
Electronic Resource Notebook - Broadcasting Students listed here.

Dear Author,
Here are the electronic proofs of your article.
• You can submit your corrections online or by fax. Together with your proof corrections youmust return the Copyright Transfer Statement to complete the proof process.
• Print out the proof. (If you do not already have Acrobat Reader, just download it from http://www.adobe.com.)
• Check the metadata sheet to make sure that the header information, especially author namesand the corresponding affiliations, are correctly shown.
• Check that the text is complete and that all figures, tables and their legends are included. Alsocheck the accuracy of special characters, equations, and electronic supplementary material ifapplicable. If necessary refer to the Edited manuscript.
• The publication of inaccurate data such as dosages and units can have serious consequences.Please take particular care that all such details are correct.
• Please do not make changes that involve only matters of style. We have generally introducedforms that follow the journal’s style. Substantial changes in content, e.g., new results,corrected values, title and authorship are not allowed without the approval of the responsibleeditor. In such a case, please contact the Editorial Office and return his/her consent togetherwith the proof.
• For online submission please insert your corrections in the online correction form. Alwaysindicate the line number to which the correction refers.
• For fax submission, please ensure that your corrections are clearly legible. Use a fine blackpen and write the correction in the margin, not too close to the edge of the page.
• The cover sheets (including the Copyright Transfer Statement and the Offprint Order Form)can either be scanned and sent electronically or sent by fax.
• If we do not receive your corrections within 48 hours, we will send you a reminder.
Please noteYour article will be published Online First approximately one week after receipt of your correctedproofs. This is the official first publication citable with the DOI. Further changes are, therefore,not possible.After online publication, subscribers (personal/institutional) to this journal will have access to thecomplete article via the DOI using the URL: http://dx.doi.org/[DOI].If you would like to know when your article has been published online, take advantage of our freealert service. For registration and further information go to: http://www.springerlink.com.Due to the electronic nature of the procedure, the manuscript and the original figures will only bereturned to you on special request. When you return your corrections, please inform us if you wouldlike to have these documents returned.The printed version will follow in a forthcoming issue.

Fax to: +91 7305880700 or +91 44 4208 9498From: Springer Correction Team
6&7, 5th Street, Radhakrishnan Salai, Chennai, Tamil Nadu, India – 600004Re: Modern Rheumatology DOI:10.1007/s10165-012-0775-x
Successful treatment of rectal ulcers in a patient with systemic lupus erythematosus usingcorticosteroids and tacrolimus
Authors: Shinjiro Kaieda · Teppei Kobayasi · Mariko Moroki · Seiyo Honda · Kentaro Yuge · HiroshiKawano · Keiichi Mitsuyama · Michio Sata · Hiroaki Ida · Tomoaki Hoshino · Takaaki Fukuda
I. Permission to publishDear Springer Correction Team,I have checked the proofs of my article andq I have no corrections. The article is ready to be published without changes.
q I have a few corrections. I am enclosing the following pages:q I have made many corrections. Enclosed is the complete article.
II. Offprint orderq Offprint order enclosed q I do not wish to order offprintsRemarks:
Date / signature ______________________________________________________________________________
III. Copyright Transfer Statement (sign only if not submitted previously)The copyright to this article is transferred to Japan College of Rheumatology (for U.S. government employees: to theextent transferable) effective if and when the article is accepted for publication. The author warrants that his/hercontribution is original and that he/she has full power to make this grant. The author signs for and accepts responsibilityfor releasing this material on behalf of any and all co-authors. The copyright transfer covers the exclusive right toreproduce and distribute the article, including reprints, translations, photographic reproductions, microform,electronic form (offline, online) or any other reproductions of similar nature.
An author may self-archive an author-created version of his/her article on his/her own website and or in his/herinstitutional repository. He/she may also deposit this version on his/her funder’s or funder’s designated repository atthe funder’s request or as a result of a legal obligation, provided it is not made publicly available until 12 monthsafter official publication. He/she may not use the publisher's PDF version, which is posted on http://www.springerlink.com, for the purpose of self-archiving or deposit. Furthermore, the author may only post his/herversion provided acknowledgement is given to the original source of publication and a link is inserted to the publishedarticle on Springer's website. The link must be accompanied by the following text: "The original publication isavailable at http://www.springerlink.com".
The author is requested to use the appropriate DOI for the article (go to the Linking Options in the article, then toOpenURL and use the link with the DOI). Articles disseminated via http://www.springerlink.com are indexed,abstracted and referenced by many abstracting and information services, bibliographic networks, subscriptionagencies, library networks, and consortia.
After submission of this agreement signed by the corresponding author, changes of authorship or in the order ofthe authors listed will not be accepted by Springer.
Date / Author’s signature ______________________________________________________________________

Offprint Order FormModern RheumatologyDOI: 10.1007/s10165-012-0775-x
Offprints are available from Springerat prices listed in the table belowprovided the order is received withthe corrected proofs.
n Ship offprints to:Name of individual Name of institution
Address
Tel.: Fax: e-mail:
n Purchaseq Privateq Official Official purchase number: : q A number will follow later
n Send invoice to: q Same as below q Same as aboveName
Address
Tel.: Fax: e-mail:
Payment in Japanese Yen only:q I remit payment to the bank account of Springer Japan.
(The account number can be found on the invoice)q Please charge my credit card:q AMERICAN EXPRESS q DINERS CLUB q MASTERCARD q VISA
Card number Expiration date
Cardholder’s name
Date Author’s signature
Please check a box to indicate the numberof copies required.
Offprint prices in Japanese Yen, including postage and handling.(Authors living in Japan will be charged consumption tax in addition.)
For orders involving more than 20 pagesor more than 500 copies, please ask forquotations.
Copies 1-4pp 5-8pp 9-12pp 13-16pp 17-20ppq 50 24,200 28,000 31,900 35,700 39,600q 100 28,600 33,000 37,400 41,800 46,200q 200 37,400 43,000 48,400 53,900 59,400q 300 46,200 52,800 59,400 66,000 72,600q 400 55,000 63,000 70,400 78,100 85,800q 500 63,800 72,600 81,400 90,200 99,000
If this order form is not returned, wewill assume that you do not wish toorder offprints.
Offprints ordered after themanuscripts have gone to press can beproduced only if 300 or more are tobe supplied as costs are thensubstantially higher.
Please do not pay for offprints beforereceipt of an invoice from SpringerJapan.
For further inquiries, please contact:Production DepartmentSpringer JapanTel.: +81-3-6831-7009Fax: +81-3-6831-7010
Office use only
No. of pages
Invoice No.
Address Code

Metadata of the article that will be visualized in OnlineFirst
ArticleTitle Successful treatment of rectal ulcers in a patient with systemic lupus erythematosus using corticosteroids andtacrolimus
Article Sub-Title
Article CopyRight Japan College of Rheumatology(This will be the copyright line in the final PDF)
Journal Name Modern Rheumatology
Corresponding Author Family Name KaiedaParticle
Given Name ShinjiroSuffix
Division Division of Respirology, Neurology and Rheumatology, Department ofMedicine
Organization Kurume University School of Medicine
Address 67 Asahi-machi, Kurume, 830-0011, Japan
Email [email protected]
Author Family Name KobayasiParticle
Given Name TeppeiSuffix
Division Division of Gastroenterology, Department of Medicine
Organization Kurume University School of Medicine
Address Kurume, Japan
Author Family Name MorokiParticle
Given Name MarikoSuffix
Division Division of Respirology, Neurology and Rheumatology, Department ofMedicine
Organization Kurume University School of Medicine
Address 67 Asahi-machi, Kurume, 830-0011, Japan
Author Family Name HondaParticle
Given Name SeiyoSuffix
Division Division of Respirology, Neurology and Rheumatology, Department ofMedicine
Organization Kurume University School of Medicine
Address 67 Asahi-machi, Kurume, 830-0011, Japan
Author Family Name YugeParticle

Given Name KentaroSuffix
Division Department of Internal Medicine
Organization Saiseikai Omuta Hospital
Address Omuta, Japan
Author Family Name KawanoParticle
Given Name HiroshiSuffix
Division Division of Gastroenterology, Department of Medicine
Organization Kurume University School of Medicine
Address Kurume, Japan
Author Family Name MitsuyamaParticle
Given Name KeiichiSuffix
Division Division of Gastroenterology, Department of Medicine
Organization Kurume University School of Medicine
Address Kurume, Japan
Author Family Name SataParticle
Given Name MichioSuffix
Division Division of Gastroenterology, Department of Medicine
Organization Kurume University School of Medicine
Address Kurume, Japan
Author Family Name IdaParticle
Given Name HiroakiSuffix
Division Division of Respirology, Neurology and Rheumatology, Department ofMedicine
Organization Kurume University School of Medicine
Address 67 Asahi-machi, Kurume, 830-0011, Japan
Author Family Name HoshinoParticle
Given Name TomoakiSuffix
Division Division of Respirology, Neurology and Rheumatology, Department ofMedicine
Organization Kurume University School of Medicine

Address 67 Asahi-machi, Kurume, 830-0011, Japan
Author Family Name FukudaParticle
Given Name TakaakiSuffix
Division Center for Rheumatic Diseases
Organization Kurume University Medical Center
Address Kurume, Japan
Schedule
Received 20 June 2012
Revised
Accepted 19 September 2012
Abstract Systemic lupus erythematosus (SLE) is frequently accompanied by gastrointestinal symptoms. Although allparts of the gastrointestinal tract may be affected, colonic involvement is quite rare. Colonic ulceration,particularly in the rectum, is associated with a high mortality rate in patients with SLE, despiteimmunosuppressive therapy. While a standard regimen for treating rectal ulcers complicated with SLE hasnot been established, combination therapy with steroids and immunosuppressive agents is necessary becauseof the associated high mortality rate. In this report, we describe a patient with SLE whose condition wascomplicated with ulcerative lesions in the rectum and sigmoid colon; the lesions were successfully treatedwith a combination of corticosteroids and tacrolimus therapy. Tacrolimus could be a useful additional oralternative modality for treating rectal involvement in SLE.
Keywords (separated by '-') Rectal ulcer - Systemic lupus erythematosus - TacrolimusFootnote Information

Author Query Form
Please ensure you fill out your response to the queries raised below
and return this form along with your corrections
Dear Author
During the process of typesetting your article, the following queries have arisen. Please
check your typeset proof carefully against the queries listed below and mark the
necessary changes either directly on the proof/online grid or in the „Author‟s response‟
area provided below
Query Details required Author’s response
1. Please check and confirm that the
authors and their respective affiliations
have been correctly identified and
amend if necessary.
2. The labels in the figures (Figs. 3 and 4)
are not readable. Please provide a new
figure with legible labels in Vector EPS
or tiff/jpeg format with 600 dpi
resolution.
3. Kindly check “complicated with SLE”
(two uses). Should this read
“complicating SLE” or “as a
complication of SLE” on each use?
4. Kindly check “change the diagnosis of
IBD”. Should this read “change the
diagnosis to IBD”?
5. Kindly check “colon fiber” (Fig. 2
caption)
6. Kindly confirm the edit to “T cell
blockade is thought to be a potential
therapeutic target”
7. Kindly confirm the edit to
“Clostridium” (genus name)
Journal: 10165
Article: 775

UNCORRECTEDPROOF
CASE REPORT1
2 Successful treatment of rectal ulcers in a patient with systemic
3 lupus erythematosus using corticosteroids and tacrolimus
4 Shinjiro Kaieda • Teppei Kobayasi • Mariko Moroki • Seiyo Honda •
5 Kentaro Yuge • Hiroshi Kawano • Keiichi Mitsuyama • Michio Sata •
6 Hiroaki Ida • Tomoaki Hoshino • Takaaki Fukuda
7 Received: 20 June 2012 / Accepted: 19 September 20128 � Japan College of Rheumatology 2012
9 Abstract Systemic lupus erythematosus (SLE) is fre-
10 quently accompanied by gastrointestinal symptoms.
11 Although all parts of the gastrointestinal tract may be
12 affected, colonic involvement is quite rare. Colonic ulcera-
13 tion, particularly in the rectum, is associated with a high
14 mortality rate in patients with SLE, despite immunosup-
15 pressive therapy.While a standard regimen for treating rectal
16 ulcers complicated with SLE has not been established,
17 combination therapy with steroids and immunosuppressive
18 agents is necessary because of the associated high mortality
19 rate. In this report, we describe a patient with SLE whose
20 condition was complicated with ulcerative lesions in the
21 rectum and sigmoid colon; the lesions were successfully
22 treated with a combination of corticosteroids and tacrolimus
23 therapy. Tacrolimus could be a useful additional or alterna-
24 tive modality for treating rectal involvement in SLE.
25
26 Keywords Rectal ulcer � Systemic lupus erythematosus �
27 Tacrolimus
28Introduction
29Systemic lupus erythematosus (SLE), a complex autoim-
30mune disease that affects various organs, is frequently
31accompanied by gastrointestinal symptoms, and lupus
32enteritis has been reported to be the most common cause of
33acute abdominal pain in SLE, accounting for up to 45 % of
34cases [1, 2]. Gastrointestinal vasculitis is one of the most
35serious complications of SLE, even though the occurrence
36of colonic lesions is quite rare (0.2 %) [1, 3]. Vasculitis of
37the bowel may lead to ulceration, hemorrhage, perforation,
38or infarction, and colonic ulceration, particularly in rectal
39lesions, has been associated with high mortality rates [4, 5].
40Despite immunosuppressive treatment, severe complica-
41tions, such as perforations of the intestinal tract, may occur,
42thus leading to an unfavorable prognosis.
43Tacrolimus, a T-cell-specific calcineurin inhibitor with
44cyclosporine A-like immunosuppressive effects, sup-
45presses T cell activation, thereby inhibiting inflammatory
46cytokine production [6]. In vivo and in vitro studies have
47shown that tacrolimus is 10 to 100 times more potent than
48cyclosporine A in inhibiting these processes [7]. Tacroli-
49mus has been approved for use worldwide in organ trans-
50plantation and for treating autoimmune diseases, including
51inflammatory bowel disease (IBD), lupus nephritis, and
52rheumatoid arthritis [8–14]. Furthermore, several reports
53have demonstrated the efficacy of tacrolimus in the treat-
54ment of various conditions not associated with nephritis,
55including arthritis, skin eruption, alopecia, cystitis, and
56hemophagocytic syndrome, in patients with SLE [15–18];
57however, its efficacy for the treatment of colonic lesions
58complicated with SLE has not been reported.
59To date, no standard therapeutic strategies for colonic
60ulcers in SLE have been established. While corticosteroids
61are routinely used as a first-line therapy, many cases have
A1 S. Kaieda (&) � M. Moroki � S. Honda � H. Ida � T. Hoshino
A2 Division of Respirology, Neurology and Rheumatology,
A3 Department of Medicine, Kurume University School of
A4 Medicine, 67 Asahi-machi, Kurume 830-0011, Japan
A5 e-mail: [email protected]
A6 T. Kobayasi � H. Kawano � K. Mitsuyama � M. Sata
A7 Division of Gastroenterology, Department of Medicine, Kurume
A8 University School of Medicine, Kurume, Japan
A9 K. Yuge
A10 Department of Internal Medicine, Saiseikai Omuta Hospital,
A11 Omuta, Japan
A12 T. Fukuda
A13 Center for Rheumatic Diseases, Kurume University Medical
A14 Center, Kurume, Japan
123Journal : Large 10165 Dispatch : 27-9-2012 Pages : 5
Article No. : 775h LE h TYPESET
MS Code : MORH-D-12-00268 h CP h DISK4 4
Mod Rheumatol
DOI 10.1007/s10165-012-0775-x
Au
tho
r P
ro
of

UNCORRECTEDPROOF
62 been reported to be steroid resistant, and perforations of the
63 intestinal tract may occur after the induction of steroid
64 therapy [3–5]. These findings suggest that combination
65 therapy with steroids and an immunosuppressant is nec-
66 essary. However, guidelines for the use of potent immu-
67 nosuppressive agents have not yet been established, and
68 low-dose oral tacrolimus may represent an alternative
69 therapy for the treatment of colonic ulcers in SLE. In the
70 current report, we describe a case of SLE complicated with
71 ulcerative lesions of the rectum and sigmoid colon in which
72 combination therapy with steroids and tacrolimus contrib-
73 uted to the remission of rectal ulcers and had steroid-
74 sparing effects for 12-month follow-up.
75 Case report
76 A 51-year-old man, who had been diagnosed with SLE and
77 lupus nephritis at 36 years of age, remained in a stable
78 condition while receiving 5 mg prednisolone (PSL) and
79 150 mg mizoribine daily. Nonsteroidal anti-inflammatory
80 drugs and antibiotics were not prescribed. Before admis-
81 sion to our department, he developed gastrointestinal
82 symptoms and experienced more than 10 episodes of
83 diarrhea associated with abdominal cramps. He presented
84 with an elevated body temperature (37.6 �C); other vital
85 signs were normal. A physical examination revealed mild
86 tenderness of the middle lower abdomen without muscular
87 defense. The palpebral conjunctiva was anemic. No skin
88 rash was evident on either the face or extremities.
89 Laboratory evaluations revealed mild anemia (Hb 9.8 g/
90 dL) and leukopenia (WBC 2500 9 102/lL). Routine blood
91 chemistry and coagulofibrinolytic tests were normal. The
92 erythrocyte sedimentation rate was elevated (93.0 mm/h),
93 but C-reactive protein (CRP) was undetectable. Urinalysis
94 findings were positive for urinary protein (1.18 g/day);
95 however, no casts were observed in the urinary sediment.
96 Serum albumin levels were mildly decreased. The results of
97 routine kidney function tests were normal, and creatinine
98 clearance was 94.4 mL/min. An immunological test
99 revealed the patient to be positive for anti-nuclear antibodies,
100 with a titer of 1:160 (a speckled pattern), and anti-dsDNA
101 antibody levels were elevated (81.2 IU/mL). Serum com-
102 plement levels were normal, and anti-Sm antibodies, anti-U1
103 RNP antibodies, anti-SS-A antibodies, and rheumatoid fac-
104 tor were positive. Anti-cardiolipin antibodies and lupus
105 anticoagulant were negative. Laboratory data revealed leu-
106 kocytopenia, proteinuria, and an increase in the anti-dsDNA
107 antibody titers, suggesting elevated disease activity.
108 An endoscopic examination revealed girdle ulcerative
109 lesions in the rectum (Rs to Ra; Fig. 1a). The fundus of the
110 ulcer and surrounding mucosa were erythrogenic and prone
111 to bleeding. A histopathological examination of biopsy
112specimens taken from the ulcer showed nonspecific gran-
113ulation and proctitis, but no evidence of vasculitis. Gast-
114rografin enema radiography detected a stenosis of the
115sigmoid colon due to an intestinal tract edema (Fig. 1b,
116arrow). An abdominal enhanced computed tomography
117(CT) image revealed bowel wall thickening of the rectum
118(Fig. 1c). The patient’s stool samples were positive for
119occult blood, and fecal cultures were positive for a small
120number of Enterobacteriaceae species, but no other
121pathogens, including Clostridium antigen and acid-fast
122bacillus. Cytomegalovirus (CMV) infection was excluded
123because intranuclear inclusions were not observed histo-
124logically, and CMV antigen-positive leukocytes were not
125detected in the patient’s peripheral blood.
126The absence of any positive evidence for infective
127agents and the presence of colonic ulcers were thought to
128be consistent with a gastrointestinal manifestation of SLE.
129IBD, such as Crohn’s disease and ulcerative colitis, was
130considered as a differential diagnosis. Although IBD is
131rarely associated with SLE, SLE is rarely active at the time
132of IBD manifestation [19]. Furthermore, neither colonos-
133copy nor pathological study revealed specific findings that
134were sufficient to change the diagnosis of IBD.
135Treatment with 500 mg intravenous methylprednisolone
136for 3 days, followed by 50 mg/day oral PSL and 2 mg/day
137tacrolimus was initiated. As shown in Fig. 2, the gastroin-
138testinal symptoms improved after the start of treatment.
139Furthermore, treatment with systemic steroids and oral ta-
140crolimus healed the ulcer endoscopically 5 weeks after ini-
141tiation of therapy (Fig. 2, CF�), and a reduction in PSL dose
142was possible. The patient was discharged from the hospital in
143an improved condition and has been monitored on an out-
144patient basis. Follow-up colonoscopies, which were con-
145ducted at 3 and 5 months after the initiation of treatment,
146demonstrated a reduction in the ulcerated area and regener-
147ation of epithelium covering the surface (Fig. 2, CF` and
148´).WBC counts normalized and anti-dsDNA antibody titers
149and proteinuria were decreased during the subsequent out-
150patient course (Fig. 2), indicating that the patient’s SLE was
151under control. Anti-DNA antibodies were examined by
152radioimmunoassay approximately 12 months after patient
153discharge and were confirmed to be within normal limits
154(5.8 IU/mL, normal range\6 IU/mL). Currently, the patient
155occasionally complains of abdominal pain without diarrhea,
156and oral tacrolimus has been increased to 3 mg/day. The
157patient has remained well for 12 months, and PSL has been
158reduced to 15 mg/day.
159Discussion
160Gastrointestinal manifestations are a frequent complication
161associated with SLE [1, 2]. Although colonic lesions are
Mod Rheumatol
123Journal : Large 10165 Dispatch : 27-9-2012 Pages : 5
Article No. : 775h LE h TYPESET
MS Code : MORH-D-12-00268 h CP h DISK4 4
Au
tho
r P
ro
of

UNCORRECTEDPROOF
162 quite rare, ulcerative lesions in the large intestine have
163 been demonstrated in several studies [3–5, 20]. Of the 25
164 cases that have been reported in Japan, complications, such
165 as perforations and fistulas, were observed in 9 patients, 4
166 of whom died [5]. In another study, perforation was
167 observed in 5 out of 6 cases involving rectal ulceration, and
168 4 of these patients died, indicating a poor prognosis for
169 such cases [4]. Colonic ulceration, particularly rectal
170 lesions, is associated with a high mortality rate. However,
171 despite this high mortality, ulcerative lesions in the rectum
172 and sigmoid colon were improved by appropriate medical
173 treatment in the present case. We emphasize that early
174 administration of immunosuppressants, such as tacrolimus
175 with high-dose steroid therapy, may contribute to an
176 improvement in its poor prognosis.
177 Intestinal vasculitis was diagnosed in 45–60 % of SLE
178 patients presenting with acute abdominal pain [1, 21, 22].
179 In our patient, findings of vasculitis were not obtained from
180 the tissue biopsy specimen. Rectal and sigmoid colon
181 ulcers were presumably caused by vasculitis based on the
182 following facts: (1) a typical vasculitis pattern is difficult to
183 prove on the basis of endoscopic biopsy [4, 5, 20]; (2) the
184 bowel wall thickness detected in abdominal CT (Fig. 1c)
185 was suggestive of bowel ischemia [23]; (3) a drop in the
186 WBC count at the time of acute abdominal pain correlates
187 with the occurrence of intestinal vasculitis, as observed in
188 the present case [1]; and (4) the rectal ulcer responded to
189immunosuppressive therapy, indicating impressive
190improvement. Thrombosis of the mesenteric vessels asso-
191ciated with antiphospholipid syndrome (APS) may give
192rise to mesenteric ischemia [24]; however, APS was
193excluded because these antibodies were not detected in the
194present case.
195High-dose corticosteroid therapy is considered the
196treatment of choice for gastrointestinal complications
197associated with SLE; however, not all patients respond
198sufficiently, and some may relapse when steroids are
199tapered. Prior studies demonstrated sustained remission
200after the use of oral mesalazine and pulse cyclophospha-
201mide when steroid therapy alone was not effective [3, 5]. It
202should be noted that the outcomes in patients with perfo-
203rations are extremely poor, and therefore immunosup-
204pressants are clearly necessary for the treatment of colonic
205ulcers, particularly when rectal lesions are involved.
206Tacrolimus, a potent T cell inhibitor, has been suc-
207cessfully administered for the treatment of inflammatory
208bowel disease, lupus nephritis, and rheumatoid arthritis [9–
20914]. While various immune response abnormalities have
210been identified in patients with SLE, aberrant and persistent
211T cell abnormalities involving signal transduction defects
212have been recognized as important factors in disease
213development in the last decade [25]. On the basis of these
214findings, T cell blockade is thought to be a potential ther-
215apeutic target for SLE and its manifestations. Recently,
(A)
(C)
(B)Fig. 1 a Endoscopic
examination of the rectum
showing girdle ulcerative
lesions. b Barium enema
examination showing narrowing
of the sigmoid colon (arrow).
c Abdominal enhanced
computed tomography showing
bowel wall thickening of the
rectum (arrow)
Mod Rheumatol
123Journal : Large 10165 Dispatch : 27-9-2012 Pages : 5
Article No. : 775h LE h TYPESET
MS Code : MORH-D-12-00268 h CP h DISK4 4
Au
tho
r P
ro
of

UNCORRECTEDPROOF
216 tacrolimus has been successfully applied in the treatment of
217 various manifestations without nephritis in SLE [15–18].
218 Furthermore, tacrolimus, a drug that has been shown to be
219 well absorbed, even in patients with severe colitis, serves
220 as a rational therapeutic option for inflammatory bowel
221 disease that is refractory to conventional therapy [26].
222 Thus, this immunosuppressive agent was administered to
223 our current patient. Tacrolimus does not act quickly, and its
224 onset of action usually requires 2–4 weeks; thus, we
225 simultaneously initiated high-dose steroid therapy and
226 tacrolimus [27]. Although an improvement in gastrointes-
227 tinal symptoms may result from high-dose corticosteroid
228 treatment, low-dose oral tacrolimus has also been shown to
229 help maintain the remission of rectal lesions while exerting
230 a steroid-sparing effect. Therefore, tacrolimus could be an
231 additional or alternative modality for treating rectal
232 involvement in SLE.
233 In conclusion, colonic lesions, particularly those
234 occurring in the rectum, are quite rare in patients with SLE,
235 but are associated with a high mortality rate. The present
236 case demonstrated that combination therapy with steroids
237and tacrolimus is an effective therapeutic option for treat-
238ing rectal involvement in patients with SLE.
239Conflict of interest None.
240References
2411. Lee CK, Ahn MS, Lee EY, Shin JH, Cho YS, Ha HK, et al. Acute242abdominal pain in systemic lupus erythematosus: focus on lupus243enteritis (gastrointestinal vasculitis). Ann Rheum Dis. 2002;61:244547–50.2452. Sultan SM, Ioannou Y, Isenberg DA. A review of gastrointestinal246manifestations of systemic lupus erythematosus. Rheumatology.2471999;38:917–32.2483. Grimbacher B, Huber M, von Kempis J, Kalden P, Uhl M, Kohler249G, et al. Successful treatment of gastrointestinal vasculitis due to250systemic lupus erythematosus with intravenous pulse cyclo-251phosphamide: a clinical case report and review of the literature.252Br J Rheumatol. 1998;37:1023–8.2534. Teramoto J, Takahashi Y, Katsuki S, Sato T, Sakamaki S,254Kobayashi D, et al. Systemic lupus erythematosus with a giant255rectal ulcer and perforation. Intern Med. 1999;38:643–9.
Mizoribine 150mg
Tacro limus 2mg
CF
3mg
Steroidtherapy
Diarrhea
Abdominalpain
2010
CF
PSL10mg
mPSL
500mg
Oct. Nov.
DischargeCF2011
PSL50 45 40 35 25 20
Admission
Dec. Jan. Feb. Mar.
17.5
CF CF
CF
35 30
May
WBC 2500 2000 12200 6200 4100 5100 5400 5700
abs 81.2 99.9 30.8 <25
Protein Urea 1.18 0.5 +/- +/- +/-
g/day g/day
Anti-dsDNA
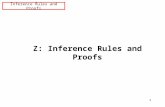
Fig. 2 Clinical course of the patient. Anti-dsDNA antibodies were quantified by enzyme-linked immunosorbent assay (normal range\25 IU/
mL). mPSLmethylprednisolone, PSL prednisolone, CF colon fiber,WBC white blood cell, Anti-dsDNA abs anti-double-stranded DNA antibodies
Mod Rheumatol
123Journal : Large 10165 Dispatch : 27-9-2012 Pages : 5
Article No. : 775h LE h TYPESET
MS Code : MORH-D-12-00268 h CP h DISK4 4
Au
tho
r P
ro
of

UNCORRECTEDPROOF
256 5. Miyahara S, Ito S, Soeda A, Chino Y, Hayashi T, Takahashi R,257 et al. Two cases of systemic lupus erythematosus complicated258 with colonic ulcers. Intern Med. 2005;44:1298–306.259 6. Sakuma S, Kato Y, Nishigaki F, Sasakawa T, Magari K, Miyata260 S, et al. FK506 potently inhibits T cell activation induced TNF-261 alpha and IL-1beta production in vitro by human peripheral blood262 mononuclear cells. Br J Pharmacol. 2000;130:1655–63.263 7. Scott LJ, McKeage K, Keam SJ, Plosker GL. Tacrolimus: a264 further update of its use in the management of organ transplan-265 tation. Drugs. 2003;63:1247–97.266 8. Shapiro R, Jordan ML, Scantlebury VP, Vivas C, Gritsch HA,267 Corry RJ, et al. The superiority of tacrolimus in renal transplant268 recipients—the Pittsburgh experience. Clin Transplant. 1995:269 199–205.270 9. Benson A, Barrett T, Sparberg M, Buchman AL. Efficacy and271 safety of tacrolimus in refractory ulcerative colitis and Crohn’s272 disease: a single-center experience. Inflamm Bowel Dis. 2008;273 14:7–12.274 10. Mok CC, Tong KH, To CH, Siu YP, Au TC. Tacrolimus for275 induction therapy of diffuse proliferative lupus nephritis: an276 open-labeled pilot study. Kidney Int. 2005;68:813–7.277 11. Miyasaka N, Kawai S, Hashimoto H. Efficacy and safety of278 tacrolimus for lupus nephritis: a placebo-controlled double-blind279 multicenter study. Mod Rheumatol. 2009;19:606–15.280 12. Morimoto S, Watanabe T, Lee S, Amano H, Kanamaru Y,281 Ohsawa I, et al. Improvement of rapidly progressive lupus282 nephritis associated MPO-ANCA with tacrolimus. Mod Rheu-283 matol. 2010;20:291–4.284 13. Takahashi S, Hiromura K, Sakurai N, Matsumoto T, Ikeuchi H,285 Maeshima A, et al. Efficacy and safety of tacrolimus for induc-286 tion therapy in patients with active lupus nephritis. Mod Rheu-287 matol. 2011;21:282–9.288 14. Kitahara K, Kawai S. Cyclosporine and tacrolimus for the289 treatment of rheumatoid arthritis. Curr Opin Rheumatol. 2007;19:290 238–45.291 15. Kusunoki Y, Tanaka N, Kaneko K, Yamamoto T, Endo H, Kawai292 S. Tacrolimus therapy for systemic lupus erythematosus without293 renal involvement: a preliminary retrospective study. Mod294 Rheumatol. 2009;19:616–21.295 16. Suzuki K, Kameda H, Amano K, Nagasawa H, Takei H, Nishi E,296 et al. Single center prospective study of tacrolimus efficacy and
297safety in the treatment of various manifestations in systemic298lupus erythematosus. Rheumatol Int. 2011;31:757–63.29917. Maruoka H, Honda S, Takeo M, Koga T, Fukuda T, Aizawa H.300Tacrolimus treatment for refractory lupus cystitis. Mod Rheu-301matol. 2006;16:264–6.30218. Watanabe H, Hirase N, Goda H, Nishikawa H, Ikuyama S. Oral303low-dose tacrolimus therapy for refractory hemophagocytic304syndrome associated with systemic lupus erythematosus. Mod305Rheumatol. 2012;22:284–9.30619. Nitzan O, Elias M, Saliba WR. Systemic lupus erythematosus and307inflammatory bowel disease. Eur J Intern Med. 2006;17:313–8.30820. Yuasa S, Suwa A, Hirakata M, Hibi N, Iwao Y, Koizumi K, et al.309A case of systemic lupus erythematosus presenting with rectal310ulcers as the initial clinical manifestation of disease. Clin Exp311Rheumatol. 2002;20:407–10.31221. Buck AC, Serebro LH, Quinet RJ. Subacute abdominal pain313requiring hospitalization in a systemic lupus erythematosus314patient: a retrospective analysis and review of the literature.315Lupus. 2001;10:491–5.31622. Medina F, Ayala A, Jara LJ, Becerra M, Miranda JM, Fraga A.317Acute abdomen in systemic lupus erythematosus: the importance318of early laparotomy. Am J Med. 1997;103:100–5.31923. Byun JY, Ha HK, Yu SY, Min JK, Park SH, Kim HY, et al. CT320features of systemic lupus erythematosus in patients with acute321abdominal pain: emphasis on ischemic bowel disease. Radiology.3221999;211:203–9.32324. Luman W, Chua KB, Cheong WK, Ng HS. Gastrointestinal324manifestations of systemic lupus erythematosus. Singapore Med325J. 2001;42:380–4.32625. Takeuchi T, Tsuzaka K, Abe T, Yoshimoto K, Shiraishi K,327Kameda H, et al. T cell abnormalities in systemic lupus erythe-328matosus. Autoimmunity. 2005;38:339–46.32926. Fellermann K, Herrlinger KR, Witthoeft T, Homann N, Ludwig330D, Stange EF. Tacrolimus: a new immunosuppressant for steroid331refractory inflammatory bowel disease. Transpl Proc. 2001;33:3322247–8.33327. Ng SC, Kamm MA. Therapeutic strategies for the management of334ulcerative colitis. Inflamm Bowel Dis. 2009;15:935–50.
335
Mod Rheumatol
123Journal : Large 10165 Dispatch : 27-9-2012 Pages : 5
Article No. : 775h LE h TYPESET
MS Code : MORH-D-12-00268 h CP h DISK4 4
Au
tho
r P
ro
of















![Abstracts of - Cell Journal · Anderson’s electronic atlas of hematology.[CD-ROM]. Philadelphia: Lippincott Williams & Wilkins; 2002. D. Proofs: Proofs are sent by email as s and](https://static.fdocuments.in/doc/165x107/5f04dbff7e708231d410114f/abstracts-of-cell-journal-andersonas-electronic-atlas-of-hematologycd-rom.jpg)