
High-flexion implants in primary total knee arthroplasty: A meta-analysis
4
High-flexion implants in primary total knee arthroplasty: A meta-analysis Rajiv Gandhi ⁎, Peggy Tso, J Roderick Davey, Nizar N. Mahomed Division of Orthopedic Surgery, University of Toronto, Canada abstract article info Article history: Received 5 May 2008 Received in revised form 12 July 2008 Accepted 4 August 2008 Keywords: Knee arthroplasty High flexion Outcomes Meta-analysis Background: We asked whether a high-flexion design implant improves patient functional outcomes or range of motion (ROM) after primary knee arthroplasty. Methods: We searched the major medical databases for randomized trials and comparison observational studies comparing high-flexion and conventional knee implants. After testing for publication bias and heterogeneity, the data were aggregated by random effect modeling. We estimated the weighted mean differences of functional outcomes scores and ROM with 95% confidence intervals. Results: Six studies met our inclusion criteria for review. We found no evidence of publication bias. The pooled mean difference for KSS scores was 0.144 (95% CI: - 0.018 to 0.306), p =0.081. The pooled mean difference for the mean changes in ROM was 0.404 (95% CI: 0.139 to 0.669), p = 0.003. Conclusion: High-flexion implant design improves overall ROM as compared to traditional implants but offers no clinical advantage over traditional implant designs in primary knee arthroplasty. © 2008 Elsevier B.V. All rights reserved. 1. Introduction The goal of total knee arthroplasty (TKA) is to produce a stable painless knee with an adequate range of motion (ROM) for activities of daily living. Studies have shown that 83° of flexion is required for stair climbing; 93° for rising from a seated position; and 106° for shoelace tying; and 120° for stair climbing [1]. Achieving a ROM beyond this may have limited clinical value except in non-Western cultures where a greater degree of flexion is needed for activities like kneeling to pray [2–4]. High-flexion implants have been designed with the goal of consistently providing greater knee flexion than conventional implants. Design features include improved posterior condylar offset with increased posterior conformity, improved articular contact area at high-flexion angles, increased patellar tendon recess in the tibial component, and increased posterior femoral translation [5–7]. There exist few studies evaluating the effectiveness of high- flexion implants in TKA. The primary goal of our study was to determine whether the use of high-flexion implants improves the clinical results of patients over that of conventional knee implants. Our secondary outcome was the difference in ROM obtained between the two implants. A systematic review of the literature and pooling of the best available evidence were performed to evaluate these questions. 2. Materials and methods 2.1. Eligibility criteria Articles included in this paper were those relevant to: (1) those patients undergoing primary total knee replacement for osteoarthritis with a standard posterior-stabilized knee implant versus a high- flexion design knee implant, (2) had Knee Society Scores (KSS) and pre- and post-operative ROM as its outcome measures, and (3) the study was a published or unpublished randomized controlled trial or comparison observational study. 2.2. Study identification A computerized search was done in duplicate of the electronic databases PubMed MEDLINE and OVID MEDLINE (1966 to Oct 2007) and EMBASE (1980 to 2007) with the following search terms (high flex OR flexion) AND (Total knee arthroplasty OR Arthroplasty, Replace- ment, Knee OR Knee prosthesis). The Cochrane Database of Systematic Reviews, the Cochrane Central Register of Controlled Trials, and Clinicaltrials.gov were also searched. Abstracts were retrieved for the studies with titles that were deemed appropriate for review. We independently evaluated these abstracts and chose those studies that were potentially relevant. References for each study meeting inclusion criteria were then screened for any further relevant studies. We also searched the archives of orthopedic meetings for potential abstracts. The Knee 16 (2009) 14–17 ⁎ Corresponding author. Toronto Western Hospital, East Wing 1-439, 399 Bathurst St, Toronto, ON, Canada M5T 2S8. Tel.: +1416 603 5642; fax: +1416 603 3437. E-mail address: [email protected] (R. Gandhi). 0968-0160/$ – see front matter © 2008 Elsevier B.V. All rights reserved. doi:10.1016/j.knee.2008.08.001 Contents lists available at ScienceDirect The Knee
-
Upload
rajiv-gandhi -
Category
Documents
-
view
212 -
download
0
Transcript of High-flexion implants in primary total knee arthroplasty: A meta-analysis

The Knee 16 (2009) 14–17
Contents lists available at ScienceDirect
The Knee
High-flexion implants in primary total knee arthroplasty: A meta-analysis
Rajiv Gandhi ⁎, Peggy Tso, J Roderick Davey, Nizar N. MahomedDivision of Orthopedic Surgery, University of Toronto, Canada
⁎ Corresponding author. TorontoWestern Hospital, EaToronto, ON, Canada M5T 2S8. Tel.: +1 416 603 5642; fa
E-mail address: [email protected] (R. Gandhi).
0968-0160/$ – see front matter © 2008 Elsevier B.V. Aldoi:10.1016/j.knee.2008.08.001
a b s t r a c t
a r t i c l e i n f oArticle history:
Background:We asked whet Received 5 May 2008Received in revised form 12 July 2008Accepted 4 August 2008Keywords:Knee arthroplastyHigh flexionOutcomesMeta-analysis
her a high-flexion design implant improves patient functional outcomes or rangeof motion (ROM) after primary knee arthroplasty.Methods: We searched the major medical databases for randomized trials and comparison observationalstudies comparing high-flexion and conventional knee implants. After testing for publication bias andheterogeneity, the data were aggregated by random effect modeling. We estimated the weighted meandifferences of functional outcomes scores and ROM with 95% confidence intervals.Results: Six studies met our inclusion criteria for review. We found no evidence of publication bias. Thepooled mean difference for KSS scores was 0.144 (95% CI: −0.018 to 0.306), p=0.081. The pooled meandifference for the mean changes in ROM was 0.404 (95% CI: 0.139 to 0.669), p=0.003.Conclusion: High-flexion implant design improves overall ROM as compared to traditional implants but offersno clinical advantage over traditional implant designs in primary knee arthroplasty.
© 2008 Elsevier B.V. All rights reserved.
1. Introduction
The goal of total knee arthroplasty (TKA) is to produce a stablepainless kneewith an adequate range of motion (ROM) for activities ofdaily living. Studies have shown that 83° of flexion is required for stairclimbing; 93° for rising from a seated position; and 106° for shoelacetying; and 120° for stair climbing [1]. Achieving a ROM beyond thismay have limited clinical value except in non-Western cultures wherea greater degree of flexion is needed for activities like kneeling to pray[2–4].
High-flexion implants have been designed with the goal ofconsistently providing greater knee flexion than conventionalimplants. Design features include improved posterior condylaroffset with increased posterior conformity, improved articularcontact area at high-flexion angles, increased patellar tendon recessin the tibial component, and increased posterior femoral translation[5–7].
There exist few studies evaluating the effectiveness of high-flexion implants in TKA. The primary goal of our study was todetermine whether the use of high-flexion implants improves theclinical results of patients over that of conventional knee implants.Our secondary outcome was the difference in ROM obtainedbetween the two implants. A systematic review of the literature
st Wing 1-439, 399 Bathurst St,x: +1 416 603 3437.
l rights reserved.
and pooling of the best available evidence were performed toevaluate these questions.
2. Materials and methods
2.1. Eligibility criteria
Articles included in this paper were those relevant to: (1) thosepatients undergoing primary total knee replacement for osteoarthritiswith a standard posterior-stabilized knee implant versus a high-flexion design knee implant, (2) had Knee Society Scores (KSS) andpre- and post-operative ROM as its outcome measures, and (3) thestudy was a published or unpublished randomized controlled trial orcomparison observational study.
2.2. Study identification
A computerized search was done in duplicate of the electronicdatabases PubMed MEDLINE and OVID MEDLINE (1966 to Oct 2007)and EMBASE (1980 to 2007) with the following search terms (high flexOR flexion) AND (Total knee arthroplasty OR Arthroplasty, Replace-ment, Knee OR Knee prosthesis). The Cochrane Database of SystematicReviews, the Cochrane Central Register of Controlled Trials, andClinicaltrials.gov were also searched. Abstracts were retrieved for thestudies with titles that were deemed appropriate for review. Weindependently evaluated these abstracts and chose those studies thatwere potentially relevant. References for each studymeeting inclusioncriteria were then screened for any further relevant studies. We alsosearched the archives of orthopedic meetings for potential abstracts.
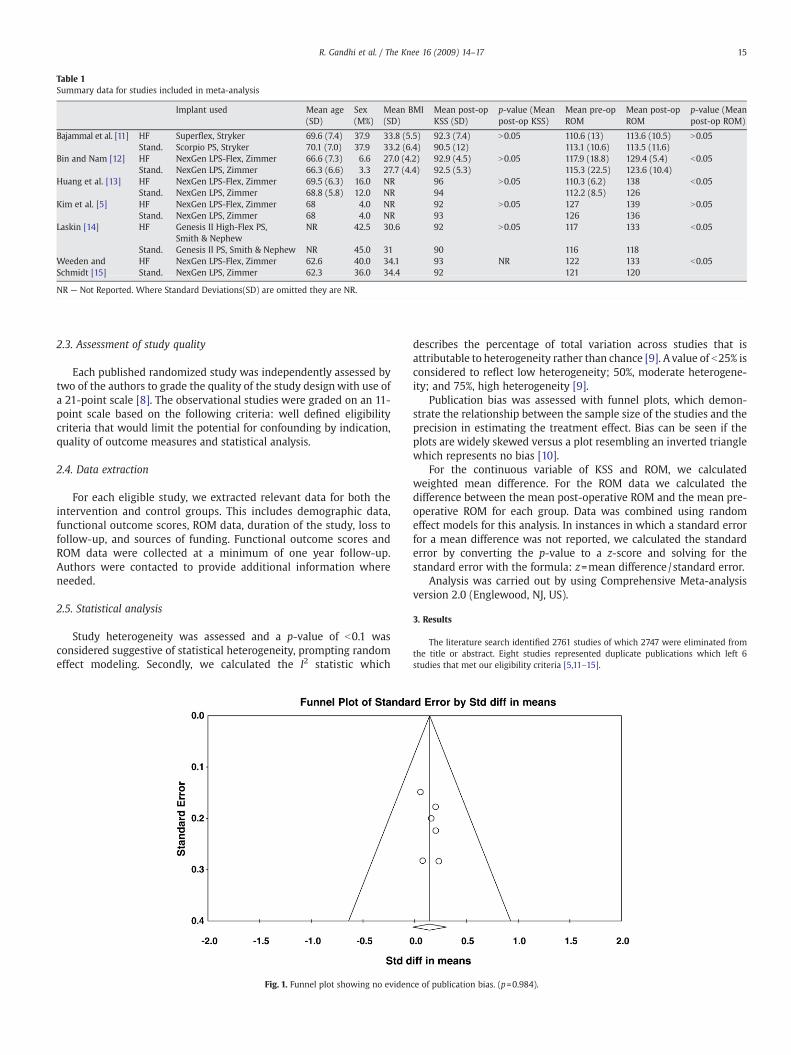
Table 1Summary data for studies included in meta-analysis
Implant used Mean age(SD)
Sex(M%)
Mean BMI(SD)
Mean post-opKSS (SD)
p-value (Meanpost-op KSS)
Mean pre-opROM
Mean post-opROM
p-value (Meanpost-op ROM)
Bajammal et al. [11] HF Superflex, Stryker 69.6 (7.4) 37.9 33.8 (5.5) 92.3 (7.4) N0.05 110.6 (13) 113.6 (10.5) N0.05Stand. Scorpio PS, Stryker 70.1 (7.0) 37.9 33.2 (6.4) 90.5 (12) 113.1 (10.6) 113.5 (11.6)
Bin and Nam [12] HF NexGen LPS-Flex, Zimmer 66.6 (7.3) 6.6 27.0 (4.2) 92.9 (4.5) N0.05 117.9 (18.8) 129.4 (5.4) b0.05Stand. NexGen LPS, Zimmer 66.3 (6.6) 3.3 27.7 (4.4) 92.5 (5.3) 115.3 (22.5) 123.6 (10.4)
Huang et al. [13] HF NexGen LPS-Flex, Zimmer 69.5 (6.3) 16.0 NR 96 N0.05 110.3 (6.2) 138 b0.05Stand. NexGen LPS, Zimmer 68.8 (5.8) 12.0 NR 94 112.2 (8.5) 126
Kim et al. [5] HF NexGen LPS-Flex, Zimmer 68 4.0 NR 92 N0.05 127 139 N0.05Stand. NexGen LPS, Zimmer 68 4.0 NR 93 126 136
Laskin [14] HF Genesis II High-Flex PS,Smith & Nephew
NR 42.5 30.6 92 N0.05 117 133 b0.05
Stand. Genesis II PS, Smith & Nephew NR 45.0 31 90 116 118Weeden andSchmidt [15]
HF NexGen LPS-Flex, Zimmer 62.6 40.0 34.1 93 NR 122 133 b0.05Stand. NexGen LPS, Zimmer 62.3 36.0 34.4 92 121 120
NR — Not Reported. Where Standard Deviations(SD) are omitted they are NR.
15R. Gandhi et al. / The Knee 16 (2009) 14–17
2.3. Assessment of study quality
Each published randomized study was independently assessed bytwo of the authors to grade the quality of the study designwith use ofa 21-point scale [8]. The observational studies were graded on an 11-point scale based on the following criteria: well defined eligibilitycriteria that would limit the potential for confounding by indication,quality of outcome measures and statistical analysis.
2.4. Data extraction
For each eligible study, we extracted relevant data for both theintervention and control groups. This includes demographic data,functional outcome scores, ROM data, duration of the study, loss tofollow-up, and sources of funding. Functional outcome scores andROM data were collected at a minimum of one year follow-up.Authors were contacted to provide additional information whereneeded.
2.5. Statistical analysis
Study heterogeneity was assessed and a p-value of b0.1 wasconsidered suggestive of statistical heterogeneity, prompting randomeffect modeling. Secondly, we calculated the I2 statistic which
Fig. 1. Funnel plot showing no eviden
describes the percentage of total variation across studies that isattributable to heterogeneity rather than chance [9]. A value of b25% isconsidered to reflect low heterogeneity; 50%, moderate heterogene-ity; and 75%, high heterogeneity [9].
Publication bias was assessed with funnel plots, which demon-strate the relationship between the sample size of the studies and theprecision in estimating the treatment effect. Bias can be seen if theplots are widely skewed versus a plot resembling an inverted trianglewhich represents no bias [10].
For the continuous variable of KSS and ROM, we calculatedweighted mean difference. For the ROM data we calculated thedifference between the mean post-operative ROM and the mean pre-operative ROM for each group. Data was combined using randomeffect models for this analysis. In instances in which a standard errorfor a mean difference was not reported, we calculated the standarderror by converting the p-value to a z-score and solving for thestandard error with the formula: z=mean difference/standard error.
Analysis was carried out by using Comprehensive Meta-analysisversion 2.0 (Englewood, NJ, US).
3. Results
The literature search identified 2761 studies of which 2747 were eliminated fromthe title or abstract. Eight studies represented duplicate publications which left 6studies that met our eligibility criteria [5,11–15].
ce of publication bias. (p=0.984).
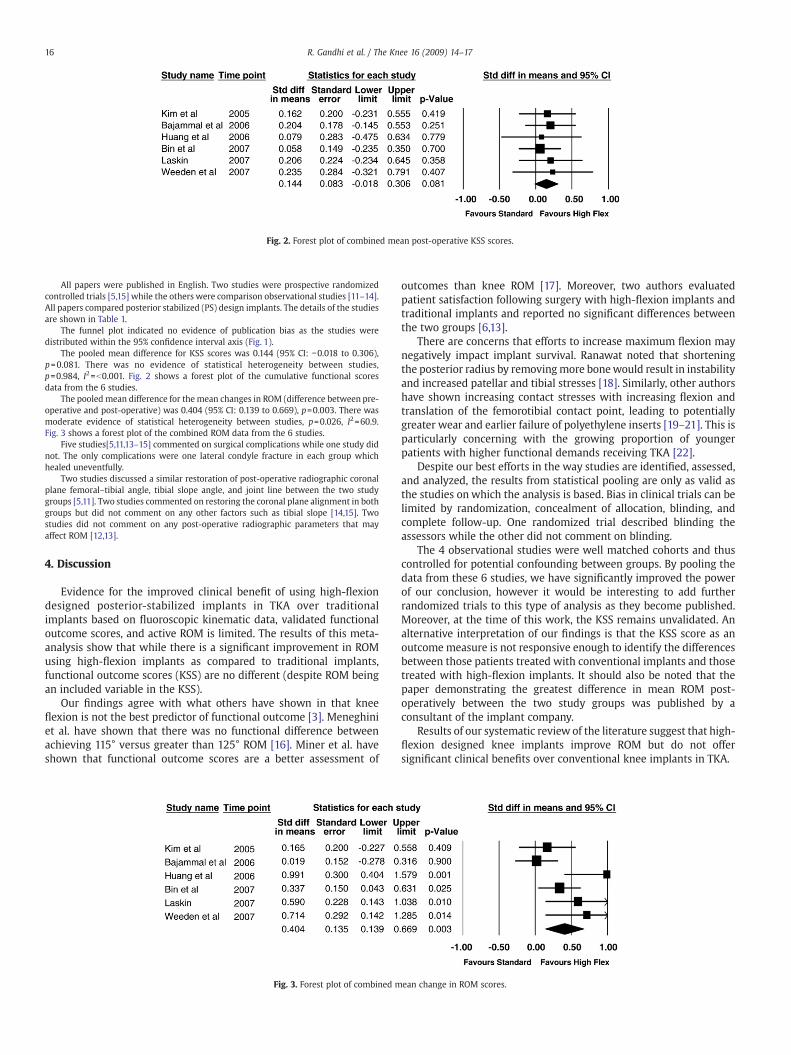
Fig. 2. Forest plot of combined mean post-operative KSS scores.
16 R. Gandhi et al. / The Knee 16 (2009) 14–17
All papers were published in English. Two studies were prospective randomizedcontrolled trials [5,15] while the others were comparison observational studies [11–14].All papers compared posterior stabilized (PS) design implants. The details of the studiesare shown in Table 1.
The funnel plot indicated no evidence of publication bias as the studies weredistributed within the 95% confidence interval axis (Fig. 1).
The pooled mean difference for KSS scores was 0.144 (95% CI: −0.018 to 0.306),p=0.081. There was no evidence of statistical heterogeneity between studies,p=0.984, I2=b0.001. Fig. 2 shows a forest plot of the cumulative functional scoresdata from the 6 studies.
The pooled mean difference for the mean changes in ROM (difference between pre-operative and post-operative) was 0.404 (95% CI: 0.139 to 0.669), p=0.003. There wasmoderate evidence of statistical heterogeneity between studies, p=0.026, I2=60.9.Fig. 3 shows a forest plot of the combined ROM data from the 6 studies.
Five studies[5,11,13–15] commented on surgical complications while one study didnot. The only complications were one lateral condyle fracture in each group whichhealed uneventfully.
Two studies discussed a similar restoration of post-operative radiographic coronalplane femoral–tibial angle, tibial slope angle, and joint line between the two studygroups [5,11]. Two studies commented on restoring the coronal plane alignment in bothgroups but did not comment on any other factors such as tibial slope [14,15]. Twostudies did not comment on any post-operative radiographic parameters that mayaffect ROM [12,13].
4. Discussion
Evidence for the improved clinical benefit of using high-flexiondesigned posterior-stabilized implants in TKA over traditionalimplants based on fluoroscopic kinematic data, validated functionaloutcome scores, and active ROM is limited. The results of this meta-analysis show that while there is a significant improvement in ROMusing high-flexion implants as compared to traditional implants,functional outcome scores (KSS) are no different (despite ROM beingan included variable in the KSS).
Our findings agree with what others have shown in that kneeflexion is not the best predictor of functional outcome [3]. Meneghiniet al. have shown that there was no functional difference betweenachieving 115° versus greater than 125° ROM [16]. Miner et al. haveshown that functional outcome scores are a better assessment of
Fig. 3. Forest plot of combined m
outcomes than knee ROM [17]. Moreover, two authors evaluatedpatient satisfaction following surgery with high-flexion implants andtraditional implants and reported no significant differences betweenthe two groups [6,13].
There are concerns that efforts to increase maximum flexion maynegatively impact implant survival. Ranawat noted that shorteningthe posterior radius by removingmore bonewould result in instabilityand increased patellar and tibial stresses [18]. Similarly, other authorshave shown increasing contact stresses with increasing flexion andtranslation of the femorotibial contact point, leading to potentiallygreater wear and earlier failure of polyethylene inserts [19–21]. This isparticularly concerning with the growing proportion of youngerpatients with higher functional demands receiving TKA [22].
Despite our best efforts in the way studies are identified, assessed,and analyzed, the results from statistical pooling are only as valid asthe studies on which the analysis is based. Bias in clinical trials can belimited by randomization, concealment of allocation, blinding, andcomplete follow-up. One randomized trial described blinding theassessors while the other did not comment on blinding.
The 4 observational studies were well matched cohorts and thuscontrolled for potential confounding between groups. By pooling thedata from these 6 studies, we have significantly improved the powerof our conclusion, however it would be interesting to add furtherrandomized trials to this type of analysis as they become published.Moreover, at the time of this work, the KSS remains unvalidated. Analternative interpretation of our findings is that the KSS score as anoutcome measure is not responsive enough to identify the differencesbetween those patients treated with conventional implants and thosetreated with high-flexion implants. It should also be noted that thepaper demonstrating the greatest difference in mean ROM post-operatively between the two study groups was published by aconsultant of the implant company.
Results of our systematic review of the literature suggest that high-flexion designed knee implants improve ROM but do not offersignificant clinical benefits over conventional knee implants in TKA.
ean change in ROM scores.

17R. Gandhi et al. / The Knee 16 (2009) 14–17
5. Conflict of Interest
None.
References
[1] Laubenthal KN. A quantitative analysis of knee motion during activities of dailyliving. Phys Ther 1972;52:34.
[2] Mulholland SJ, Wyss UP. Activities of daily living in non-Western cultures: range ofmotion requirements for hip and knee joint implants. Int J Rehabil Res2001;24:191–8.
[3] Park KK, Chang CB, Kang YG, Seong SC, Kim TK. Correlation of maximum flexionwith clinical outcome after total knee replacement in Asian patients. J Bone Jt SurgBr 2007;89(5):604–8.
[4] Kurosaka M, Yoshiya S, Mizuno K, Yamamoto T. Maximizing flexion after total kneearthroplasty: the need and the pitfalls. J Arthroplast 2002;17(Suppl 1):59–62.
[5] Kim YH, Sohn KS, Kim JS. Range of motion of standard and high-flexion posteriorstabilized total knee prostheses. A prospective, randomized study. J Bone Jt SurgAm 2005;87(7):1470–5.
[6] Argenson JNA, Komistek RD, Mahfouz M, Walker SA, Aubaniac JM, Dennis DA. Ahigh flexion total knee arthroplasty design replicates healthy knee motion. ClinOrthop 2004;428:174.
[7] Argenson JN, Ariaudi S, Aubaniac JM. The factors governing high flexion after totalknee arthroplasty. J Bone Jt Surg, Br 2004;86(Suppl IV):403.
[8] Detsky AS, Naylor CD, O'Rourke K, McGeer AJ, L'Abbe KA. Incorporating variationsin the quality of individual randomized trials into meta-analysis. J Clin Epidemiol1992;45:255–65.
[9] Higgins JP, Thompson SG, Deeks JJ, Altman DG. Measuring inconsistency in meta-analyses. BMJ 2003;327:557–60.
[10] Egger M, Davey SG, Schneider M, Minder C. Bias in meta-analysis detected by asimple, graphical test. BMJ 1997;315:629–34.
[11] Bajammal S, de Beer J, Petruccelli D, Adili A, Winemaker M. Can a change inimplant articular geometry affect postoperative range of movement in patientsundergoing primary total knee arthroplasty for osteoarthritis? SA Orthop J May2006:34–42.
[12] Bin SI, Nam TS. Early results of high-flex total knee arthroplasty: comparison studyat 1 year after surgery. Knee Surg Sports Traumatol Arthrosc 2007;15(4):350–5.
[13] Huang HT, Su JY, Wang GJ. The early results of high-flex total knee arthroplasty aminimum of 2 years of follow-up. J Arthroplast 2005;20(5):674–9.
[14] Laskin RS. The effect of a high-flex implant on postoperative flexion after primarytotal knee arthroplasty. Orthopedics 2007;30(8 Suppl):86–8.
[15] Weeden SH, Schmidt R. A randomized, prospective study of primary total kneecomponents designed for increased flexion. J Arthroplast 2007;22(3):349–52.
[16] Meneghini RM, Pierson JL, Bagsby D, Ziemba-Davis M, Berend ME, Ritter MA. Isthere a functional benefit to obtaining high flexion after total knee arthroplasty?J Arthroplast 2007;22(Suppl 6):43–6.
[17] Miner AL, Lingard EA, Wright EA, Sledge CB, Katz JN. Knee range of motion aftertotal knee arthroplasty: how important is this as an outcome measure?J Arthroplast 2003;18:286–94.
[18] Ranawat CS. Designmay be counterproductive in optimizing flexion after TKR. ClinOrthop 2003;416:174.
[19] Blunn GW, Walker PS, Joshi A, Hardinge K. The dominance of cyclic sliding inproducing wear in total knee replacements. Clin Orthop 1991;273:253–60.
[20] Sharma A, Komistek RD, Scuderi GR, Cates Jr HE. High-flexion TKA designs: whatare their in vivo contact mechanics? Clin Orthop Relat Res 2007;464:117–26.
[21] Swany MR, Scott RD. Posterior polyethylene wear in posterior cruciate ligament-retaining total knee arthroplasty. A case study. J Arthroplast 1993;8:439–46.
[22] Jain NB, Higgins LD, Ozumba D, Guller U, Cronin M, Pietrobon R, et al. Trends inepidemiology of knee arthroplasty in the United States, 1990–2000. ArthritisRheum 2005;52(12):3928–33.









![Edinburgh Research Explorer · 4 Introduction Ten year survival of unicompartmental knee arthroplasty (UKA) varies from 80 to 96% between implants and institutions [1-3].Unexplained](https://static.fdocuments.in/doc/165x107/5f938b51bb9e8a5c17140af2/edinburgh-research-explorer-4-introduction-ten-year-survival-of-unicompartmental.jpg)








