > 35 years old à Greater exposure to
infections/diseases; increased risk for developmental
abnormalties
o Woman greater than or equal to 35 years of age had a 2
fold greater risk for fetal death (Fretts, et al.)
o Fetal deaths are highest in teenagers (< 18 years old) and
women (> 35 years old) (Denmark data)
- Maternal Height
o 60 inches (153 cm) or less à Increased risk for cephalo
pelvic disproportion
o Increased rate for birth trauma, caesarean section,
congenital anomalies, and prematurity
o 42% contracted pelvis
- Maternal Weight
o Obesity/Abnormal BMI causes:
§ Increased fetal growth
§ Medical Complications (hypertension and diabetes
mellitus)
§ Increased need for operative delivery§ Increased still birth and neonatal death
§ Obesity increases propensity for cardiovascular
disease
- Social Factors
o Smokingà Teratogenic
§ Intrauterine Growth Restrictions
§ It would induce vascular damage, leading to placental
insufficiency
o Drugs
§ Opium, Barbiturates, Amphetamines, and Methadone:
Low birth weight
§ Tetracyclinw: Brownish staining of deciduous teeth
§ Chloramphenicol: Gray's Syndromeà Ash gray
cyanosis of baby due to vascular collapse; RDS
§ Streptomycin: Congenital Deafness
o Alcohol à Fetal mental retardation
§ Delerium Tremens
§ Craniofacial defect
§ Limb defects
§ Cardiovascular defects
§ IUGR
B. Obstetric History
- Multiparity (>5)
- Abruptio Placenta
- Placenta Previaà displacement of placenta anterior to fetal head; the placenta "blocks" the birth canal
- Postpartum Haemorrhage
- Uterine Rupture
- Twinning
- Dysfunctional Labor
- Congenital anomalies
C. PROM and Preterm Birth
- Cord prolapsed
- Intrauterine amniotic infection
- Respiratory distress syndrome
- Intraventricular haemorrhageà preterm
- Necrotizing enterocolitisà preterm
D. Fetal Growth Disorders
- IUGR
o Prematurity, Death
- Fetal Macrosomia
o Asphyxia
o Fetal distress
o Trauma
o Vaginal lacerations
o Uterine atony
à decreased contractions due to over
stretched uterus
E. Amniotic fluid abnormalities
- Polyhydramnios (> 24 cm)
- Oligohydramnios (< 5 cm)
F. Post-term pregnancy
- Sharp rise in both fetal and neonatal mortality
- Fetal injury from fetopelvic disproportion
- Asphyxial damage from fetal distress with increased chance of
mental subnormality and neurologic deficit
G. Maternal Medical Conditions
- Renal diseasesà increased risk for fetal pulmonary edema
- Diabetes Mellitusà macrosomic baby
- Thyroid disorders
o Hyperthyroidism à tachycardia, hepatosplenomegaly,
IUGR, craniosyntosis
o Hypothyroidismà Neurologic abnormalities, respiratory
difficulty, dysmorphic facies, hypotonia
- Cardiovascular disordersà predisposition to eclampsia
- Respiratory disorders
- Hematologic disorders
- Anemia
- Malnutritionà LBW infant
7/28/2019 High Risk Pregnancy HB Tranx
http://slidepdf.com/reader/full/high-risk-pregnancy-hb-tranx 2/11
High Risk Clinic
- Pregnancies at extremes of reproductive age
o 17 years and below
o Primigravida 35 years and above
- Placenta Previaà increased chance of bleeding preterm
@Poor Obstetrical History
2 Consecutive Abortions 3 or more Repeated Abortions
Previous Preterm Delivery Previous Fetal and/or Neonatal
DeathPrevious birth with Congenitalanomaly
- Diagnosed medical conditionsà Hypertension, Diabetes
- Generative tract disorders
- Co-existing trophoblastic diseases or had a trophoblastic disease
within the last year
- Psychiatric conditions
- Problems in fetal, aging, structure, or size
- Malignancies (genital and extragenital)
- Polyhydramnios or Oligohydramnios
@ Intermittent Auscultation
Low Risk Pregnancy High Risk Pregnancy
1st stage of labor
Monitor every 30minutes
Monitor every 15minutes
2nd stage of labor
Monitor every 15minutes
Monitor every 5 minutes
Electronic Fetal Monitoring
- Done only for high risk patients
- Types:
a. External (Indirect)à Ultrasound Doppler Principle
b. Internal (Direct)à Electrode attached to fetal scalp
- Increased the overall CS rate (relative risk [RR], 1.66; 95%
confidence interval, 1.30-2.13) and the CS rate for abnormal Fetal
Heart Rate (FHR) or acidosis or both
- Increased the risk of both vacuum and forceps operative vaginal
delivery
- The use of Electronic Fetal Monitoring (EFM)
a. Reduces the risk of neonatal seizures (RR, 0.50; 95% CI,
0.31 - 0.80) à Only advantage
b. Does not reduce the perinatal mortality (RR, 0.85; 95% CI,
0.59 - 1.23)
c. Does not reduce the risk of cerebral palsy (RR 1.74; 95% CI,
0.97 - 3.11)
- Continuous EFM should be offered and is recommended for HighRisk Pregnancies
- Current evidence does not support the use of admission tocogram
in low risk pregnancy (Leve III, C)
From the book: Although maternal heart tones are 5x higher than the
baby’s, the machine selectively picks up the fetal heart tone. So one
way for the phycisan to know if the baby is dead is if the machine
already picks up the maternal heart tone.
Antepartum Surveillance à focuses on fetal physical activites (well being)
Intrapartum Surveillance à focuses on fetal heart rate analysis
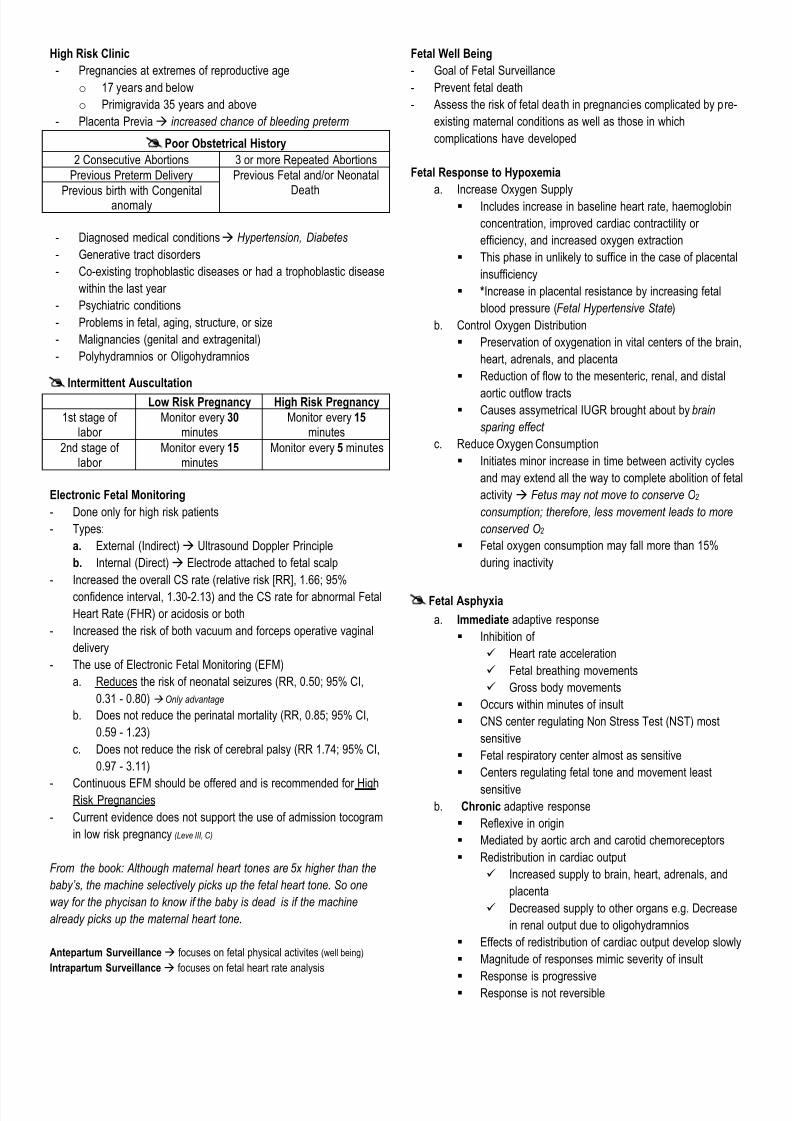
Fetal Well Being
- Goal of Fetal Surveillance
- Prevent fetal death
- Assess the risk of fetal death in pregnancies complicated by pre-
existing maternal conditions as well as those in which
complications have developed
Fetal Response to Hypoxemia
a. Increase Oxygen Supply
§ Includes increase in baseline heart rate, haemoglobin
concentration, improved cardiac contractility or
efficiency, and increased oxygen extraction
§ This phase in unlikely to suffice in the case of placental
insufficiency
§ *Increase in placental resistance by increasing fetal
blood pressure (Fetal Hypertensive State)
b. Control Oxygen Distribution
§ Preservation of oxygenation in vital centers of the brain,
heart, adrenals, and placenta
§ Reduction of flow to the mesenteric, renal, and distal
aortic outflow tracts§ Causes assymetrical IUGR brought about by brain
sparing effect
c. Reduce Oxygen Consumption
§ Initiates minor increase in time between activity cycles
and may extend all the way to complete abolition of fetal
activity à Fetus may not move to conserve O2
consumption; therefore, less movement leads to more
conserved O2
§ Fetal oxygen consumption may fall more than 15%
during inactivity
@Fetal Asphyxia
a. Immediate adaptive response
§ Inhibition of
ü Heart rate acceleration
ü Fetal breathing movements
ü Gross body movements
§ Occurs within minutes of insult
§ CNS center regulating Non Stress Test (NST) most
sensitive
§ Fetal respiratory center almost as sensitive
§ Centers regulating fetal tone and movement least
sensitive
b. Chronic adaptive response
§ Reflexive in origin
§ Mediated by aortic arch and carotid chemoreceptors
§ Redistribution in cardiac output
ü Increased supply to brain, heart, adrenals, and
placenta
ü Decreased supply to other organs e.g. Decrease
in renal output due to oligohydramnios
§ Effects of redistribution of cardiac output develop slowly
§ Magnitude of responses mimic severity of insult
§ Response is progressive
§ Response is not reversible
7/28/2019 High Risk Pregnancy HB Tranx
http://slidepdf.com/reader/full/high-risk-pregnancy-hb-tranx 3/11
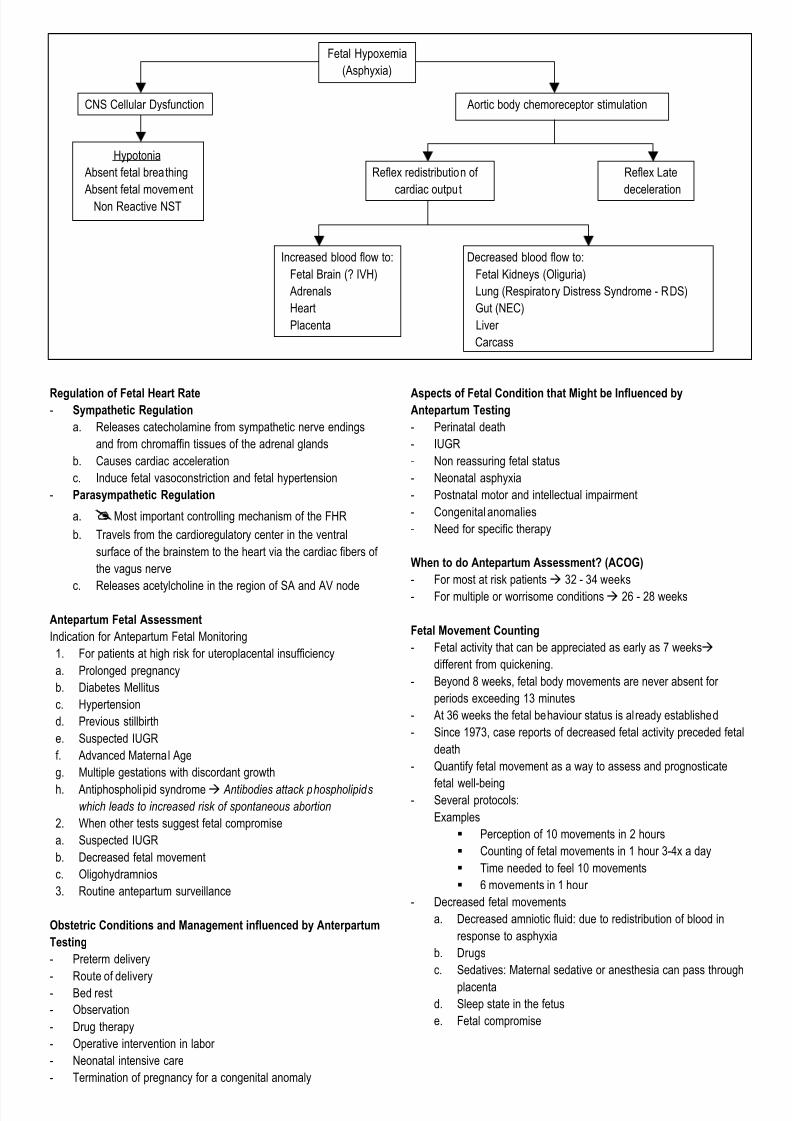
Fetal Hypoxemia
(Asphyxia)
CNS Cellular Dysfunction Aortic body chemoreceptor stimulation
Hypotonia
Absent fetal breathing Reflex redistribution of Reflex Late
Absent fetal movement cardiac output deceleration
Non Reactive NST
Increased blood flow to: Decreased blood flow to:
Fetal Brain (? IVH) Fetal Kidneys (Oliguria)
Adrenals Lung (Respiratory Distress Syndrome - RDS)
Heart Gut (NEC)
Placenta Liver
Carcass
Regulation of Fetal Heart Rate- Sympathetic Regulation
a. Releases catecholamine from sympathetic nerve endings
and from chromaffin tissues of the adrenal glands
b. Causes cardiac acceleration
c. Induce fetal vasoconstriction and fetal hypertension
- Parasympathetic Regulation
a. @Most important controlling mechanism of the FHR
b. Travels from the cardioregulatory center in the ventral
surface of the brainstem to the heart via the cardiac fibers of
the vagus nerve
c. Releases acetylcholine in the region of SA and AV node
Antepartum Fetal Assessment
Indication for Antepartum Fetal Monitoring
1. For patients at high risk for uteroplacental insufficiency
a. Prolonged pregnancy
b. Diabetes Mellitus
c. Hypertension
d. Previous stillbirth
e. Suspected IUGR
f. Advanced Maternal Age
g. Multiple gestations with discordant growth
h. Antiphospholipid syndrome à Antibodies attack phospholipids
which leads to increased risk of spontaneous abortion
2. When other tests suggest fetal compromise
a. Suspected IUGR
b. Decreased fetal movement
c. Oligohydramnios
3. Routine antepartum surveillance
Obstetric Conditions and Management influenced by Anterpartum
Testing
- Preterm delivery
-
Route of delivery- Bed rest
- Observation
- Drug therapy
- Operative intervention in labor
- Neonatal intensive care
- Termination of pregnancy for a congenital anomaly
Aspects of Fetal Condition that Might be Influenced byAntepartum Testing
- Perinatal death
- IUGR
- Non reassuring fetal status
- Neonatal asphyxia
- Postnatal motor and intellectual impairment
- Congenital anomalies
- Need for specific therapy
When to do Antepartum Assessment? (ACOG)
- For most at risk patientsà 32 - 34 weeks
- For multiple or worrisome conditions à 26 - 28 weeks
Fetal Movement Counting
- Fetal activity that can be appreciated as early as 7 weeksà
different from quickening.
- Beyond 8 weeks, fetal body movements are never absent for
periods exceeding 13 minutes
- At 36 weeks the fetal behaviour status is already established
- Since 1973, case reports of decreased fetal activity preceded fetal
death
- Quantify fetal movement as a way to assess and prognosticate
fetal well-being- Several protocols:
Examples
§ Perception of 10 movements in 2 hours
§ Counting of fetal movements in 1 hour 3-4x a day
§ Time needed to feel 10 movements
§ 6 movements in 1 hour
- Decreased fetal movements
a. Decreased amniotic fluid: due to redistribution of blood in
response to asphyxia
b. Drugs
c. Sedatives: Maternal sedative or anesthesia can pass through
placenta
d. Sleep state in the fetus
e. Fetal compromise
7/28/2019 High Risk Pregnancy HB Tranx
http://slidepdf.com/reader/full/high-risk-pregnancy-hb-tranx 4/11
Pros and Cons of Fetal Movement Counting
PROS CONS
Simple Intrude on the woman's time
Can be Done at Home Unnecessary anxiety to the mother
No human or material resourcesneeded
Staff overload as additionalinvestigations may have to be done
exclusive to fetal compromise
Might increase antenatal admissions,obstetric interventions, and
prematurity
- Related Studies:
a. Four studies, involving 71,370 women, were incuded in this
review; 68,654 in one cluster-randomised trial
b. Not enough evidence to influence practice
c. No trials compared fetal movement counting with no fetal
movement counting
d. Results neither confirm nor refute the effectiveness of fetal
movement counting as a method of fetal surveillance
e. Not enough evidence to recommend or not to recommend
formal fetal movement counting
f. Insufficient data to assess stillbirths accurately
g. Woman to count distinct fetal movements on a daily basis
after 28 weeks AOG
h. Perception of 10 distinct movements in up to 2 hours is
considered reassuring
i. The counting can be discontinued for that day after 10
movements
Fetal Behavioral States
1F: Quiescence (quiet sleep)
2F: Frequent gross body movements, Continuous eye movements, and
Oscillation of FHR (REM sleep)3F: Continuous eye movements, Without body movements, No
increase in FHR
4F: Vigorous body movements, Continuous eye movements (Awake
state)
- Fetuses spend most of their time in states 1F and 2F
- Sleep Awake Cycles
a. Independent of maternal sleep awake cycles
b. 20 - 75 minutes (mean: 40 minutes)
Biophysical Profile
- Non-invasive test that combines data from 2 sources:a. Ultrasound imaging
b. Fetal heart rate monitoring
- It predicts the presence or absence of fetal asphyxia and the risk
of death during the antenatal period
Parameters
a. Fetal breathing movements
b. Fetal movement
c. Fetal tone
d. Fetal heart rate activity
e. Amniotic fluid volume
Markers
f. Acute Markers
§ Fetal breathing movements
§ Fetal movement
§ Fetal tone
§ Fetal heart rate activity
b. Chronic Marker
§ Amniotic fluid volume
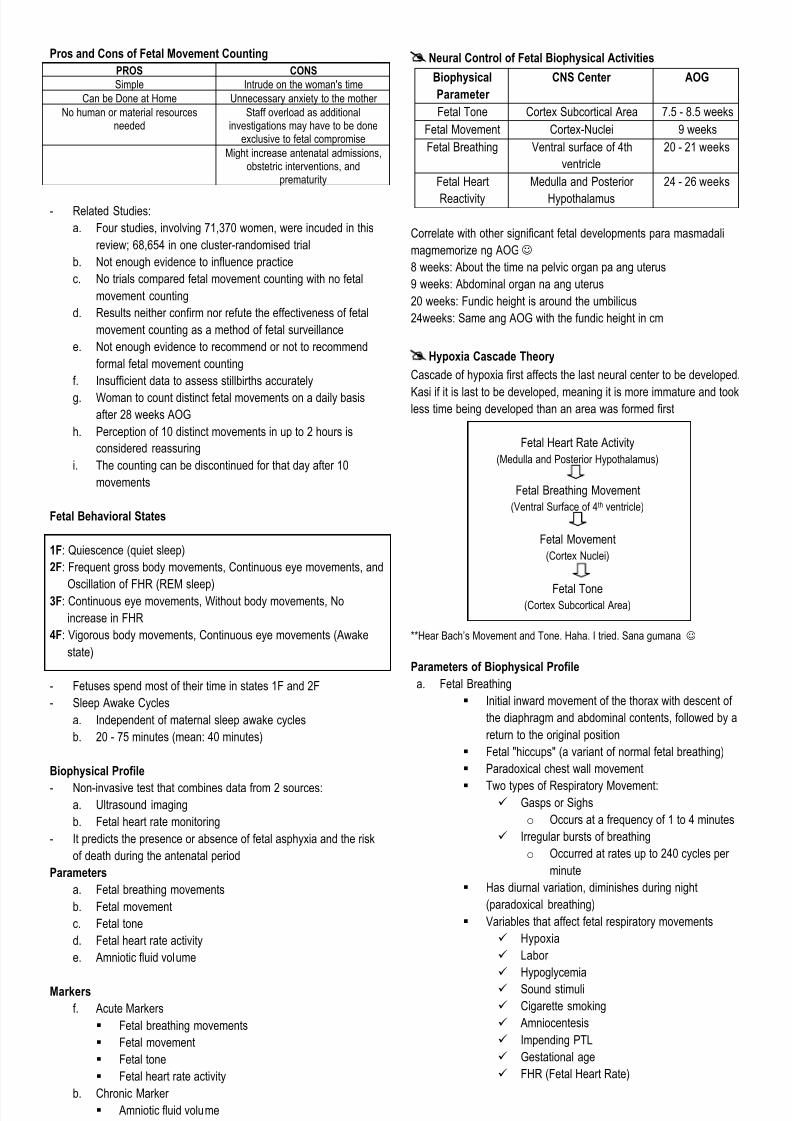
@Neural Control of Fetal Biophysical Activities
Biophysical
Parameter
CNS Center AOG
Fetal Tone Cortex Subcortical Area 7.5 - 8.5 weeks
Fetal Movement Cortex-Nuclei 9 weeks
Fetal Breathing Ventral surface of 4th
ventricle
20 - 21 weeks
Fetal Heart
Reactivity
Medulla and Posterior
Hypothalamus
24 - 26 weeks
Correlate with other significant fetal developments para masmadali
magmemorize ng AOGJ
8 weeks: About the time na pelvic organ pa ang uterus
9 weeks: Abdominal organ na ang uterus
20 weeks: Fundic height is around the umbilicus
24weeks: Same ang AOG with the fundic height in cm
@Hypoxia Cascade Theory
Cascade of hypoxia first affects the last neural center to be developed.
Kasi if it is last to be developed, meaning it is more immature and tookless time being developed than an area was formed first
Fetal Heart Rate Activity
(Medulla and Posterior Hypothalamus)
Fetal Breathing Movement
(Ventral Surface of 4th ventricle)
Fetal Movement
(Cortex Nuclei)
Fetal Tone(Cortex Subcortical Area)
**Hear Bach’s Movement and Tone. Haha. I tried. Sana gumana J
Parameters of Biophysical Profile
a. Fetal Breathing
§ Initial inward movement of the thorax with descent of
the diaphragm and abdominal contents, followed by a
return to the original position
§ Fetal "hiccups" (a variant of normal fetal breathing)
§ Paradoxical chest wall movement
§ Two types of Respiratory Movement:ü Gasps or Sighs
o Occurs at a frequency of 1 to 4 minutes
ü Irregular bursts of breathing
o Occurred at rates up to 240 cycles per
minute
§ Has diurnal variation, diminishes during night
(paradoxical breathing)
§ Variables that affect fetal respiratory movements
ü Hypoxia
ü Labor
ü Hypoglycemia
ü Sound stimuli
ü Cigarette smoking
ü Amniocentesis
ü Impending PTL
ü Gestational age
ü FHR (Fetal Heart Rate)
7/28/2019 High Risk Pregnancy HB Tranx
http://slidepdf.com/reader/full/high-risk-pregnancy-hb-tranx 5/11
b. Fetal Tone
§ Limb or trunk extension with return to flexion
§ Opening of hand with finger and thumb extension with
return to closed-fist formation
§ Hand remains in flexed formation for the entire 30
minute period
c.
Amniotic Fluid Volume§ Largest single vertical pocket
§ Chronic Marker
§ Amniotic fluid index
ü Oligohydramnios: < 5 cm
ü Low normal: 5 - 7.9 cm
ü Normal: 8 - 18 cm
ü High Normal: 18.1 - 24 cm
ü Polyhydramnios: > 24 cm
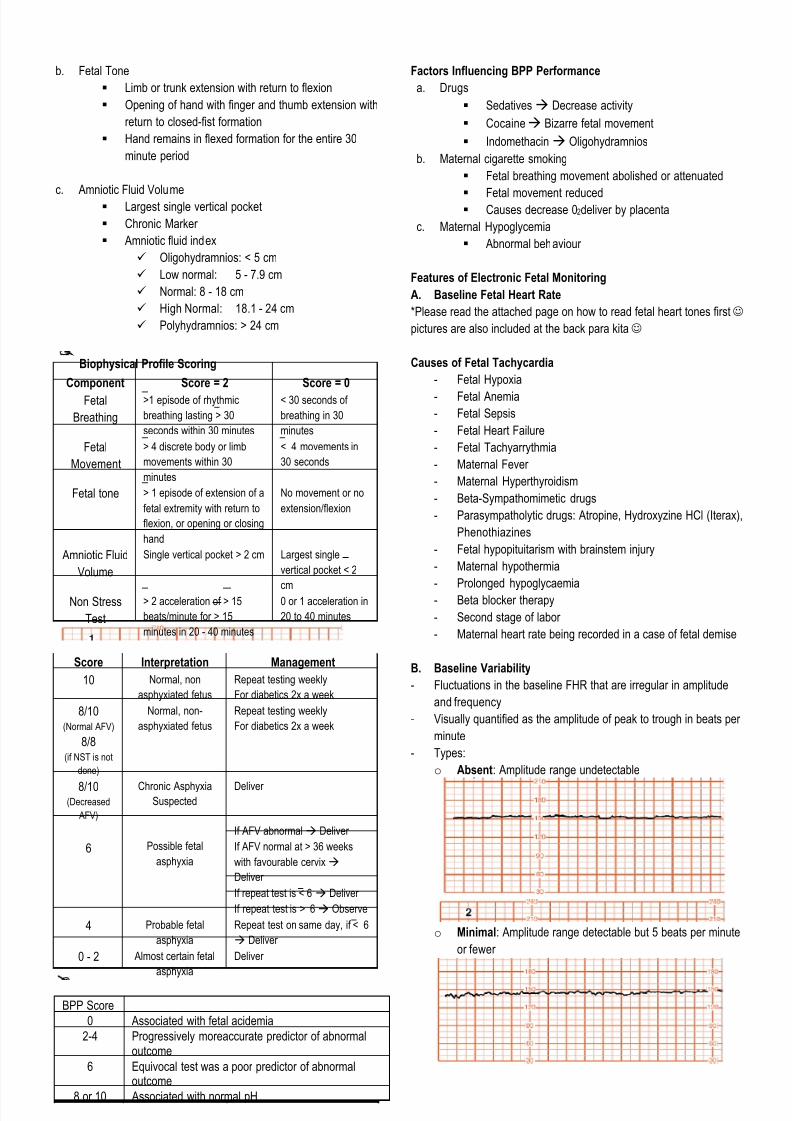
@ Biophysical Profile Scoring
Component Score = 2 Score = 0
Fetal
Breathing
>1 episode of rhythmic
breathing lasting > 30
seconds within 30 minutes
< 30 seconds of
breathing in 30
minutes
Fetal
Movement
> 4 discrete body or limb
movements within 30
minutes
< 4 movements in
30 seconds
Fetal tone > 1 episode of extension of a
fetal extremity with return to
flexion, or opening or closing
hand
No movement or no
extension/flexion
Amniotic Fluid
Volume
Single vertical pocket > 2 cm Largest single
vertical pocket < 2
cmNon Stress
Test
> 2 acceleration of > 15
beats/minute for > 15
minutes in 20 - 40 minutes
0 or 1 acceleration in
20 to 40 minutes
Score Interpretation Management
10 Normal, non
asphyxiated fetus
Repeat testing weekly
For diabetics 2x a week
8/10(Normal AFV)
8/8(if NST is not
done)
Normal, non-
asphyxiated fetus
Repeat testing weekly
For diabetics 2x a week
8/10(Decreased
AFV)
Chronic AsphyxiaSuspected
Deliver
6 Possible fetal
asphyxia
If AFV abnormal à Deliver
If AFV normal at > 36 weeks
with favourable cervixà
Deliver
If repeat test is < 6 à Deliver
If repeat test is > 6à Observe
4 Probable fetal
asphyxia
Repeat test on same day, if < 6
à Deliver
0 - 2 Almost certain fetal
asphyxia
Deliver
BPP Score
0 Associated with fetal acidemia
2-4 Progressively moreaccurate predictor of abnormaloutcome
6 Equivocal test was a poor predictor of abnormaloutcome
8 or 10 Associated with normal pH
Factors Influencing BPP Performance
a. Drugs
§ Sedatives à Decrease activity
§ Cocaineà Bizarre fetal movement
§ Indomethacin à Oligohydramnios
b. Maternal cigarette smoking
§ Fetal breathing movement abolished or attenuated
§ Fetal movement reduced§ Causes decrease 02deliver by placenta
c. Maternal Hypoglycemia
§ Abnormal behaviour
Features of Electronic Fetal Monitoring
A. Baseline Fetal Heart Rate
*Please read the attached page on how to read fetal heart tones first J
pictures are also included at the back para kita J
Causes of Fetal Tachycardia
- Fetal Hypoxia
- Fetal Anemia
- Fetal Sepsis
- Fetal Heart Failure
- Fetal Tachyarrythmia
- Maternal Fever
- Maternal Hyperthyroidism
- Beta-Sympathomimetic drugs
- Parasympatholytic drugs: Atropine, Hydroxyzine HCl (Iterax),
Phenothiazines
- Fetal hypopituitarism with brainstem injury
- Maternal hypothermia
-
Prolonged hypoglycaemia- Beta blocker therapy
- Second stage of labor
- Maternal heart rate being recorded in a case of fetal demise
B. Baseline Variability
- Fluctuations in the baseline FHR that are irregular in amplitude
and frequency
- Visually quantified as the amplitude of peak to trough in beats per
minute
- Types:
o Absent: Amplitude range undetectable
o Minimal: Amplitude range detectable but 5 beats per minute
or fewer
7/28/2019 High Risk Pregnancy HB Tranx
http://slidepdf.com/reader/full/high-risk-pregnancy-hb-tranx 6/11
o Moderate (Normal) Amplitude ranges 6 - 25 beats per
minute
o Marked: Amplitude range greater than 25 beats per minute
Causes of Decreased FHR variability
- Fetal sleep cycles
- Hypoxia/Acidosis
- Extreme prematurity
- Congenital anomalies
- Fetal tachycardia
- Pre-existing neurological abnormality
- Drugs: CNS depressants, parasympatholytics (atropine), Beta
Blockers
C. Periodic Changes
Acceleration
- Abrupt increase in FHR: Onset to peak in < 30 seconds
- Peak: > 15 bpm lasting 15 seconds from onset to return to
baseline
- Prolonged acceleration: > 2 minutes but less than 10 minutes
- Acceleration > 10 minutes = Baseline change
- A visually apparent abrupt increase (onset to peak in less than
30 seconds) in the FHR
- 32 weeks of gestation and beyond
§ Peak of 15 beats per minute or more above baseline, withduration of 15 seconds or more but less than 2 minutes
from onset to return
- Before 32 weeks of gestations
§ Acceleration has a peak of 10 beats per minute or more
above baseline, with duration of 10 seconds or more but
less than 2minutes from onset to return
- Prolonged acceleration
§ Lasts for 2 minutes or more but less than 10 minutes in
duration
- Baseline change
§ Acceleration lasts 10 minutes or longer
Deceleration
- Transient episode of slowing of the fetal heart rate beow the
baseline level of more than 15 bpm and lasting 15 seconds or
more
- If rate is below 110 bpm and duration is > 10 minutes à
bradycardia
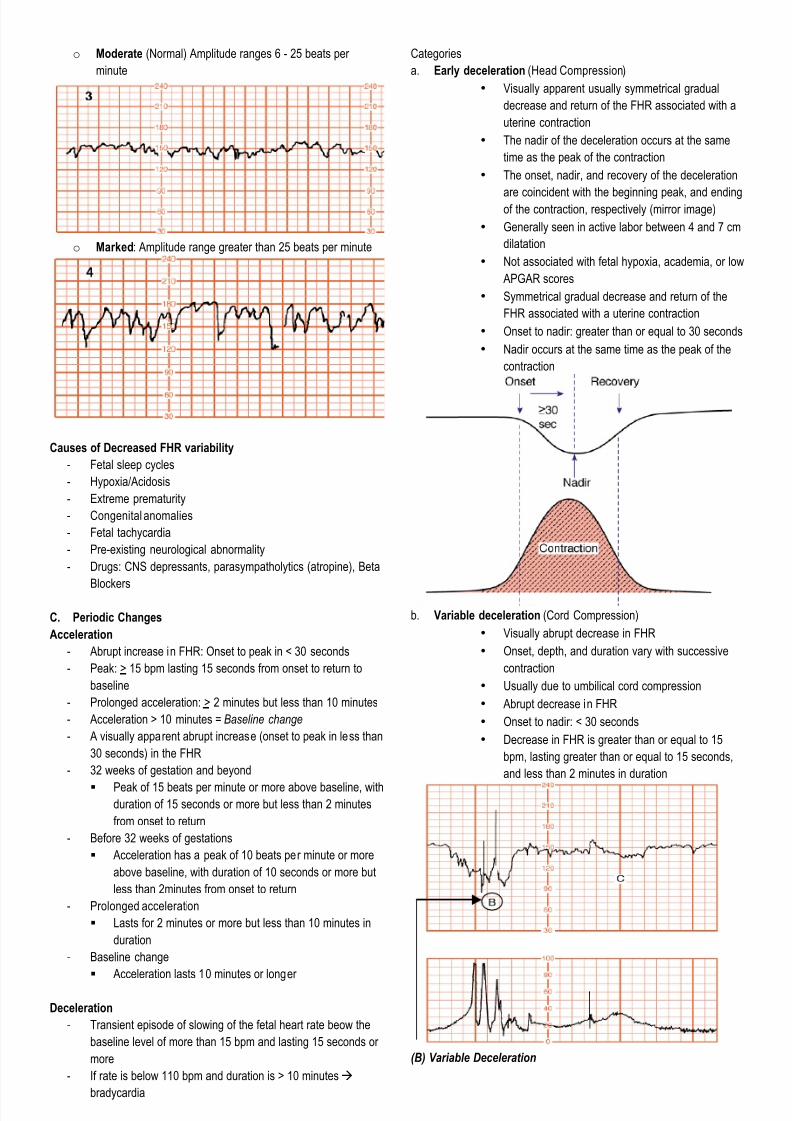
Categories
a. Early deceleration (Head Compression)
• Visually apparent usually symmetrical gradual
decrease and return of the FHR associated with a
uterine contraction
• The nadir of the deceleration occurs at the same
time as the peak of the contraction
• The onset, nadir, and recovery of the deceleration
are coincident with the beginning peak, and endingof the contraction, respectively (mirror image)
• Generally seen in active labor between 4 and 7 cm
dilatation
• Not associated with fetal hypoxia, academia, or low
APGAR scores
• Symmetrical gradual decrease and return of the
FHR associated with a uterine contraction
• Onset to nadir: greater than or equal to 30 seconds
• Nadir occurs at the same time as the peak of the
contraction
b. Variable deceleration (Cord Compression)
• Visually abrupt decrease in FHR
• Onset, depth, and duration vary with successive
contraction
• Usually due to umbilical cord compression
• Abrupt decrease in FHR
• Onset to nadir: < 30 seconds
• Decrease in FHR is greater than or equal to 15
bpm, lasting greater than or equal to 15 seconds,
and less than 2 minutes in duration
(B) Variable Deceleration
7/28/2019 High Risk Pregnancy HB Tranx
http://slidepdf.com/reader/full/high-risk-pregnancy-hb-tranx 7/11
7/28/2019 High Risk Pregnancy HB Tranx
http://slidepdf.com/reader/full/high-risk-pregnancy-hb-tranx 8/11
Non Stress Test (NST)
- Done without uterine contractions
- Fetal heart rate of a fetus that is not acidotic or neurologically
depressed will temporarily accelerate with fetal movements
- Heart rate reactivity thought to be a good indicator of normal fetal
autonomic function
- Diurnal rhythm in mature fetuses:
• Acme (145 bpm): midday
• Nadir (120 bpm): early morning hours
Parameter @Normal
(Reactive)
Atypical
(Nonreactive)
Abnormal
(Nonreactive)
Baseline 100 - 160 100-110
>160, < 30
minutes
Rising Baseline
< 100
>160, >30
minutes
Erratic baseline
Variability 6 - 25
< 5 for < 40
minutes
< 5 for 40 - 80
minutes
< 5 for > 80
minutes
> 25 for > 10
minutes
Sinusoidal
Decelerations None or
occasional
but < 30
seconds
Variable
deceleration 30 -
60 seconds
Variable for > 60
seconds
Late
decelerations
Accelerations
Term
> 6 at > 15
bpm for 15
seconds
< 40 minute
testing
< 2 at > 15 bpm
for 15 seconds in
40 - 80 minutes
< 2 at > 15 bpm
for 15 seconds >
80 minutes
Accelerations
< 32 weeks
> 2 at > 10
bpm for 10
seconds
< 40 minute
testing
< 2 > 10 bpm for
10 seconds in 40
- 80 minutes
< 2 > 10 bpm for
10 seconds in >
80 minutes
Action Further
assessment
optional
Further
assessment
required
Urgent action
required
Reactive VS Non Reactive NST
REACTIVE NON-REACTIVE
BFHR 130-135 bpm 150 bpm
Variability Moderate Minimal to absent
Accelerations + -
Decelerations - -
- Loss of reactivity may be associated:
• Fetal Sleep Cycles
• Fetal Acidosis
• Central nervous system depression
- Indications
• It is initiated at 32 weeks AOG on a weekly basis or earlier or
more frequent in very high risk situations
• Twice weekly for women with post term pregnancy, multifetal
gestation, type 1 diabetes, IUGR, and PIH
Causes of FALSE NEGATIVE NST
- Prematurity
- Maternal smoking and stress
- Malnutrition
§ Glycemic levels§ Fetal sleep states
Causes of FALSE POSITIVE NST
§ Caffiene
§ Cocaine
§ Morphine
§ Sedatives
§ Alcohol
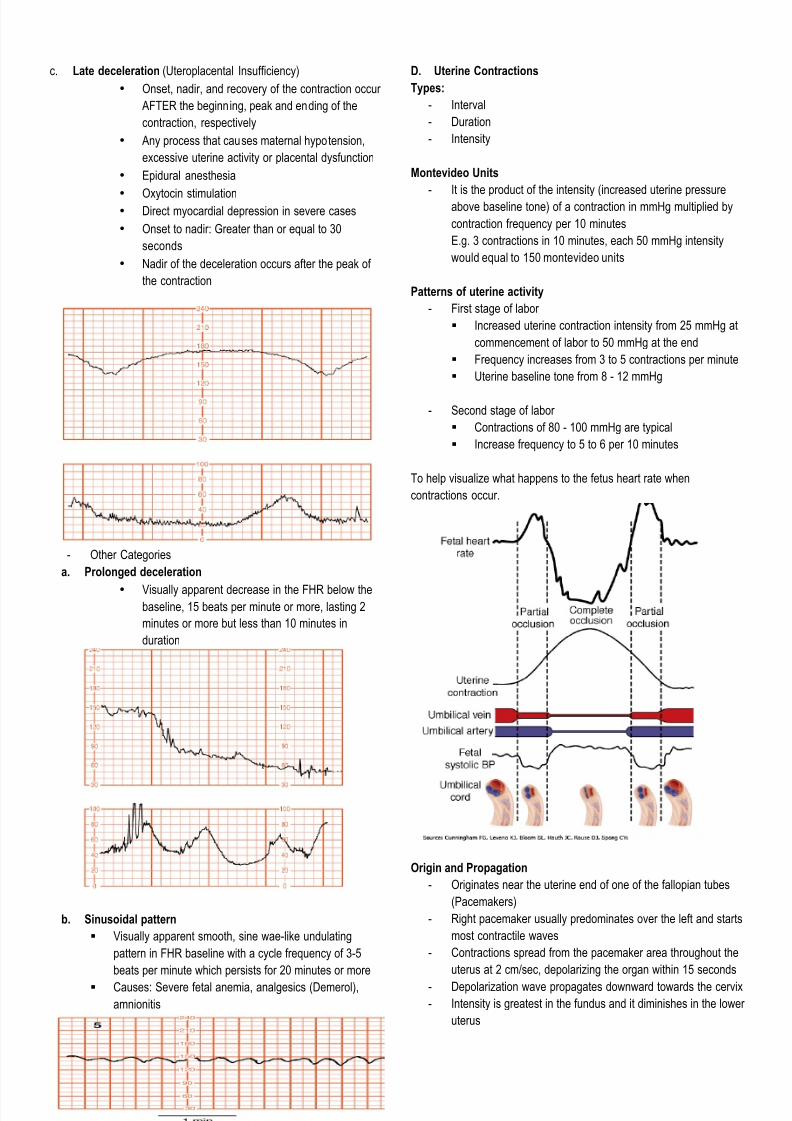
Contraction Stress Test (CST)
- Used to determine if there is Late deceleration à Uteroplacental
insufficiency
- Detection of presence or absence of FHR decelerations in
response to either spontaneous or induced uterine contraction
- Fetus with reduced placental reserve will develop transient fetal
hypoxemia in association with the interruption of uteroplacental
blood flow caused by contractions
- CST Method
- Mother in semi-recumbent position or in a left lateral tilt
- Initial trace of 15 minutes to determine baseline FHR and to
note for spontaneous contractions
- Induction of contraction:
- Intravenous oxytocin
• 10 'u'/1 L saline titrated (not to exceed 60 m'u'/min)
• Goal: 3 contractions in 10 minutes
- Manual Nipple Stimulation
• Not to exceed 2 minutes in duration, not less than 5
minutes apart
• Goal 3 contractions in 10 minutes
Contraindications for CST
- Absolute
§ Placenta previa
§ Chronic fetal abruption
§ Proven or suggested cord presentation
§ Upper uterine segment scar
- Relative
§ Pregnancy at risk for premature delivery
§ E.g. Multiple gestation, Incompetence
@ Interpretation
Category Interpretation
Normal or Negative No late or significant variable decelerationsPositive Late decelerations following 50% or more of
contractions
Equivocal-suspicious Intermittent late decelerations or significant
variable decelerations
Equivocal -
hyperstimulatory
Fetal heart rate decelerations with contractions >
every 2 minutes or lasting longer than 90
seconds
Unsatisfactory Fewer than three contractions in 10 minutes or
an uninterpretable tracing
*Take Note:
Negative CSTà Good indicator of fetal health
Positive CSTà Relatively poor predictor of fetal compromise
CSTà Best used in combination with other tests of fetal well-being
Intrapartum Fetal Assessment
- Done when the patient is already in labor
Fetal Heart Rate Analysis
- The primary means in which a fetus is evaluated for adequacy of
oxygenation
7/28/2019 High Risk Pregnancy HB Tranx
http://slidepdf.com/reader/full/high-risk-pregnancy-hb-tranx 9/11
7/28/2019 High Risk Pregnancy HB Tranx
http://slidepdf.com/reader/full/high-risk-pregnancy-hb-tranx 10/11

7/28/2019 High Risk Pregnancy HB Tranx
http://slidepdf.com/reader/full/high-risk-pregnancy-hb-tranx 11/11
How to read fetal heart tones 101
Acme: Peak/ Highest point
Nadir: Trough/ Lowest point
Baseline Heart Rate Criteria:
§ Mean fetal heart rate rounded to increments of 5 beats per minute during a 10 minute segment excluding:
a. Periodic or episodic changes (e.g. acceleration,deceleration)
b. Periods of marked FHR variability (e.g. absent, minimal, marked)
c. Segments of baseline that defer by more than 25 beats per minute (only increments of 5)
§ The baseline must be for a minimum of 2 minutes in any 10 minute segment.
Here is a picture of normal FTH recording. Take note that 1 square=10 seconds. 6 squares = 1 min. The thickened line will mark 1 minute.The
vertical numbers correspond to the number of beats/minute. Each horizontal line= 10 beats. The baseline should follow the 2nd criteria. So dapat,
medyo steady/constant yung line at certain number of beats for at least 2 squares. The baseline you see in a 10 minute segment can be reported as
the range with increments of 5. So for this example, the FTR is 140-145 bpm.
Findings:Normal FHR baseline: 110 - 160 beats per minute
Tachycardia: FHR baseline values > 160 beats per minute
Bradycardia: FHR baseline values< 110 beats per minute
Acceleration
Deceleration











![Relazione mandrino.rete.ppt [modalità compatibilità]...2019/05/08 · + thal α othal Hb S β thal δβ thal Hb Lepore Hb E Hb O Arab Hb C Hb D Punjab HPFH Not a carrier α+ thal](https://static.fdocuments.in/doc/165x107/5e9a890fb98c3712227912ea/relazione-modalit-compatibilit-20190508-thal-othal-hb-s-thal.jpg)





