Hemodialysis and Hemofiltration in Pediatrics: An Approach to Intoxication Karen Papez MD University...
23
Hemodialysis and Hemodialysis and Hemofiltration in Hemofiltration in Pediatrics: An Pediatrics: An Approach to Approach to Intoxication Intoxication Karen Papez MD Karen Papez MD University of Michigan University of Michigan Pediatric Nephrology, Pediatric Nephrology, Dialysis & Dialysis & Transplantation Transplantation 3rd annual PCRRT, 3rd annual PCRRT, Orlando, FL Orlando, FL
-
Upload
osborn-owens -
Category
Documents
-
view
226 -
download
4
Transcript of Hemodialysis and Hemofiltration in Pediatrics: An Approach to Intoxication Karen Papez MD University...

Hemodialysis and Hemodialysis and Hemofiltration in Hemofiltration in
Pediatrics: An Approach Pediatrics: An Approach to Intoxicationto Intoxication
Karen Papez MDKaren Papez MD
University of MichiganUniversity of Michigan
Pediatric Nephrology, Dialysis & Pediatric Nephrology, Dialysis & TransplantationTransplantation
3rd annual PCRRT, Orlando, FL 3rd annual PCRRT, Orlando, FL

2002 Annual Report of American 2002 Annual Report of American Association of Poison Control Association of Poison Control
CentersCenters Nearly 2.4 million human exposures reported Nearly 2.4 million human exposures reported
by 64 participating poison centers in 2002.by 64 participating poison centers in 2002. 4.9% increase from 20014.9% increase from 2001
Children <3 yrs: 39% of all human exposuresChildren <3 yrs: 39% of all human exposures Children <6 yrs: 51.6% of all exposuresChildren <6 yrs: 51.6% of all exposures
*Pediatricians and pediatric subspecialists *Pediatricians and pediatric subspecialists need to be prepared to handle the need to be prepared to handle the majority of poison exposures.majority of poison exposures.
Watson WA et al. Am J Emerg Med 21: 2003Watson WA et al. Am J Emerg Med 21: 2003 Litovitz TL et al. Am J Emerg Med 20: 2002Litovitz TL et al. Am J Emerg Med 20: 2002

Enhanced Elimination Techniques Enhanced Elimination Techniques for Poisoningsfor Poisonings
Enhanced elimination techniques were used Enhanced elimination techniques were used for 1457 cases (0.06%) in 2002.for 1457 cases (0.06%) in 2002. A near 8% increase over 2001 reportsA near 8% increase over 2001 reports
Hemodialysis: 1400 [up 9% from 2001]Hemodialysis: 1400 [up 9% from 2001] Hemoperfusion: 30 [down 33% from 2001]Hemoperfusion: 30 [down 33% from 2001] Other Extracorporeal Procedures: 27Other Extracorporeal Procedures: 27
*Pediatric nephrologists and intensivists *Pediatric nephrologists and intensivists need to be equipped with advanced need to be equipped with advanced techniques to handle such clinical techniques to handle such clinical situations.situations.

Treatment Measures AvailableTreatment Measures Availablefor Poisoningsfor Poisonings
Enhance Elimination (Cont.)Enhance Elimination (Cont.)Extracorporeal MethodsExtracorporeal Methods
HemodialysisHemodialysisStandardStandardHigh Efficiency/High FluxHigh Efficiency/High Flux
HemofiltrationHemofiltrationHemoperfusionHemoperfusionExchange TransfusionExchange TransfusionPlasma exchangePlasma exchange

Toxin ClearanceToxin Clearance
What effects clearance?What effects clearance?Volume of distributionVolume of distributionWhether or not the drug is primarily renally Whether or not the drug is primarily renally
excreted (competing pathways)excreted (competing pathways)Protein bindingProtein bindingMolecular size of the drugMolecular size of the drugMode of therapy-HD, CVVH vs CVVHD vs Mode of therapy-HD, CVVH vs CVVHD vs
CVVHDFCVVHDFHemofilter membrane propertiesHemofilter membrane properties
Pond, SM - Med J Australia 1991; 154: 617-622Pond, SM - Med J Australia 1991; 154: 617-622

HEMODIALYSISHEMODIALYSISOptimal drug characteristics for removal:Optimal drug characteristics for removal:
Relative molecular mass < 500 DaltonsRelative molecular mass < 500 DaltonsWater solubleWater solubleSmall Vd (< 1 L/Kg)Small Vd (< 1 L/Kg)Minimal plasma protein bindingMinimal plasma protein bindingSingle compartment kineticsSingle compartment kineticsLow endogenous clearance (< 4ml/Kg/min)Low endogenous clearance (< 4ml/Kg/min)
Pond, SM - Med J Australia 1991; 154: 617-622Pond, SM - Med J Australia 1991; 154: 617-622

HEMOFILTRATIONHEMOFILTRATIONOptimal drug characteristics for removal:Optimal drug characteristics for removal:
Relative molecular mass less than the cut-off of the Relative molecular mass less than the cut-off of the filter fibres (usually < 40,000 daltons)filter fibres (usually < 40,000 daltons)
Small Vd (< 1 L/Kg)Small Vd (< 1 L/Kg)Single compartment kineticsSingle compartment kineticsLow endogenous clearance (< 4ml/Kg/min)Low endogenous clearance (< 4ml/Kg/min)
Pond, SM - Med J Australia 1991; 154: 617-622Pond, SM - Med J Australia 1991; 154: 617-622

Additional Factors when Additional Factors when Considering Enhanced Elimination Considering Enhanced Elimination
MethodsMethodsDrug kinetics should be reviewedDrug kinetics should be reviewed
Note: Kinetics may differ in an overdose Note: Kinetics may differ in an overdose situationsituationValproic acid: 90% protein bound with nl levelsValproic acid: 90% protein bound with nl levelsValproic acid: 70% bound at levels of 135 mcg/mlValproic acid: 70% bound at levels of 135 mcg/ml
: 35% bound at levels of 300 mcg/ml: 35% bound at levels of 300 mcg/ml
*The higher the levels and the more *The higher the levels and the more unbound drug that exists, the more unbound drug that exists, the more effectively it may be removed.effectively it may be removed.

Case 1Case 1
14 year old female with history of 14 year old female with history of depression, found slurring words, depression, found slurring words, intermittently confused in her bedroom.intermittently confused in her bedroom.
During period of lucency, told mother she During period of lucency, told mother she drank something a schoolmate gave her to drank something a schoolmate gave her to “get high.” States this was 18 hours “get high.” States this was 18 hours before presentation to local ER.before presentation to local ER.

Physical Exam at Admission to Physical Exam at Admission to PICUPICU
T 38.8 P 125 RR 32 BP 158/75 Wt 75 KgT 38.8 P 125 RR 32 BP 158/75 Wt 75 KgGenerally: GCS variable, from verbal Generally: GCS variable, from verbal
response to voice to mild response to pain.response to voice to mild response to pain.HEENT: Pupils equally round, sluggishly HEENT: Pupils equally round, sluggishly
reactive to light, mucous membranes dryreactive to light, mucous membranes dryResp: Deep, tachypneic, clear to auscultationResp: Deep, tachypneic, clear to auscultationCV: RRR, no murmur, peripheral pulses 2/4CV: RRR, no murmur, peripheral pulses 2/4Abd: Soft, nondistended, hypoactive bowel Abd: Soft, nondistended, hypoactive bowel
soundssounds

Laboratory AnalysesLaboratory Analyses 148 121 13 98148 121 13 98
5.4 7 2.15.4 7 2.1
9.4 38 0.39.4 38 0.3
4.8 4.0 59 1434.8 4.0 59 143
11.7 11.7 16.816.8 163 163
50.450.4
7.24 / 18 / 113 / 87.24 / 18 / 113 / 8
UA SG 1.015, pH 5, normal for UA SG 1.015, pH 5, normal for all substratesall substrates
AG AG 2020
Calc osm Calc osm 306306
Serum osm Serum osm 311311
CPK 388CPK 388
NHNH33 38 38
Ethanol negativeEthanol negative
Urine drug screen Urine drug screen negativenegative
ββhCG negativehCG negative
Salicylate <1Salicylate <1
Acetaminophen <10Acetaminophen <10
Ethylene glycol Ethylene glycol 24.224.2

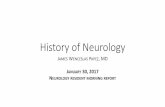
Calculated Osmolality with Dialysis Calculated Osmolality with Dialysis in Ethylene Glycol Intoxicationin Ethylene Glycol Intoxication
275
295
315
24 27 34 36 40 53
Hours After Ingestion
Osm
ola
lity
(m
osm
/K)
CalculatedosmolalitySerumosmolality
HD Started
CVVHDF Started
CT-190
Prisma dialyzer Multiflo-100
BFR -HD 250 ml/min
-CVVHDF 180 ml/min
PO4 based dialysate
- 4L/1.73m2/hr

Case 2Case 2
12 year old female with history of bipolar 12 year old female with history of bipolar disorder had started an increased dose of disorder had started an increased dose of lithium 6 weeks prior to admission.lithium 6 weeks prior to admission.
Was slurring her speech on morning of Was slurring her speech on morning of admission, and had irregular constant admission, and had irregular constant movements of her arms and legs.movements of her arms and legs.

Physical Exam at Admission to Physical Exam at Admission to PICUPICU
T afebrile P 82 RR 23 BP 104/46 Wt 33 KgT afebrile P 82 RR 23 BP 104/46 Wt 33 Kg Generally: Confused, slurring speechGenerally: Confused, slurring speech HEENT: NC, AT, Mucous membranes moistHEENT: NC, AT, Mucous membranes moist Resp: Clear to auscultationResp: Clear to auscultation CV: Regular rate and rhythm, no murmurCV: Regular rate and rhythm, no murmur Abdomen: Soft, normoactive bowel soundsAbdomen: Soft, normoactive bowel sounds Skin: Erythematous rash over abdomenSkin: Erythematous rash over abdomen Neuro: Athetoid movements as noted in HPINeuro: Athetoid movements as noted in HPI

Laboratory AnalysesLaboratory Analyses 133133 107 31 73 107 31 73 4.3 22 1.24.3 22 1.2 6.8 6.8 7.0 35 0.6 7.0 35 0.6
4.1 25 2154.1 25 215
10.5 12.1 17610.5 12.1 176 34.434.4
7.36 / 50 / 28 / 287.36 / 50 / 28 / 28UA SG 1.010, pH 6.5, UA SG 1.010, pH 6.5, pro 1+, ket pro 1+, ket
2+, LE 1+,2+, LE 1+, otherwise normal otherwise normal
AG 4AG 4CPK CPK 939939NHNH33 38 38Ethanol and volatile acids Ethanol and volatile acids
negative negativeUrine drug screen Urine drug screen
negativenegativeββhCG negativehCG negativeSalicylate <1Salicylate <1Acetaminophen <10Acetaminophen <10Lithium Lithium 7.347.34EKG EKG First degree heart First degree heart
block, PR 188 ms, block, PR 188 ms, prolonged QTc 520 msprolonged QTc 520 ms

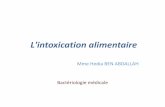
Lithium Clearance on DialysisLithium Clearance on Dialysis
0
1
2
3
4
5
6
7
8
0 3 4 5 6 11 15 20 23 25 30 33 36
Time After Presentation (Hours)
Lit
hiu
m C
on
cen
trat
ion
(m
Eq
/L) Lithium
CVVHD Started
HD Started CVVHD
Stopped
CT-190Prisma dialyzer Multiflo-100BFR -HD 250 ml/min -CVVHDF 180 ml/minPO4 based dialysate - 4L/1.73m2/hr

Lithium Redistributes from Intracellular Lithium Redistributes from Intracellular Compartment: Compartment:
Arrows indicate beginning and end of HD. A significant rebound in serum concentration occurred after a 5-hr HD treatment with recurrence of neurologic impairment. An
additional 4-hour hemodialysis treatment was then begun. From Goldfarb DS in Goldfrank’s Toxologic Emergencies, 7th Ed. 2002
Hemofiltration May Attenuate Rebound Phenomenon!

0
2
4
6
8
10
Hours After Presentation
Lit
hiu
m c
once
ntr
atio
n (
mE
q/L
)
Pt #1Pt #2Pt #3
CVVHD Following HD for Lithium Poisoning
HD started
CVVHD startedCT-190 (HD)Prisma dialyzer -Multiflo-60 (#1,2) -Multiflo-100 (#3)BFR- HD -pt # 1 200 ml/min -pt # 2 325 ml/min -pt # 3 250 ml/minBFR- CVVHD 200 ml/min - All 3 pts.PO4 Based dialysate at
2L/1.73m2/hr (#1,2) 4L/1.73m2/hr (#3)
Li Therapeutic range0.5-1.5 mEq/L

DrugDrug MWMW
[Daltons][Daltons]
H2O H2O SolSol
% Prot % Prot BoundBound
Vol of Distrib Vol of Distrib [L/kg][L/kg]
Endogenous Endogenous ClearanceClearance
LithiumLithium 77 YesYes 00 0.6-1.00.6-1.0 0.4 ml/min/kg0.4 ml/min/kg
MethanolMethanol 3232 YesYes 00 0.70.7 0.7 ml/min/kg0.7 ml/min/kg
Ethylene Ethylene GlycolGlycol
6262 YesYes 00 0.60.6 2.0 ml/min/kg2.0 ml/min/kg
SalicylatesSalicylates 138138 YesYes 90%*90%* 0.15-0.20.15-0.2 0.88 ml/min/kg0.88 ml/min/kg
Valproic acidValproic acid 144144 NoNo 90%*90%* 0.19-0.23 0.19-0.23 TotTot
1.3 1.3 FreeFree
0.13 ml/min/kg0.13 ml/min/kg
1.1 ml/min/kg1.1 ml/min/kg
TheophyllineTheophylline 180180 YesYes 55%55% 0.4-0.70.4-0.7 0.65 ml/min/kg 0.65 ml/min/kg
PhenobarbPhenobarb 232232 NoNo 24-60%24-60% 0.50.5 0.1 ml/min/kg0.1 ml/min/kg
Carbamaz-Carbamaz-epineepine
236236 NoNo 75%75% 0.8-1.60.8-1.6 1.3 ml/min/kg1.3 ml/min/kg
VancomycinVancomycin 14861486 YesYes 10-50%10-50% 0.47-1.10.47-1.1

Conclusions Conclusions
High efficiency hemodialysis and High efficiency hemodialysis and hemofiltration may alter the current hemofiltration may alter the current “treatment of choice”. “treatment of choice”.
Pediatric nephrologists need to be aware Pediatric nephrologists need to be aware
that more than one treatment option exists that more than one treatment option exists for many toxicology situations, and the for many toxicology situations, and the modality selected should be that tailored to modality selected should be that tailored to their patient’s needs. their patient’s needs.

ACKNOWLEDGEMENTSACKNOWLEDGEMENTSTHERESA MOTTESTHERESA MOTTESTIM KUDELKATIM KUDELKABETSY ADAMSBETSY ADAMSTAMMY KELLYTAMMY KELLYROBIN NIEVAARDROBIN NIEVAARDDAVID KERSHAWDAVID KERSHAWPATRICK BROPHYPATRICK BROPHY

OTHER ISSUESOTHER ISSUESOptimal prescriptionOptimal prescriptionBiocompatible filters - may increase protein Biocompatible filters - may increase protein
adsorptionadsorptionMaximal blood flow rates (i.e. good access)Maximal blood flow rates (i.e. good access)Physiological solution (ARF vs non ARF)Physiological solution (ARF vs non ARF)Potential removal of antidotePotential removal of antidoteCounter-current dialysate maximal removal of Counter-current dialysate maximal removal of
toxinstoxins

Specific AntidotesSpecific Antidotes
Should be used adjunctively with supportive Should be used adjunctively with supportive therapy.therapy.
ExamplesExamples:: N-acetyl cysteine N-acetyl cysteine [for Acetaminophen][for Acetaminophen] Benzodiazepines Benzodiazepines [for Flumazenil][for Flumazenil]
Flumazenil Flumazenil [for Benzodiazepines][for Benzodiazepines] Naloxone Naloxone [for Opiates][for Opiates] Calcium Calcium [for Calcium channel blockers][for Calcium channel blockers] Atropine Atropine [for Acetylcholinesterase inhibitors][for Acetylcholinesterase inhibitors] Fomepizole Fomepizole [for Ethylene glycol, Methanol, & Diethylene [for Ethylene glycol, Methanol, & Diethylene
Glycol] Glycol] Ethanol Ethanol [for Ethylene glycol, Methanol, & Diethylene Glycol][for Ethylene glycol, Methanol, & Diethylene Glycol]