High altitude and hypertension during pregnancy
11
AMERICAN JOURNAL OF HUMAN BIOLOGY 7:183-193 (1995) High Altitude and Hypertension During Pregnancy STACY ZAMUDIO'*4,5, SUSAN K. PALMER',5 JUDITH G. REGENSTEINER2,5, AND LORNA GRINDLAY MOORE3*4,5 'Department of Anesthesiology; 'Section of Vascular Disease "Cardiouascular Pulmonary Research Laboratory, University of Colorado Health Sciences Center, Denuer, Colorado 80262; 4Department of Anthropology, University of Colorado at Denuer, Denuer, Colorado 8021 7; "Women's Health Research Center. Uniuersity of Colorado Health Sciences Center, Denuer, Colorado 80262 ABSTRACT Hypertensive complications of pregnancy are more common at high than low altitudes. Hypertension in pregnancy is associated with increased maternal and fetal morbidity and mortality; thus natural selectionmay be operat- ing against women who develop the disorder and their infants. It has long been hypothesized that chronic hypoxia due to residence at high altitude predisposes women to develop hypertension during pregnancy. Prior studies indicate that maternal adaptation to pregnancy is altered by residence at high altitude such that some physiological characteristics of women pregnant at high altitude resem- ble those of women who develop hypertension during pregnancy at low altitude. This paper reviews data from studies, conducted over the past decade, which support a relationship between chronic hypoxia and hypertension during preg- nancy. The results suggest that both the requirements for successfuladaptation to high altitude, as well as the effect of lowered Po, during pregnancy, may contrib- ute to the development of hypertension during pregnancy. 8 1995 WiIey-Liss, Inc. Hypertensive complications of pregnancy are more common at high (32,500 m) than low altitude in the United States (Moore et al., 1982) and are among the leading causes of maternal and infant morbidity and mor- tality in industrialized nations (Lehmann et al., 1987; Ales et al., 1990). Hypertension in pregnancy is the third most frequent cause of very low birth weight, following prema- ture birth or rupture of the membranes (Ales et al., 1988). It may be inferred that any condition compromisingwomen's ability to maintain their health during pregnancy and to deliver a healthy, normally grown in- fant may result in natural selection against both mothers and their infants. Thus, it is important to understand why residence at high altitude is associated with a greater incidence of hypertension during pregnancy. It has been hypothesized that mild, chronic hypoxia due to residence at high altitude predisposes women to develop hypertension in pregnancy (Moore et al., 1982). The present review considers results of research, conducted over the past decade or so, which has been directed towards an understanding of the relationship between chronic hypoxia and hypertension during pregnancy. PHYSIOLOGICAL ADJUSTMENTS TO NORMAL PREGNANCY Normal pregnant women have a reduced blood pressure response to angiotensin 11, suggesting that vascular responsiveness to vasoconstrictors is attenuated during preg- nancy (Chesley and Tepper, 1967; Gant et al., 1973; Nisell et al., 1985). Normal preg- nancy is characterized by a fall in mean ar- terial pressure and increase in cardiac out- put, indicative of vasodilation and lowered systemic vascular resistance (Page and Christianson, 1976; Ueland et al., 1969). Only one-third of the fall in systemic vascu- lar resistance is due to the addition of the uteroplacental circuit; hence, the residual- systemic circulation is responsible for the Received December 30, 1993; accepted May 25,1994. Address reprint requests to Stacy Zamudio, Ph.D., Depart- ment of Anesthesiology 8-113, University of Colorado Health Sciences Center, 4200 E. 9th Avenue, Denver, CO 80262. 0 1995 Wiley-Liss, Inc.
-
Upload
stacy-zamudio -
Category
Documents
-
view
213 -
download
0
Transcript of High altitude and hypertension during pregnancy

AMERICAN JOURNAL OF HUMAN BIOLOGY 7:183-193 (1995)
High Altitude and Hypertension During Pregnancy STACY ZAMUDIO'*4,5, SUSAN K. PALMER',5 JUDITH G. REGENSTEINER2,5, AND LORNA GRINDLAY MOORE3*4,5 'Department of Anesthesiology; 'Section of Vascular Disease "Cardiouascular Pulmonary Research Laboratory, University of Colorado Health Sciences Center, Denuer, Colorado 80262; 4Department of Anthropology, University of Colorado at Denuer, Denuer, Colorado 8021 7; "Women's Health Research Center. Uniuersity of Colorado Health Sciences Center, Denuer, Colorado 80262
ABSTRACT Hypertensive complications of pregnancy are more common at high than low altitudes. Hypertension in pregnancy is associated with increased maternal and fetal morbidity and mortality; thus natural selection may be operat- ing against women who develop the disorder and their infants. It has long been hypothesized that chronic hypoxia due to residence at high altitude predisposes women to develop hypertension during pregnancy. Prior studies indicate that maternal adaptation to pregnancy is altered by residence at high altitude such that some physiological characteristics of women pregnant at high altitude resem- ble those of women who develop hypertension during pregnancy at low altitude. This paper reviews data from studies, conducted over the past decade, which support a relationship between chronic hypoxia and hypertension during preg- nancy. The results suggest that both the requirements for successful adaptation to high altitude, as well as the effect of lowered Po, during pregnancy, may contrib- ute to the development of hypertension during pregnancy. 8 1995 WiIey-Liss, Inc.
Hypertensive complications of pregnancy are more common at high (32,500 m) than low altitude in the United States (Moore et al., 1982) and are among the leading causes of maternal and infant morbidity and mor- tality in industrialized nations (Lehmann et al., 1987; Ales et al., 1990). Hypertension in pregnancy is the third most frequent cause of very low birth weight, following prema- ture birth or rupture of the membranes (Ales et al., 1988). It may be inferred that any condition compromising women's ability to maintain their health during pregnancy and to deliver a healthy, normally grown in- fant may result in natural selection against both mothers and their infants. Thus, it is important to understand why residence at high altitude is associated with a greater incidence of hypertension during pregnancy. It has been hypothesized that mild, chronic hypoxia due to residence at high altitude predisposes women to develop hypertension in pregnancy (Moore et al., 1982). The present review considers results of research, conducted over the past decade or so, which has been directed towards an understanding
of the relationship between chronic hypoxia and hypertension during pregnancy.
PHYSIOLOGICAL ADJUSTMENTS TO NORMAL PREGNANCY
Normal pregnant women have a reduced blood pressure response to angiotensin 11, suggesting that vascular responsiveness to vasoconstrictors is attenuated during preg- nancy (Chesley and Tepper, 1967; Gant et al., 1973; Nisell et al., 1985). Normal preg- nancy is characterized by a fall in mean ar- terial pressure and increase in cardiac out- put, indicative of vasodilation and lowered systemic vascular resistance (Page and Christianson, 1976; Ueland et al., 1969). Only one-third of the fall in systemic vascu- lar resistance is due to the addition of the uteroplacental circuit; hence, the residual- systemic circulation is responsible for the
Received December 30, 1993; accepted May 25,1994. Address reprint requests to Stacy Zamudio, Ph.D., Depart-
ment of Anesthesiology 8-113, University of Colorado Health Sciences Center, 4200 E. 9th Avenue, Denver, CO 80262.
0 1995 Wiley-Liss, Inc.

S. ZAMUDIO ET AL. 184
remainder of the fall (Curran-Everett et al., 1991). The pregnancy-associated fall in blood pressure reaches a nadir by week 20 and rises toward nonpregnant values there- after (Page and Christianson, 1976). Car- diac output increases early in pregnancy and peaks early in the third trimester (Ue- land et al., 1969). Total blood volume in- creases by 40-50%, due primarily to in- creased plasma volume and secondarily to increased red cell mass (Longo and Hard- esty, 1984). These cardiovascular and hema- tological adaptations to pregnancy contrib- ute to a 100-fold increase in uterine blood flow, thereby supplying the fetus with the nutrients and oxygen required for growth (Palmer et al., 1992). These changes are likely to be attributable, at least in part, to the hormonal alterations of pregnancy, which include marked increases in proges- terone and estradiol concentrations (Tulchin- sky et al., 1972).
HYPERTENSION DURING PREGNANCY The criteria of the American College of
Obstetrics and Gynecology were used to de- fine transient hypertension, preeclampsia, and chronic hypertension (Hughes, 1972; Roberts, 1989). Transient hypertension was defined as a systolic pressure 2140 mmHg or a diastolic pressure a90 mmHg on two or more occasions at least 6 hours apart while pregnant, during labor (but not during a contraction or in the last stage of labor), or in the first 24 hours postpartum in a woman who had been normotensive when nonpreg- nant and whose blood pressure returns to normal postpartum. Preeclampsia was de- fined as a resting systolic pressure 3140 mmHg or a diastolic pressure 390 mmHg on two or more occasions as defined above plus either 32+ proteinuria or 22+ pitting edema of the upper extremities or face ob- served on two or more occasions. In the ab- sence of a clinical notation of edema in the subject record, 3 5 lb weight gain in one week was accepted as evidence of edema (Hughes, 1972). Symptoms of central ner- vous system (CNS) dysfunction (clonus, vi- sual disturbances, headache), hepatic dys- function (elevated liver function tests, epigastric pain), or coagulation abnormali- ties (elevated prothrombin time, elevated partial thromboplastin time, or plate- lets < 150 x lO’/liter) are considered evi- dence of additional organ system involve- ment (Roberts, 1989). Chronic hypertension
was defined as either a documented medical history of hypertension or a resting blood pressure a140 mmHg systolic or 390 mmHg diastolic in the nonpregnant state or before the 20th week of gestation (Hughes, 1972; Roberts, 1989). Superimposed preec- lampsia was present in a chronically hyper- tensive woman if blood pressure during pregnancy rose by 230 mmHg systolic or a 1 5 mmHg diastolic from her nonpregnant value and there was proteinuria and/or edema as discussed above.
Women who develop preeclampsia lose their refractoriness to angiotensin I1 as early as 18-20 weeks of pregnancy (Gant et al., 1973). Blood volume is lower in preec- lamptic than normotensive women, due ei- ther to a fall in blood volume during late pregnancy, or failure of blood volume to ex- pand during pregnancy (Blekta et al., 1970; Gallery et al., 1979). Systemic vascular re- sistance and vascular resistance response to vasoconstrictors are increased in preec- lamptic women (Groenendijk et al., 1984; Nisell et al., 1985) and blood pressures rise markedly. Data on cardiac output are con- tradictory, possibly due to the efefcts of anti- hypertensive treatment, or failure of inves- tigators to correct for body size, with both higher and lower values seen in preeclamp- tic compared with normal pregnant women (Easterling et al., 1990; Groenendijk et al. 1984). Preeclampsia is often associated with placental insufficiency, whether due to ab- normal trophoblastic invasion, vasospasm, or any other condition limiting uteroplacen- tal blood flow (Browne and Veall, 1953; Brosens et al., 1972; Nylund et al., 1983). Conversely, the presence of an unusually large conceptus (as in twins or macrosomia) is also associated with preeclampsia, and in this case placental insufficiency is likely due to the higher demand placed upon the utero- placental system. Taken together, these characteristics of preeclampsia suggest that insufficient delivery of oxygen and nutrients to the developing fetus prompts the produc- tion of a substance(sj of fetal or placental origin which increase maternal blood pres- sure, damages the vascular endothelium, and produces the symptoms of preeclampsia in various organ systems (Clemetson and Churchman, 1953; Roberts et al., 1989). In- deed the origin of an older term for preec- lampsia, “toxemia,” stems from the concept that a humoral agent is responsible for the disorder. It has been suggested that the rise

HYPOXIA AND PREECLAMPSIA 185 Pregnancy
hypoxia Normal pregnancy P -/
i v a s o r e a c t i v y
4
I
I Blood pressure t I Systemic vascular t resistance
t Blood volume (
1 UleroplacPntal blood flow
\ Maternawelal well-being i
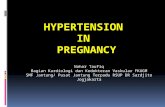
Fig. 1. Hypothesis concerning effects of chronic hy- poxia on pregnancy outcome. The arrows to the left of each variable indicate the expected direction of change in normal pregnancy. The arrows to the right of each variable indicate the hypothesized affect of chronic hy- poxia. We speculate that chronic hypoxia may alter hor- monal profile during pregnancy in such a fashion as to limit the normal pregnancy-related fall in vasoreactiv- ity.
in blood pressure which occurs even among normal women late in pregnancy may be a “physiological response to a pathophysiolog- ical problem” (Broughton-Pipkin, 1989). Since increase in cardiac output, blood vol- ume, and perhaps in some individuals maxi- mal increase in uterine blood flow are at- tained by the mid-third trimester (Zamudio et al., 1995a), only an increase in blood pres- sure and hence perfusion pressure to the uteroplacental circulation can further in- crease oxygen and nutrient delivery t o the growing fetus (Broughton-Pipkin, 1989).
Given these observations, the hypotheti- cal schema for evaluating the influence of chronic hypoxia on the development of preeclampsia at high altitude is given in Figure 1. The left hand side of each variable in the schema shows the adjustments that occur in normal pregnancy, i.e., a hormon- ally mediated fall in vascular reactivity, leading to reduced systemic vascular resis- tance, lowered blood pressure, and in- creased blood volume. These adjustments, in turn, contribute to increased uteroplacen- tal blood flow and the health of both moth- ers and infants. It is hypothesized that chronic hypoxia interferes with these nor- mal adjustments to pregnancy in one or more possible ways: 1) by altering hormonal balance during pregnancy, and hence in- creasing vasoreactivity; 2) by inhibiting the vasodilatory action of normal hormonal con- centrations through an unidentified mecha-
nism; or 3) hypoxia could exert a nonhor- monally mediated vasoconstrictor effect upon the vasculature, which is more pro- nounced during pregnancy due to the greater stress placed upon the maternal cir- culation and hence more readily observed during pregnancy. Regardless of the exact mechanism, support for the overall hypothe- sis that chronic hypoxia predisposes women to develop hypertension during pregnancy would require evidence of an altered hor- monal profile, andlor increased blood pres- sure and decreased blood volume (which to- gether indicate increased systemic vascular resistance), and lowered uteroplacental blood flow during high-altitude compared with low-altitude pregnancies.
STUDIES AND SUBJECTS The majority of the data is derived from
two prospective and two retrospective stud- ies conducted in the state of Colorado, be- tween 1979 and 1991. Some similar data have been gathered in Peru and Tibet (Moore, 1990), but it is beyond the scope of this paper to compare high-altitude popula- tions.
During the 12 years from 1979 to 1991 a total of 79 women living at 3,100 m and 53 women living at 1,600 m were prospectively studied in protocols designed to examine the influence of ventilatory, circulatory, and hormonal changes during pregnancy upon pregnancy outcome (Table 1). All high-alti- tude women were of European descent. Seven of the low-altitude women were Afri- can-American or of Asian descent, and the remainder were of European descent. Pro- spectively studied women at high altitude were slightly younger, and fewer were primiparous than their low-altitude coun- terparts (Table 1). The low and high-alti- tude women were similar in stature, non- pregnant weight, weight gain with pregnancy, the number using cigarettes during pregnancy, and prenatal care. Gesta- tional age was similar a t 1,600 m and 3,100 m, but infant birth weight was lower at high altitude. More women developed transient hypertension or preeclampsia at high than at low altitude, while the numbers of chron- ically hypertensive women who participated in studies a t each altitude were similar (Ta- ble 1). The numbers of chronically hyperten- sive subjects at each location likely underes- timate the true population incidence, as most of the protocols excluded women with

S. ZAMUDIO ET AL.
TABLE 1. Characteristics ofthe Colorado low- and high-altitude subjects studied prospectively (1979-19911
186
1,600 m 3,100 m All subjects All subjects
(n = 53) (n = 79)
Age (years) Height (cm) he-pregnant weight (kg) Weight gain wipregnancy (kg) Primigravidas (%I Lifelong residents >3,000 m Smokers (%) Prenatal care (no. visits) lnfant birth weight (g) Gestational age (weeks) % preterm (<37 weeks) % small for gestational age ( 4 0 t h percentile) Maternal hypertensive complications
Transient hypertension (% of entire sample) Preeclampsia (% of entire sample) Chronic hypertension (70 of entire sample) Chronic hypertension + preeclampsia (Q of chl
28 i 1 164 -t 1 59.6 ? 1.5 14.3 2 0.8
47% 0
14% 13 C 1
3,350 i 84 39.7 i 0.2
2% 4%
2 (4) 3 (6) 2 (4)
ponic hypertensives) l ( 5 0 )
26 -t 1* 165 t 1
61.9 L 1.1 13.6 L 0.6
32%* 21
20% 12 -t 1
3,116 2 56* 39.4 i 0.2
4% 8%
9 (11)* 11 (14)*
5 (6 ) 4 (80)
*P = <.05, residents of 1,600 vs. 3,100 m
chronic medical conditions. Four of five chronically hypertensive women at high al- titude developed superimposed preeclamp- sia (Table 1). Three of these five women had proteinuria a 2 + , four had significant edema, and two had CNS symptoms. The 11 women who developed preeclampsia at high altitude were without conditions known to predispose women to develop preeclampsia (vascular disease, diabetes, twin pregnancy, etc.). Eight of the 11 preeclamptic women were primigravid; thus nearly one-third of primigravid women studied prospectively at high altitude developed preeclampsia. Of the 11 preeclamptic women, 7 had protei- nuria >2+ and 8 had significant edema. Other symptoms included hepatic (n = 3), CNS (n = 21, and coagulation abnormalities (n = 3). One woman developed eclampsia. Infant birth weight and gestational age were reduced among the preeclamptic women at high altitude (2,763 5 233 g, 37.6 2 1.0 weeks vs. 3,174 + 58 g, 39.9 + 0.2 weeks in women at 3,100 m who remained normotensive, P < .05).
In addition to the prospectively studied subjects, data from two chart review studies were considered. The first compared blood pressures and symptoms of preeclampsia in near-term Denver (1,600 m, n = 138) and Leadville (n = 167) pregnancies (Moore et al., 1982). The second was a more recent study which compared blood pressure throughout pregnancy, symptoms, and risk
factors for preeclampsia in low- and high- altitude Colorado communities matched for demographic characteristics (Burlington, 1,260 m, n = 125; and Leadville, 3,100 m n = 97, Palmer et al., 1994). This review considers the data derived from these previ- ous studies with respect to (or in the context of) each component of the model presented in Figure 1.
ESTROGEN, PROGESTERONE, AND VASOREACTIVITY
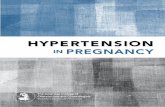
Ovarian steroid hormones likely influence the control of blood pressure and vascular tone. In nonpregnant women there is nor- mally little change in blood pressure with age until the time of the menopause, when blood pressure begins to rise and continue to rise with age (Roberts and Maurer, 1977; Weiss, 1972). Premenopausal women com- pared with men have lower systemic vascu- lar resistance at any given blood pressure (Messerli et al., 1987). Blood pressure falls slightly during the luteal phase of the men- strual cycle (Dunne et al., 1991). Adminis- tration of estrogen or progestin separately to post-menopausal women did not change mean arterial pressure. However, treatment with estrogen and progestin combined, re- sulting in serum concentrations comparable to the follicular and luteal phases of men- strual cycle, lowered mean arterial pressure (Regensteiner et al., 1991; Fig. 2).

HYPOXIA AND PREECLAMPSIA 187
-10- Estrogen Progeslin Eslrogen+Progeslin
Treatment data from Regenoleiner etel. 1991 * p<.O5 compared with placebo
Fig. 2. Neither estrogen nor progestin treatment (7 days) had any effect on the blood pressure of post-meno- pausal women. However, estrogen and progestin com- bined reduced mean arterial pressure (drawn from data in Regensteiner et al., 1991).
In normal pregnancy both estradiol and progesterone increase progressively and in proportion to one another; hence, the ratio of progesterone to estradiol is unchanged from the nonpregnant state throughout preg- nancy, even though absolute hormone con- centrations increase dramatically (Tulchin- sky et al., 1972). The balance between estradiol and progesterone may be as impor- tant as the absolute levels of the hormones present, as suggested by review of vasospas- tic conditions which are more common in women than men, and are associated with changes in hormone balance (White et al., 1994). In vitro studies indicate that estra- diol enhances endothelium-dependent va- sodilation (Bell and Coffey, 1982; Miller and Vanhoutte, 1991), but few studies have ad- dressed the combined effects of estrogen and progesterone. Limited data suggest that an excess of progesterone relative to estradiol may increse vascular reactivity. Progester- one opposes estradiol's enhancement of en- dothelium-dependent relaxation (Miller and Vanhoutte, 1991). Placentas from preec- lamptic women produce more progesterone than those of normal women, and this excess of progesterone inhibits the vasodilator prostacyclin (Walsh and Coulter, 1989). Since unchanged or falling estrogen with no change in progesterone concentrations have been reported to precede the onset of hyper- tension in preeclamptic women (August et al., 1990; Tulchinsky and Okada, 1975), it was therefore asked whether women resid-
ing at high altitude had reduced estradiol and/or elevated progesterone concentra- tions.
Nonpregnant estradiol and progesterone concentrations were within the low-altitude range (Table 2; Zamudio et al., 1994). Women who remained normotensive during pregnancy had no change in estradiol con- centrations after week 20, and hence values were lower at week 36 of pregnancy than values reported at sea level (Table 2). Women who developed transient hyperten- sion or preeclampsia had a marked fall in estradiol concentrations between weeks 30 and 36 of pregnancy (Table 2). These obser- vations are consistent with results of previ- ous investigations in Peru, where Sobrevilla et al. (1968) found that urinary excretion of estradiol was lower in near-term pregnant women at 4,200 m compared with women at sea level. Hypoxia may be relevant to the failure of estradiol to increase in normal women and to the fall in estradiol among hypertensive subjects at 3,100 m. The Po, of cord blood in the infants of preeclamptic women is lower than that of infants of nor- motensive women (Clemetson and Church- man, 1953). Likewise, placental oxygen con- sumption is decreased in the placentas of preeclamptic women (MacKay, 1957). The aromatase enzyme complex is required for the production of estradiol (but not progest- erone), and is sensitive to Po, (Kautsky and Hagennan, 1980). At the reduced placental P0,s present at 3100 m inhibition of the aro- matase enzyme complex could limit estra- diol production (Blechner et al., 1968). Thus, data from several sources indicate that low- ered placental oxygen transfer and/or con- sumption may be a characteristic of preec- lamptic pregnancy, and might thereby contribute to the low estradiol concentra- tions observed in preeclamptic women (Au- gust et al., 1990; Tulchinsky and Okada, 1975). Progesterone had not been measured during pregnancy at high altitude prior to our study. Progesterone concentrations rose progressively throughout pregnancy at 3100 m, resulting in higher progesterone/ estradiol ratios than in the nonpregnant state or during normal pregnancy at low al- titude (Table 2). Progesterone concentra- tions were similar in normotensive and transiently hypertensive women, but women who developed preeclampsia had an extraordinary rise in progesterone concen- trations between week 30 and 36 of preg-

S. ZAMUDIO ET AL.
TABLE 2. Placental steroid hormone eoncentratwns (mean -t SEM, nglmd, during pregnancy at 3,100 m1
1 aa
Nonpregnant2 Week 203 Week 304 Week 365
Normotensive (n = 32) Estradiol 0.11 + 0.03 5.7 t 0.8* 6.8 i 1.2* 6.8 i 1.0* Progesterone 3 2 2 94 i 6* 174 i 13* 223 & 14* Progesterondestradio16 8 * 2 28 * 5* 49 i 10* 57 i 10*
Preeclampsia (n = 4) 1.8 C 0.2*>** Estradiol 0.11 -t 0.03 6.6 -t 2.6" 11.3 2 2.5*
Progesterone 4 2 3 92 ? 17* 193 t 29** 418 2 63*,"* F'rogesteroneiestr adioP 16 2 4 56 ? 45 20 t 7 248 -t 56*>**
Estradiol 0.20 i 0.08 3.3 ? 0.9* 7.7 ? 0.6* 1.8 + 0.1*,** Transient hypertension (n = 4)
Progesterone 1 + 0 80 i 10* 236 i 71* 200 ? 34* 113 i 25* Progesterone1estradiol6 7 t 16 34 i 12 30 t 7
'Sea level rilllges (references = Tulchinsky et al., 1972; Yen 1986). 2Nonpregnant: estradiol 0.0W.4 ng/ml, progesterone 2.5-28 nglml. 'Week 20: estradiol2-8 nglml, progesterone 20-75 nglml. 4Week 3 0 estradiol615 ng/ml, progesterone 4s-180 ng/ml. 5Week 36: estradiol7-28 nglml, progesterone 96220 ngiml. 'Progesteroneiestradiol ratio: 2-30, nonpregnant and all stages of pregnancy. *P < .05 mmparison with nonpregnant value. **P < .05, comparison of preeclampsia or transient hypertension with norrnotensive women at 3,100 m. (Data from Zamudio et al., 1994).
nancy. Estradiol correlated negatively and progesterone positively with maternal mean arterial pressure. It was concluded that the ratio of progesterone to estradiol was in- creased during pregnancy at high altitude and that elevated progesterone relative to estradiol concentrations may contribute to the development of high blood pressure dur- ing pregnancy (Zamudio et al., 1994b).
BLOOD PRESSURE Women at 3,100 m were compared to
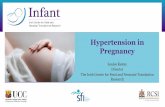
women at 1,600 m. The distribution of blood pressures near term was right-shifted towards higher values among pregnant women at high altitude (Moore et al., 1982). This shift towards higher blood pressures was associated with a higher incidence of hypertension during pregnancy and its ac- companying symptoms, upper extremity edema and proteinuria (Fig. 3). In a more recent study conducted in two Colorado com- munities (1,260 m and 3,100 m) matched for census characteristics, the earlier observa- tion of an increased incidence of preeclamp- sia was confirmed (16.1% at 3,100 m vs. 3.5% at 1,260 m, Palmer et al., 1994). Even among women who remained normotensive, the second trimester fall in blood pressure that occurs during normal pregnancy was absent; thus blood pressures were higher from weeks 16 to 32 in normotensive women at 3,100 m compared with 1,260 m (Palmer et al., 1993). This failure of blood pressure to fall is important to pregnancy outcome.
30, Hypertension in pregnancy
Proteinuria 2 I + 0 bpper extremit/ edema
u)
0 .cI
a 20 a S u)
0 c
10
0 1600m 2410m 3100111
Altitude datafrom Moore etal. 1982
Fig. 3. The incidence of hypertension in pregnancy increased with altitude in Colorado. Data on upper ex- tremity edema were available only from 1,600 m and 3,100 m, but this symptom was also increased at high altitude. The incidence of proteinuria was similar at 1,600 m and 2,410 m, but greater at 3,100 m.
When second trimester mean arterial pres- sures are 285 mmHg, the incidence of still- births, perinatal mortality, and the risk for developing a hypertensive complication of pregnancy are increased (Page and Chris- tianson, 1976; Moutquin et al., 1985; Ales et al., 1990). In our samples, 53% of women at 3,100 m vs. 25% of women at 1,260 m had second trimester mean arterial pressures 385 mmHg (2' < .001, Palmer et al., 1994). Others have observed that blood pressure fails to show the normal second trimester decline in women destined to develop pre-

HYPOXIA AND PREECLAMPSIA 189
2000 1 -
3100 m low-altitude 3100 m normotensive hypertensive normal
(Long0 and Haraesly 19811
Fig. 4. Blood volume expansion was lower in women who developed transient hypertension or preeclampsia compared with those who remained normotensive. The total increase in blood volume among women who re- mained normotensive was consistent with values re- ported from normal pregnancy at low altitude.
eclampsia; thus all pregnant women at high altitude, not just those who developed preec- lampsia, had a blood pressure course more characteristic of preeclampsia than of nor- mal pregnancy.
BLOOD VOLUME The increase in blood volume during preg-
nancy was normal in women who remained normotensive during pregnancy at 3,100 m (Zamudio et al., 1993a). However, women who developed preeclampsia or transient hypertension had either a fall in blood vol- ume during the third trimester or failed to increase their blood volume during preg- nancy. As a result, the blood volume in- crease with pregnancy was two-thirds lower in women who developed hypertension com- pared with those who did not (Fig. 4). Greater maternal plasma volume expansion during pregnancy correlated with lower mean arterial pressure (r = -0.73, P < .001). Lower mean arterial pressure, in turn, correlated with higher maternal arte- rial 0, saturation (r = -0.58, P < .01). Blood volume expansion was important to both maternal and fetal well-being, as in- fant birth weight also correlated positively with third trimester volume expansion (Za- mudio et al., 1993a).
While blood volume expansion with preg- nancy was normal in women who remained normotensive, the subjects’ absolute blood volumes were much lower than those ob- served in pregnant women at low altitude, due to lower values in the nonpregnant
state. Nonpregnant women at 3,100 m had a normal red cell mass and reduced plasma volume compared with women at 1,600 m (Zamudio et al., 1993a). This finding was unexpected, as it is well known that in male residents of high altitude, blood volume is higher than values at sea level, due to a sub- stantially increased red cell mass and lower or normal plasma volume (Hurtado et al., 1945; Sanchez et al., 1970). Blood volume in women residing at high altitude had not been measured prior t o our study. Low non- pregnant plasma volumes have been associ- ated with the development of preeclampsia and other pregnancy complications( Croall et al., 1978; Gibson, 1973). It is possible that women increase oxygen canying capacity at high altitude via hemoconcentration rather than increase in red cell number, resulting in a chronic reduction in plasma volume, which may in turn compromise pregnancy. Chronic reduction in plasma volume could be due to arterial or venoconstriction. Arte- rial vasoconstriction is supported by the finding that plasma volume decreases as pe- ripheral resistance increases (Dustan et al., 1973). Venoconstriction is supported by de- creased venous distensibility in acute high- altitude exposure (Weil et al., 1971). Re- gardless of whether the reduction in plasma volume is due to arterial and/or venocon- striction, it is possible that the low nonpreg- nant plasma volumes present in women re- siding at high altitude present an additional challenge to successful physiological adjust- ment to pregnancy.
SYSTEMIC VASCULAR RESISTANCE Data from humans who are permanent
residents rather than visitors to the high altitude environment are scant. Moret et al. (1972) measured systemic vascular resis- tance in men residing at 3,700 and 4,375 m, and found slightly higher systemic vascular resistance. Men native to 4,540 m who were studied prior to and after moving to sea level had a fall in systemic vascular resistance with residence at sea level (Banchero and Cruz, 1970). Systemic vascular resistance has not been measured in women residing at high altitude, and certainly not during preg- nancy. However, if women pregnant at high altitude have lower blood volume and higher blood pressures than their low altitude counterparts, it may be inferred that sys- temic vascular resistance is elevated. This is supported by experimental animal studies

190 S. ZAMUDIO ET AL.
in which pregnant guinea pigs at high alti- tude had higher systemic vascular resis- tance than low altitude controls (Harrison and Moore, 1990). Increased systemic vascu- lar resistance during pregnancy may lead to reduced uteroplacental blood flow, as mea- sured by radiolabelled tracers or by Doppler ultrasound arterial wave form indices such as absent diastolic flow in the uterine arter- ies (Nylund et al., 1983; Campbell et al., 1983).
UTEROPLACENTAL BLOOD FLOW Noninvasive techniques for determining
volumetric uterine artery blood flow during human pregnancy were developed to estab- lish values for women pregnant at low alti- tude. Using Doppler and imaging ultra- sound, we found that an increase in uterine artery volumetric flow during pregnancy at low altitude was due in equal proportion to increased uterine artery diameter and to in- crease in blood mean flow velocity. Uterine artery diameter doubled by week 20 of preg- nancy and thereafter increased only mod- estly. Increase in mean flow velocity was progressive throughout pregnancy, account- ing for the majority of change in volumetric flow after week 20 (Palmer et al., 1992). In similar studies conducted at 3,100 m, unilat- eral uterine artery blood flow at week 36 of pregnancy was one-third lower than in women at 1,600 m. However, the sample sizes for these quantitative studies were very small (n = 5 and n = 8 at 3,100 m and 1,600 m, respectively; Zamudio et al., 1995b). Uterine artery flow velocity did not increase after week 24 of pregnancy in women who eventually developed preec- lampsia at 3,100 m (n = 7 preeclampsia, n = 3 chronic hypertension plus preeclamp- sia), suggesting that uterine artery volumet- ric blood flow failed to increase during the third trimester in these women (Zamudio et al., 1995a).
MATERNAUFETAL WELL-BEING Residence at high altitude undoubtedly
compromises maternal and fetal well-being, at least in the available North American studies. Reduced birth weights and an in- creased incidence of preeclampsia are detri- mental to maternal and infant health and survival (Ales et al., 1990; Lindheimer and Katz , 1985). During the period 1957-1976, Colorado statewide statistics indicated that infant mortality was twice as great at high compared with low altitude (McCullough et
al., 1977). More recent data indicated that, while infant mortality is no longer greater at high altitude in Colorado, women from high altitude utilize tertiary care facilities three times as often as women from low altitude (Unger et al., 1988). Add to this the cost of treating women with preeclampsia (gener- ally hospitalization, bedrest, antihyperten- sive medications, and often early delivery) and the economic costs in health care and lost productivity can be enormous. There may be more subtle disadvantages as well. The infants of preeclamptic women do not score as well as infants delivered to nor- motensive women on standard neonatal neurophysiological and behavioral assess- ments, showing evidence of dysmaturity for their gestational age. At least one study from Peru demonstrated that high-altitude neonates delivered to normotensive mothers resembled the infants of preeclamptics in motor and behavioral assessments (Saco- Pollitt, 1981). Such studies have not been performed in Colorado and other high-alti- tude locations, but would be of interest, par- ticularly if infants could be studied longitu- dinally.
This review was limited to those studies which we have conducted on residents of Colo- rado. The subjects were primarily of Euro- pean descent and were no more than second or third generation inhabitants of high altitude. The increased incidence of hypertension dur- ing pregnancy, and the reduction in blood vol- ume and uterine blood flow noted among North American women at high altitude may not hold true for high-altitude populations elsewhere. For example, Tibetans show little evidence of altitude-associated intrauterine growth retardation, and Peruvians have an altitude-associated reduction in birth weight that is less than that observed in North Amer- icans (Moore, 1990; Zamido et al., 199313). The absence of intrauterine growth retardation among Tibetans may be due to maternal physiological characteristics which more closely resemble those observed at sea level. If natural selection disfavors women who de- velop hypertension during pregnancy, it would be expected that populations with longer evolutionary histories at high altitude have an incidence of hypertension during pregnancy that is no more than that observed at sea level.
SUMMARY Data from women pregnant at high com-
pared with low altitude suggest that a num-

HYPOXIA AND PREECLAMPSIA 191
ber of physiological adjustments to preg- nancy are compromised, either by the influence of chronic hypoxia on maternal ad- aptation to pregnancy (e.g., low estradiol levels during pregnancy), or by the subject's preexisting characteristics resulting from high-altitude residence (e.g., low plasma volume in the nonpregnant state). In gen- eral, the physiological profile of women pregnant at high altitude is similar to that of women who develop hypertension during pregnancy at lower elevations, as evidenced by altered hormonal profiles (low estradiol), no second trimester fall in blood pressure, low blood volume, presumably increased systemic vascular resistance, and lower uterine blood flow, which might combine to compromise both fetal growth and maternal well-being.
Physiological adaptation to high altitude allows for increased oxygen transport and better health for individuals. However, such adjustments may contribute to lowered re- productive success for women whose resi- dence at high altitude may predispose them to develop hypertensive complications of pregnancy. That adaptation to altitude for short-term survival may impose a reproduc- tive disadvantage upon some women point to the difficulties in determining whether a physiological adjustment to a chronic envi- ronmental stress is beneficial or not. Clearly, more studies are warranted con- cerning female adaptation to high altitude and upon the likelihood that these adjust- ments are truly beneficial in the sense of better enabling an organism to live and to reproduce in a particular environment (Dobzhansky, 1968).
ACKNOWLEDGMENTS The research reviewed in this manuscript
was supported by NIH HL 14895, HD 00681, HL 07171, NSF BNS-8903554, the Univer- sity of Colorado Health Sciences Center De- partment of Anesthesiology Research Fund, and a Deans Small Grant Fund Dissertation Award from the University of Colorado at Boulder.
LITERATURE CITED Ales IU, Norton ME, and Druzin ML (1988) Early pre-
diction of antepartum hypertension. Obstet. Gynecol. 73:92&933.
Ales KL, Norton ME, and Druzin ML (1990) The clinical significance of predictions based on screening second trimester mean arterial pressure: Adverse maternal and infant outcomes. J . Clin. Epidemiol. 43t117-124.
August P, Lenz T, Ales KL, Druzin ML, Edersheim TG, Hutson M, Muller FB, Laragh JH, and Sealy JE (1990) Longitudinal study of the renin-angiotensin- aldosterone system in hypertensive pregnant women: Deviations related to the development of superim- posed preeclampsia. Am. J . Obstet. Gynecol. 163: 1612-1621.
Banchero N, and Cruz JC (1970) Hemodynamic changes in the Andean native after two years at sea level. Aerospace Med. 41:84%853.
Bell C, and Coffey S (1982) Factors influencing oestro- gen-induced sensitization to acetylcholine of guinea pig uterine artery. J. Reprod. Fertil. 66:133-137.
Blechner JN, Cotter JR, Hinkley CM, and Prystowsky H (1968) Observations on prebmancy at high altitude. Am. J. Obstet. Gynecol. 102t794-805.
Blekta M, Hlavaty V, Trnkova M, Bend1 J , Bendova L, and Cytil M (1970) Volume of whole blood and abso- lute amount of serum proteins in the early stage of late toxemia of pregnancy. Am. J. Obstet. Gynecol. 106:lC-13.
Brosens IA, Robertson WB, and Dixon HG (1972) The role of the spiral arteries in the pathogenesis of preec- lampsia. In RM Wynn (ed.): Obstetrics and Gynecol- ogy Annual. New York Appleton-Century-Crofts, pp.
Broughton-Pipkin F (1989) Hypertension in pregnancy: A physiological response to a pathological problem? Dev. Pharmacol. Ther. 13t184-189.
Browne JL, and Veal1 N (1953) The maternal placental blood flow in normotensive and hypertensive women. J . Obstet. Gynaecol. Br. Commonwealth 6Or141-147.
Campbell D, Griffin DR, Pearce JM, Diaz-Recasens J, Cohen-Overbeek TE, Wilson K, and Teague MJ (1983) New Doppler technique for assessing uteroplacental blood flow. Lancet 26t675-677.
Chesley LC, and Tepper IH (1967) Effects of progester- one and estrogen on the sensitivity to angiotensin 11. J. Clin. Endocrinol. 27.576-586.
Clemetson CAB, and Churchman J (1953) Oxygen and carbon dioxide content of umbilical artery and vein blood in toxaemic and normal pregnancy. J . Obstet. Gynaecol. Br. Commonwealth 6Ot335-344.
Croall J, Sherrif S, and Matthews J (1978) Non-preg- nant maternal plasma volume and fetal growth retar- dation. Br. J. Obstet. Gynaecol. 85:9&95.
Curran-Everett D, Morris KG, and Moore LG (1991) Regional circulatory contributions to increased sys- temic vascular conductance of pregnancy. Am. J . Physiol. 261:H1842-1847.
Dobzhansky T (1968) Adaptedness and fitness. In RC Lewontin (ed.): Population Biology and Evolution. Syracuse: Syracuse University Press, p. 111.
Dunne FP, Barry DG, Ferris JB, Grealy G, and Murphy D (1991) Changes in blood pressure during the normal menstrual cycle. Clin. Sci. 81.515-518.
Dustan HP, Tarazi RC, Bravo EL, and Dart RA (1973) Plasma and extracellular fluid volumes in hyperten- sion. Circ. Res. Suppl. ltI73-181.
Easterling TR, Benedetti TJ, Schmucker BC, and Mill- ard SP (1990) Maternal hemodynamics in normal and preeclamptic pregnancies: A longitudinal study. Ob- stet. Gynecol. 76t1061-1069.
Gallery EDM, Ilunyor SN, Ross M, and Gyory AZ (1979) Plasma volume contraction: A significant factor in both Dremancv-associated hmertension (DreeclamD-
177-191.
sia) and-chronic hypertensi'on in pregn&cy. Q. 3. Med. 192r593-602.
Gant NF, Daley GL, Chand S, Whalley PJ, and MacDon- ald PC (1973) A study of angiotensin I1 pressor re-

S. ZAMUDIO ET AL. 192
sponse throughout primigravid pregnancy. J . Clin. In- vest. 52t2682-2687.
Gibson HM (1973) Plasma volume and glomerular fil- tration rate in pregnancy and their relation to differ- ences in fetal growth. J. Obstet. Gynaecol. Br. Com- monwealth 80: 1067-1074.
Groenendijk R, Trimbos BMJ, and Wallenburg HCS (1984) Hemodynamic measurements in preeclampsia: Preliminary observations. Am. J. Obstet. Gynecol. 25Ur232-236.
Harrison GL, and Moore LG (1990) Systemic vascular reactivity during high-altitude pregnancy. J. Appl. Phvsiol. 69:201-206.
Hughes EC (ed) (1972) Obstetric-Gynecologic Terminol- ogy. Philadelphia: Davis.
Hurtado A, Merino CF, and Delgado E (1945) Influence of anoxemia on hematopoietic activity. Arch. Intern. Med. 75t284-323.
Kautsky MP, and Hagerman DD (1980) Kinetic proper- ties of steroid 19-hydroxylase and estrogen synthetase from porcine ovary microsomes. J . Steroid Biochem. 13:1283-1290.
Lehmann DK, Mabie WC, Miller JM, and Pernoll ML (1987) The epidemiology and pathology of maternal mortality: Charity Hospital of Louisiana in New Or- leans, 1965-1984. Obstet. Gynecol. 69:835-840.
Lindheimer MD, and Katz AL (1985) Hypertension in pregnancy. N. Engl. J. Med. 313t675-680.
Longo LD, and Hardesty J S (1984) Maternal blood vol- ume: Measurement, hypothesis of control and clinical considerations. Rev. Perinat. Med. 5:35-59,
MacKay RB (1957) Observations on placental oxygen uptake in placentas from normal and toxaemic preg- nancies. J. Obstet. Gynaecol. Br. Commonwealth 64: 185-197.
McCullough RE, Reeves JT, and Liljegren RL (1977) Fetal growth retardation and increased infant mortal- ity at high altitude. Arch. Environ. Health 32:36-39.
Messerli FH, Garavaglia GE, Schneider RE, Sundgaard- Riise K, Nunez BD, and Amodeo C (1987) Disparate cardiovascular findings in men and women with es- sential hypertension. Ann. Intern. Med. 107:158-161.
Miller VM, and Vanhoutte PM (1991) Progesterone and modulation of endothelium-dependent responses in canine coronary arteries. Am. J. Physiol. 261rR102% R1027.
Moore LG (1990) Maternal 0, transport and fetal growth in Colorado, Peru and Tibet high-altitude res- idents. Am. J. Hum. Biol. 2t627-637.
Moore LG, Hershey DW, Jahnigen I), and Bowes W (1982) The incidence of pregnancy-induced hyperten- sion is increased among Colorado residents at high altitude. Am. J. Obstet. Gynecol. 144.423429,
Moret P, Covarrubias E, Coudert J, and Duchosal F (1972) Cardiocirculatory adaptation to chronic hy- poxia 111. Comparative study of cardiac output, pul- monary and systemic circulation between sea level and high altitude residents. Acta Cardiol. 27:59& 619.
Moutquin JM, Rainville RN, Giroux L, Raynauld P, Amyot G, Bilodeau R, and Pelland N (1985)A prospec- tive study of blood pressure in pregnancy: Prediction of preeclampsia. Am. J. Obstet. Gynecol. 1,51:191- 196.
Nisell H, Kjemdahl P, and Linde B (1985) Cardiovascu- lar responses to circulating catecholamines in normal pregnancy and in pregnancy-induced hypertension. Clin. Physiol. 5t479-493.
Nylund L, Lunnell NO, Lewander R, and Sarby B (1983)
Uteroplacental blood flow in intrauterine growth re- tardation of fetal or maternal origin. Br. J. Obstet. Gynaecol. 90: 16-20,
Page EW, and Christianson R (1976) The impact of mean arterial Dressure in the middle trimester uaon the outcome 2 pregnancy. Am. J. Obstet. Gynecol. 225:740-745.
Palmer SK, Zamudio S, Coffin C, Parker S, Stamm E, and Moore LG (1992) Quantitative estimation of hu- man uterine artery blood flow and pelvic blood flow redistribution in pregnancy. Obstet. Gynecol. 80: 1000-1006.
Palmer SK, Moore LG, Berman JC, Cregger B, and Za- mudio S (1994) Altitude and hypertensive complica- tions of pregnancy. Am. J. Phys. Anthropol. Suppl. 18:158 (abstract).
Regensteiner JG, Jiatt WR, Ryyny RL, Pickett CK, Woo- dard WD, and Moore LG (1991) Short-term effect of estrogen and pmgestin on blood pressure of normoten- sive postmenopausal women. J. Clin. Pharmacol. 31: 543-548.
Roberts J (1989) Pregnancy-related hypertension. In R Creasy and R Resnick (eds.): Maternal-Fetal Medi- cine. Philadelphia: Saunders, pp. 777-823.
Roberts J, and Maurer K (1977) Blood pressure levels of persons G74 years, United States, 1971-1974. Vital and Health Statistics, Series 11, No. 203.
Roberts JM, Taylor RN, Musci TJ, Rodgers GM, Hubel CA, and McLaughlin ML (1989) Preeclampsia: An en- dothelial cell disorder. Am. J. Obstet. Gynecol. 261: 1200-1204.
Saco-Pollitt C (1981) Birth in the Peruvian Andes: Phys- ical and behavioral consequences in the neonate. Child Dev. 52839-846.
Sanchez C, Merino C, and Figallo M (1970) Simulta- neous measurement of plasma volume and red cell mass in polycythemia of high altitude. J. Appl. Phys- iol. 28r775-778.
Sobrevilla LA, Romero I, Kruger F, and Whittembury J (1968) Low estrogen excretion during pregnancy a t high altitude. Am. J. Obstet. Gynecol. 102:828-833.
Tulchinsky D, and Okada DM (1975) Hormones in hu- man pregnancy. Am. J. Obstet. Gynecol. 121.293-299.
Tulchinsky D, Hobel CJ, Yeager E, and Marshall JR (1 972) Plasma estrone, estradiol, estriol progesterone and 17-hydroxyprogesterone in human pregnancy. Am. J. Obstet. Gynecol. 112:1095-1100.
Ueland K, Novy MJ, Peterson EN, and Metcalfe J (1969) Maternal cardiovascular dynamics: IV. The influence of gestational age on the maternal cardiovascular re- sponse to posture and exercise. Am. J. Obstet. Gyne- col. 104:85&863.
Unger C, Weiser JK, McCullough RE, Keefer S, and Moore LG 11988) Altitude, low birth weight and infant mortality in Colorado. J. Am. Med. Assoc. 259:3427- 3432.
Walsh SW, and Coulter S (1989) Increased placental progesterone may cause decreased placental prostacy- clin production in preeclampsia. Am. J. Obstet. Gyne-
Weil JV, Byme-Quinn E, Battock DJ, Grover RF, and Chidsey CA (1971) Forearm circulation in man at high altitude. Clin. Sci. 40:235-246.
Weiss NS (1972) Relationship of menopause to serum cholesterol and arterial blood pressure: The United States health examination survey of adults. Am. J. Epidemiol. 96r237-241.
White M, Zamudio S, Stevens T, Tyler R, Lindenfeld J, Leslie K, and Moore LG (1994) Estrogen, progesterone
C O ~ . 262:1586-1592.

HYPOXIA AND PREECLAMPSIA 193
and cellular mechanisms of vascular control. Endo- crine Reviews (in press).
Yen SSC (1986) Endocrine physiology of pregnancy. In DN Danforth and JR Scott (eds.): Obstetrics and Gy- necology, 5th Edition. Philadelphia: J.B. Lippincott, pp. 340457.
Zamudio S, Palmer SK, Dahms TE, Berman JC, McCul- lough RG, McCullough RE, and Moore LG (1993a) Blood volume expansion, preeclampsia, and infant birth weight at high altitude. J. Appl. Physiol. 74: 1566-1573.
Zamudio S, Droma T, Norkyel KY, Acharya G, Zamudio JA, Niermeyer SN, and Moore LG (1993b) Protection from intrauterine growth retardation in Tibetans at high altitude. Am. J. Phys. Anthropol. 91:215-224.
Zamudio S, Palmer SK, Dahms TE, Berman JC, and Moore LG (1995a) Alterations in uteroplacental blood flow precede the onset of hypertension in preeclamp- sia at high altitude. J . Appl. Physiol. (in press).
Zamudio S, Leslie KK, White M, Hagerman DD, and Moore LG (1994) Low serum estradiol and high serum progesterone concentrations characterize hyperten- sive pregnancies at high altitude. J. SOC. Gynecol. In- vest. 1:197-205.
Zamudio S, Palmer SK, Droma TS, Coffin C, Stamm E, and Moore LG (1995b) Effect of altitude on uterine artery blood flow during normal pregnancy. J . Appl. Physiol. (in press).