HGBH Evaluation- UJIK

If you can't read please download the document
Transcript of HGBH Evaluation- UJIK
-
7/27/2019 HGBH Evaluation- UJIK
1/31
Service User
and CarerInvolvement in
the NationalMental Health
DevelopmentUnit
-
7/27/2019 HGBH Evaluation- UJIK
2/31
AcknowledgementsThis report was written by Dr DanRobotham and Jo Ackerman of theMental Health Foundation.
The following people also contributedto this evaluation through guidance,editing, and/or through attendance atsteering group meetings:
Anne Beales, Laurie Bryant, PatriciaChambers, Julie Charles, Sean Cobley,David Crepaz-Keay, Lu Duhig, AlisonFaulkner, Denise Forde, Kathryn Hill,Kirsten Morgan, Vicky Nicholls, PhilPartridge, Fran Singer, Dominic Walker,Sarah Yiannoullou.
-
7/27/2019 HGBH Evaluation- UJIK
3/3101
Contents02 Executive Summary04 Background06 Method08 Results17 Discussion
19 References20 Appendices
-
7/27/2019 HGBH Evaluation- UJIK
4/3102
01ExecutiveSummary
demographic groups, with somedegree of success. However,particular care needs to be made toensure that carers and people withsevere mental illness can berepresented. Furthermore, thelanguage and culture of involvementmay be o-putting to people who havenot been involved previously.
NMHDU had involvement processesin place prior to NIP input. Serviceusers and carers contributed to keydocuments and were involved insteering and advising projects.However, some people wanted orneeded more support to be involved.This included practical support (suchas expenses and fees being paid), andemotional support. Feedback fromNMHDU suggested that NIP had dealtwith these matters sensitively when
they arose, but NIP should explicitlyfocus on providing clear guidance onsupport, which may inuence peoplesdecision to get involved.
Feedback to service users and carersabout the impact of their involvementwas needed. Changing circumstanceswith projects and programmes madeit dicult to maintain this consistentlyacross the lifespan of NMHDU andprior organisations. Collecting and
providing feedback from organisationslike NMHDU (and others who maycommission NIP in future) is anothertask that NIP should undertake.
This study should be commended forits use of various, pragmatic methods,but it should also be noted for its smallsample size, which was notnecessarily representative of serviceusers and carers more widely. Onenotable example is that there were alarge number of responses from white
British females over the age of 45.
Within the PPPI framework, NIPappears to have the potential tofacilitate involvement practices withinorganisations such as NMHDU. BothNIP and NMHDU have a wealth ofinformation about how to involveservice users and carers eectively.NIP is now in the position to collect,share and harness this information.The key challenge for the future will
be how NIP orientates itself within thenew external environment. The legacyof NMHDU regarding service user andcarer involvement will depend uponthe continued existence of serviceuser and carer-led collaborations likeNIP.
The National Mental HealthDevelopment Unit (NMHDU) hasbeen working with the NationalInvolvement Partnership (NIP) topromote service user and carerinvolvement in Government led(Department of Health and NHScommissioned) mental healthprojects and initiatives. NIPincludes a number of organisationsfocusing on service user and/orcarer involvement. The partnersare NSUN, Together, Aya Trust,Catch-a-Fiya, Attend, EqualitiesNational Council, the MentalHealth Foundation and the SocialPerspectives Network.
This report highlights the ndings ofan evaluation of service user and carerinvolvement within NMHDU and priororganisations such as the Care
Services Improvement Partnership(CSIP) and the National Institute forMental Health in England (NIMHE).We evaluated how NIP has facilitatedservice user and carer involvement inthis context. Findings were analysedand are presented in accordance withthe PPPI (Purpose, Presence, Processand Impact) framework, as devised byNIP during the course of this project.
Data was collected from a variety of
sources; service users, carers andprofessionals who had been involvedin NMHDU, NIMHE and CSIP projects.We collected data through severalmethods; surveys, interviews, practiceexamples, and collecting feedbacksurveys from NIP activities.
NIP activities included runningpromotional events to developnetworks of service users and carers,facilitating seminars to shareinformation between service users,
carers and professionals, organisingfocus groups for NMHDU projects inorder to represent the voice of serviceusers and carers, collecting casestudies to inform the mental healthstrategy, and distributingquestionnaires to members of thenetwork.
The evaluation highlights how NIP andNMHDU have worked together tofacilitate service user and carer
involvement. Within this, there havebeen positives and negatives.Ensuring diverse representation fromservice users and carers waschallenging. The two organisationsattempted to ensure diverserepresentation across dierent
-
7/27/2019 HGBH Evaluation- UJIK
5/3103
RecommendationsWhat is the purpose of involvement?Organisations seeking to involveservice users and carers shouldconsult with service user ledorganisations (such as NIP) to agreethe reason why involvement isneeded.
- The culture and language of serviceuser and carer involvement shouldbe understandable within thecontext of everyday life, not justwithin the context of policy andpractice. This will:
- Facilitate the presence of a morediverse range of service users andcarers within the network.
- Help NIP to build links witha more diverse range of
statutory, voluntary and privateorganisations.
- Processes should be in placefor service users and carers tomove from being interestedin involvement to becomingactive participants. Follow up forparticipants after initial engagementis essential in order to maintaininterest.
- Continuity needs to be embeddedinto the culture of service user andcarer involvement. Therefore, uponcompletion of projects, NIP canhelp signpost those involved otheropportunities and projects.
- Practical and emotional supportshould be available to help peoplebecome involved. NIP could developmentoring schemes; those whohave been involved in the past couldsupport others to become involved.
- Organisations that wish to involveservice users and carers shouldprovide feedback to those who havebeen involved NIP could collate anddisseminate feedback, providingparticipants with information aboutproject impact.
-
7/27/2019 HGBH Evaluation- UJIK
6/3104
02Background
Service user led organisations play avital role in allowing people withmental health problems to supporteach other in taking control of theirown lives and nding a road torecovery. Something Inside SoStrong (2001) is a collection ofaccounts by individuals of theirmental distress and the variety ofways they have explored to managetheir mental health. Although thethird sector have a belief in socialinclusion, and in placing the needsof the service user rst, it has beenargued that they are not the voiceof service users and that serviceuser involvement needs to improvewithin the sector (Crepaz-Keay,2008).
The National Institute of Mental Healthin England (NIMHE), which was the
national organisation supportingpolicy implementation from 20022008 prior to the establishment ofNMHDU in April 2009, had conductedvarious pieces of work to demonstrateservice user and carer involvement.The Making a Real Dierence project(MaRD; NIMHE, 2007) aimed toimprove service user and carerinvolvement in mental healthdevelopment work. MaRD developeda series of products that could be
used to guide and improveinvolvement standards, for example; aset of minimum standards to supportinvolvement with people frommarginalised groups, and a set ofguidelines for regional developmentworkers regarding payment forservice user and carer involvement.
Eective service user and carerinvolvement is needed at a nationallevel across all Governmentdepartments. The aim is to ensure
that the advice of service users andcarers is taken on board whendeveloping and implementingdecisions, particularly in relation todecisions about policy and practicewithin the eld of mental health. Thework of the National Mental HealthDevelopment Unit (NMHDU), forthe Department of Health and theNHS, provides an ideal platform bywhich to test appropriate models ofservice user and carer involvement,
which if successful can be translatedinto other areas of Government andbeyond.
The NMHDU was preceded by similarorganisations such as the Care
Services Improvement Partnership(CSIP) and the aforementionedNational Institute of Mental Healthin England (NIMHE). Both of theseorganisations strived to involveservice users and carers within theirwork. When they were disbanded, thenational support for putting policyinto practice and practice moved toNMHDU and many of the nationalwork programmes continued. Sevenseparate work programmes were runduring the existence of NMHDU, theseare listed as follows:
- Mental Health Commissioning- Improving Access to PsychologicalTherapies
- Mental Health Equalities Programme- Social Inclusion and Social Justice- Improving Mental Health CarePathways
- Promoting Wellbeing and PublicHealth
- Personalisation
In April 2009, NMHDU invitedapplications for the following tender,entitled:
Delivery of Service User and CarerInvolvement in the work of NMHDU toassure and improve programmeoutcomes and to increase active
participation in all aspects of ourwork.
The purpose of issuing this tenderwas to further develop capacity forservice user and carer involvementwithin NMHDU. The National SurvivorUser Network (NSUN) was the leadorganisation of a multi-agencypartnership that won the bid. Thisbecame known as the NationalInvolvement Partnership (NIP), whichaimed to assist service user and carer
involvement at a national and regionallevel. NIP includes a number oforganisations specialising andfocusing on service user and/or carerinvolvement in mental health. Thepartners included NSUN, Together,Aya Trust, Catch-a-Fiya, Attend,Equalities National Council, theMental Health Foundation and theSocial Perspectives Network.
The basis for NIP involvement was
reviewed in order to establishstrengths, gaps and the potential fordevelopment in involvement forservice users and carers acrossNMHDU. A scoping review gauged thelevel of service user and carer
-
7/27/2019 HGBH Evaluation- UJIK
7/3105
involvement and highlighted examplesof good practice (Faulkner, 2010). Aguideline of minimum standards forservice user and carer involvementwere drawn up. This was based uponearlier work, such as MaRD. Theguideline recommended working tothe principles of Purpose, Presence,Process and Impact (PPPI), as denedbelow:
- Purpose: having a clear purpose forinvolvement enables everyone tounderstand their role, avoidingtokenism and involvement for itsown sake.
- Presence:the number of serviceusers and carers involved; theircharacteristics in relation to theproject or programme
- Process: at what level in theproject or programme are service
users and carers involved? Are goodpractice guidelines (such as forexpense and payment policies)being applied?
- Impact: what impact, if any, areservice users or carers having onthe project or programme?
Therefore, the NIP engaged in anumber of activities in partnershipwith NMHDU. A full list of NIPactivity, including the nature and
scope of the work is given in Appendix1. This includes the following:
1 NIP promotional events. Thisinvolved organising and facilitatingtwo service user and carer eventsbased upon the PPPI standard.These events aimed to build up anetwork of service users and carerscontact details. They also aimed toinform potentially interestedparties about development workwithin national policy and practice
organisations, such as NMHDU.
2 Seminars, which involved organisingand facilitating a seminar withattendees from service user andcarer networks. This involved acollaboration between NIP and theMental Health EqualitiesProgramme, and covered how tonegotiate with GP consortia andnew commissioning landscape inlight of Equity and excellence:
Liberating the NHS whitepaper(Department of Health, 2010).
3 Four focus groups, two with serviceusers and two with members fromthe Council of Voluntary
Organisations. These took the formof two in-depth half-day sessions.The work was commissioned bythe NMHDU Social Inclusion andSocial Justice workstream, aroundthe themes of liaison and diversionwithin the criminal justice system.
4 Collating a series of 30 casestudies of service users and carers.This was for use in the formation ofthe new Mental Health Strategy.
5 Working with the Mental HealthCommissioning workstreamto provide input with thecommissioning framework,including a guideline for GPs,which led to a mental healthcommissioning panel of which NIPrepresents service user and carerviews.
6 Distributing two questionnaires toservice users and carers within thenetwork. One questionnaire wascommissioned by the Mental HealthStrategy team, and one was for theImproving Access to PsychologicalTherapies workstream withinNMHDU.
This report evaluates the work of NIPin relation to NMHDU. Specically, it
uses the PPPI standard as a model forservice user and carer involvement inorder to evaluate the following:
- service user and carer involvementwithin NMHDU (including workcarried over from CSIP and NIMHE),and;
- the eectiveness of NIP in facilitating service user and carer involvement.
-
7/27/2019 HGBH Evaluation- UJIK
8/3106
03Method
3.1 DesignThe evaluation followed theemerging PPPI model (Faulkner,2010), which provided a backgroundfor service user and carerinvolvement. Data were collectedto gauge the level of involvementin NMHDU (with reference toprojects carried over in previousorganisations such as NIMHE andCSIP), and to see how NIP hadinuenced service user and carerinvolvement work in NMHDU.
A mixed methods design wasemployed throughout the study,including qualitative methods(interviews, good practice examples)and quantitative methods (structuredsurveys).
3.2 Sample
The sample database was drawnup in collaboration with the NIPsteering group. The databaseincluded service users, carers andprofessionals who had previouscontact with national mental healthorganisations (either with CSIP,NIMHE or NMHDU).
In November 2009, surveys were sentto service users (n=51) and carers(n=8) on the NIP database. This
garnered 14 responses, acomparatively low response rate(23%). Of those who responded, themajority were female (71%) and allbut two were aged 46 or over, theremaining two respondents wereaged between 31 and 46. Some 67%described their ethnicity as WhiteBritish, one described themselvesas White and Black Caribbean, onedescribed themselves as White andAsian, two described themselves asIndian, one as Other, and one gave no
answer. English was the rst languagefor all but two of the surveyrespondents. In addition, ten of thoseservice users and carers had takenpart in a qualitative follow-upinterview. Twenty six professionalswere invited for telephone interviews,of which four responded.
In June 2010, following NIPpromotional events, a second round ofsurveys were sent to all service users
(n=123) and carers (n=62) on the NIPdatabase. We received 26 responses,again representing a low responserate (14%). The majority (81%) wereaged 45 or older, but there was aneven spread of gender (54% female).
The majority of the sample describedthemselves as White British (20/26,76%). English was the rst languagefor all but two of the surveyrespondents. In addition, 17 of thoseservice users and carers took part ina qualitative follow-up interview. Fortythree professionals were invited tocomplete a telephone interview witha member of the research team, ofwhich eight responded.
Feedback data from the NHS WhitePaper seminar and the Liaison andDiversion focus groups facilitated byNIP are also presented, 17 peopleprovided feedback for the seminarand 22 provided feedback on thefocus groups.
3.3 MeasuresInitially, the evaluation team created
two surveys to gauge service userand carer involvement; a serviceuser/carer survey and aprofessionals survey. Surveyswere reviewed and developed bymembers of the NIP steering group.The same questions were used forboth service users and carers, as wewere keen to establish similaritiesand dierences in how thesequestions were answered amongstthe two groups. The questionnaire
was initially based on the draft ofthe scoping report (prior to thedevelopment of the PPPI framework)and the MaRD report.
The service user/carer survey wasdesigned to investigate thefollowing key areas; which projectsservice users and carers had beenworking on (and in which workprogrammes these were situated),the purpose of their involvement, theamount of support oered to become
involved (including emotional andpractical support), perceived levelof inuence, and satisfaction withinvolvement. The survey included amixture of yes/no questions,open-ended questions to allowparticipants to explain and elaborate,and 5 point Likert scale questions(i.e., asking participants to respond tothe statement or question on a scalethat included the following options;Always, Often, Sometimes, Rarely,
Never). The survey also askeddemographic questions regardingage, gender and ethnicity. Finally,survey respondents were askedwhether they would like to take part ina telephone interview to explore their
-
7/27/2019 HGBH Evaluation- UJIK
9/3107
views in further detail. A full version ofthe questionnaire is shown inAppendix 2.The professionals survey exploredsimilar areas. However it was morefocused on the mechanisms that hadbeen in place to ensure successfulinvolvement, such as training andsupport, and the need to involvepeople from marginalised groups. Forthis reason, the professionalssurvey included a higher proportion ofqualitative questions, and was bettersuited to a telephone interview than toa questionnaire. It was then developedin order to guide the interviewprocess. The survey nevertheless hada number of questions on a 5 pointLikert scale in order to gainquantitative data about involvement.The professionals survey is given in
Appendix 3.
Following the NIP promotional events,the aforementioned surveys weredeveloped to include questions basedon the PPPI framework to investigatethe purpose, presence, process, andimpact of involvement. Questionswere also included to investigate theeect of the NIP events that had takenplace up until that time. Full versionsof the revised service user and carer
questionnaire are shown in Appendix4 and the professional questionnaireis shown in Appendix 5.
3.4 ProcedureSurveys were sent out via email toservice users and carers on the NIPdatabase. An email was sent outto professionals on the databaseinviting them to take part in atelephone interview. For all potentialparticipants, a reminder email wassent out seven days later to each
of the people who had not yetresponded. Telephoneinterviews were conducted bymembers of the evaluation team.Notes were taken during thetelephone interviews. These notesrepresented a written record of theinterview.
3.5 Data analysisQuantitative data was entered intoSPSS Version 16 for Windows (SPSS,
2007). Descriptive statistics wereused to explore the data. Qualitativedata was analysed using ContentAnalysis. One researcher (JA)analysed all of the transcripts,searching for key themes that arose
within the data. A second researcher(DR) also looked at the transcriptsindependently. The two researchersthen met to discuss the analysis,and reached consensus about themeaning of the themes. Analysisframeworks for the data weredeveloped and rened throughoutthe evaluation, in case new themeswere developed.
-
7/27/2019 HGBH Evaluation- UJIK
10/3108
04Results
Data are presented in two sections.Firstly, the results are presentedrelating to involvement prior to theimplementation of NIP. Secondly,results are presented in relation toinvolvement work of the NIP. Thedata are structured around the fourtenets of the PPPI framework in bothinstances.
4.1 Service user and carerinvolvement prior to NIP and the PPPIThis section describes how serviceuser and carer involvement wasimplemented in NMHDU, CSIP andNIMHE prior to the input of NIPand the development of the PPPIframework. However, the resultshave been appraised according tothe theoretical framework for PPPI(against the standards of purpose,presence, process and impact). It
assimilates data from the surveysand interview data referring toprojects that existed prior to NIP.
1 PurposeThe role of purpose in service userand carer involvement cannot beoverstated. This relates strongly tothe idea of managing expectations.Identifying the purpose ofinvolvement from the beginningand communicating it to those
who are involved is essential. Thisrelates to clarity of role in projects.A clear sense of purpose, it wasfelt, would immeasurably improvethe mechanism for service userand carer involvement:
Purpose is very important,otherwise it never works.(NMHDU Professional)
As advisors we are there to adviseand inuence not to make policy or
manage. I have seen service usersresign from national committeesbecause their role was not madeclear from start; they assumed theywere there to make policy.(Carer)
It would be valuable to involveservice users who are alreadyheavily involved in the thirdsector developing new services.We have expertise and experience
which could be utilised at theplanning and development stage.This would be far more valuable thanoccasionally asking someone to talkgenerally about service user
involvement at the oddconference.(Service user)
According to the survey data, allbut one service user felt that thepolicy and practice organisationhad shown a clear purpose in theirinvolvement, and 86% felt that theirrole had been clearly explained.
2 Presence Survey data revealed that all
of the 14 respondents to theservice user/carer questionnairehad previously been involvedin helping to change policy formental health. All had heard ofNIHME and CSIP, and all but one(a service user) had heard ofNMHDU. The service users andcarers who responded to the
questionnaire had been involvedin a variety of projects. Onaverage, the respondents hadbeen involved in three workprogrammes each. The exactbreakdown across each of thework programmes is shown belowin Table 1:
Table 1: Number of service usercarers involved in NMHDUprogrammes
WorkProgramme
NumberInvolved (n=14)
Mental HealthCommissioning
ImprovingAccess toPsychologicalTherapies
Mental HealthEqualities
SocialInclusion andSocial Justice
ImprovingMental CarePathways
Promoting
Wellbeing andPublic Health
Personalisation
6
6
8
6
9
5
6
-
7/27/2019 HGBH Evaluation- UJIK
11/3109
All but one service user hadattended national meetings for theprojects they had been working on.When asked whether theyconsidered service users or carersto be more involved in mental healthpolicy; 42% said they thoughtservice users were more involved,14% said they thought carers weremore involved. The remainder saidthat there was a similar level ofinvolvement for each.
According to data from theinterviews, there was somescepticism about therepresentativeness of serviceusers and carers involved inprevious NMHDU (and NIMHE/CSIP) projects. Furthermore, itseems that there was anestablished, traditional culture of
service user and carer involvement,bound up with an establishedlanguage.
From a BME perspective it is notthe way we envisagedinvolvement. There is still a long wayto go to make service users andcarers feel valued andrespected. There is little or no keyinvolvement nationally, and none ata strategic level.
(NMHDU Professional) You have to t in, its not for
everybodyyou have to learn thejargon(Carer)
NMHDU language is a barrier(Carer)
Service user representativeness inthe projects could have been biasedtowards people who had certain
types of mental health problems,and/or had recovered from theirmental health problem.
Just the same faces and the samevoices spouting their own views.(Service user)
People with severe mental healthproblems are rarely represented.Individuals with conditions such aslong term and enduring
psychotic conditions are poorlyrepresented simply because thevast majority of service useradvisors are mostly individualswith depressive conditions not, forexample schizophrenia.(Carer)
There is a danger that one group is expressing the needs of others
without having any realunderstanding what those needstruly are.(Carer)
Again, regardingrepresentativeness, there wassome discrepancy betweenservice user involvement and carerinvolvement. Carers sometimesfelt that their own identity had notbeen developed as fully as those ofservice users.
In New Horizons: carers only haveone sentence.(Carer)
Lumping service users andcarers together is no good for carers
because they will always put theservice users needs before theirown.(Carer)
However, this view was notuniversal:
I feel very blessed to have beenworking in a time where I waslistened to as a carer.(NMHDU Professional/Carer)
Communication between NMHDUand voluntary sector organisationswas seen as essential. A lack ofcommunication was acknowledged.This appeared to be beingaddressed:
NMHDU need to link in withvoluntary organisations, who mayhave databases of service usersand carers.(Carer)
We want to work with NSUN toreview the policies we have aboutinvolving service users and carersand would like them torecommend othershopefully wewill be able to learn from a rangeof approaches we would like tosee observations that come outthe evaluation as they happen sothat we can start to make ongoingchanges
(NMHDU Professional)
Some projects attempted to achievediversity of representation. The Shiftinitiative within the Social Inclusionand Social Justice programmeaimed to tackle stigma and
-
7/27/2019 HGBH Evaluation- UJIK
12/3110
discrimination surroundingmental health issues in England.The early intervention forpsychosis programme workedalongside other workstreams inattempting to achieve diversity:
The board attempted to berepresentative of service usersand carers across the gender, age,ethnicity, faith, sexual orientationand region.(Practice example, Shift)
There was regular participationwith some members from thePromoting Equalities in MentalHealth work programme to try toensure diversity in representation,for example, the programmeevaluated outcomes relating tofurther education opportunities for
people from black and minorityethnic backgrounds.(Practice example,early intervention in psychosis )
3 ProcessThis relates rst to ensuring thatservice users and carers areinvolved at an adequatelevel within programmes andprojects. Views of the processof involvement were often
positive. From the survey, 71%of the respondents felt that theirinvolvement was always or oftenvalued; only one respondent feltthat their involvement had neverbeen valued. 86% said theirinvolvement had been positivelyreceived by other members of theproject board.
Two examples show how managingthe involvement process requiresfacilitating clear, structured, tangible
activities. The early intervention forpsychosis programme included adeclaration and practice manualco-written by service users andcarers.
All 14 members of the advisoryboard were informed of all activitiesby email and invited to participate inclearly dened events such asconferences, presentations andconsultations. Members of the
advisory board discussed andcontributed to plans, proposals andprojects. They acted as advisors asopposed to decision makers; boardmembers were free to oer a widerange of responses and ideas.(Practice example, Shift)
Several chapters of the practicemanual for early intervention wereco-authored with service users andcarers. The programmeincluded regular hothouse events.These were facilitated as interactivesessions that mixed service usersand families alongside serviceprofessionals and other partners(such as local authority workers andyouth agencies).(Practice example, earlyintervention in psychosis)
Involvement processes also need tosupport service users andcarers to be involved. From thesurvey, 71% also said that they feltthey had been adequatelysupported always or often duringthe period of their involvement, theremaining 29% felt that they had
sometimes been adequatelysupported. Some service usersand carers who had been involvedin projects wanted clarication onsome aspects of the paymentprocess.
Advisors received a daily ratebased on MaRD guidelines. Boardmembers received one daytraining on negotiating andmarketing skills using role play with
a senior civil servant, and one daytraining on voice production andpublic speaking with a coach fromthe National Theatre. There wasalso the option for up to 1000worth of Continuing ProfessionalDevelopment training, including theopportunity to train as aMental Health First Aid instructor.(Practice example, Shift)
I have to ask for travel expensesand theres no payment for
attendance.(Carer)
The MaRD payment stu isnt clear,does time include travel time?(Service user)
Regarding specic emotionalsupport, half said they receivedemotional support when needed,however 29% said that they rarelyor never received this. 76% said
they always or often receivedprompt payment of fees andexpenses, however, 14% said thatthis rarely happened. Interview datapresented above suggested that
-
7/27/2019 HGBH Evaluation- UJIK
13/3111
some participants had dicultyclaiming expenses, which acted as abarrier to people becominginvolved.
4 ImpactHaving a demonstrable impacton projects and programmes isvital to service user and carerinvolvement. Survey data revealedthat 71% felt as though they wereable to have an inuence in theprojects that they were workingon, 14% gave a neutral answer,and 14% felt that they had limitedinuence. Half said they felt theirvoice was always or often heard,21% said that it was sometimesheard, 14% said that their voicewas rarely heard. Data frompractice examples suggest someways in which service users and
carers could see the impact of theproject directly.
A sub group of the advisory boardhave co-produced a series of fourDVDs that can be used as aresource for employers educationand awareness raising programme.(Practice example, Shift)
The programme was viewed byprofessionals at the NHS Institute
of Innovation and Improvement asan example of social movement.The project lead was invited to workwith the World Health OrganisationEurope & European Commission toestablish user and carerinvolvement. Service users andcarers were involved in conferencepresentations and workshops withprofessionals.(Practice example, earlyintervention in psychosis)
Data from the interviews highlightedthe importance ofdemonstrating that involvementhad had an impact. It was importantfor those involved to feel a sense ofachievement and closure.Participants highlighted a lack ofcontinuity in projects andprogrammes, and may have feltdisappointed that they had put timeand energy into projects that wereonly funded for a short period. There
was recognition by at least oneprofessional that this area neededimprovement in future:
There has been a lot ofupheavaldont know what willhappen when the projectnishes I hope the work canbe continued in another project.(Service user)
The programme came to nothing, Ifelt let down, left in limbo.(Service user)
Money has been spent by NIMHEand CSIP to train me as afacilitator and but Ive never beenused.(Carer)
The project was fantastic. Therewas a lot of work put into it byservice users but the products havenot been made widely available forsome reason. I dont know why this
decision was made.(Service user)
There are ups and downs. Wehavent got everything right, butthere is goodwill. We will continue towork with service users andcarers to get it right.(NMHDU Professional)
To some extent it may not be thatprogrammes came to nothing, but
that there was a lack of sucientfeedback mechanisms to ensurethat service users and carers wereinformed about the impact of theirinvolvement.
4.2. Service user and carerinvolvement following NIP and thePPPIThis section describes how serviceuser and carer involvement wasimplemented in NMHDU during andafter input from NIP. The PPPI
framework had been developed fullyby the time that these data werecollected.
1 Purpose To some, the initial work by NIP in
scoping involvement work inNMHDU was a good way ofbeginning to look at the purposeof involvement.
Its important to identify roles early
on. The initial NSUN report was veryuseful in kicking things o. This wasa good guide for getting going withservice user and carer involvement.(NMHDU Professional)
-
7/27/2019 HGBH Evaluation- UJIK
14/3112
Overall, service user and carerinvolvement has gone well withinNMHDU. However, this has notbeen in a traditional sense, such ashaving service users oncouncils. Our model throughout hasbeen dierent, we wanted to haveinvolvement permeating through allthe work that weve done.(NMHDU Professional)
NIP promotional events aimed toprovide opportunities for involvement amongst people withexperience of mental healthproblems, and the friends andfamily who support them. Theyaimed to expand the pool of serviceusers and carers who were involved.There was considerable positivefeedback from NIP promotionalevents. For one event, 87%
felt good or very good aboutunderstanding of the purpose oftheir involvement, and 96% feltgood or very good about beinglistened to and having their opinionvalued. Many of whom appreciatedthe opportunity to meet with others,share their views, experience andideas.
I am new to the work of NMHDUand hope to get more involved. I
have found sta to be veryapproachable and interested inmy experiences so far. This is arefreshing change from localservices.(Service user)
However, participants at theseevents said they had unclearpurpose. The language ofinvolvement may have beenconfusing or discouraging for somepeople. Perhaps more importantly,
some commented that there waslittle opportunity to follow up withinvolvement activity after the event.
It was dicult and confusing.Feeling frustrateddidnt have afeeling of what aims of the day were,what they were hoping to achieve.(Carer)
There is a need to follow uppeople after the events to
encourage them to participate.(Service user)
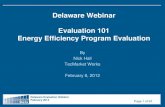
The NIP seminar in collaborationwith the Mental Health EqualitiesProgramme, and the focus groupin collaboration with Social Justiceworkstream were better received.This was because they appearedto have greater sense of purpose.Figure 1 shows the percentage ofpeople who rated the seminar andfocus group as good or very good,relating to the purpose of the eventand the quality of informationprovided. The focus group wasparticularly well received.
Figure 1: Feedback from NIPevents; seminar and focus group
Seminar
Focus Groups
Participants appreciated in thefact that they helped facilitateinformation ow betweenprofessionals and service users/carers. Many who attended feltthat they provided a learningopportunity. Participants reportedsharing experience and identifyingcommon barriers to involvement.
Ive discovered a wealth ofknowledge to take back to service
users/commissioners(Focus group feedback)
I picked up a good idea from afellow participant on an easy wayto reach out to GPs and informthem about existing involvementnetworks(Seminar feedback)
I found out about Departmentof Health policy on how it mightbe inuencing service users andcarers. Hearing from delegates ontheir frustration with services wasenlightening.(Seminar feedback)
-
7/27/2019 HGBH Evaluation- UJIK
15/3113
The relationship between thecommissioning body (NMHDU)and the consultant (NIP) waspivotal in agreeing the purpose ofinvolvement. Both organisationswere involved in co-ordinating theseminar.
Service user and carer involvementworked well during my time atNMHDU. Initially we met with NIPto identify issues that we couldwork on together. The white paperSeminar had been identied as apriority for us to work together on.The purpose was to get peoplethinking in their localities aboutwhat they could get involved in.(NMHDU Professional)
However, there was also a need toclarify the meaning of involvement
and to manage expectations, bothwithin NIP and within NMHDU:Some attendees used the day as aplatform to air their own grievances,but it was very well managed bythe chairs for the seminar and NIPfacilitators(NMHDU Professional)
There is a need to manageexpectations, I think NIP had a lot
of experience in this area and hadobviously thought a lot about it, thisshowed on the day of the WhitePaper seminar(NMHDU Professional)
2 PresenceOf the 26 people who respondedto the second survey, 19 (73%)identied themselves as havingexperienced past or presentmental distress and 15 (57%)identied themselves as being
carers. Twenty two (85%) hadheard of NSUN, 23 (86%) ofNMHDU, 19 (73%) of NIMHE andCSIP. However, only 12 (46%) hadbeen involved in NMHDU projects.The number of people involved inNMHDU programmes is shown intable 2.
WorkProgramme
NumberInvolved(n=14)
Mental HealthCommissioning
ImprovingAccess toPsychologicalTherapies
Mental HealthEqualities
SocialInclusion andSocial Justice
ImprovingMental CarePathways
PromotingWellbeing andPublic Health
Personalisation
4
3
6
4
6
7
4
Table 2: Number involved in NM-HDU programmes
Participants indicated that theyfelt diversity issues in involvementwere well covered. Gender, age,sexual orientation, disability, socialclass and race were felt to be wellrepresented in the projects. Over60% said yes in all cases. However,ensuring diverse representationof dierent groups of peoplepresented challenges.
Race and gender were wellrepresented throughout; in fact the
gender reference group had a goodethnic mix within it. Regarding age,we tried to involve people in specicprojects that older people couldrelate to, for example a project thatinvolved looking at care homes.Areas such as religion, disability andsexuality were more challenging,largely because they were newareas to our portfolio as of April lastyear.(NMHDU Professional)
NIP worked with the NMHDUstrands to try to help NMHDUinvolve service users and carersfrom a range of backgrounds. Oneexample of this arose when invitingservice users and carers to NMHDU
-
7/27/2019 HGBH Evaluation- UJIK
16/3114
seminars and focus groups. Anotherinvolved the collection of casestudies of service users for themental health strategy:
NIP ensured that we involved andinvited a good mix of service usersand carers. They had a targetedaudience of service user and carernetworks, which we reviewedtogether with NIP. We had a fairlygood representation across gender,race, age and disability.(NMHDU Professional)
We have secured a greater numberof case studies by engaging peoplein localities via a service userrun organisation facilitating thecollection. I know that people willhave been engaged sensitively andtheir needs responded to within the
process.(NMHDU Professional)
Those professionals involvedin organising the focus groupsalong with NIP echoed positivesentiments around the how serviceusers and carers were reached. Inone case, service users were giventhe deciding vote on an interviewpanel for a NMHDU tender.
It ensured that service users andcarers were involved in the processfrom beginning to the end.(Focus group feedback)
The fact that we have had anopportunity to have our viewsheard changed other peoplesperspective. I am more inspired tocontinue campaigning for change.(Focus group feedback)
The involvement of NSUN in
engaging the right group of serviceusers for this piece of work wasinvaluable(Focus group feedback)
In one case I was on the interviewpanel with two service users, sothey had the deciding vote over whowas chosen.(NMHDU Professional)This view was not always shared
across all NIP activity, particularly;the initial promotional events mayhave been more aimed at peoplewho had been involved before. The
culture of service user and carerinvolvement may have been o-putting for some who attendedthese events who had been lessinvolved in the past:
Many people already knew eachother and what it was all about.(Service user)
I was very disappointed to see theevent being chaired by white middleclass men who were leading on anumber of national projects. This isnot a reection people who work inand deliver services or the diversityof people who receive services.(Service user)
In particular, carers with full-timeemployment and people withsevere mental health problems may
nd barriers in attending. In thiscase promotional events may notalways represent the best way toinvolve people representing thesegroups:
As a working carer I am excludedfrom these events I know severalothers who are carers and do notknow about how to get involved.You dont seem to know how to ndus! How was the event advertised?
I only saw it by chance as an emailwas forwarded to me.(Carer)
The event wasnt aimed at peopleliving and going through severemental illness.(Carer)
3 ProcessMost respondents to the survey(8 out of 11) said they always oroften received documents and
information on time. However,some participants did not feel asthough they received sucientsupport in their role; three outof the 10 respondents said theyrarely or never received sucientsupervision, administrativesupport, or emotional supportthroughout the project.
The fact that we have had anopportunity to have our views
heard changed other peoplesperspective. I am more inspired tocontinue campaigning for change.(Focus group feedback)
-
7/27/2019 HGBH Evaluation- UJIK
17/3115
Regarding payment of expensesand fees, half (5/10) said theysometimes received them on time.Diculties were expressed aroundthe rates of payment for travelexpenses and the time taken forreimbursement. This needs to beaddressed in future meetings andevents.
It took me some time to nd outwhat the payment rates wereand which policy they camefromwhether they would payfor travelling time or overnightaccommodationon balance Idecided that the approach wasnot thought-through and thereforepotentially dangerous to mymental health and I decided not toparticipate. (Service user)
The cost of attending the meetingwas not met until some six weeksafter the event and then only afterseveral emails. (Service user)
There were some suggestions forfuture improvement, for example,not everyone thought that serviceuser and carers should be togetherin such events.
Im not sure if carers and service
users should be lumped together asthey have dierent agenda.(Seminar feedback)
Optimum involvement processeswere also somewhat hampered bythe external nancial environment.For example, NMHDU funding wasnite, and sta members were oftenlimited to spending up to 4,000per project. Commissions betweenNMHDU and NIP needed to twithin this budget framework:
It was dicult to work withinthe 4,000 constriction. Timeboundaries were of concern. It wassometimes dicult to balancewith NMHDU watching budgetand NIP watching the quality ofinvolvement.(Service user)
Some projects were hampered byshort tenure; from September 2010
we knew that the funding wouldno longer be available from March2011 onwards.(NMHDU Professional)
4 ImpactTwenty of the 26 surveyrespondents (77%) had beento a NIP promotional event. Themajority (15 out of 20 - 75%) saidthat these events were good orvery good. However, the majority(15 out of 20) also said that theyhad not been involved in nationalmental health projects sinceattending the event, and halfsaid they had not signicantlyinuenced to be more involvedin NMHDU projects (9 out of 18,50%), although some (6 out of 18,33%) said that it had inuencedthem signicantly. All but one (20out of 21 - 95%) intended to beinvolved in NMHDU projects in thefuture.
Service users and carers valued
the opportunity to contributeto discussions at seminars andfocus groups. This is an exampleof a tangible impact which canbe felt immediately by those whohad been involved, particularlyfor professionals who could learndirectly from service users andcarers about pertinent issues.
I thought my involvement wasneeded to ensure that the service
user view is incorporated intodesigning and shaping services(Focus group feedback)
The fact that we have had anopportunity to have our viewsheard changed other peoplesperspectives. I am more inspired tocontinue campaigning for change.(Focus group feedback)
The perspective of carers as expertpartners, we live in communities
and need support networks andthat carers are integral to mentalhealth services.(Seminar feedback)
The importance of feedback toservice users and carers to showimpact cannot be underestimated.
This experience will be moremeaningful if we get feedback aboutwhat dierence our ideas have
made which hopefully will happenas part of this process. (Seminarfeedback)
-
7/27/2019 HGBH Evaluation- UJIK
18/3116
At the white paper event, serviceusers and carers were invitedto give feedback. This workedwell, and would denitely dothis more extensively if doingsomething similar in the future.Feedback is good practice becauseotherwise service users andcarers involvement can feel a bittokenistic.(NMHDU Professional)
Professionals viewed NIP as apositive step for service userand carer involvement, andprofessionals expressed interest inusing the Partnership in their work.There were some positive viewstowards the Purpose, Presence,Process, Impact (PPPI) frameworkfor involvement, although it mayneed some more testing in practice
before it is wholly applicable:
The workshops were very dynamicand useful. We want NIP to get upa source of service user and carerreference groups across the workstream. I think all the issues of thePPPI model are relevant and its agood ideabut I have found it abit problematic would need tobe working full time to get all theinformation neededdidnt have
time to start lling it all out.(NMHDU Professional)
There is a future for this kind ofwork and involvementa powerfuldyad of professional and carer canchange practice.(NMHDU Professional)
It has added a whole newdimension to involvementallowsservice users and carers to be muchmore integratedthey are integral
to the work, and are the sta ratherthan just being on the periphery.(NMHDU Professional)
One of the aims of NMHDU and NIPwas to leave a legacy of service userand carer involvement work withinmental health. The co-operation ofthe two organisations was seen asessential for this to happen, possiblyfor logistical and continuity reasonssuch as stang.
NIP has a vital role in making sureNMHDU leaves a legacy. This isbecause lots of NIP people have
worked with NMHDU. NMHDUprovides a springboard for NIPwork, not only in funding but alsotrough human resources and skills.(Service user)
Id say that our legacy was in beingbrave about exposing what we do;making involvement demonstrable.It wasnt perfect, and we haventachieved everything we wantedto achieve, but some things didchange as a consequence of thework. (Professional)
Part of this legacy lies in developingcapacity for service user andcarer involvement work outside ofNMHDU, in the wider sense. If thishappens in the long term, then it willbe a signicant impact of NMHDUservice user and carer involvement:
One of the reasons we did theevent jointly with NIP was to assistNIP in developing a platform withservice user networks on issuesaround the white paper andequalities. I hope that NIP can usethis when planning future actions.(NMHDU Professional)
-
7/27/2019 HGBH Evaluation- UJIK
19/3117
Summary of ndingsThe ndings of this report serve tohighlight the practicalities, benetsand diculties of involving serviceusers and carers in national policyand practice work, whether it wasfor NMHDU, CSIP or NIMHE. ThePPPI model was used to providea framework for assessing thesuccess of service user and carerinvolvement. Results indicatethat the four domains of purpose,presence, process and impactwere being implemented acrossthe lifespan of the NIP to varyingdegrees.
Clarity of purpose is needed in orderto ensure meaningful involvement.This evaluation indicates that peoplewere well briefed about purpose inNMHDU (including NIMHE and CSIP)
work. NIP and some of the NMHDUprojects appeared to meet to discusspurpose at the outset. Projects andcommissions such as the focusgroups and seminars appeared tohave a clear purpose, but initial NIPpromotional events fared less well,which made have made it dicultto capitalise on contacts gained. Acommon purpose of involvementwas information sharing, particularlyin cases when service users and
carers could interact directly withprofessionals, such as in seminars orevents. Purpose needs to be set at areasonable level as to be achievablewithin the circumstances. Within this,NMHDU and NIP aimed to manageexpectations about the purpose ofinvolvement.
Ensuring a diverse, representationalpresence within projects andprogrammes was challenging toboth NMHDU and NIP. Prior to NIP,
representation was limited to aminority of service users and carers.Others may have been discouragedor alienated by use of jargonterminology, service users with moresevere and present mental ill healthfound it dicult to be involved, as didsome carers. NIP itself had dicultyaddressing diversity, and their initialpromotional events were criticisedon these grounds. Ensuring diversityfor involvement across the dierent
strands within NMHDU provedchallenging, but there was positivefeedback about how NIP had workedto ensure representation from adiverse spread of people. NIP alsosucceeded in engaging a greater
05Discussion
number of service users and carersthat had not before been involved.
It appeared that there were someexamples of appropriate process inNMHDU prior to NIP, such as serviceusers and carers co-authoringdocuments and acting as valuedadvisors. However, there was roomfor improvement in supporting peopleto be involved, such as payment offees and expenses and in providingemotional support where necessary.There also appeared to be somediscrepancy between NMHDU andNIP about the level of service user andcarer involvement that was expected.This was no doubt hindered bypressure from the external nancialenvironment.
Showing impact of involvement
work is important. One way in whichthis can be improved is in receivingfeedback, and it is here in which itlinks with the process of involvement.Before NIP, there was evidencethat feedback was happening insome projects, but that changingcircumstances with projects andprogrammes led to upheaval whichmade it dicult. Similarly, people whoattended NIP events wanted somedirection on how they could follow up
their interest. When service users andcarers were shown the impact of theirwork, then the results were positive,as shown in joint information sharingevents for professionals, service usersand carers. In the longer term, thelasting impact of service user andcarer involvement in NMHDU remainsto be seen. Much will depend uponthe capacity of NIP to capitalise onthe legacy of NMHDU. The work withNMHDU provides a platform fromwhich NIP can develop and expand its
remit.
Strengths and limitations of theevaluationThis is evaluation used a mixtureof methods to collect data andcorroborate ndings. This wasdeemed particularly important totriangulate information and checkfor inconsistencies. For example,participants may be positive aboutinvolvement when asked in a survey
but revealed more negative views ininterviews.
There are a number of weaknesseswith the study design however, suchas the small sample size. It should be
-
7/27/2019 HGBH Evaluation- UJIK
20/3118
noted that the study sample includeda majority of white British femaleswho were over the age of 45. Thelack of people responding to surveyswho were from BME communitiesis also a concern and could be saidto represent the lack of diversity inservice user involvement projects persee. Data collected from feedbackforms and case studies also lack thetransparency of that which is collectedthrough questionnaire and interviewmethods.Implications for the futureThere have been positive andnegative practices in the serviceuser and carer involvement work ofNMHDU (and NIMHE/CSIP). NMHDUand NIP have worked togetherto attempt to improve this. Thetwo organisations have worked
on several specic projects andcommissions. The NIP work hasbeen successful in developing aframework by which to appraiseinvolvement, and has succeededin running a number of serviceuser and carer events which haveembodied elements of goodpractice. However, there are somehurdles yet to be overcome, forexample, ensuring that people fromall groups (including carers and
people with severe mental illnesses)can be represented.
NIP itself needs to orientate within thenew external political environment. Itneeds to identify strengths and to beable to communicate them to otherswho may not be immediately familiarwith the concept of service user andcarer involvement. Both NIP andNMHDU have a wealth of informationabout how to involve service usersand carers, including key learning
points from projects they have workedon in the past. It remains to be seenhow the work of NIP will be valuedwithin the new health commissioningframework. The new HealthWatchprojects may be ideal places for NIPto promote service user and carerinvolvement. Local HealthWatch willbe interlinked with GP Consortia, whowill decide whether to commissionservices from organisations such asNIP.
NIP has an established track recordof working with NMHDU. Many of thesta involved in NIP have also beeninvolved in NMHDU projects prior tothis. NIP therefore has the expertise to
develop, and to establish its identityand unique selling points. NMHDUcan be credited if NIP manages tobecome a self-sucient organisationrepresenting service user and carerinvolvement. Time will tell whether thiswill happen.
Recommendations- What is the purpose of
involvement? Organisationsseeking to involve service usersand carers should consult withservice user led organisations(such as NIP) to agree the reasonwhy involvement is needed.
- The culture and language ofservice user and carer involvementshould be understandable withinthe context of everyday life, notjust within the context of policy
and practice. This will:
- Facilitate the presence of a morediverse range of service usersand carers within the network.
- Help NIP to build links witha more diverse range ofstatutory, voluntary and privateorganisations.
- Processes should be in place
for service users and carers tomove from being interestedin involvement to becomingactive participants. Follow upfor participants after initialengagement is essential in orderto maintain interest.
- Continuity needs to be embeddedinto the culture of service user andcarer involvement. Therefore, uponcompletion of projects, NIP canhelp signpost those involved other
opportunities and projects.
- Practical and emotional supportshould be available to help peoplebecome involved. NIP coulddevelop mentoring schemes;those who have been involved inthe past could support others tobecome involved.
- Organisations that wish to involveservice users and carers should
provide feedback to those whohave been involved NIP couldcollate and disseminate feedback,providing participants withinformation about project impact.
-
7/27/2019 HGBH Evaluation- UJIK
21/3119
06References
Crepaz-Keay, D. (2008). About theNational Survivor User Network, OpenMind, 149, 8-9.
Department of Health. (2010). Equityand excellence: Liberating the NHS.London: DH.
Faulkner, A. (2010). Service User andCarer Involvement inThe National Mental HealthDevelopment Unit, On behalf of theNSUN Partnership.
NIMHE / CSIP. (2007). Making a RealDierence, Strengthening ServiceUser and Carer Involvement in NIMHE.
Read, J (ed) (2001) Something InsideSo Strong, Mental Health FoundationPublications.
SPSS [computer program]. Version 16.Chicago (IL): SPSS Inc.; 2007
-
7/27/2019 HGBH Evaluation- UJIK
22/3120
07Appendices
1 Selection of NIP work activity within NMHDU until December 2010
Activity Quality/Evidence ofImpact
Timescale
Collation of 30 casestudies- Advertising- Responding to
enquiries
- Collating casestudies- Selecting and
formatting casestudies
- Diverse response- Detailed information- Support oered and
provided- Feedback
Phase 1Sep Oct 2010Phase 2Nov - Dec 2010
20 days
Recruitment andsupport of Liaison andDiversion focus groups- Advertising- Responding to
enquiries
- Diverse response- Detailed information- Support oered and
provided- Feedback
16/17 Sep 2010
12 days
Initial commentson extracts of newcommissioning guide- Good practice
examples foraccessiblecommissioning guide
- Focused response- Fast access tofeedback
13 - 24 Sept 20101 day
1 day seminar for 40delegates from the NIPnetwork- Understanding and
planning for the newpolicy environment- Proposed regional
events (see below)
- Diverse response- Detailed information- Support oered and
provided
- Feedback- Dissemination model
Sep 10 Mar 2011
5 days
Collation of 20 Yes/No/Yes But responses intoa Venn Diagram- Collated comments
from NIP networkabout proposedguiding principles
of new draft mentalhealth strategy
- Diverse response- Detailed information- Focused response- Fast access to
feedback- Dissemination model
Oct Nov 2010
4 days
-
7/27/2019 HGBH Evaluation- UJIK
23/3121
2 Service user and carer surveyPart A Service user and carerinvolvement in mental healthpolicy
Please mark answers with an Xinside the appropriate boxes unlessotherwise stated
1 Do you consider yourself to be auser of mental health services, pastor present?
oYesoNo
2 Do you consider yourself to be acarer of someone with mental healthproblems, past or present?
oYesoNo
3 Have you heard of the followingorganisations?
oNational Mental HealthDevelopment Unit (NMHDU)oNational Mental Health
Development Unit (NMHDU)oCare Services in Partnership
(CSIP)
4 Have you ever been involved inhelping to change Governmentpolicy for mental health?
oYesoNo
5 In what way have you beeninvolved? (Please describe)
6 To what extent do you feel thatyour involvement in mental healthpolicy has been valued?
oA oO oS oR oN
7 Was the purpose of yourinvolvement in mental health policymade clear by the policy makingorganisation?
oYesoNo
8 Have you been involved in any ofthe following work programmes?(Please mark any that apply)
oMental Health CommissioningoIAPToMental Health EqualitiesoPromoting Social Inclusion and
Social Justice
oImproving Mental Health CarePathwaysoPromoting Wellbeing and Public
Mental HealthoPersonalisation in Mental Health
9 Which mental health policyprojects have you been involved in?(Please describe)
To what extent do you agree with thefollowing two statements:
10 I am able to inuence mentalhealth policy
oSA oA oNE oD oSD
11 I have been accurately informedof how much inuence I may haveon mental health policy
oSA oA oNE oD oSD
12 Was your role in mental healthpolicy clearly explained by theproject lead?
oYesoNo
13 Have you attended nationalmeetings for mental health policyprojects?
oYesoNo
14 Have you felt adequatelysupported in your involvement withmental health policy? (Please markone)
oA oO oS oR oN
15 Between service users andcarers, who do you feel is mostinvolved in mental health policy?
oSU oC oND
Key
AOSRN
AlwaysOftenSometimesRarelyNever
SAA
NEDSD
Strongly AgreeAgree
NeutralDisagreeStrongly Disagree
SUCND
Service UsersCarersNo Dierences
-
7/27/2019 HGBH Evaluation- UJIK
24/3122
16 Has your involvement beenpositively received by others workingon the project?
oA oO oS oR oN
17 Did you feel that your voice isbeing heard by mental health policymakers?
oA oO oS oR oN
18 If you needed emotional supportat any time during your involvement,was this provided?
oA oO oS oR oN
19 Are you provided with clear
information in order to support yourinvolvement?
oA oO oS oR oN
20 Did you receive promptpayment of expenses/fees for yourinvolvement?
oA oO oS oR oN
21 Did you receive feedback aboutthe impact your involvement hashad on mental health policy?
oA oO oS oR oN
22 How are you made aware ofhow new government mental healthpolicies might aect you? (pleasedescribe)
23 What do you feel that you havegained from becoming involvedin mental health policy making?(please describe)
Part B Demographic information
24 Age
o
-
7/27/2019 HGBH Evaluation- UJIK
25/3123
3 Professionals survey
1 What job do you do? Are youemployed by NMHDU?
1a What is your experience ofinvolving service users/ carers in thework that you do?
1b Are you aware of any policiesthat your organisation has aboutthis?
1c Which work stream(s) are youinvolved with?
1d How many service users /carersare involved in the work stream(s)?SU Co oMental Health Commissioningo oIAPTo oMental Health Equalitieso oPromoting Social Inclusion and
Social Justiceo oImproving Mental Health Care
Pathways
o oPromoting Wellbeing andPublic Mental Health
o oPersonalisation in MentalHealth
1e How do you ensure that serviceusers and carers feel that theirinvolvement is valued?
2 How do you enable service usersand carers to oversee the work ofNMHDU?
2a How would you aim to increasethe number of service users andcarers involved?
2b Do you enable service users andcarers to give their perspective atnational programme boards?
2c Is service user and carerinvolvement part of the inductionpackage for new sta?
2d To what extent are serviceusers and carers made aware of thelimitations of their inuence?
2e Do you oer training for existingsta to facilitate service user and
carer involvement?
3 How do you monitor and evaluateservice user and carer involvement?
4 Do you provide emotional supportfor service users and carers whenneeded?
oA oO oS oR oN
Key
SUC
Service UsersCarers
AOSRN
AlwaysOftenSometimesRarelyNever
-
7/27/2019 HGBH Evaluation- UJIK
26/3124
5 Do you provide a role descriptionfor service users and carers at thebeginning of their involvement?
oA oO oS oR oN
6 Do service users and carers haveaccess to clear information in a
variety of formats?oA oO oS oR oN
7 Do service users and carersreceive prompt payment ofexpenses/fees?
oA oO oS oR oN
8 Do you involve service users andcarers from marginalised groups?
oA oO oS oR oN
9 Do you give service users andcarers feedback about the eecttheir involvement has had?
10 How are service users and carersmade aware of how new policiesmight aect them?
11 What benets do you thinkinvolving service users has to oer?
12 What benets do you thinkinvolving carers has to oer?
13 Are there any other comments
you would like to make?
14 Can I just ask you a fewdemographic questions please?
15 Age
___ years
16 Gender
oMaleoFemale
26 Ethnicity
WhiteoBritishoIrish
Asian/AsianBritishoIndianoPakistanioBangladeshi
Black/BlackBritishoCaribbeanoAfrican
MixedoWhite and Black caribbeanoWhite and Black AfricanoWhite and Asian
Chinese/Other Ethnic GroupoChineseoOther
18 Is English your rst language?
oYesoNo
Key
AOSRN
AlwaysOftenSometimesRarelyNever
-
7/27/2019 HGBH Evaluation- UJIK
27/3125
4 Service user and carer surveyPart A Service user and carerinvolvement in mental healthpolicy
Please mark answers with an Xinside the appropriate boxes unlessotherwise stated
1 Do you consider yourself to have
experienced mental distress past orpresent?
oYesoNo
2 Do you consider yourself to befamily/carer of someone with mentalhealth problems, past or present?
oYesoNo
3 Have you heard of the followingorganisations?
oNational Survivor User Network(NSUN)oNational Mental Health
Development Unit (NMHDU)oNational Mental Health
Development Unit (NMHDU)oCare Services in Partnership
(CSIP)
4 Have you been involved in anyNMHDU projects?
oYesoNo
If you answered yes to Question4 please go to Question 5. If youanswered no please go to Question21.
5 Have you been involved in any ofthe following work programmes?(Please mark any that apply)
oMental Health CommissioningoIAPToMental Health EqualitiesoPromoting Social Inclusion and
Social JusticeoImproving Mental Health Care
PathwaysoPromoting Wellbeing and Public
Mental Health
oPersonalisation in Mental Health
If you ticked any of the above pleasedescribe your role:
6 Was your role in the project/smade clear?
oA oO oS oR oN
7 Have you been involved in thedirection of the project/s? (Forexample, member of steeringgroup?)
oA oO oS oR oN
8 Have you been involved inreviewing the project/s? (Forexample, consultations/proofreading?)
oA oO oS oR oN
9 Are you involved in stangdecisions for the project/s? (Forexample, sitting on a recruitmentpanel?)
oA oO oS oR oN
10 Do you feel the project/s reectsa diversity of:
GenderoYesoNo oDont Know
RaceoYesoNo oDont Know
Sexual OrientationoYesoNo oDont Know
AgeoYesoNo oDont Know
FaithoYesoNo oDont Know
DisabilityoYesoNo oDont Know
Social ClassoYesoNo oDont Know
11 Do you receive meetingdocuments on time?
oA oO oS oR oN
12 Do you receive sucientinformation about the aims of theproject/s?
oA oO oS oR oN
13 Do you receive sucientsupervision in your role/s?
oA oO oS oR oN
Key
AOSRN
AlwaysOftenSometimesRarelyNever
-
7/27/2019 HGBH Evaluation- UJIK
28/3126
14 Do you receive sucientadministrative support in yourrole/s?
oA oO oS oR oN
15 Do you receive sucientemotional support in your role/s?
oA oO oS oR oN
16 Do you receive sucient trainingfor your role/s?
oA oO oS oR oN
17 Do you receive prompt paymentof expenses/fees?
oA oO oS oR oN
18 Do you receive feedback aboutyour involvement in the project/s?
oA oO oS oR oN
19 Have you been given theopportunity to present the project/sto a wider audience?
oA oO oS oR oN
20 Please use the space below forfurther comments:
21 Have you attended any NMHDUInvolvement Partnership events?
oYesoNo
If you answered yes to Question21 please go to Question 22. If youanswered no please go to Question28.
22 How have you found the NMHDUInvolvement Partnership events?
oVG oG oNE oP oVP
23 Have you been involvedin any national mental healthprojects since attending a NMHDUInvolvement Partnership event?
oYesoNo
24 To what extent has a NMHDUInvolvement Partnership eventinuenced your involvement innational mental health project/s?
oALOoQA oNE oAL oNAL
25 What do you consider to be themain challenges of service user andcarer involvement in NMHDU?
26 To what extent has a NMHDUInvolvement Partnership eventidentied some of these challenges?
oT oM oNE oAB oNAL
27 Do you intend to be involved inany national mental health projectsin the future (e.g, for NMHDU)?
oYesoNo
Part B Demographic information
28 Age
o
-
7/27/2019 HGBH Evaluation- UJIK
29/3127
5 Professionals survey
1 What is your job title? Are youemployed by NMHDU/NSUN?
2 Which work stream(s) are youinvolved with?
3 How many service users /carersare involved in the work stream(s)?
SU Co oMental Health Commissioning
o oIAPTo oMental Health Equalitieso oPromoting Social Inclusion and
Social Justiceo oImproving Mental Health Care
Pathwayso oPromoting Wellbeing and
Public Mental Healtho oPersonalisation in Mental
Health
4 How do you involve SU/C in yourwork?
5 Are you aware of any policiesyour organisation has about SU/Cinvolvement?
6 Have you attended any NMHDUPartnership Involvement events?
oYesoNo
7 If yes, how helpful have you foundtheir meetings?
oV oQ oIN oNV oNAL
8 Are they relevant to your work?
oYesoNo
9 How much potential do youbelieve the NMHDU InvolvementPartnership has to recruit serviceusers and carers?
oALO oQAL oNM oNNE
Please comment:
10 How would you use theNMHDU Involvement Partnershipin your work? (Would you considerusing their knowledge/expertise/database?)
11 Have you heard of the PPPI(Purpose, Presence, Process,Impact) framework for SU/Cinvolvement?
12 How useful do you think thisframework is??
oV oQ oIN oNV oNAL
13 Is the role of SU/C in theprogramme made clear?
oA oO oS oR oN
14 Are SU/C involved in thedirection of the programme? (Forexample, member of steering
group?)oA oO oS oR oN
15 Are SU/C involved in thereviewing of the project/prog?(For example, consultations/proofreading?)
oA oO oS oR oN
16 Are SU/C involved in stangdecisions for the project/prog? (Forexample, sitting on a recruitmentpanel?)
oA oO oS oR oN
Key
SUC
Service UsersCarers
VQINNVNAL
VeryQuiteIndierentNot VeryNot At All
ALOQALNMNNE
A LotQuite A LotNot MuchNone
AOSRN
AlwaysOftenSometimesRarelyNever
-
7/27/2019 HGBH Evaluation- UJIK
30/3128
17 Do you feel the project reects adiversity of:
Gender
oYesoNo oDont Know
Race
oYesoNo oDont Know
Sexual Orientation
oYesoNo oDont Know
Age
oYesoNo oDont Know
Faith
oYesoNo oDont Know
Disability
oYesoNo oDont Know
Social Class
oYesoNo oDont Know
18 Do SU/C receive meetingdocuments on time?
oA oO oS oR oN
19 Do SU/C receive sucientinformation about the aims of theprogramme?
oA oO oS oR oN
20 Do SU/C receive sucientsupervision in their role?
oA oO oS oR oN
21 Do SU/C receive sucientadministrative support in their role?
oA oO oS oR oN
22 Do SU/C receive sucientemotional support in their role?
oA oO oS oR oN
23 Do SU/C receive sucienttraining for their role?
oA oO oS oR oN
24 Do SU/C receive prompt
payment of expenses/fees?
oA oO oS oR oN
25 Do SU/C receive feedback abouttheir involvement in the programme?
oA oO oS oR oN
26 Are SU/C given the opportunityto present the project to a wideraudience?
oA oO oS oR oNPart B Demographic information
27 Age
o
-
7/27/2019 HGBH Evaluation- UJIK
31/31
changing
Mental Health Foundation
Sea Containers House20 Upper GroundLondon SE1 9QBUnited Kingdom
Telephone
020 7803 1100Fax020 7803 1111
Registered Charity No.England 801130Scotland SC039714