SAEMSsaemscouncil.com/wp-content/uploads/2014/12/AbdominalPainSLP109… · hematuria or melena...
17
SAEMS ABDOMINAL PAIN STANDING ORDER Self-Learning Module Mary Ann Matter University Medical Center January 27, 2009
Transcript of SAEMSsaemscouncil.com/wp-content/uploads/2014/12/AbdominalPainSLP109… · hematuria or melena...
SAEMSABDOMINAL PAIN STANDING ORDER
Self-Learning Module
Mary Ann MatterUniversity Medical Center
January 27, 2009

SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
2
PURPOSE
This SAEMS Standing Order Training Module has been developed to serve as atemplate for EMS provider training. The intent is to provide consistent andconcise information to all providers practicing within the SAEMS Region. Thecontent of the Training Module has been reviewed by the Protocol Developmentand Review Sub-Committee, and includes the specific standing order, resourceand reference material, and instructions for completing the Training Module toobtain continuing education credit. One hour of SAEMS continuing educationcredit may be issued following successful completion of the module.
OBJECTIVES
Upon completion of this learning module the participant will be able to:
1. Review basic abdominal evaluation techniques
2. Recognize life-threatening abdominal pathology
3. Apply the Abdominal Pain Standing Order appropriately
INSTRUCTIONS
1. Watch the Power Point presentation. Review the accompanying information,Standing Order, and any additional reference material as necessary.
2. Complete the attached posttest by and return it to your supervisor or basehospital manager:
3. A SAEMS CE Form will be issued to providers scoring greater than ____%on the Posttest.
TABLE OF CONTENTS
1. Purpose 22. Objectives 23. Instructions 24. Table of Contents 25. Introduction 36. Abdominal Pain 37. Glossary 88. Standing Order 109. Ondansetron Profile 1110. Posttest 1311. References 1612. Evaluation 17

SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
3
INTRODUCTION
The Abdominal Pain Standing Order was originally developed in 2005, inresponse to an increasing number of patients presenting with the chief complaintof abdominal discomfort. Although the abdominal cavity contains most of ourinternal organs and is responsible for a multitude of physiologic processes,recognition and management of the acute, life-threatening case is fairlystraightforward for the EMS provider.
ABDOMINAL PAIN
Incidence
The complaint of abdominal pain is a common one. It is however, one of the mostdifficult conditions to diagnose and treat. Fortunately, EMS providers are notexpected to diagnose, but are expected to assess, recognize, and treat thepatient with an acute abdominal condition.
Abdominal pain represents approximately five to ten percent of all emergencydepartment visits, many of which arrive by ambulance. The symptoms ofabdominal pain can be associated with transient, mild disorders or seriousdisease, but determining the cause is very difficult. Pain may be the onlyindication of the need for surgery, with fifteen to thirty percent of abdominal painpatients requiring immediate surgical intervention. Fortunately, the majority ofpatients with the complaint of abdominal pain will not experience a catastrophicevent.
Most complaints of abdominal pain and the associated symptoms of nausea,vomiting, and diarrhea arise from problems within the abdomen itself. Acute andsevere abdominal pain is almost always a symptom of intraabdominal disease.However, ten to fifteen percent of abdominal pain originates from outside theabdomen such as; lumbar spine fracture, myocardial infarction, pulmonaryembolism, and pneumonia, yet the primary complaint is abdominal pain.
As a prehospital provider it is not necessary to identify the cause, but torecognize the basic signs of serious conditions, and to provide necessaryinterventions and transportation. The patient with an acute abdomen candeteriorate quickly, requiring frequent reassessment and rapid transportation.
Abdominal Pathology
Several organ systems (gastrointestional, genitourinary, circulatory, andreproductive) are found in the abdomen; it is the largest body cavity. Pain in theabdomen can be a symptom of inflammation, disease, injury, or organdysfunction. Associated symptoms such as nausea, vomiting, anorexia,hematuria or melena usually indicate a serious problem. The “acute abdomen”

SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
4
refers to the sudden onset of abdominal pain that is often associated with othersigns and symptoms such as nausea, vomiting, anorexia, and tenderness topalpation upon physical examination. Many of the conditions that produce anacute abdomen can result in death if not recognized and treated early.
The “acute abdomen” can be defined as: An intraabdominal process of recentonset (up to three days) causing severe pain and often requiring surgicalintervention. This may be caused by one or more of the following conditions:
Inflammatory process (appendicitis)Mechanical process (incarcerated hernia)Vascular occlusion (mesenteric arterial thrombosis)Congenital defect (omphalocele)Traumatic event (ruptured spleen)
Abdominal emergencies can be divided into gastrointestional, genitourinary, orreproductive system emergencies. It is difficult for the prehospital provider todetermine the source of the abdominal problem in the field, therefore theapproach to managing the patient with acute abdominal pain should beconsistent regardless of the system involved.
Following is a list of some conditions which may result in acute abdominaldiscomfort requiring rapid, life-saving surgical intervention:
• Bleeding Esophageal Varices• Abdominal Aortic Aneurysm• Ruptured Ectopic Pregnancy• Perforated Ulcer• Abdominal Trauma• Appendicitis• Incarcerated Hernia• Peritonitis• Intestinal Obstruction• Mesenteric Infarction
Prehospital providers should consider the possibility of a gastrointestionalhemorrhage in any patient with acute abdominal pain, especially if syncope hasoccurred or evidence of blood loss (shock) is present. Severe pain that precedesthe onset of vomiting and lasts longer than six hours is likely to be caused by asurgically correctable illness.
Abdominal Assessment
Begin the assessment with airway breathing and circulation, skin color, condition,and temperature. Determine the patient’s level of consciousness and obtainbaseline vital signs. If the patient presents with fever, shock, hemorrhage,

SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
5
dehydration, or cardiac decompensation then a rapid survey with immediatetransport would be prudent.
Prehospital providers should inquire about Allergies, Medications, Past medicalhistory, Last oral intake and the Events leading up to the present illness.Assessing the characteristics of pain is essential in any patient complaining ofpain, but particularly in the patient with abdominal pain.
Pain Assessment
There are three patterns of pain that are associated with the abdomen; visceral,somatic, and referred. Since pain is the most prominent presenting complaint inthe patient with an acute abdomen, it is helpful to understand the origin, location,and character of abdominal pain in order to understand its significance.
Visceral pain originates from the stretched muscle fibers in the wall of a holloworgan, spasm of these muscles, or stretching of the capsule of the organ when itattempts to relieve an obstruction. It is usually the first type of pain experienced.The sensory supply to the viscera is sparse and although visceral pain can besevere, it is diffuse and poorly localized. Visceral pain is often associated withnausea and vomiting. The intermittent quality of the pain with obstruction of ahollow viscus coincides with the peristaltic waves of the organ and can bedescribed as colicky. Patients appear restless attempting to find some relief withwrithing and massage of the affected area.
Visceral pain is followed by somatic pain. The parietal peritoneum lines theabdominal cavity and the interior surface of the diaphragm. The peritoneumbecomes irritated when there has been bacterial invasion due to a rupturedviscus (i.e., perforated peptic ulcer), bleeding into the cavity (i.e., trauma), anextending infection (i.e., pelvic inflammatory disease), or through an ischemicprocess (i.e., mesenteric occlusion). When the parietal peritoneum is irritated,somatic pain results. Somatic pain is more localized and can be sharp andconstant. It is usually aggravated by movement. These patients are typicallyhunched over and immobile.
Pain experienced at a site other than where the local irritation is occurring istermed referred pain. The overlapping sensory nerves in the spinal cord result inpain being felt in two areas. Pain can also radiate to distant sites, such as theright scapula with acute cholecystitis, or pain that originates in the flank andradiates to the groin suggesting renal colic.
Obtaining a thorough history of the patient’s pain is also important in determiningthe pathophysiologic alterations contributing to the pain, and in makingjudgments about appropriate supportive measures such as the implementation ofthe Abdominal Pain Standing Order. Many practitioners find the followingmnemonic helpful in evaluating pain:

SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
6
O = onset: When did the pain begin? Was it sudden orgradual?
P = provocation: What initiates or aggravates the pain? Whatmakes it better? Is it aggravated by position?
Q = quality: What is the patient’s own description of thepain? Dull, sharp, crampy, burning, tearing
R = region: Where does the pain originate? radiation: Is it felt in other areas? referred: Does it travel to other areas?S = severity (pain scale): What is the degree of discomfort on a scale of
1to10?T = timing: Is the pain constant or intermittent? Does it
occur or resolve in relation to meals?
Associated Symptoms
Inquire about associated symptoms such as fever, nausea and vomiting,diarrhea, constipation, and anorexia. An infectious process may result in anelevated temperature. Acute appendicitis often causes anorexia, and bowelobstructions often lead to vomiting. Remember that age and gender can providehelpful hints as well. Abdominal pain in babies is usually indicative of atresia,hernia or stenosis. In children it may be an intussuseption, hernia orappendicitis. Females could be suffering from cholecystitis, an ectopicpregnancy, or from pelvic inflammatory disease (PID). Males more commonlysuffer from ulcers than do females. A geriatric patient might present withmesenteric emboli following the onset of atrial fibrillation, or a bowel obstructiondue to adhesions from a prior abdominal surgery. Always ask about prior diseaseor surgeries. Pain that awakens the patient from sleep usually indicatessignificant disease.
Physical Exam
Assessment of the abdomen during the secondary survey begins by observingthe patient, preferably in a supine position with the knees bent to reduce intra-abdominal pressure. Look for any scars, rashes, lesions, bruising, discolorationor indications of ascites. Observe the symmetry of the abdomen and look at theshape. If a pulsatile mass is observed, it may be indicative of an abdominal aorticaneurysm (AAA), which could potentially rupture if palpated. Patients with apalpable, pulsating mass should be immediately transported to the closesthospital capable of rapid surgical intervention.
Auscultation of the abdomen typically follows inspection because the bowel issensitive to touch, and bowel sounds are best evaluated prior to palpation.Percussion determines the presence of gas or fluid in the hollow organs or in theperitoneal cavity. It is also performed to determine the size of an enlarged organ

SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
7
(spleen or liver) or an intraabdominal mass. In the prehospital environmentauscultation and percussion are two abdominal assessment techniques whichare rarely performed.
Establish the location of the pain by having the patient point to the area mosttender. Begin palpating from the furthest quadrant away from the pain. Palpateeach quadrant by placing one (warm) hand on the abdomen and applying gentlepressure with the other hand over the top of the first. Note if the abdomen is softor firm, and if there is increased pain when pressure is applied (pointtenderness), if the patient tenses (guarding), or if the pain increases when rapidlyreleasing your hands (rebound tenderness).
Management
The SAEMS Abdominal Pain Standing Order may be considered for patientsgreater than 16 years of age who complain of abdominal pain. All patients shouldbe managed with immediate supportive care to include oxygen and cardiacmonitoring as appropriate. The following list includes the Abdominal PainStanding Order exclusionary conditions which require medical direction authoritycontact:
• Pregnancy: These patients may often be transported directly to a laborand delivery in-patient unit, bypassing the emergency department.Telemetry information regarding gestational age, complications, etc. isimportant in making destination decisions.
• Trauma triage criteria: Patients who meet the SAEMS Trauma TriageProtocol criteria are not eligible for standing order usage. A full telemetryreport to the trauma center is required.
• Abdominal trauma: Isolated blunt injury to the abdomen carries with it ahigh likelihood of severe intraabdominal injury. Consultation with a medicaldirection authority is suggested.
• Mixed symptoms: Abdominal pain associated with other complicatingfindings such as; chest pain, shortness of breath, or an altered level ofconsciousness would prohibit the use of the standing order.
• Known history of cardiac disease: Abdominal pain may sometimes be thepresenting complaint of an extraabdominal event such as myocardialinfarction.
After determining that the Abdominal Pain Standing Order is appropriate, theblood pressure and heart rate next define whether the patient iscategorized as stable or unstable. For the stable patient with a blood pressuregreater than 90 systolic and a heart rate less than 110, pain assessment andtransportation in a position of comfort with supportive measures is indicated. Theunstable abdominal pain patient presents with a blood pressure less than 90systolic and a heart rate greater than 110. These patients require a fluid bolus ofnormal saline and the administration of intravenous ondansetron for nausea or

SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
8
vomiting. Medication to address the pain requires an on-line order. Alwaysreassess after each intervention.
Communication
As with any standing order, the receiving facility requires certain information toallow them to prepare for the patient’s arrival. Relay the following essentialinformation to the hospital:
• Age• Sex• Abdominal Pain Standing Order• Transporting Unit• Estimated Time of Arrival• Stable or Unstable patient
This information will maintain continuity of care and facilitate patient transferupon arrival.
Summary
Acute abdominal distress may be the result of conditions involving severaldifferent organ systems. According to some references there are approximatelyone hundred different causes of abdominal pain. The expectation of the fieldprovider is not to diagnose, but to recognize and manage those potentially life-threatening conditions in patients complaining of abdominal pain. The SAEMSAbdominal Pain Standing Order has been developed to allow providers thefreedom to assess and transport these patients with consistency in managementand minimal interruption in patient care.
GLOSSARY
Ascites: the accumulation of serous fluid in the peritoneal cavity typically causedby liver disease.Atresia: an abnormal condition in which a normal opening or tube in the body isclosed or absent.Cholecystitis: inflammation of the gallbladder.Hematuria: the presence of blood in the urine.Incarcerated Hernia: a hernia (a breakthrough of an organ through a tear in themuscle wall that surrounds it) that cannot be reduced without surgery.Intussuseption: the telescoping of a length of intestine into an adjacent portionusually producing an obstruction.Mesenteric Arterial Thrombosis: the formation of a blood clot inside amesenteric blood vessel, obstructing the flow of blood.Mesenteric Emboli: the migration of a clot that blocks a mesenteric blood vesselsupplying the bowel.

SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
9
Omphalocele: a congenital abdominal wall defect in which the intestines, liver,and occasionally other organs remain outside of the abdomen in a sac due to adefect in the development of the muscles of the abdominal wall.Pelvic Inflammatory Disease: inflammation of the female reproductive pelvicorgans.Stenosis: a constriction or narrowing of a duct or passage.
SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
10
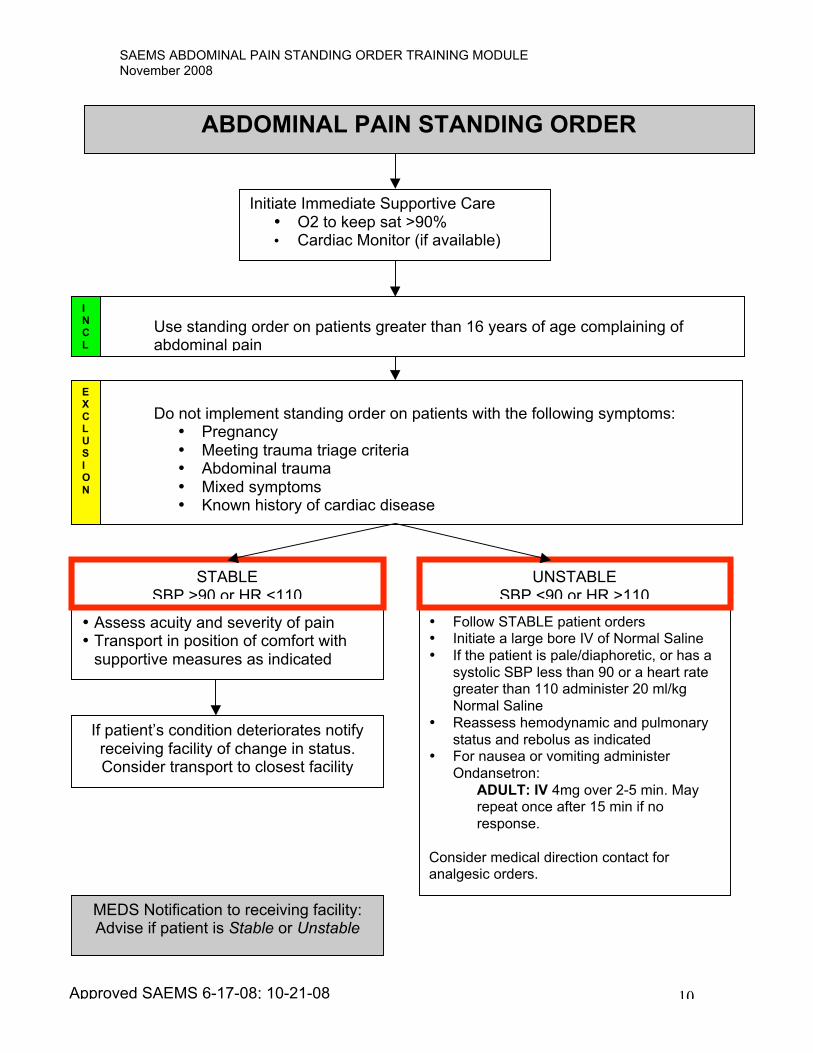
ABDOMINAL PAIN STANDING ORDER
Initiate Immediate Supportive Care• O2 to keep sat >90%• Cardiac Monitor (if available)
Use standing order on patients greater than 16 years of age complaining ofabdominal pain
MEDS Notification to receiving facility:Advise if patient is Stable or Unstable
Do not implement standing order on patients with the following symptoms:• Pregnancy• Meeting trauma triage criteria• Abdominal trauma• Mixed symptoms• Known history of cardiac disease
INC
L
EX
CLU
SIO
N
• Assess acuity and severity of pain• Transport in position of comfort with
supportive measures as indicated
• Follow STABLE patient orders• Initiate a large bore IV of Normal Saline
• If the patient is pale/diaphoretic, or has a
systolic SBP less than 90 or a heart rategreater than 110 administer 20 ml/kg
Normal Saline
• Reassess hemodynamic and pulmonary
status and rebolus as indicated• For nausea or vomiting administer
Ondansetron:
ADULT: IV 4mg over 2-5 min. Mayrepeat once after 15 min if no
response.
Consider medical direction contact foranalgesic orders.
STABLESBP >90 or HR <110
UNSTABLESBP <90 or HR >110
If patient’s condition deteriorates notifyreceiving facility of change in status.Consider transport to closest facility
Approved SAEMS 6-17-08; 10-21-08
SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
11
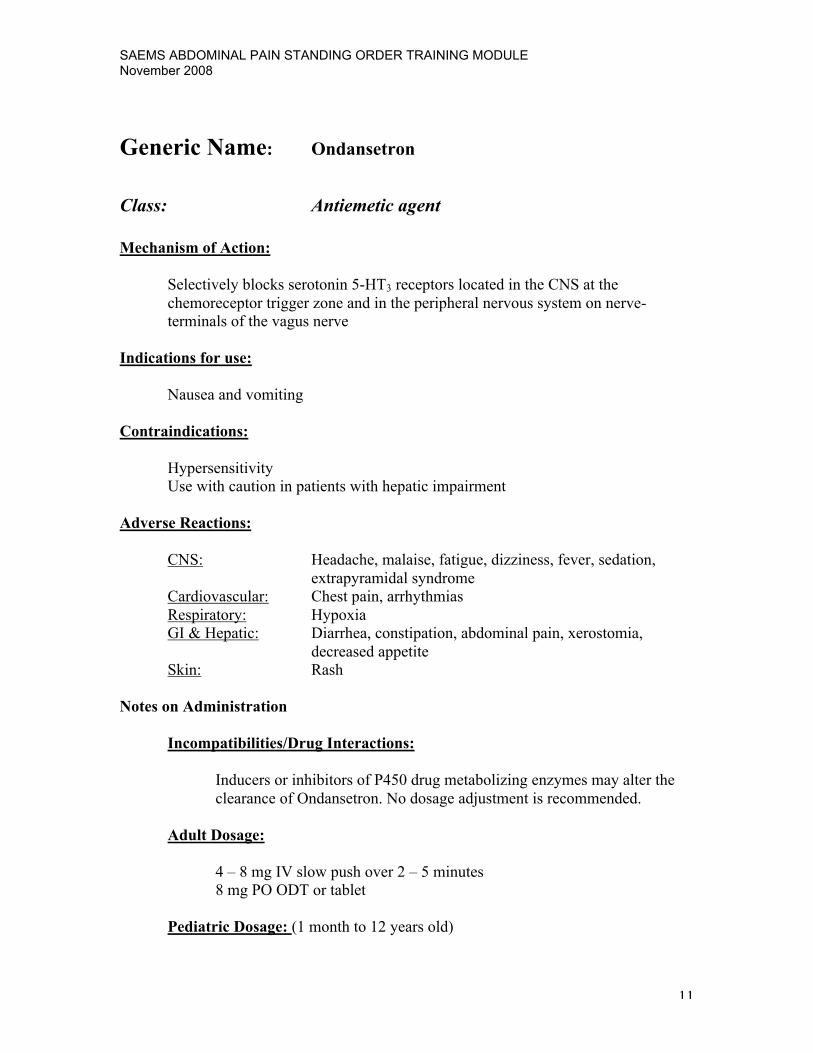
Generic Name: Ondansetron
Class: Antiemetic agent
Mechanism of Action:
Selectively blocks serotonin 5-HT3 receptors located in the CNS at the
chemoreceptor trigger zone and in the peripheral nervous system on nerve-
terminals of the vagus nerve
Indications for use:
Nausea and vomiting
Contraindications:
Hypersensitivity
Use with caution in patients with hepatic impairment
Adverse Reactions:
CNS: Headache, malaise, fatigue, dizziness, fever, sedation,
extrapyramidal syndrome
Cardiovascular: Chest pain, arrhythmias
Respiratory: Hypoxia
GI & Hepatic: Diarrhea, constipation, abdominal pain, xerostomia,
decreased appetite
Skin: Rash
Notes on Administration
Incompatibilities/Drug Interactions:
Inducers or inhibitors of P450 drug metabolizing enzymes may alter the
clearance of Ondansetron. No dosage adjustment is recommended.
Adult Dosage:
4 – 8 mg IV slow push over 2 – 5 minutes
8 mg PO ODT or tablet
Pediatric Dosage: (1 month to 12 years old)

SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
12
Greater than 40 kg- 4 mg IV slow push over 2 – 5 minutes
Less than 40 kg- 0.1 mg/kg IV slow push over 2 – 5 minutes
4-12 years old 4 mg PO ODT or ODT
Route of Administration:
IV, IM, PO
Onset of Action:
Unknown but probably 10 to 30 minutes
Peak effects:
Unknown
Duration of Action:
Half life is approximately 4 hours. Exact duration unknown but appears to
be prolonged compared to half-life
Dosage Forms/Packaging:
4 mg/2 mL vial
4 or 8 mg ODT or tablet
Arizona Drug Box Standard Minimum Supply:
Optional- 4 mg
Special Notes:
Instructions for Use/Handling ZOFRAN ODT Orally Disintegrating
Tablets: Do not attempt to push ZOFRAN ODT Tablets through the foil
backing. With dry hands, PEEL BACK the foil backing of 1 blister and GENTLY
remove the tablet. IMMEDIATELY place the ZOFRAN ODT Tablet on top of
the tongue where it will dissolve in seconds, then swallow with saliva.
Administration with liquid is not necessary.
Bottles: Store between 2°and 30°C (36° and 86°F). Protect from light.
Dispense in tight, light-resistant container as defined in the USP.
Unit Dose Packs: Store between 2° and 30°C (36°and 86°F). Protect from
light. Store blisters in cartons.

SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
13
POSTTEST NAME: DATE:
1. Which of the following conditions are exclusion criteria for the AbdominalPain Standing Order?
a. Pregnancy, abdominal trauma, mixed symptoms, known history ofcardiac disease.
b. Patient with severe abdominal pain on-and-off for 6 months withassociated weight loss.
c. Patient with severe abdominal pain for less than 4 hours associatedwith vomiting.
d. 17-year-old female who complains of abdominal cramps.
2. Patients with severe abdominal pathology will typically:
a. Be moving around, as they cannot get comfortableb. Lie as still as possible in the fetal positionc. Be seated, leaning forward in an attempt to relieve the paind. All of the above
3. Pain with cholecystitis is often acute and located in which abdominalquadrant?
a. Left lowerb. Left upperc. Right lowerd. Right upper
4. Pain that occurs when nerve fibers carrying the pain message cross at thespinal cord is called?
a. Parietal painb. Referred painc. Visceral paind. Reactionary pain
5. The kidneys are protected relatively well against injury due to their locationin the?
a. Chest cavityb. Right lower quadrantc. Pelvic regiond. Retroperitoneal space

SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
14
6. The Abdominal Pain Standing Order pediatric dose for ondansetron is0.1mg/kg over 2 to 5 minutes up to a maximum dose of 4mg.
a. Trueb. False
7. The highest priority when treating a patient with abdominal pain is to:
a. Transport the patient in the most comfortable positionb. Treat the patient for shockc. Maintain the airway, breathing, and circulationd. Palpate the abdomen for pulsating mass
8. Your adult male patient presents with abdominal cramps, low-grade fever,pale, moist skin, nausea and vomiting, and tenderness to the lower leftside of the abdomen. This patient qualifies for the Abdominal PainStanding Order.
a. Trueb. False
9. You are transporting the above patient using the Abdominal Pain StandingOrder. You have O2 at 3 liters (96%), FSBG of 82, cardiac monitor withsinus tachycardia at 128, BP of 88/52, initiated the large bore IV andadministered a normal saline bolus. Your next intervention(s) would be to:
a. Repeat vital signs, listen to lung sounds, and consider repeat fluidbolus.
b. Reassess FSBG, administer morphine and ondansetronc. Redirect to a closer facilityd. Start a second large bore IV, change the patient to a non-rebreather
mask at 15 liters, give 1/2 amp of D-50
10. Your 68 year old female diabetic patient is complaining of abdominal painthat also radiates to her neck. She would be an appropriate candidate forthe Abdominal Pain Standing Order.
a. Trueb. False
11. Which of the following characteristics of visceral pain are true?
a. Results from irritation to the peritoneal liningb. Begins as sharp, turning to dull and intermittent over timec. Results from stretching of muscle fibers in organsd. Indicates a non-acute abdomen

SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
15
12. Which of the following acute conditions usually require surgery?
a. AAA, perforated ulcer, incarcerated herniab. Abdominal trauma, peritonitis, appendicitisc. Ruptured ectopic pregnancy, PID, intestinal obstructiond. Mesenteric infarction, ascites, hematuria
13. Abdominal emergencies can include the gastrointestional, genitourinaryand reproductive systems.
a. Trueb. False
14. It is important for the prehospital provider to identify the organ systemcausing the abdominal pain prior to implementing the standing order.
a. Trueb. False
15. An incarcerated hernia is defined as:
a. A hernia that needs surgical interventionb. A hernia that affects prisonersc. A hernia that can be reduced manuallyd. A hernia that spontaneously reduces

SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
16
REFERENCES
Bates, B. (1983) A Guide to Physical Examination Third Edition. Philadelphia,Pennsylvania: JB Lippincott Company.
Bledsoe, B.E., Porter, R.S., Shade, B.R., (1994) Paramedic Emergency CareSecond edition. Englewood Cliffs, New Jersey: Prentice Hall.
Cunningham, C. (2008). Say a Prayer for the Pretender. JEMS.com. RetrievedNovember 13, 2008 from http://www.jems.com/news_and_articles/columns
Medical Sciences for Clinical Practice - A Self-Instructional Tutorial CurriculumMinicourse 4: The Acute Abdomen: Retrieved November 10, 2008 fromhttp://www.ece.ncsu.edu/imaging/MedImg/SIMS/Module2/GE2 4.html
Newberry, L. Editor, (2003) Sheehy’s Emergency Nursing Principals and PracticeFifth Edition. St. Louis, MO: Mosby.

SAEMS ABDOMINAL PAIN STANDING ORDER TRAINING MODULENovember 2008
17
EVALUATION
Please answer the following questions by marking the appropriate response:
LowestWorstLeast
HighestBestMost
1. To what extend did this module meetyour needs?
1 2 3 4 5
2. There was a balance betweentheoretical and practical information.
1 2 3 4 5
3. The time required was appropriate tothe content.
1 2 3 4 5
4. The module increased my knowledgeand understanding of the topic.
1 2 3 4 5
5. References or audiovisuals wereadequate.
1 2 3 4 5
6. Overall, this program was worthwhile. 1 2 3 4 5
7. Additional comments:
________________________________________________________________________________________________________________________________