High-Frequency Oscillatory Ventilation in Adult Patients
37
Sarah Adams RT 214 December 9, 2010
-
Upload
sarahlindsey143 -
Category
Documents
-
view
410 -
download
2
Transcript of High-Frequency Oscillatory Ventilation in Adult Patients
Sarah Adams
RT 214
December 9, 2010
Objectives Six W’s and One H
What is HFOV?
Why should HFOV be used?
Who would this benefit?
When should HFOV be considered?
Where do you start?
How is HFOV implemented?
Weaning
What is HFOV? Alternative mode of ventilation
Based on protective “open lung” principles
Keep it simple: CPAP with a wiggle
Continuous airway pressure (mPaw and bias flow) keeps the lungs open
Oscillatory movement (amplitude and frequency) produces Vt
Vt is often less than deadspace
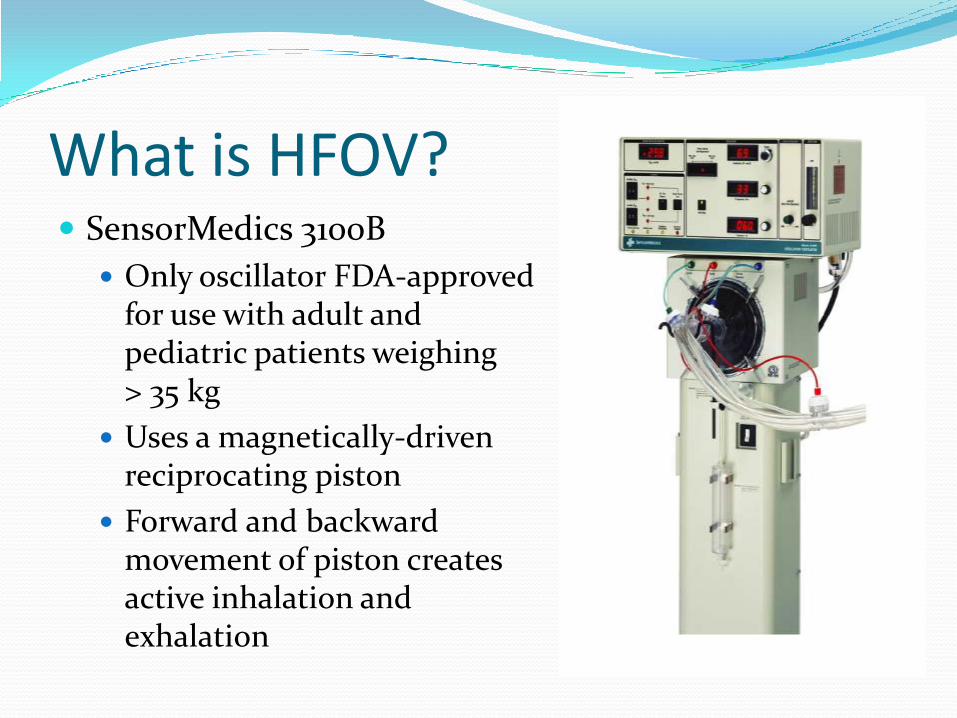
What is HFOV? SensorMedics 3100B
Only oscillator FDA-approved for use with adult and pediatric patients weighing > 35 kg
Uses a magnetically-driven reciprocating piston
Forward and backward movement of piston creates active inhalation and exhalation
Why should HFOV be used? Rescue therapy
ARDS patients who are failing CMV
Prophylactically
At-risk patients
Decreases the risk of developing VILI/VALI
Derdak et al (2002) found that there was a reduction in inflammatory mediator levels with HFOV as compared to CMV when applying similar mPaw values
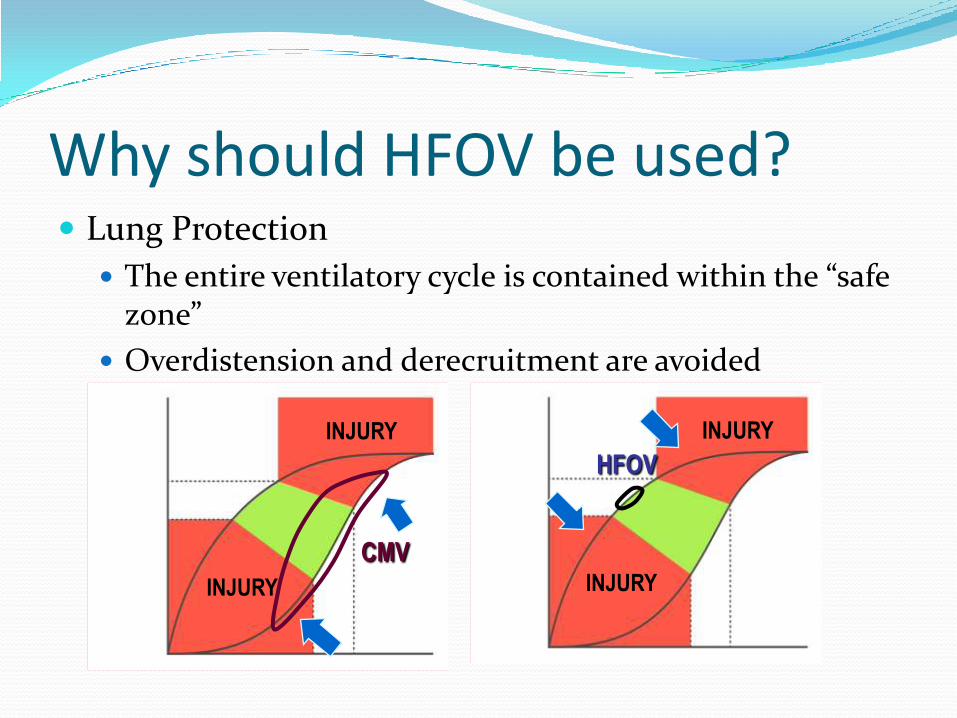
Why should HFOV be used? Lung Protection
The entire ventilatory cycle is contained within the “safe zone”
Overdistension and derecruitment are avoided
INJURY
INJURY
CMV
INJURY
INJURY
HFOV
Who would this benefit? ARDS patients
Patients at-risk for developing VILI/VALI
Special subpopulations:
Major Burn
Trauma
Traumatic Brain Injury
Who would this benefit? Major burn patients
54% of patients on CMV develop ARDS
Treatment of ARDS in burn patients is two-fold and HFOV can supplement both aspects
First, support hypoxemic patient with noncompliant lungs
Second, surgical excision and wound closure
Cartotto et al (2005) states that the need for burn wound surgery influences their decision to start HFOV before surgery due to patients’ rapid improvement in oxygenation
Who would this benefit? Major burn patients with smoke inhalation injury
Improvement in oxygenation was slower and less substantial
72 hrs for improvement, compared to 12 hrs for burn-only patients
Cartotto does not consider smoke inhalation injury a contraindication
Who would benefit? Trauma patients
HFOV has been found to significantly improve oxygenation in patients with blunt trauma
Severity of traumatic injury and organ system failure are greater predictors of survival than respiratory parameters in these patients
The Adult HFOV Outcome Assessment has been found to be non-reliable in these patients, the mortality prediction is lower than actuality
Who would this benefit? Traumatic Brain Injury Patient mortality was found to be much less than the
predicted value calculated from the Adult HFOV Outcome Assessment
Lung protective strategies and brain protective strategies appear contradictory Permissive hypercapnia v. normocapnia goals
However, improvement has been noted in both oxygenation and ICP
Continuous monitoring of ICP, CPP, and PaCO2 is needed
When should HFOV be considered? Criteria recommended by SensorMedics: FiO2 ≥ 60
PEEP ≥ 10
PaO2/FiO2 ratio < 200
Plateau pressure > 30 cmH20
Oxygenation Index (OI) > 24
Bilateral infiltrates on a chest x-ray consistent with ARDS
Contraindications: None, although HFOV may be less effective in
COPD/asthma patients due to air-trapping and hyperinflation
When should HFOV be considered? Oxygenation Index (OI)
From respiratory standpoint – primary indicator of mortality
Calculated as: OI = FiO2 x mPaw
Experts agree: Early intervention produces better outcomes
PaO2
When should HFOV be considered? Ideally, the patient should be hemodynamically stable
MAP ≥ 75 mmHg
If MAP <75 mmHg, fluid boluses and vasopressors
pH > 7.20
If pH ≤ 7.20, aggressive measure should be taken before transition
Manipulation of PaCO2 is significantly slower than on CMV
When should HFOV be considered? After STAT procedures which cannot be performed in
the unit(CT scans, MRIs)
Oscillator is not able to be used during transport
Electrical needs exceed battery capability
Requires two separate pressurized gas sources
After the airway is deemed to be patent
Suction
If there are concerns about airway patency, bronchoscopy recommended
When should HFOV be considered? After patient sedation/paralysis
Spontaneous respirations by the patient can interfere with the oscillator’s ability to effectively ventilate
Large changes in pressure will cause the ventilator to alarm and the oscillatory function to pause
Patient will receive only bias flow of gas when the oscillatory function is paused
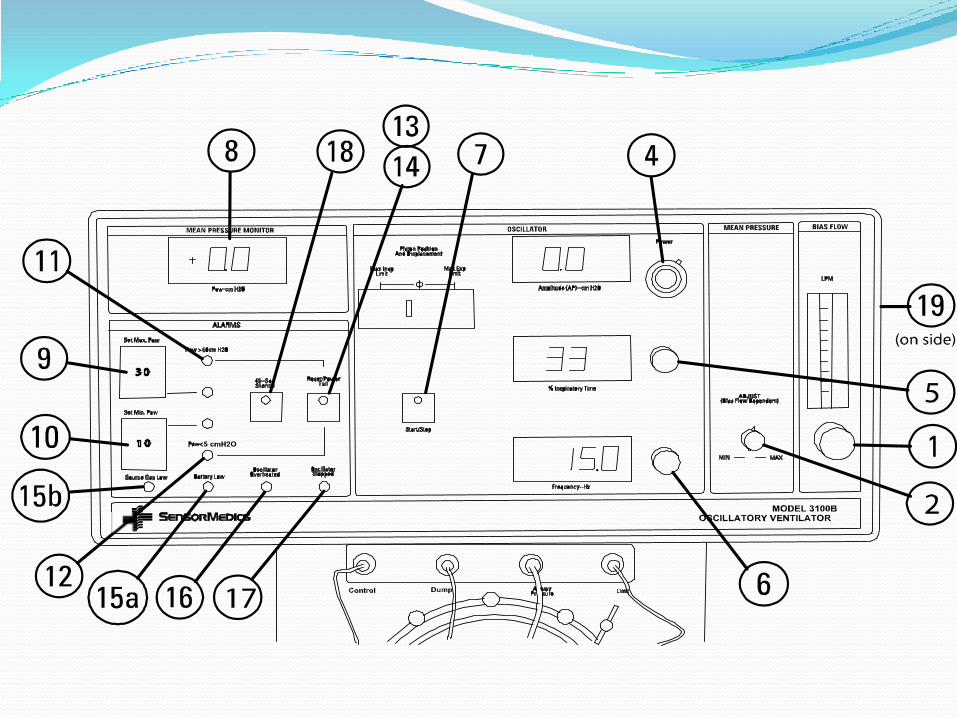
Where do you start? Become familiar the machine
Control panel
Piston
Disposable diaphragm
Non-compliant patient circuit
Water trap
Heated humidifier (not seen)
Blender (not seen)
Where do you start? Become familiar with the control panel/parameters
mPaw
Power
Frequency
Inspiratory time percent (Ti%)
Bias flow
Where do you start? mPaw
Adjustment knob manipulates a balloon valve in the expiratory limb of the patient circuit
Balloon valve is able to restrict the flow of expiratory gas (PEEP)
Determines lung volume
Primary control for oxygenation
An incorrectly set bias flow can either hinder or enhance mPaw
Where do you start? Power
Control knob adjusts amplitude, which is shown on a numerical display
Amplitude is the change in pressure created by the forward and backward movement of the piston
This pressure gradient determines Vt
Primary control for ventilation
Where do you start? Frequency
Adjusts the amount of time the piston is allotted for forward and backward movement
Value is measured in Hertz (Hz)
1 Hz = 60 cycles(breaths)/minute
Secondary control for ventilation
Relationship between frequency and Vt is inverse
As frequency increases, volume displacement decreases, which results in a decreased Vt
Where do you start? Inspiratory time percent (Ti%)
Adjusts I:E ratio
Allots the percent of time the piston spends in forward motion during one ventilatory cycle
Default setting is 33% (I:E ratio of 1:2)
Tertiary control for ventilation
Once an appropriate setting is found (usually left to the default), it is rarely adjusted
Where do you start? Bias flow
Adjusted with a knob, monitored with a Thorpe tube
When HFOV is being initiated, this is the first parameter to be set
If the flow is insufficient, then desired mPaw cannot be reached
If the flow is too high, the negative force of the active exhalation may be negated
Where do you start? Oscillatory function
The button is either on or off
FiO2
Controlled independent of the ventilator with the use of a blender
Pre-use check
Patient circuit calibration
Must be completed with every circuit change
Ventilator performance check
Where do you start? Set up heated humidifier
Attach a closed-system suction catheter
Suctioning required at least every 12 hrs to prevent occlusion of the ETT
Patient/family education
Complications: pneumothorax, hemodynamic compromise, mucus plugging, anesthesia-related, possible exposure to infectious droplets
Noise
Chest wiggle
How is HFOV implemented? Recruitment maneuvers should be performed upon
initiation of HFOV
Also, after patient circuit disconnection, suctioning, or when SpO2 decreases >5%
Amount of pressure and timing is facility specific
Oscillatory function should be paused during maneuver
If a permissible cuff leak is being used to control PaCO2, the cuff should be reinflated for the duration of the maneuver
Contraindications: pneumothorax, unstable hemodynamics
How is HFOV implemented? Initial settings:
Bias flow is to be set between 25-40 LPM
mPaw is to be set 5 cmH2O higher than CMV mPaw
If hemodynamically unstable, mPaw may be set at 2-3 cmH2O higher than CMV mPaw
Set the power to 4.0 and increase until adequate chest wiggle is achieved
Adequate chest wiggle can be determined by placing a tongue depressor on the patient’s mid-thigh and increase the power until the patient visibly shakes from shoulders to mid-thigh
How is HFOV implemented? Initial settings:
Frequency should be set in the range of 5-6 Hz
Ti% should be left to the default
FiO2 set to 100%
How is HFOV implemented? Confirmation of appropriate settings can be achieved
by chest x-ray and ABG, both to be done within 1 hr of transition
Visualization that the 9th posterior rib is above the diaphragm shows adequate lung expansion and appropriate mPaw setting
The oscillatory function should not be paused during the chest x-ray
Chest x-rays should be reordered whenever there is a suspected change in lung volume or disease process
How is HFOV implemented? Confirmation of appropriate settings can be achieved
by chest x-ray and ABG, both to be done within 1 hr of transition
If ABG shows elevated PaO2:
FiO2 should be weaned in 5% increments, until <60%
If lung volume remains the same, it is safe to wean to 40%
If lungs are near hyperinflation, mPaw should be decreased by 1-2 cmH2O while also weaning FiO2 to 40%
After FiO2 has been weaned to 40%, mPaw should be decreased by 1-2 cmH2o every 4-6 hrs
How is HFOV implemented? If ABG shows a PaO2 that is lower than acceptable:
Increase FiO2 to 100%
Increase mPaw by 3-5 cmH20 every 20-30 minutes until oxygenation improves
Lung volume should be rechecked via chest x-ray
If ARB shows a pH that is higher than acceptable:
Decrease the power, while maintaining adequate chest wiggle
If not resolved, then frequency should be increased
If not resolved, then decrease Ti%, to 33%
How is HFOV implemented? If ARB shows a pH that is lower than acceptable:
Increase the power, while maintaining adequate chest wiggle
If not resolved, then frequency should be decreased
Minimum of 3Hz
If not resolved, generate cuff leak
Slowly deflate cuff until mPaw decreases by 5 cmH2O
Then increase bias flow until previous mPaw value returns
If not resolved, then increase Ti%, to 50%
Permissive hypercapnia: as long as the patient’s pH remains >7.20, an elevated PaCO2 is not corrected
How is HFOV implemented? General patient assessment every 2 hrs
Chest wiggle factor
Watch for changes in vibration and symmetry
Auscultation
Normal BS will not be heard, but changes within the lungs can alter the sound of the pistons as heard through the lungs
Perfusion status via capillary refill
VS
Weaning Can be considered after the underlying disease process
has resolved, and the patient tolerates the following:
mPaw 22-24 cmH20
SpO2 >88%, with FiO2 ≤ 40%
When back on CMV, a mode that is also lung protective (PVC, PRVC) is beneficial
mPaw on CMV should be the same as on HFOV
Vt should remain low-normal (6-10 ml/kg IBW)
Rate, PEEP, FiO2 determined by ABG values
Summary HFOV appears to be a safe alternative therapy for
patients who are failing CMV
Main benefit is improved oxygenation
This has been found not to ensure patient survival
Early intervention improves outcome
Questions?