High Grade Glioma; What Else? El-Ghoneimy E (M.D.) – Moustafa M (M.D.) Abdulla M (M.D.) Department...
35
High Grade Glioma; What Else? El-Ghoneimy E (M.D.) – Moustafa M (M.D.) Abdulla M (M.D.) Department of Clinical Oncology Kasr El-Aini School of Medicine Cairo University Barcelona – March, 2002
-
Upload
kelsie-bays -
Category
Documents
-
view
213 -
download
1
Transcript of High Grade Glioma; What Else? El-Ghoneimy E (M.D.) – Moustafa M (M.D.) Abdulla M (M.D.) Department...

High Grade Glioma;What Else?
El-Ghoneimy E (M.D.) – Moustafa M (M.D.)Abdulla M (M.D.)
Department of Clinical OncologyKasr El-Aini School of Medicine
Cairo UniversityBarcelona – March, 2002

Neurological Deficits Already
Present at Time of
Diagnosis
Lack of Tissue Repair
Following Surgical Trauma
Current Therapeutic
Modalities are Lacking The Appropriate
Effectiveness
*2% of all malignant Diseases
*Disproportionate Morbidity & Mortality
* 3rd cause of cancer related mortality

Why Poor Prognosis?
• Incompatible with life even at a relatively small burden.
• Symptomatic at a size between 30-60 gms (3-6 X 1010 cells).
• Fatal when reaching about 100 gms (10 11 cells).
• Lack of draining lymphatics; impedes removal of necrotic debris; life-threatening ++ ICT; death of patient.

Survival Issues of Malignant Glioma
14
20
36
50
0 20 40 60 80 100
ConservativeManagement
Surgery
Surgery + Rth
Surgery + Rth + Cth
(Huncharek & Muscat, 1998)

Biological Associations:Biological Associations:
P-53 mutationsRB mutationmdm-2 overexpressionbcl-2 mutationPDGFR,PDGF-A overexpressionEGFR overexpression
Mitotic ActivityInvasion.Vascularization.Chemoresistance Radioresistance.

Complete Surgical Removal is Impossible Due to Surrounding Vital Regions.
Infiltrative Nature of The Lesion.
Limitations of Radiation Dose Delivery Because of Tolerance.
Chemo-resistance & Lack of Drug Concentration within The Lesion

Dose Escalation & Altered Fractionation Schedules
Conformal Radiation, Radiosurgery with the advent of Mutlileaf Collimators and IMRT.
The Use of Radiation Therapy

Nitrosureas: Marginal Benefit.
PCV Regimen: Minimal Improvement in TTP only in Anaplastic Astrocytoma not in G.M.
Investigational: CPT-11, Platinum Compounds, Taxanes….etc
The Use of Chemotherapeutics:

Basic Requirements for Investigational Therapies of
Malignant Gliomas:
Non Invasive. Least Morbidity. No further affection of Neurological
Insult. Not associated with further
deterioration of performance status.

Single Institution Experience

NEMROCK EXPERIENCE; 1988-2003:1988-1990
1991-1995
1997-1999
1999-2002
1999-2002
2001 - Ongoing
Whole Brain + Boost RTh vs Localized Rth in GM & AA.
Hypofractionated Rth in GM.
Lomustine/Platinum X 2 + Radical Rth Vs Radical Rth in GM & AA.
SRS Single Fraction vs Lomustine+VCR X3-6 in Recurrent or Residual GM & AA.
The Use of TEMOZOLOMIDE in High Grade Gliomas at Relapse.
Adjuvant P.O. SRT vs Conventional Rth in Low Grade Glioma

NEMROCK 1997-199860 patients with high grade glioma
Arm A29 Pts
Arm B31 Patients
CCNU/Platinum No Cth
Radical Irradiation
RadicalIrradiation
The Role of Neoadjuvant Cth

24 m. OAS Among Both Groups
0%
50%
100%
Duration (Months)
%
Surv
ival
G AG B
The Role of Neoadjuvant Cth

24 months Progression Free Survival Among Both Groups
0%
50%
100%
Duration (Months)
%
Surv
ival
G AG B
The Role of Neoadjuvant Cth

Drug Related Toxicity Profile Among 30 Patients with High Grade Glioma Treated by
TEMOZOLOMIDE at Relapse (NEMROCK 2000-2002)
73%
7% 3% 13% 3%0%
50%
100%
Nau
sea
-
Vom
itin
g G
I
- II
Neu
tropen
ia
Thro
mbocy
top
enia
Dep
ress
ion
Cuta
neo
us
Ras
h
Toxicity
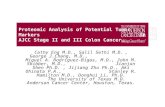
%Temozolomide at Relapse:

Post-Treatment Changes in KPS Among 30 Patients with Hiogh Grade Gliomas Treated by
TEMOZOLOMIDE at Relapse (NEMROCK 2000-2002)
10%
30%
60%
0%
50%
100%
Improved Deteriorated Stationary
KPS
%Temozolomide at Relapse:

Post-Treatment Chganges in Manifestations of ++ ICT and Steroid Dependance Among 30 Patients with High Grade
Glioma Treated by TEMOZOLOMIDE at Relapse (NEMROCK 2000-2002)
7%
50%43%
0%
50%
100%
Improved Stationary DeterioratedICT Status
%
Temozolomide at Relapse:

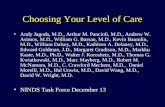
Radiological Response Among 30 Patients with High Grade Glioma Treated by TEMOZOLOMIDE at Relapse (NEMROCK
2000-2002)
33%
22%
45%
0%
50%
100%
Regression Progression Stationary
Radiological Response
%Temozolomide at Relapse:

TEMOZOLOMIDE
X
6 Courses

Survival & Response Parameters:Median Time to Progression = 32.6 Weeks.
Survival Range: 10-36 Months
Median Survival: 17.3 months
Actuarial 12-month OAS = 63.7%
Temozolomide at Relapse:

Th
e U
se o
f TEM
OZ
OLO
MID
EADEQUATE SAFETY PROFILE
NO G III-IV MORBID EVENTS
+ VE SUBJECTIVE EFFECT IN THE MAJORITY OF PATIENTS
+ VE OBJECTIVE RESPONSE

Future Directions
Adjuvant Basis
Metaststic Disease
Concurrent Use with Rth
Temozolomide at Relapse:

Rational For High Rational For High Precision External Beam Precision External Beam RT:RT:
Dose Reduction
To Normal Tissue
Dose Escalation
To CTV

Biological Considerations:Biological Considerations:
Significant Improvement in Tumor Coverage
+ Significant Reduction to Normal Tissue Dose
Dose Escalation to
CTV
Maximum Locoregional
Tumor Control
? Improved Survival

Palliat ive Combinat ion
Chemotherapy
CCN U/ VCR
S tereotact ic Radiosurgery
"S ingle S ession"
15- 17 Gy
40 Pat ients with
H igh Grade Glioma
at Relapse
Radiosurgery at Relapse:

• Headring and Mask Headring and Mask SystemSystem
• Localizer boxLocalizer box
• CouchmountCouchmount
• QA HardwareQA Hardware
• Target Positioner boxTarget Positioner box
• Conical Collimator SetConical Collimator Set
• Conformal blocksConformal blocks
• Headring and Mask Headring and Mask SystemSystem
• Localizer boxLocalizer box
• CouchmountCouchmount
• QA HardwareQA Hardware
• Target Positioner boxTarget Positioner box
• Conical Collimator SetConical Collimator Set
• Conformal blocksConformal blocks
NEMROCK NEMROCK BrainSCAN BrainSCAN Hardware consists Hardware consists of:of:
NEMROCK NEMROCK BrainSCAN BrainSCAN Hardware consists Hardware consists of:of:

Head ring Head ring
For flexible patient fixation and referencing
For single fraction & consists of:
For flexible patient fixation and referencing
For single fraction & consists of:
• Carbon fiber post - variable angle and position - maximum vertical length for
Deep seated lesions.
• Carbon fiber post - variable angle and position - maximum vertical length for
Deep seated lesions.
• Robust and lightweight frame ( Positioned at least 2 cm below lesion)• Robust and lightweight frame ( Positioned at least 2 cm below lesion)
• Two torque wrenches for pressure adjustment of pins• Two torque wrenches for pressure adjustment of pins
• Artifact-free fixation pins for CAT scan with ceramic tips (S.C local anesthesia is applied at fixation site)
• Artifact-free fixation pins for CAT scan with ceramic tips (S.C local anesthesia is applied at fixation site)

• CT Localization• CT Localization
Treatment Planning StepsTreatment Planning Steps
• Automatic Image Fusion (if required)• Automatic Image Fusion (if required)• Outlining of lesion and critical organs• Outlining of lesion and critical organs• Treatment planning• Treatment planning
• Dose Verification - Isodose Lines and Dose-Wash - DVH - 3D Dose representations
• Dose Verification - Isodose Lines and Dose-Wash - DVH - 3D Dose representations

• First radiological assessment among 40 First radiological assessment among 40 patients with residual or recurrent brain patients with residual or recurrent brain tumorstumors
• (Most of the patient in both groups (Most of the patient in both groups experienced PR followed by SD and CR) experienced PR followed by SD and CR)
• (NEMROCK, April 1999-April 2001)(NEMROCK, April 1999-April 2001) • (P-value: 0.603)(P-value: 0.603)
01020304050607080
Group A Group B%

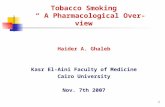
• First clinical and neurological assessment among 40 patients First clinical and neurological assessment among 40 patients with residual or recurrent brain tumorswith residual or recurrent brain tumors
• (Most of the patient in both groups experienced improvement (Most of the patient in both groups experienced improvement followed by persistence) followed by persistence)
• (NEMROCK, April 1999-April 2001)(NEMROCK, April 1999-April 2001)• (P-value: 0.41)(P-value: 0.41)
75
20
5
60
30
10
0
20
40
60
80
100
Group A Group B

PFS dating end of Chemotherapy & date of SRS showed insignificant survival benefit in the Chemotherapy arm (P- value: 0.1)

Overall survival dating initial diagnosis showed insignificant survival benefit in favor of the SRS arm. (P- value: 0.19)

0
5
10
15
20
25
%
Headache Convulsive Fits Nausea & Vomiting Worsening of
Pretreatment
Manifestations
Manifestations
Immediate Post-SRS & SRT Side Effects

• Establishment of SRS & SRT.• > 300 Cases “Cranial & Extra-
Cranial” Targets are Treated.• Ongoing Research.• Committee Decision• Upgrading.
Current Situation:

Why to Irradiate More if we can Irradiate Less?