Hemodynamics Study of Carotid Stenosis Paper 1st Gramma Auto Review
19
HEMODYNAMICS STUDY OF CAROTID STENOSIS: CORRELATION BETWEEN WALL SHEAR STRESS AND STENOSIS SEVERITY Mauricio Santos¹, Hamidreza Gharahi¹, David C. Zhu², J.Kevin DeMarco², Seungik Baek¹ ¹Cardiovascular & Tissue Mechanics Lab, Department of Mechanical Engineering and ²Departement of Radiology, Michigan State University ,East Lansing, MI 48824 Keywords: WSS, Carotid artery bifurcation, stenosis severity, atherosclerosis, autoregulation, RCR model. Abstract The term Carotid stenosis refers to the narrowing of a carotid artery, which is caused by the accumulation of plaque. Plaque is a substance composed of low-density lipoprotein (LDL) cholesterol; calcium and immune cells that sticks to artery wall and leads to narrowing and hardening of the artery. This disease increases the risk of stroke of the brain due the narrowed artery. This diseased artery increases the possibility of plaque breaking off and the clot travels to small blood vessels in the brain. Conditions of hemodynamics and arterial mechanics, such as blood flow, pressure waves, blood vessel deformation, and wall shear stress (WSS) are directly related to the disease progression. The Carotid artery bifurcation is the place most affected by plaque accumulation because of the flow division and the low WSS that results in a biomechanical response of endothelium (inner layer of wall) that contributes to the increase of the permeability of this layer. The goals of this study are to find a relation between WSS and plaque formation in the bifurcation of carotid artery, find the influence of deformed lumen’s profile to blood flow, and compare fluid mechanics proprieties of healthy and unhealthy patients. To perform this study, Time of Flight MRI (TOF-MRI) scans were used to generate 3D model of diseased carotid arteries and CT scan was used to generate the 3D model of healthy artery. Computational fluid dynamics (CFD) is applied to analyze WSS and pressure in anatomically realistic models of one healthy and four patients with different stenosis severity.
-
Upload
mauricio-novaes -
Category
Documents
-
view
222 -
download
1
description
gg
Transcript of Hemodynamics Study of Carotid Stenosis Paper 1st Gramma Auto Review

HEMODYNAMICS STUDY OF CAROTID STENOSIS: CORRELATION BETWEEN WALL SHEAR STRESS AND STENOSIS SEVERITY
Mauricio Santos¹, Hamidreza Gharahi¹, David C. Zhu², J.Kevin DeMarco², Seungik Baek¹
¹Cardiovascular & Tissue Mechanics Lab, Department of Mechanical Engineering and ²Departement of Radiology, Michigan State University ,East Lansing, MI 48824
Keywords: WSS, Carotid artery bifurcation, stenosis severity, atherosclerosis, autoregulation, RCR model.
Abstract
The term Carotid stenosis refers to the narrowing of a carotid artery, which is caused by the accumulation of plaque. Plaque is a substance composed of low-density lipoprotein (LDL) cholesterol; calcium and immune cells that sticks to artery wall and leads to narrowing and hardening of the artery. This disease increases the risk of stroke of the brain due the narrowed artery. This diseased artery increases the possibility of plaque breaking off and the clot travels to small blood vessels in the brain. Conditions of hemodynamics and arterial mechanics, such as blood flow, pressure waves, blood vessel deformation, and wall shear stress (WSS) are directly related to the disease progression. The Carotid artery bifurcation is the place most affected by plaque accumulation because of the flow division and the low WSS that results in a biomechanical response of endothelium (inner layer of wall) that contributes to the increase of the permeability of this layer. The goals of this study are to find a relation between WSS and plaque formation in the bifurcation of carotid artery, find the influence of deformed lumen’s profile to blood flow, and compare fluid mechanics proprieties of healthy and unhealthy patients. To perform this study, Time of Flight MRI (TOF-MRI) scans were used to generate 3D model of diseased carotid arteries and CT scan was used to generate the 3D model of healthy artery. Computational fluid dynamics (CFD) is applied to analyze WSS and pressure in anatomically realistic models of one healthy and four patients with different stenosis severity.
1.Background
Carotid stenosis is the constriction of lumen (inner surface of blood vessel, which it is in direct contact with the blood) of carotid artery caused by atherosclerosis. Atherosclerosis is the accumulation of plaque on the wall of arteries. Plaque is composed by cholesterol, calcium, white blood and others fatty components. Hypertension, cigarette smoking, diabetes and aging cause atherosclerosis. There are two carotid artery in the body, one on each side of the neck. The carotid artery is divided into two branches: internal and external carotid artery. The internal artery supply blood to the brain and external to face and scalp. In addition, carotid artery begins at top of aorta, after ascending aorta artery. This diseased blood vessel can leads to brain stroke by three mechanisms: the plaque accumulation can grow larger until cause a severe narrowing of artery and reduce the blood flow to the brain, blood-clotting formation or plaque accumulated

can rupture and block a smaller blood vessel in the brain, causing a brain stroke. According to the World Health Organization, 15 million patients suffer from stroke annually and four of every ten people who died of stroke could be saved if their pressure had been regulated [1, 2].
Three layers compose carotid artery: tunica intima, tunica media and tunica adventitia. Each one of these layers has a different role. The innermost layer, tunica intima, is also called endothelium. The endothelium is a high responsible structure that interact with blood and play an important role in regulation of permeability and platelet aggregation. The middle layer (tunica media) is composed by vascular smooth muscle cells (VSMCs) surrounded by a matrix of elastin. Inflammation and stress applied at tunica intima alters the composition of tunica media by migration of VSCM .This migration occurs in response of a protein, cytokine, released by damaged endothelial cells. The outer layer is strong and mostly composed by collagen. Thus, the stiffness is direct related with the ratio of elastin of tunica media and collagen of tunica adventitia [3].
The process of atherosclerosis may begin as a child. However, the effects are usually noticed with aging (50-60 years old). There are many favorable conditions to explain this fact. With aging arteries become stiffer because of VSMCs die. In addition, there is degradation of elastin and the body does not produced it as before. The heart has to works harder to pump the blood and receive the blood back. There is an increase of possibility of plaque buildup with a weaker and less elastic artery. In addition, a harder artery means a higher pressure due the higher resistance to the blood flow. When the wall of artery is exposed to a higher pressure, there is more chance of the endothelium be damaged and accelerate the formation of plaque [3, 4]. Moreover, there is one more important factors associated with age: the production of nitric oxide (NO). Healthy endothelial cells produces NO, an important molecule that helps prevent white blood cells from accumulate to the artery wall. NO is used by endothelial cells to subdue the oxygen free radicals (reactive atom, or a group of them, that can damage cells altering their chemical structure) of the body, but during this process NO destroy themselves. Associated with aging there is the prevalent presence of a hormone, angiotensin II, that increase free radical production and artery inflammation [1]. .
It is possible make an analogy between the heart and a reciprocating pump, because a cardiac cycle is usually represented by 1/3 of time for systole and 2/3 for diastole. In this way, only during 1/3 of total time the heart is pumping blood to the body. However, during systole there is elastic energy been stored at blood vessels that will drive the blood through downstream vessels during diastole, when aortic valves is closed. For a stiffer artery is required a higher pressure to stretch carotid’s wall in order to store energy. Because of the heart works as reciprocating pump and the artery wall is not rigid, the blood flow rate and pressure is not the same for all cardiac cycle. There are pressure and blood flow rate waves. In a stiffer artery, the pulse wave reflection can return soon enough to be added to the wave generated by the heart (systolic pressure) or to have add effect on diastolic pressure. For example, a stiffer aorta has a higher systolic pressure and lower diastolic pressure due the fact the reflect wave is added to the heart-generated pressure of systole. Atherosclerosis is also called hardening of artery, because advanced plaque is formed by calcification and fibrous connection tissue (VSMC). The

hardening of artery and change of lumen area caused by plaque accumulation on artery’s wall are two relevant facts for change in pressure wave of carotid artery. There are reflection of the pressure and flow wave whenever there is a change in stiffness or cross-sectional area of lumen [6, 7].
Endothelial cells are very responsive cells that can detect pressure, oxygen and flow changes. Also, it is very responsive to change of magnitude and direction of wall shear stress (WSS). A blood vessel is not a linear and rigid tube. An artery change shape, length, curvature and diameter due the dynamic interaction with blood flow waves. Because of that, the flow is not strictly laminar, i.e., it is not strictly a gradient of velocity that increase as moved to the center of a tube. WSS is the tangential force created at the wall by the friction between the blood and wall. WSS is an important parameter associated with plaque formation and rupture, because it changes wall composition and spatial orientation of the cells. The most common place where there is plaque accumulation is at vessel bifurcation. When the laminar flow separates at carotid artery bifurcation, the highest velocities is in contact with the flow divisor. Also, there is flow separation at the branches. Thus, the branches of carotid artery are exposed to low velocities and high change of direction of the flow due the more disturbed flow. Moreover, high WSS results in elongation and alignment of endothelium cells in the direction of the flow. However, endothelium cells exposed to low WSS do not have preferred orientation. In addition, low WSS may increases permeability of endothelium cells. That happens because the stress applied on endothelium cells affects the production of substances, as NO [1, 8].
The mechanism of maintain constant blood flow despite change in perfusion pressure is called autoregulation of blood flow. It is important to brain normal activity, since the brain uses 20% of oxygen available in the body. For the brain is critical that blood flow rate be in a tight range. The autoregulation of blood flow can be achieved because of the ability of constrict and dilate of blood vessel. There are three hypothesis to explain vasodilatation: metabolic, myogenic and endothelial mechanisms. According to myogenic hypothesis small arteries and arterioles responds to pressure as a stimulus to causing constriction (if the pressure rises) or vasodilation (if the pressure falls). For metabolic mechanism, blood flow and tissue activity are coupled in such way that reduction of blood flow rate will cause vasodilation in blood vessel. Thus, the decrease of blood flow rate due to carotid stenosis can leads to dilation of downstream blood vessels [9-11]. Due the limitation of data available was assumed the function of autoregulation of blood flow is working perfectly. Thus, there will be always the same flowsplit between the braches of carotid artery , despite of the differents stenosys severity. However , that can not represent what happens in the reality. There is the possibility of increase of blood flow thourght the internal carotid artery of the other side of the neck. In addition , The vertebral artery also supply blood to the brain. The body can also increase the blood flow trought vertebral artery to compesete the lower blood flow trought carotid artery.

2. Methods
This study was made using real patient image, CT scan and time on flight (TOF) MRI, acquired from the department of radiology from MSU. The images were imported to an image processing software package called MIMICS®. Using that software was possible select and generated the 3D model of carotid artery. In addition, the blood flow velocity data used was acquired from PC-MRI of a healthy patient.
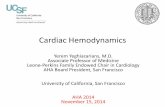
Figure 1.1. Blood flow rate (cardiac cycle)
After segmentation of carotid artery computational fluid dynamic (CFD) simulation was performed in all 3D model created using a software called SimVascular. However, many assumptions and boundary conditions had to be set in order to be possible get results, as WSS, pressure and velocity. The blood flow wave inlet was used as major boundary condition. Thus, the follow parameters were set:
• Cardiac Cycle 1.0 s;
• Peak systolic at 0.96 s;
• Time step of 0.005 sec ( 200 fields/cycle);
• Systolic Pressure :117 mmHg;
• Diastolic Pressure : 76 mmHg;
Moreover, the follow assumptions were made:
Wall of carotid artery is assumed to be rigid [12]; Laminar flow pattern; Steady state flow; Conservation of mass ( continuity equation) and conservation of momentum ( navier
stoke equation)[8]; Newtonian behavior of fluid is assumed [12]; The function of autoregulation of blood flow is working perfectly, i.e., there is 70%
of blood flow in internal carotid artery. For a healthy carotid artery, the percentage of

blood flow rate thought internal carotid artery is in the range of 60-70 % of the flow rate at common carotid artery [13].
A hydraulic-electrical analogy at downstream vessels as outlet boundary condition was used to calculate pressure of carotid artery. This analogy is referred as RCR model. RCR stand for proximal resistance, compliance and distal resistance of blood vessels. Proximal resistance is related to large arteries and arterioles, distal resistance is related to small arterioles and capillaries and capacitance is related to large arteries wall compliance.
In this model blood flow rate is analogue to current and voltage difference is analogue to pressure difference. The RCR values are initially estimated using SimVascular, but it is necessary set diastolic pressure, systolic pressure, pulse pressure, mean arterial pressure and blood flow target at every inlet and outlet. The target flow was obtained running the simulation for the healthy patient with only blood vessels resistance until get 70% of inlet blood flow in the internal carotid artery. When required, the RCR values had to be changed to match with pressure or blood flow rate expected.
Figure 1.2 Circuit representation RCR model [retrieved from: http://simvascular.ucsd.edu/docsFlowSolver.html]

3. Results
Using the wave form acquired at the inlet, many computational simulations were performed on a coarse mesh to obtain acceptable pressure wave at inlet at outlets. The target systolic and diastolic pressure at whole system were 117 mmHg and 76 mmHg, respectively. All follow results displayed will be results of fourth cardiac cycle at diastole phase (0.5 seconds).
3.1 Healthy right carotid artery results
The figure below shown the results using the boundary conditions and assumptions described previously. The figures shown hemodynamics results for a healthy carotid artery. Despite the fact of high pulse pressure (figure 3), the pressure wave for inlet is out phase with blood flow rate (figure 1.1), as expected. In addition, the magnitude of WSS is in agreement with literature and there is highest stress at artery bifurcation (figure 5)
Figure 2.Pressure (Pa)-healthy artery (right) Figure 3.Pressure wave (inlet)-healthy artery (right)
Figures 2 shows that pressure on the surface of the artery is in the range of 73 mmHg and 75mmHg, with the peak of pressure applied at flow divisor and lower pressures at internal carotid artery. A noticeable result is the fact is that at flow divisor the velocity of the blood is lowest (figure 4). In addition, inlet fully developed flow has the peak of velocity mostly directed to internal carotid artery.
The table 1 shows that RCR parameters used satisfied the assumption of perfectly autoregulation of blood flow: 70.1% of blood flow of the inlet goes to internal carotid artery.
Pressure average(mmHg)
Flow rate average(mm³/s)
Inlet 83.96 8334outlet_1 81.76 5849outlet_2 80.88 2485

Table 1.Pressure and flow rate average of healthy carotid artery
The WSS results shows that the edges and surrounding of outlets are submitted to highest values (magnitude) of WSS. Despite the fact that range have not been displayed, that was verified the edges and surrounding are exposed to stress higher than 15 KPa. Figure 5 shows that external carotid artery is subjected to highest values of WSS than internal carotid artery. The blood flow divisor is exposed to higher stress than other parts of the artery (most of the artery wall, internal and external carotid artery). The magnitude that some point of flow divisor are exposed reaches 20 Pa (figure 5.c).However , a considerable surface portion of flow divisor is exposed to 10 Pa (figure 5.b) , but most of it is submitted , at least , to 5 Pa ( figure 5.a). In addition, it is possible noticed that beginning of external carotid bifurcation and almost all end of external and internal carotid artery are exposed to 5 Pa (figure 5.a).
Figure 4. Blood velocity- healthy artery (right)
Figure 5.WSS applied on carotid artery surface within three different ranges of magnitudes for a healthy patient-right carotid artery
3.2 Diseased right carotid artery results

The figure below shown the results using the boundary conditions and assumptions described previously. The figures show hemodynamics results for a diseased right carotid artery. Figure 7 shows a very similar pressure wave profile with the previous analysis, but the systolic and diastolic pressure are slightly higher. In addition, it is possible notice that the pressure wave of this diseased artery is advanced if compared with the healthy patient – approximately 0.0125 seconds.
Figure 6.Pressure (Pa)-diseased artery (right) Figure 7.Pressure wave (inlet)-diseased artery (right)
Figures 6 shows that pressure on the surface of the artery is in the range of 73.6 mmHg and 76.7 mmHg, with the peak of pressure applied at flow divisor and lower pressures at internal carotid artery. In addition, the velocity in the internal carotid artery for this patient is higher than the blood flow velocity of the healthy patient. For the healthy patient the maximum velocity was 743.54 mm/s (figure 4), but for this diseased patient the velocity reaches 983 mm/s (figure 8). The velocity is higher at than branches and it is highest at internal carotid artery. It is also possible to notice that high velocity is reached before in the branches if compared with the healthy patient. In addition, the velocity near flow divisor is lower than others regions of the carotid artery. Also, inlet fully developed flow has the peak of velocity mostly directed to external carotid artery.
Figure 8. Blood velocity –diseased artery (right)

The table 2 below show that the diseased artery has a lower proportion of blood flow through internal carotid artery than healthy carotid artery. However, that difference is only 0.04%.
Pressure average(mmHg)
Flow rate average(mm³/s)
Inlet 85.03 8334outlet_1 81.02 5817outlet_2 82.19 2517
Table 2.Pressure and flow rate average of diseased right carotid artery
The results also show similar behavior of WSS if compared with the results of healthy patient. The edges and its surrounding are exposed to highest values of stress. Some points of the flow divisor are exposed to at least 50 Pa (figure 9.c), but that is not true for all surfaces of the artery. Within the range of 10 Pa (figure 9.b) is possible notice that flow divisor and the beginning of external carotid artery are exposed to, at least, 10 Pa. In addition, most of the surfaces of internal and external carotid artery are exposed to 5 Pa (figure 9.a).
Figure 9. WSS applied on carotid artery surface within three different ranges of magnitudes for diseased right carotid artery
3.3 Diseased left carotid artery results
The figure below shown the results using the boundary conditions and assumptions described previously. The figures shown hemodynamics results for a diseased left carotid artery. Figure 11 shows a very similar pressure wave profile to the two arteries analyzed previously, but the systolic and diastolic pressure are slightly higher. In addition, it is possible to notice that the pressure wave of this diseased left artery is advanced if compared with the two previous subject results – approximately 0.25 seconds, if compared with the healthy patient.

Figure 10. .Pressure (Pa)-diseased artery (left) Figure 11. Figure 12.Pressure wave (inlet)-diseased artery (left)
Figures 11 shows that pressure on the surface of the artery is in the range of 73.5 mmHg and 76.5 mmHg. The flow divisor still has high pressure, but it is not much higher than beginning of internal carotid. However, as the diseased right carotid artery, the internal bifurcation has the lowest pressure near the outlet. Figure 12 shows that near flow divisor the velocity is the lowest in artery. In addition, the velocity is higher in the direction of internal carotid artery at plaque accumulation. The blood flow can reaches 1266 mm/s.
Figure12. Blood velocity –diseased artery (right)
The table 3 below show that the diseased artery has a 70.3% of inlet blood flow going to internal carotid artery.
Pressure average(mmHg)
Flow rate average(mm³/s)
Inlet 85.8 8334outlet_1 81.78 5859outlet_2 81.83 2475

Table 3.Pressure and flow rate average of diseased left carotid artery
The edge of the outlet and it surround is also exposed to higher stress with the magnitude of at least 15 KPa. There are few points at flow divisor where the WSS is 80 Pascal, but a considerable portion of flow divisor surface are exposed to 50 Pascal (figure 13.b). Moreover, the figure 13.a shows that the surface narrowed by plaque in the internal carotid artery is exposed to WSS of 20 Pa.
Figure 13. WSS applied on carotid artery surface within three different ranges of magnitudes for diseased right carotid artery
4. Discussion/ Conclusion
The results obtained only can be analyzed in a comparative way, in order to try finding a pattern and agreement with studies made previously. Many assumptions had to be made in order to be possible run CFD simulation, because of that, the results may not represent what happens in reality. Thus, more data is required to find a more accurate tendency. It was not possible run simulation in three-segmented very constricted artery, because the software did not give reasonable results (The wall shear stress on practically all surface was zero). In addition, it is possible notice from the results that diastolic pressure is low, less than 55 mmHg. These low diastolic pressures probably were results from three assumptions to get RCR values using SimVascular. It was necessary set: blood flow target for outlets and inlet, mean arterial pressure for inlet and outlets and always use the same blood flow rate at inlet for all patient to get initial RCR values and run the computational fluid simulation. Thus, it is important improve the process of calculation of RCR parameters in order to get a more realistic range of pressure during a cardiac cycle.
Results from hemodynamics simulation at common carotid artery show that diseased carotid artery is exposed to higher WSS. The pressure wave of diseased carotid artery is modified, which results in slightly higher diastolic and systolic pressure. However, not all the hemodynamic changes can be exclusively attributed to stenosis. There are others relevant factors, such as diameter, tortuosity, pulse pressure and mean arterial pressure.

Diseased carotid artery is submitted to higher stress and pressure. In addition, the branches of common carotid artery are exposed to plaque formation due low blood velocity and zones of disturbed flow. CFD simulation is an important tool to study hemodynamic of arterial diseases and development of a patient specific methodology to predict and prevent disease progression.
References
[1] Biofluid Mechanics: Blood Flow in Large Vessels, vol. 11. Springer Science & Business Media, 2013.
[2] Biofluid Mechanics: Blood Flow in Large Vessels, vol. 11. Springer Science & Business Media, 2013.
[4] “Atherosclerosis: Types, Causes & Symptoms.” [Online]. Available: http://www.healthline.com/health/atherosclerosis#ReadThisNext0. [Accessed: 21-Jun-2015].
[5] Biofluid Mechanics: Blood Flow in Large Vessels, vol. 11. Springer Science & Business Media, 2013.
[6] Biofluid Mechanics: Blood Flow in Large Vessels, vol. 11. Springer Science & Business Media, 2013.
[7] Biofluid Mechanics: Blood Flow in Large Vessels, vol. 11. Springer Science & Business Media, 2013.
[8] H. Gharahi, B. A. Zambrano, D. C. Zhu, J. K. DeMarco, and P. D. Seungik Baek, “Computational fluid dynamic simulation of human carotid artery bifurcation based on anatomy and blood flow velocity measured with magnetic resonance imaging --Manuscript Draft-,” Int. J. Adv. Eng. Sci. Appl. Math. Comput., pp. 1–9, 2013.
[9] P. C. Johnson, “Brief Review Autoregulation of Blood Flow,” Circ. Res., pp. 483–495, 1986.
[10] “CV Physiology: Autoregulation.” [Online]. Available: http://www.cvphysiology.com/Blood Flow/BF004.htm. [Accessed: 13-Jul-2015].
[11] M. J. Cipolla, “Control of Cerebral Blood Flow.” Morgan & Claypool Life Sciences, 2009.
[12] Steinman, D.A., 2012. Assumptions in modelling of large artery hemodynamics. In: Modeling of Physiological Flows. Springer, pp. 1–18.
[13] Biofluid Mechanics: Blood Flow in Large Vessels, vol. 11. Springer Science & Business Media, 2013.