
HFOV HIGH FREQUENCY OSCILLATORY VENTILATION BECKY VARELA & JAMIE WOOD.
21
HFOV HIGH FREQUENCY OSCILLATORY VENTILATION BECKY VARELA & JAMIE WOOD
-
Upload
elaina-alvarez -
Category
Documents
-
view
370 -
download
2
Transcript of HFOV HIGH FREQUENCY OSCILLATORY VENTILATION BECKY VARELA & JAMIE WOOD.
HFOVHIGH FREQUENCY OSCILLATORY VENTILATION
BECKY VARELA & JAMIE WOOD
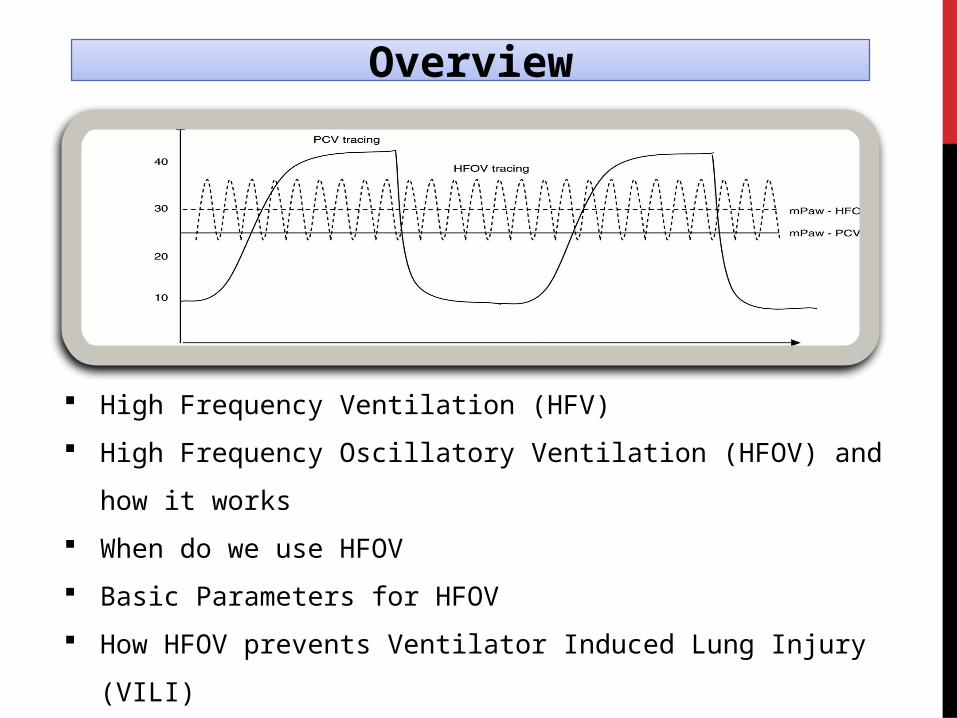
High Frequency Ventilation (HFV)
High Frequency Oscillatory Ventilation (HFOV) and how it works
When do we use HFOV
Basic Parameters for HFOV
How HFOV prevents Ventilator Induced Lung Injury (VILI)
Overview
High Frequency Ventilation
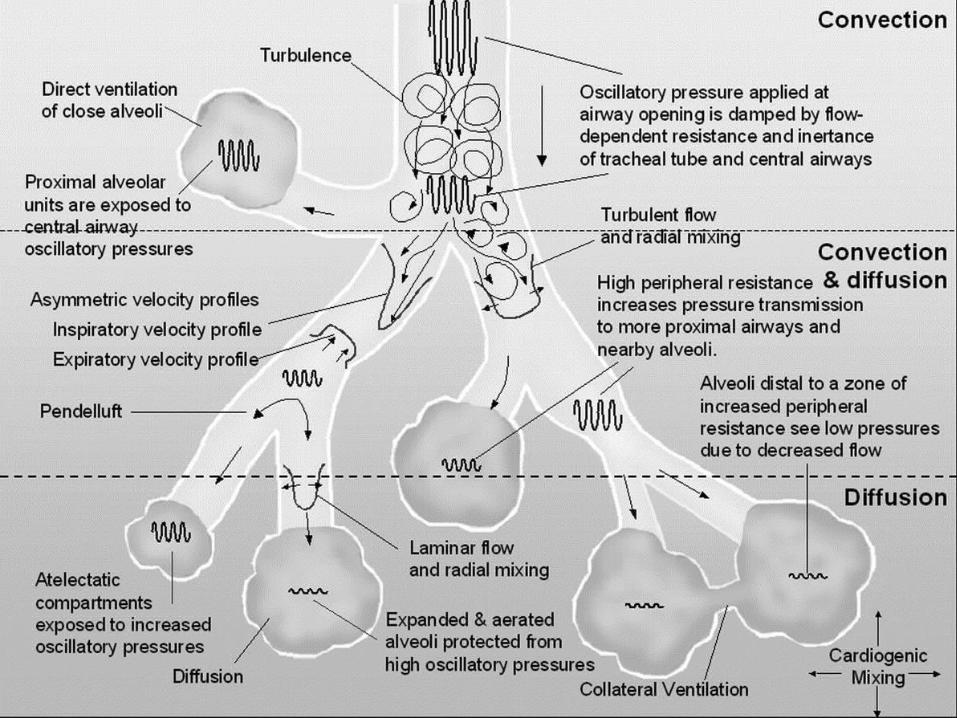
Provides augmented gas distributionBy means of numerous gas transport mechanisms.
Convection, transit time, direct ventilation Pendalluft effect Taylor dispersion Asymmetric velocity Cardiogenic Mixing Molecular diffusion Collateral Ventilation
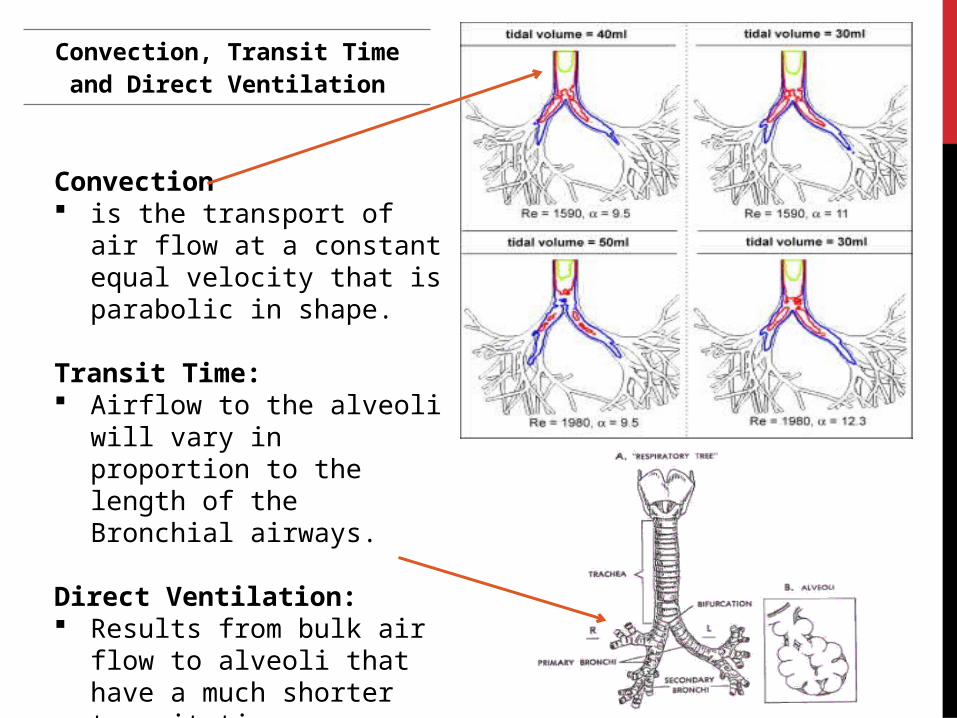
Convection, Transit Time and Direct Ventilation
Convection is the transport of air flow at a
constant equal velocity that is parabolic in shape.
Transit Time: Airflow to the alveoli will vary
in proportion to the length of the Bronchial airways.
Direct Ventilation: Results from bulk air flow to
alveoli that have a much shorter transit time.
Taylor DispersionPendalluft Effect
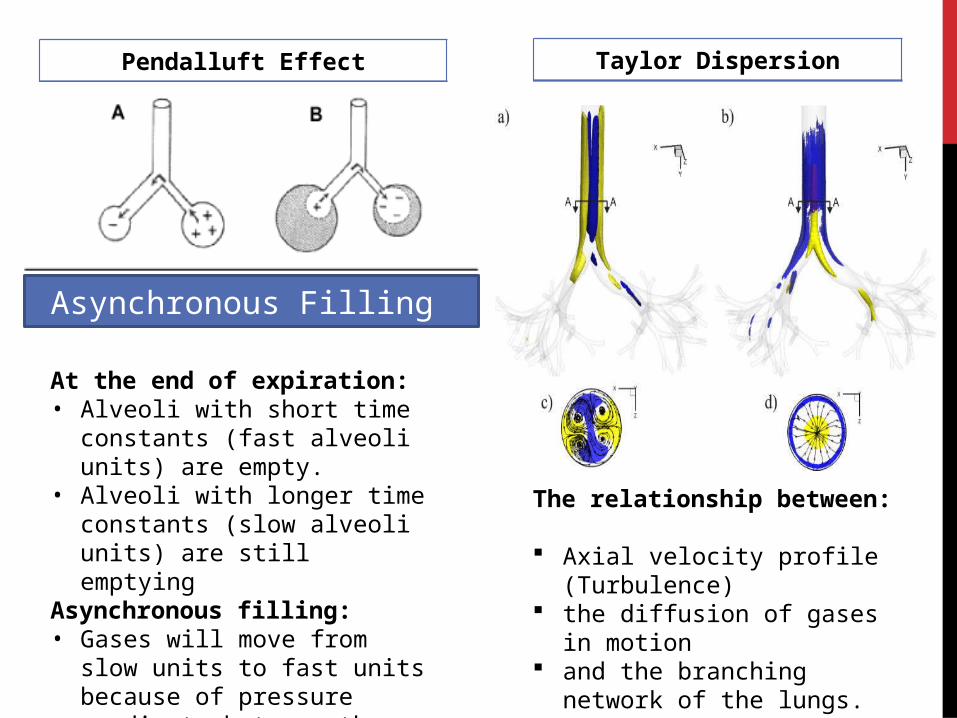
At the end of expiration:• Alveoli with short time constants
(fast alveoli units) are empty. • Alveoli with longer time constants
(slow alveoli units) are still emptying
Asynchronous filling:• Gases will move from slow units
to fast units because of pressure gradients between the alveoli.
Asynchronous Filling
The relationship between:
Axial velocity profile (Turbulence) the diffusion of gases in motion and the branching network of the
lungs.
Asymmetry Cardiogenic Mixing
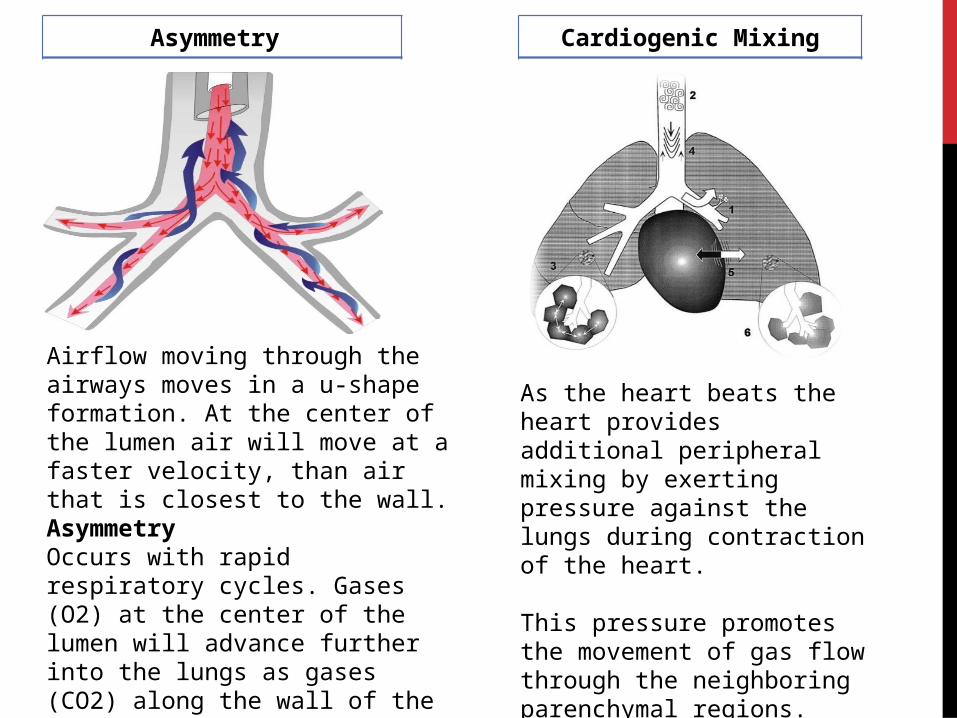
Airflow moving through the airways moves in a u-shape formation. At the center of the lumen air will move at a faster velocity, than air that is closest to the wall.AsymmetryOccurs with rapid respiratory cycles. Gases (O2) at the center of the lumen will advance further into the lungs as gases (CO2) along the wall of the airway moves out towards the mouth.
As the heart beats the heart provides additional peripheral mixing by exerting pressure against the lungs during contraction of the heart.
This pressure promotes the movement of gas flow through the neighboring parenchymal regions.
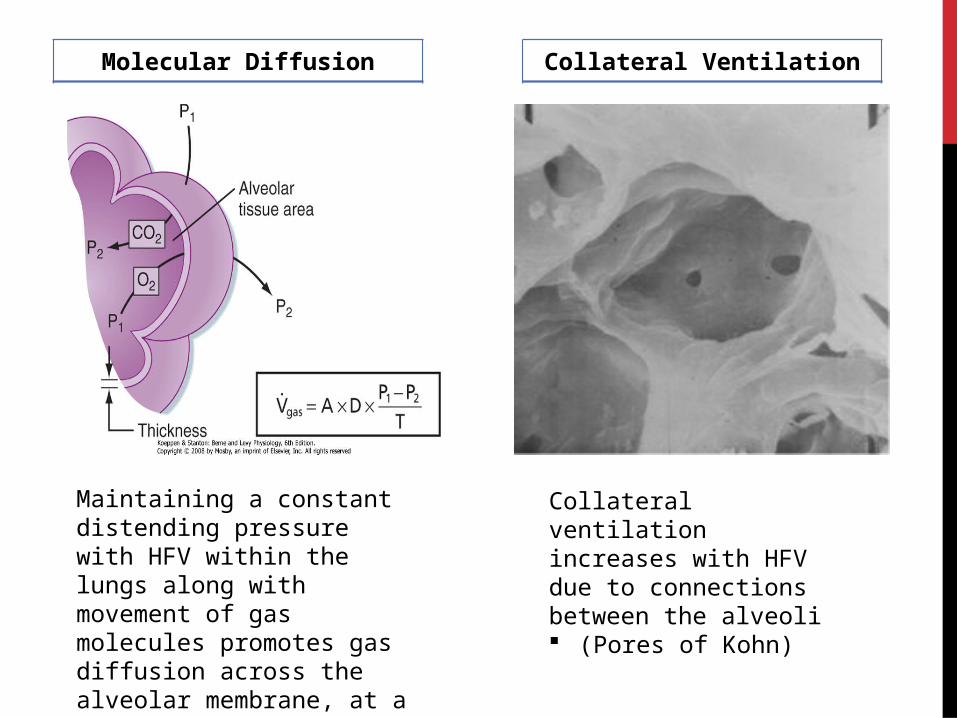
Collateral VentilationMolecular Diffusion
Maintaining a constant distending pressure with HFV within the lungs along with movement of gas molecules promotes gas diffusion across the alveolar membrane, at a faster rate.
Collateral ventilation increases with HFV due to connections between the alveoli (Pores of Kohn)
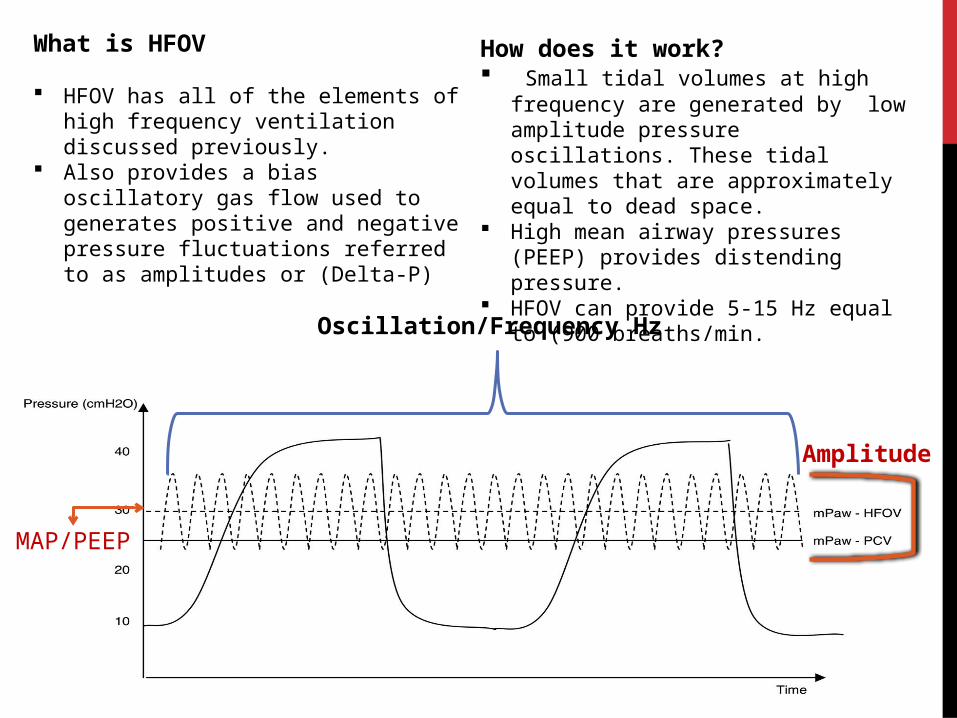
How does it work? Small tidal volumes at high frequency are
generated by low amplitude pressure oscillations. These tidal volumes that are approximately equal to dead space.
High mean airway pressures (PEEP) provides distending pressure.
HFOV can provide 5-15 Hz equal to (900 breaths/min.
What is HFOV
HFOV has all of the elements of high frequency ventilation discussed previously.
Also provides a bias oscillatory gas flow used to generates positive and negative pressure fluctuations referred to as amplitudes or (Delta-P)
Amplitude
Oscillation/Frequency Hz
MAP/PEEP
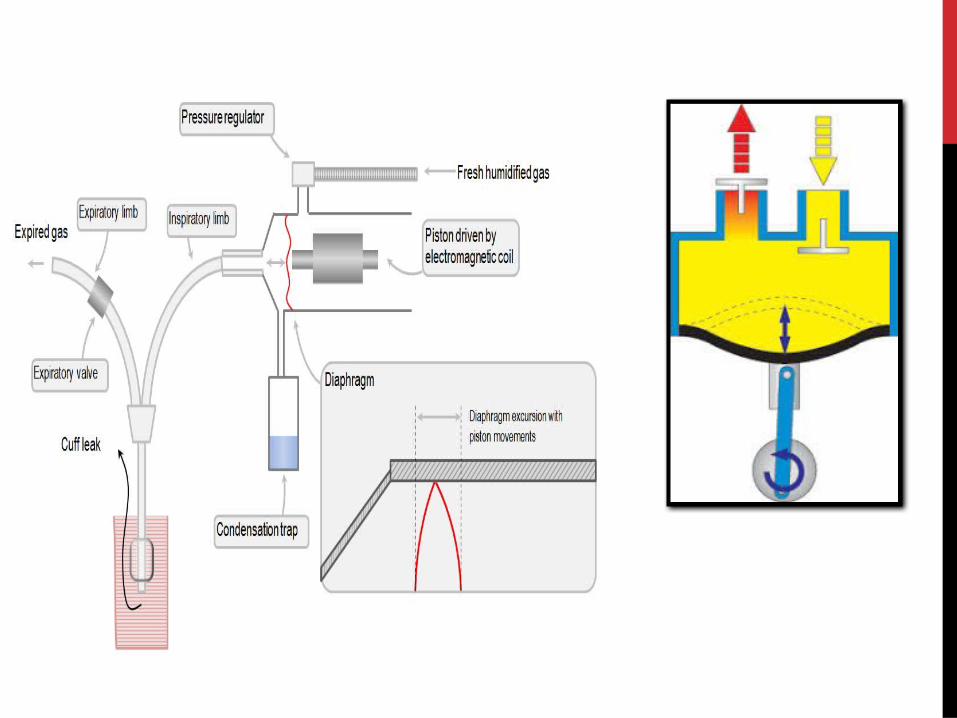
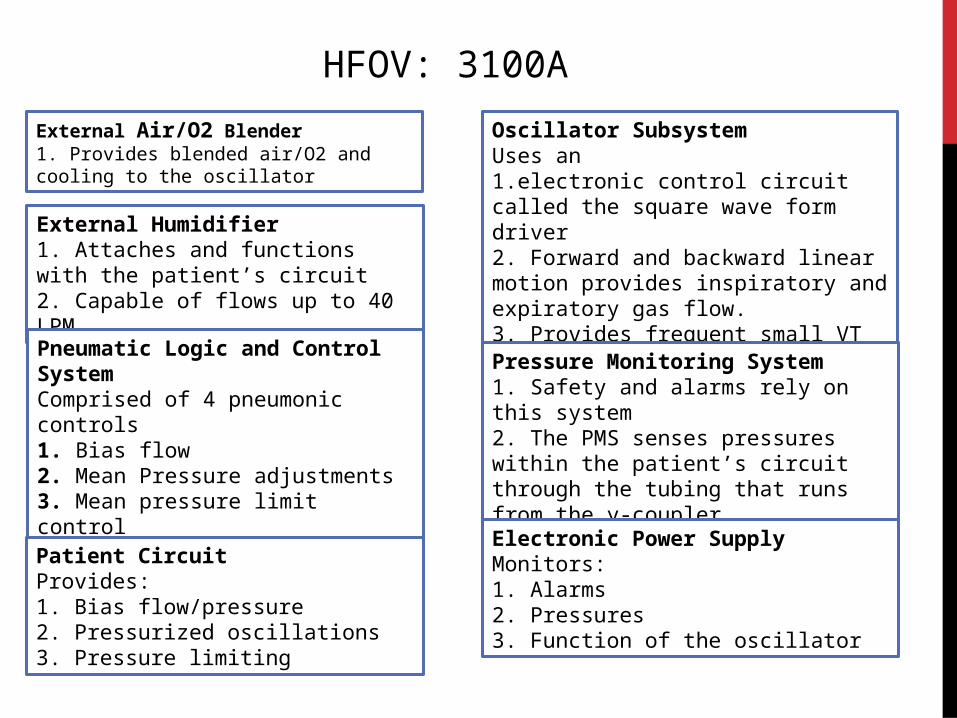
External Air/O2 Blender1. Provides blended air/O2 and cooling to the oscillator
External Humidifier1. Attaches and functions with the patient’s circuit2. Capable of flows up to 40 LPM
Pneumatic Logic and Control SystemComprised of 4 pneumonic controls1. Bias flow2. Mean Pressure adjustments3. Mean pressure limit control4. Patient circuit calibration adjustment
Patient CircuitProvides:1. Bias flow/pressure2. Pressurized oscillations3. Pressure limiting
Oscillator SubsystemUses an 1.electronic control circuit called the square wave form driver2. Forward and backward linear motion provides inspiratory and expiratory gas flow.3. Provides frequent small VT in HZ
Pressure Monitoring System1. Safety and alarms rely on this system2. The PMS senses pressures within the patient’s circuit through the tubing that runs from the y-coupler
Electronic Power SupplyMonitors:1. Alarms2. Pressures3. Function of the oscillator
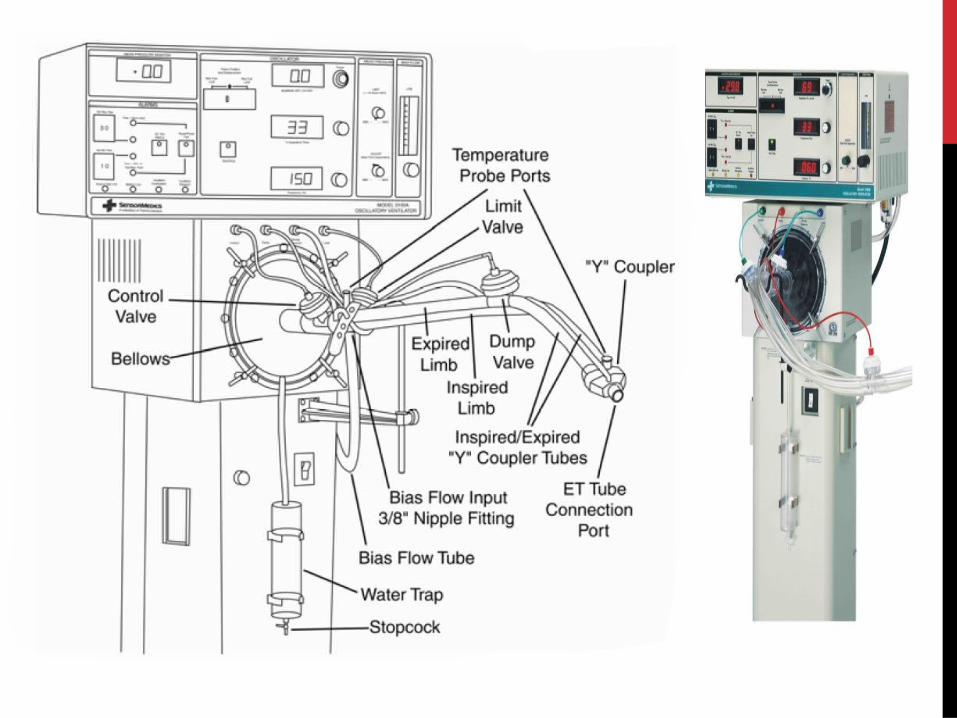
HFOV: 3100A
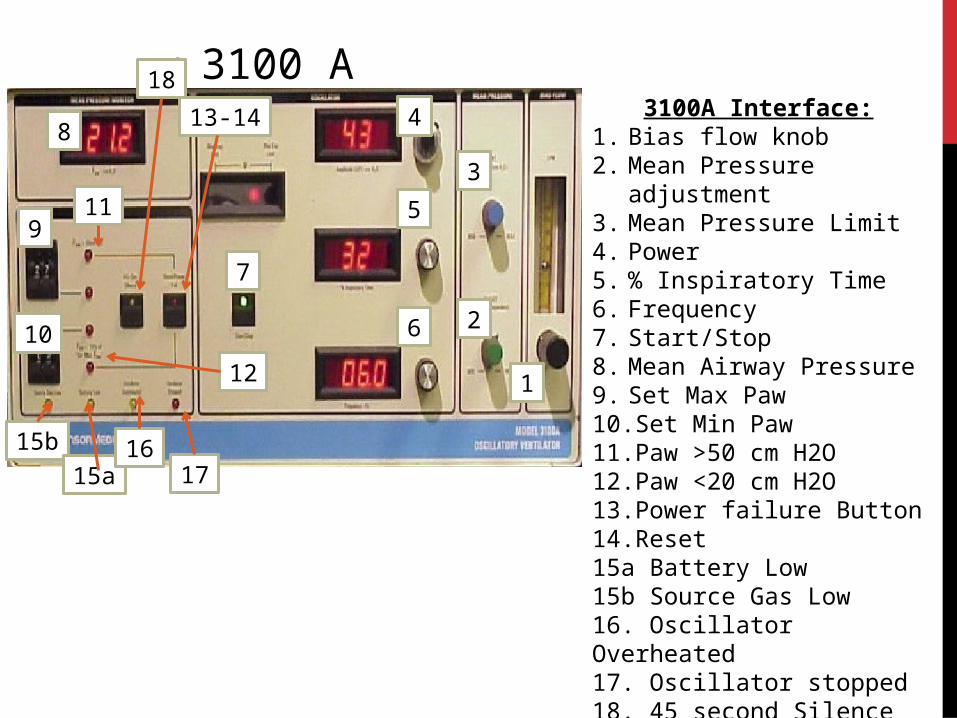
• 3100 A3100A Interface:
1. Bias flow knob2. Mean Pressure adjustment3. Mean Pressure Limit4. Power5. % Inspiratory Time6. Frequency7. Start/Stop8. Mean Airway Pressure9. Set Max Paw10.Set Min Paw11. Paw >50 cm H2O12.Paw <20 cm H2O13.Power failure Button14.Reset15a Battery Low15b Source Gas Low16. Oscillator Overheated17. Oscillator stopped18. 45 second Silence
4
2
3
5
6
1
7
8
9
10
15b
15a16
17
13-14
11
12
18
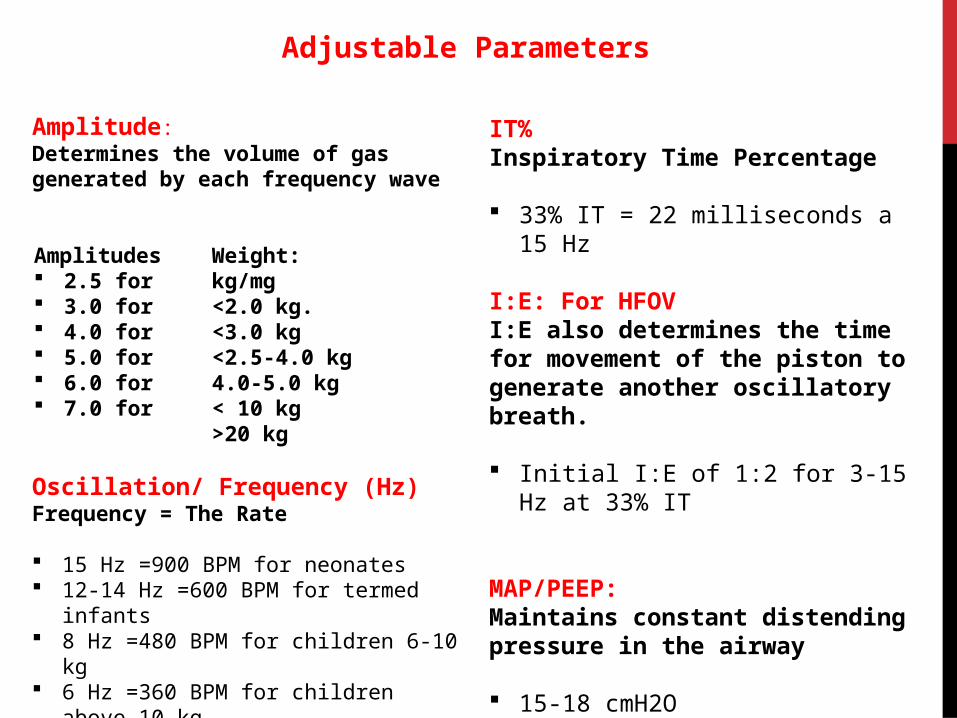
Amplitude: Determines the volume of gas generated by each frequency wave
Oscillation/ Frequency (Hz)Frequency = The Rate
15 Hz =900 BPM for neonates 12-14 Hz =600 BPM for termed infants 8 Hz =480 BPM for children 6-10 kg 6 Hz =360 BPM for children above 10 kg
Amplitudes 2.5 for 3.0 for 4.0 for 5.0 for 6.0 for 7.0 for
Weight: kg/mg<2.0 kg.<3.0 kg<2.5-4.0 kg4.0-5.0 kg< 10 kg>20 kg
IT%Inspiratory Time Percentage
33% IT = 22 milliseconds a 15 Hz
I:E: For HFOVI:E also determines the time for movement of the piston to generate another oscillatory breath.
Initial I:E of 1:2 for 3-15 Hz at 33% IT
MAP/PEEP:Maintains constant distending pressure in the airway
15-18 cmH2O
Adjustable Parameters
PULMONARY DISEASES AND DISORDERS TREATED WITH
HFOV
https://www.youtube.com/watch?v=dHuXtoODHuA
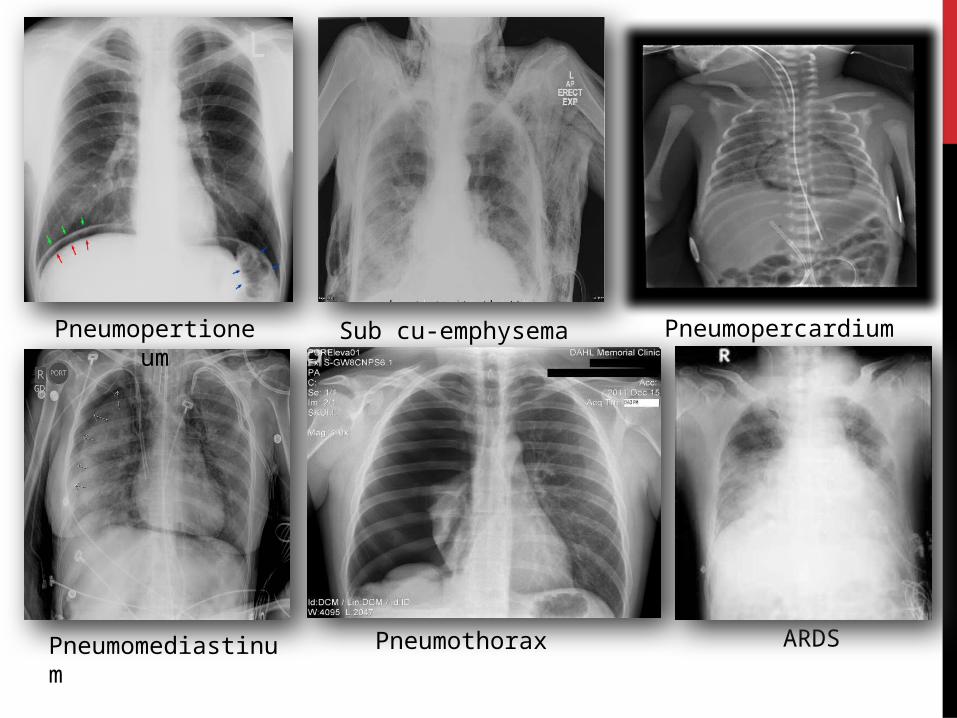
Pneumopertioneum Sub cu-emphysema Pneumopercardium
Pneumomediastinum Pneumothorax ARDS
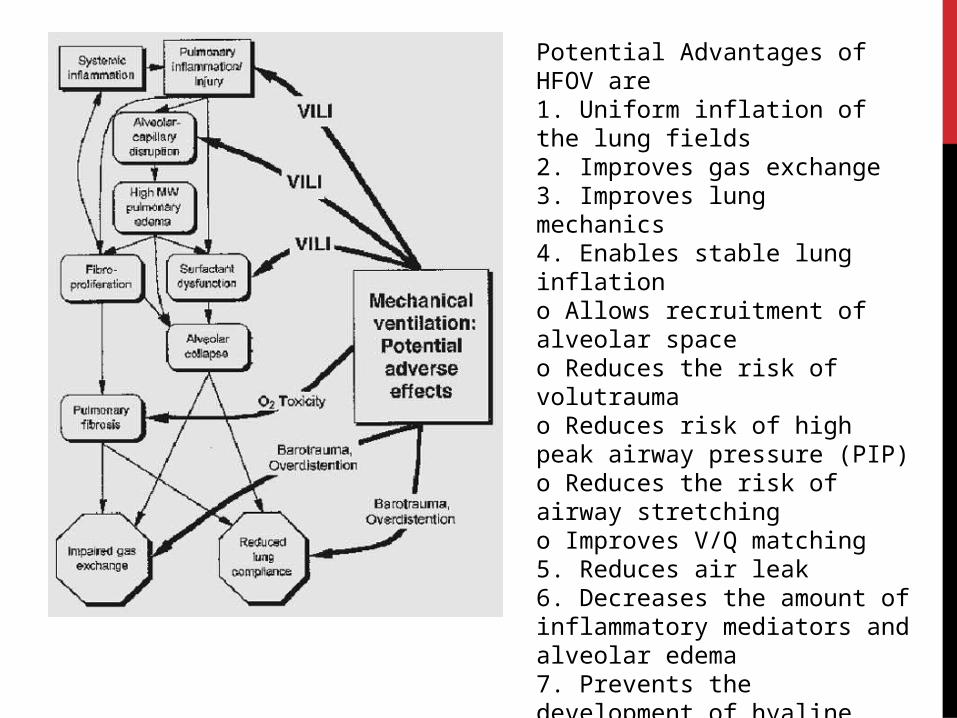
Potential Advantages of HFOV are 1. Uniform inflation of the lung fields2. Improves gas exchange 3. Improves lung mechanics 4. Enables stable lung inflationo Allows recruitment of alveolar spaceo Reduces the risk of volutrauma o Reduces risk of high peak airway pressure (PIP)o Reduces the risk of airway stretchingo Improves V/Q matching5. Reduces air leak 6. Decreases the amount of inflammatory mediators and alveolar edema7. Prevents the development of hyaline membrane disease (HMD)
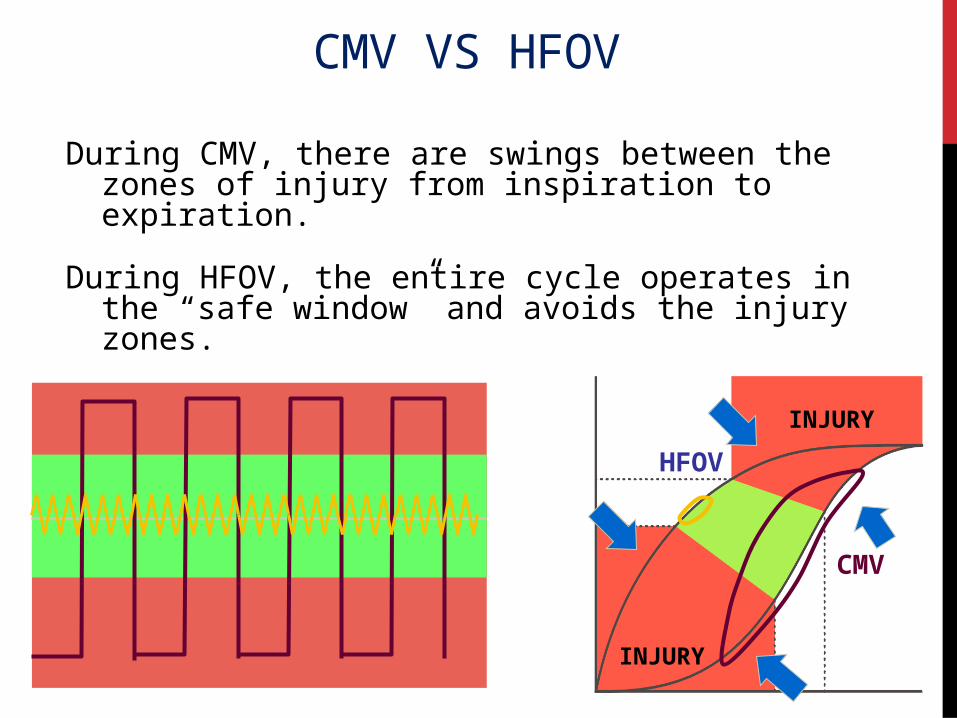
During CMV, there are swings between the zones of injury from inspiration to expiration.
During HFOV, the entire cycle operates in the “safe window” and avoids the injury zones.
CMV
HFOV
INJURY
INJURY
CMV VS HFOV
Volume
Pressure
Zone of Overdistention
Safe window
Zone of Derecruitment and atelectasis
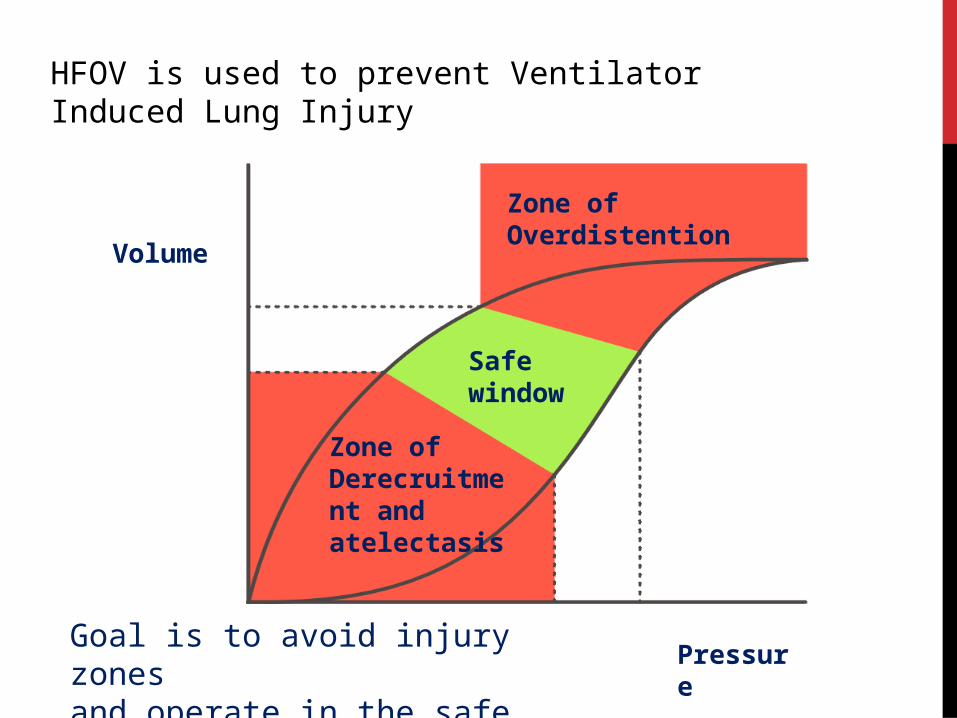
Goal is to avoid injury zones and operate in the safe window
HFOV is used to prevent Ventilator Induced Lung Injury
Indications:
• When traditional ventilation fails
• Airleak syndromes
• For patients with severely low lung compliance
• Refractory hypoxemia
Contraindications:
• ICP
• obstructive lung disease
• increased airway resistance (small endotracheal tube)
• asthma
• secretions
• increased physiological dead space
Work Citations Page:
Alves, Amanda. “High Frequency Oscillatory Ventilation HFOV; a new strategy in the Treatment of patients with Acute Respiratory Distress Syndrome and low lung compliance.” CIMC 2000. Web 13 August 2014.
Birch, Pita. “Newborn Services Clinical Guideline High Frequency Oscillatory Ventilation.” Web. 14 August 2014. http://www.adhb.govt.nz/newborn/guidelines/respiratory/hfov/hfov.htm
CareFusion; “3100A High frequency oscillatory ventilation; Operator’s manual.” CareFusion Corporation. 222745 Savi Ranch Parkway Yorba Linda, CA 92887-4668. Web 18 August 2014
Haines, Mike. “Mechanical Ventilation: High Frequency Ventilation.” Respiratory Therapy Files. http://www.respiratorytherapyfiles.net Web. 8 August 2014.
Jeng, Mei-Jy. Lee, Chen, Soong. “Neonatal air leak syndrome and the role of high-frequency ventilation.” Sci Verse Science Direct Journal of the Chinese Medical Association 75 (2012) 551e559 Web. 8 August 2014. http://homepage.vghtpe.gov.tw/~jcma/75/11/551.pdf
Prost, Allen. “High Frequency Oscillation Ventillation.avi.” Youtube.com. 2011. Web 24 Aug. 2014.
Slee-Wijffels1, Fieke YAM. RM van der Vaart, Twisk, Markhorst, Plötz5 “High-frequency oscillatory ventilation in children: a single-center experience of 53 cases, pp. R274” Open Access. 16 Web August 2104. http://www.biomedcentral.com/content/pdf/cc3520.pdf
Slee-Wijffels1, Fieke YAM. RM van der Vaart, Twisk, Markhorst, Plötz5 “High-frequency oscillatory ventilation in children: a single-center experience of 53 cases, pp. R274” Open Access. 16 Web August 2104. http://www.biomedcentral.com/content/pdf/cc3520.pdf


















