
Herve Reychler Oral imaging in Implantology
32
Oral imaging in oral implantology H. Reychler
-
Upload
luc-vrielinck -
Category
Documents
-
view
231 -
download
2
description
Oral imaging in oral H. Reychler Medical imaging -without X-rays -with X-rays -principles -radioprotection -digitalisation -tomography -orthopantomogram -CT scan -Denta scan -ConeBeamCT -3D and related devices Principles of X-rays –Preop planning –Immediate postop control –Not accurate for measurements –Information on healing !! X-rays
Transcript of Herve Reychler Oral imaging in Implantology

Oral imaging in oral
implantology
H. Reychler
Medical imaging
- without X-rays
- with X-rays
- principles
- radioprotection
- digitalisation
- tomography
- orthopantomogram
- CT scan
- Denta scan
- ConeBeamCT
- 3D and related devices

Principles of X-rays
-To visualise, after or during radiation, hard tissues
- no accessible to clinical exam
- no accessible otherwise
- some geometrical rules and constraints
- during radiation
- position of the patient
- enlargement of the images
- immobility of the patient
- some limits
- projection
- superimposition
- morphological details without informations on physiopathology
Ballinger PW. Merrill's Atlas of Radiographic Positions and Radiologic Procedures. St Louis, Mosby, 1986 - Goaz
PW & White SC. Oral Radiology : Principles and Interpretation. St Louis, Mosby, 1987 - Langland OE et al.
Textbook of Dental Radiology. Springfield, Ill, Thomas, 1984 - Mailland M. Techniques de radiologie dentaire.
Paris, Masson, 1987 - Manson-Hing LR. Fundamentals of Dental Radiography. Philadelphia, Lea & Febiger, 1985
- Pasler FA. Zahnärztliche Radiologie. Stuttgart, Thieme, 1987

- Retroalveolar– Preop planning
– Immediate postop control
– Not accurate for measurements
– Information on healing !!
X-rays

– Quality of bone
Classification of Lekholm & Zarb (1985).
Implants survival rates depend on bone quality :
Class I : almost exclusively compact homogenous bone
Class II : thick compact bone around dense trabecular spongious bone
Class III : thin cortical bone around dense trabecular spongious bone
Class IV : thin cortical bone around dense spongious bone
Symphyseal bone
of edentulous patient
Symphyseal +
mandibular bone
Maxillary bone
Limits of X-rays
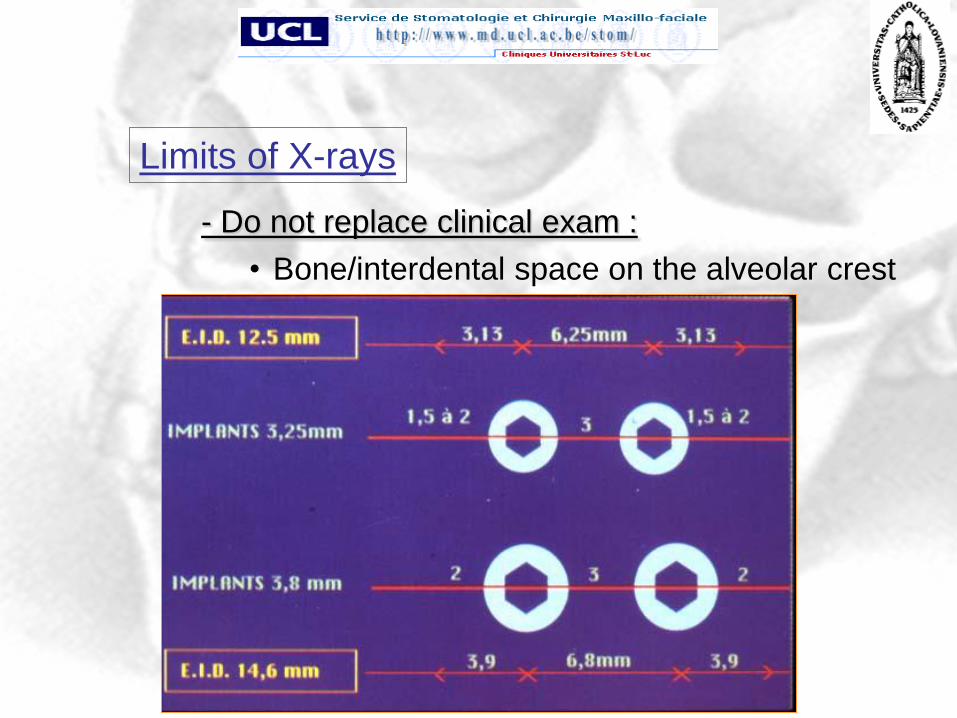
- Do not replace clinical exam :
• Bone/interdental space on the alveolar crest
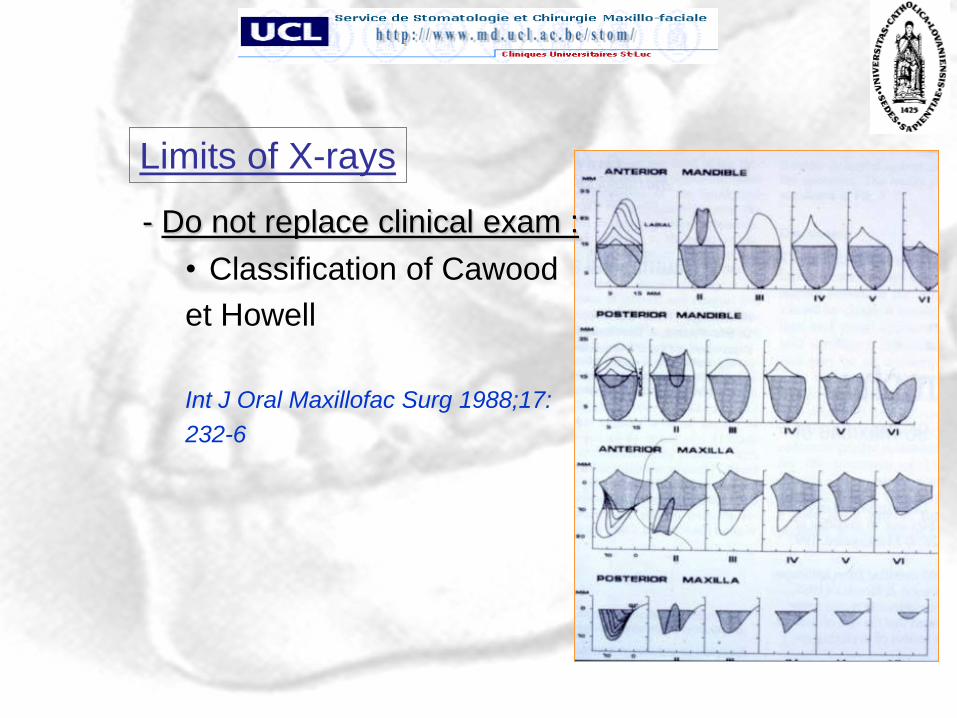
Limits of X-rays

- Do not replace clinical exam :
• Alveolar crest thickness
Limits of X-rays

Height :
- screwed prosthesis : 5 mm
- sealed prosthesis : 7,5 mm
- Bona : 12, 5 mm
- Bar : 18,5 mm
Limits of X-rays
- Do not replace clinical exam :– Vertical intermaxillary space/dimension
- Do not replace clinical exam :
• Classification of Cawood
et Howell
Int J Oral Maxillofac Surg 1988;17:
232-6
Limits of X-rays

Radioprotection
- « As Low As Reasonably Achievable » principle
- To choose the most performant technique to visualise what you want,
with the lowest radiation dosis
- Mean dosis due to dental X-rays = 0.37 mSv/year/ Belgian patient
- = « only » 10 % of total radiation dosis (3.5 mSv/year)
- « Optimisation principle » means X-rays only acceptable if not any
other diagnostic tool is possible and taking into account radiation dosis
>< image quality
http://ec.europa.eu/energy/nuclear/radioprotection/publication/136en.htm - http://www.fanc.fgov.be -

Radioprotection

Digitalisation
- To modify an analogic signal/image to a digital one
- 2 different techniques :
- direct = sensors : CCD (photoelectric effect) ou CMOS (semiconductive agents)
- indirect = phosphor plates : PSPP + laser scanning
- Advantages :
- speed
- radiation dosis lowering
- computerisation
- « user-friendly » with patient, with colleagues ..
- Disadvantages :
- cost
- some hard- and software aspects
Alcaraz M et al, Dentomaxillofac Radiol, 2009 - Wakoh M et al, Bull Tokyo Dent Coll, 2001

CCD
CMOS
PSPP
X-rays
Scanner
Laser
= DIRECT
= INDIRECT
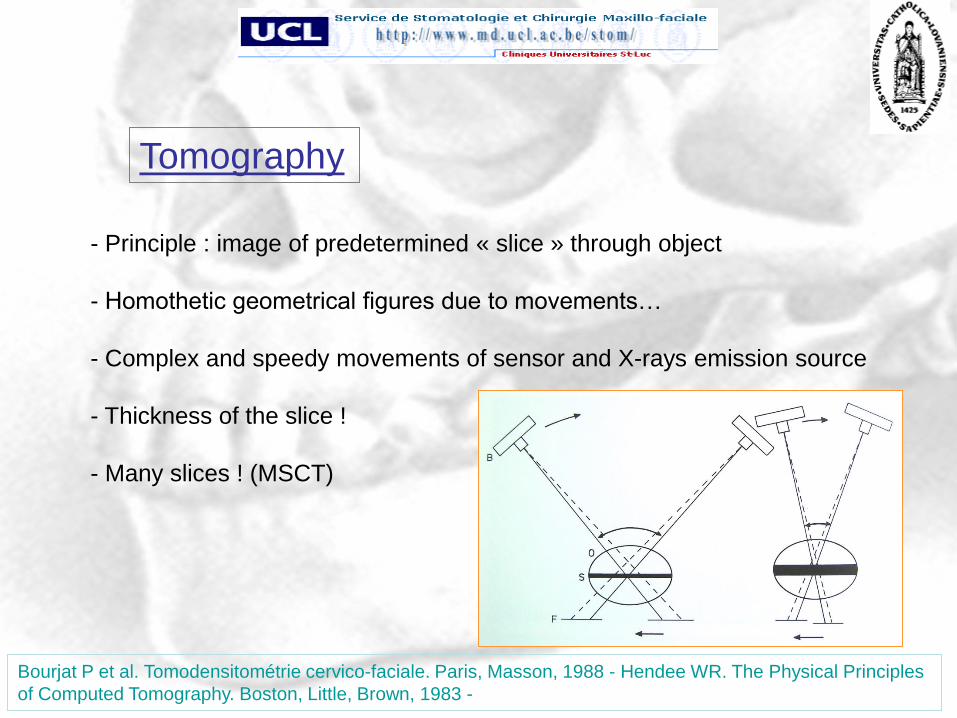
Tomography
- Principle : image of predetermined « slice » through object
- Homothetic geometrical figures due to movements…
- Complex and speedy movements of sensor and X-rays emission source
- Thickness of the slice !
- Many slices ! (MSCT)
Bourjat P et al. Tomodensitométrie cervico-faciale. Paris, Masson, 1988 - Hendee WR. The Physical Principles
of Computed Tomography. Boston, Little, Brown, 1983 -

Orthopantomogram
- Tomography adapted to the form and shape
of dental arches and adjacent tissues
- Enlargement and deformations
- Indicated as overview, must be completed
by other techniques (retroalveolar, TeleX-ray …)
Chomenko AG. Atlas of Maxillofacial Pantomographic Interpretation. Chicago, Quintessence, 1985 - Jung T.
Panorama-Röntgenographie. Heidelberg, Hüthig, 1984 - Langland OE et al. Principles and Practice of
Panoramic Radiology. Philadelphia, Saunders, 1982

Orthopantomogram
- some devices allow for 3D imaging but
only for limited areas

CT scan
- Digitalisation
- Millimetric slice thickness
- High radiation dosis (MSCT!)
- « Windows » (hard and soft tissues)
- « 3D » diagnosis may be difficult


Denta scan
- CT scan applied to dental arches and
adjacent tissues
- Images are reconstructed !
- Same limits as CT scan ones



– Anatomical pitfalls


Cone Beam CT
- CT scan principle, but
- radiation dosis is limited (10 to 30 lower than CT scan, but = 2 OPG!)
- radiation time is short : 20 to 30 seconds !
- volumetric tomography (FOV 4x4, 8x8 or 15x15 cm)
- conic beam, no slices as for MSCT
- Not any diagnostic information on soft tissues
- Patient is seated or standing
- 2D images are reconstructed in a 3D data set using algorithm
- Images may be combined to laser optical clinical view
- Images of high resolution : voxel size in mm3
- Images may be integrated in 3D images analysis software
- Most evidence-based technique
- USA : 35 % of CBCT are indicated for implantology, Am Assoc Oral &
Maxillofac Radiol recommends it for planning dental implants
De Vos W et al, Int J Oral Maxillofac Surg, 2009 – Horner K et al, Dentomaxillofac Radiol, 2009

Cone Beam CT
- Not recommended as a routine imaging technique for all implant cases
- Accuracy of measurements : error of 3 to 8 % (0,5 on 10 mm)!
- Accuracy of measurements : error of max 4 °
- But if many in-vitro studies, very few in-vivo …..
- Quality of bone : corelated to implant stability !
- Reliability of implant placement > flapless surgery (98,4 % fit of surgical
template)
- Allows for surgical navigation, surgical guide, 3D imaging
- volumetric evaluation
- 3D planning (implant axis…)
- augmentation surgery before implanting
Nickenig H-J et al, J Cranimaxillofac Surg, 2007 - Naitoh M et al, Int J Oral Maxillofac Implants, 2009 – Rugani
P et al, Int J Comput Dent, 2009 - Song Y et al, Int J Oral Maxillofac Implants, 2009 -
…/…

Cone Beam CT
- Anatomical pitfalls :
- maxillary sinus
- mandibular canal (bifid in 65 % of patients !)
- retromolar canal (in 25 % of patients !)
- mental foramina
- mandibular incisive canal
- nasal floor
- nasopalatine canal
- cortical perforations
- (TMJ)
Dreiseidler T et al, Int J Oral Maxillofac Implants, 2009 - Leitlinie der DGZMK, DZZ, 2009 -

3D Imaging
- Do not confuse 2D images of 3D structures and real 3D images and models
- Seems tricky…but errors :
- human / application / imaging / technical / registration errors
- Reliability of implant placement > flapless surgery (98,4 % fit of surgical
template)
- In real time = navigation (tracking system) : very reliable but necessitates
hard- and software : 1,5 mm / 4°
- But is essential in implantology
- to avoid some anatomical pitfalls
- to accurately plan implantation, taking care of
- constraints and occlusal aims
- constraints and esthetic aims
- anatomical aspects (bone principally)
Parel S et al, J Oral Maxillofac Surg, 2004 – Nickenig H-J et al, J Craniomaxillofac Surg, 2007 – Chen X et al,
Int J Med Robot, 2008 – Xiaojun C et al, Comput Methods Programs Biomed, 2009 – Widmann G et al, Oral
Surg Oral Med Oral Pathol Oral Radiol Endod, 2009 -

– Bony volume
– Bony structure
– Insertion axis
– Implants diameter
– Anatomical pitfalls (zygoma !)
– Accuracy of images
– Transfer to peroperative :
• 3D model
• 3D splint
• References ??
– …/…
3D Imaging

3D Imaging

- On models
Surgical guides

Surgical guides
– Computerized
Nickenig H-J et al, J Craniomaxillofac Surg, 2007 – Ersoy AE et al, J Periodontol, 2008 -

Surgical guides
– Computerized
- flapless surgery
- accuracy : 1,5 mm / 5°
Jabero M et al, Implant Dent, 2006 - Nickenig H-J et al, J Craniomaxillofac Surg, 2007 – Ersoy AE et al, J
Periodontol, 2008 -


















