Hematologic Disorders
4
Vox Sang. 51: suppl. 2, pp. 18-21 (1986) 0 1986 S. Karger AG, Basel 0042-9007/86/05 16-001 8 $2.7510 Hematologic Disorders William Harrington Center for Blood Diseases, University of Miami School of Medicine, Miami, Fla, USA Abstract. A distinction is made between postinfection thrombocytopenia of childhood and idiopathic thrombo- cytopenia (ITP) of adulthood. Relative advantages of treatment modalities, including splenectomy, are weighed, with an emphasis on the administration of intravenous immunoglobulin (WIG) as an emergency measure in the adult patient with ITP. Management of thrombotic thrombocytopenic purpura (TTP) is also discussed, as is the case of a patient who became alloimmunized after 2 years of multiple transfusions used to treat an arteriovenous malforma- tion of the small bowel. Thrombocytopenia: A Matter of Definitions There is a great difference between the postinfection thrombocytopenia of childhood (mistakenly called idio- pathic) and the truly idiopathic disease of adulthood. ‘Idiopathic’ thrombocytopenia of childhood virtually always follows a viral infection or immunization and is generally self-limiting. Exposure to any of innumerable viruses can bring on this form of thrombocytopenia. It is believed to be due to an immune complex composed of viral antigen and newly raised antibody to that antigen. The child usually recovers within several days or a few weeks. Idiopathic thrombocytopenic purpura (ITP) is most common in young women. It occurs without any apparent antecedent viral or chemical exposure; it is, therefore, truly idiopathic. In ITP, plasma cells, for reasons unknown, make an IgG autoantibody that reacts with platelets, rendering them vulnerable to phagocytosis and destruction by macrophages (cells that have receptors for Fc subunits of immunoglobulins). The spleen, with its unique microenvironment of tortuous sinusoidal blood flow and an abundance of intravascular macrophages, is the primary site of the platelet destruction. Even the normal spleen harbors one third of the circulating plate- lets as they slowly negotiate their way through the sinu- soids (fig. 1). Note, however, that there are some patients with ITP in whom autoantibody has not been demonstrated. They are presumed to have some defect in megakaryocyte ripening. As a treatment of ITP, splenectomy removes the obsta- cle course and a large mass of intravascular macrophages. Hence, a splenectomized women may be clinically cured of ITP. Yet because of circulating ITP autoantibody that can cross the placenta, her child, having a spleen, may be born with neonatal ITP. The mechanism, which we described 35 years ago, has recently been reiterated by Karpatkin [2] (fig. 2). Methods of Treating ITP ITP is chronic or recurrent in 90% of cases. Since the disorder occurs most frequently in young women, the management strategy usually entails weighing the side effects of long-term therapy. For example, glucocorticoids are effective in retarding antibody synthesis; however, their protracted use has serious, well-known conse- quences. Splenectomy, on the other hand, removes much
-
Upload
william-harrington -
Category
Documents
-
view
213 -
download
0
Transcript of Hematologic Disorders

Vox Sang. 51: suppl. 2, pp. 18-21 (1986) 0 1986 S. Karger AG, Basel
0042-9007/86/05 16-001 8 $2.7510
Hematologic Disorders
William Harrington Center for Blood Diseases, University of Miami School of Medicine, Miami, Fla, USA
Abstract. A distinction is made between postinfection thrombocytopenia of childhood and idiopathic thrombo- cytopenia (ITP) of adulthood. Relative advantages of treatment modalities, including splenectomy, are weighed, with an emphasis on the administration of intravenous immunoglobulin (WIG) as an emergency measure in the adult patient with ITP. Management of thrombotic thrombocytopenic purpura (TTP) is also discussed, as is the case of a patient who became alloimmunized after 2 years of multiple transfusions used to treat an arteriovenous malforma- tion of the small bowel.
Thrombocytopenia: A Matter of Definitions
There is a great difference between the postinfection thrombocytopenia of childhood (mistakenly called idio- pathic) and the truly idiopathic disease of adulthood.
‘Idiopathic’ thrombocytopenia of childhood virtually always follows a viral infection or immunization and is generally self-limiting. Exposure to any of innumerable viruses can bring on this form of thrombocytopenia. It is believed to be due to an immune complex composed of viral antigen and newly raised antibody to that antigen. The child usually recovers within several days or a few weeks.
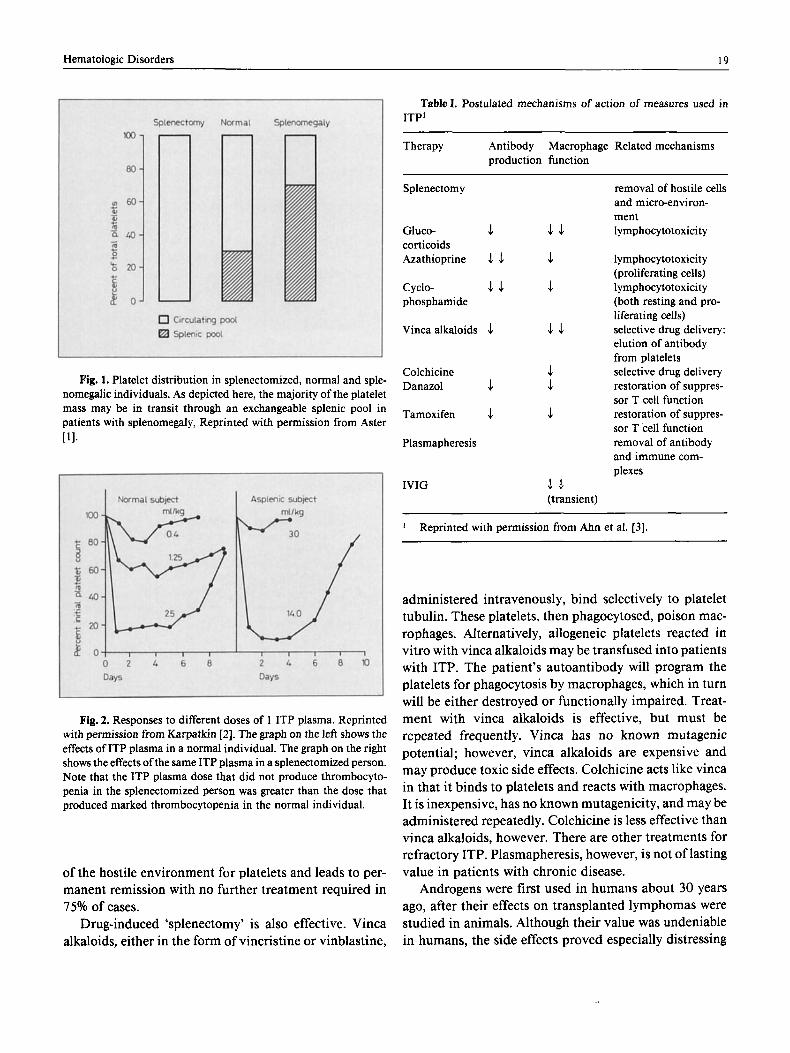
Idiopathic thrombocytopenic purpura (ITP) is most common in young women. It occurs without any apparent antecedent viral or chemical exposure; it is, therefore, truly idiopathic. In ITP, plasma cells, for reasons unknown, make an IgG autoantibody that reacts with platelets, rendering them vulnerable to phagocytosis and destruction by macrophages (cells that have receptors for Fc subunits of immunoglobulins). The spleen, with its unique microenvironment of tortuous sinusoidal blood flow and an abundance of intravascular macrophages, is the primary site of the platelet destruction. Even the normal spleen harbors one third of the circulating plate-
lets as they slowly negotiate their way through the sinu- soids (fig. 1).
Note, however, that there are some patients with ITP in whom autoantibody has not been demonstrated. They are presumed to have some defect in megakaryocyte ripening.
As a treatment of ITP, splenectomy removes the obsta- cle course and a large mass of intravascular macrophages. Hence, a splenectomized women may be clinically cured of ITP. Yet because of circulating ITP autoantibody that can cross the placenta, her child, having a spleen, may be born with neonatal ITP. The mechanism, which we described 35 years ago, has recently been reiterated by Karpatkin [2] (fig. 2).
Methods of Treating ITP
ITP is chronic or recurrent in 90% of cases. Since the disorder occurs most frequently in young women, the management strategy usually entails weighing the side effects of long-term therapy. For example, glucocorticoids are effective in retarding antibody synthesis; however, their protracted use has serious, well-known conse- quences. Splenectomy, on the other hand, removes much
Hematologic Disorders 19
Fig. 1. Platelet distribution in splenectomized, normal and sple- nomegalic individuals. As depicted here, the majority of the platelet mass may be in transit through an exchangeable splenic pool in patients with splenomegaly, Reprinted with permission from Aster 111.
Fig. 2. Responses to different doses of 1 ITP plasma. Reprinted with permission from Karpatkin [2]. The graph on the left shows the effects of ITP plasma in a normal individual. The graph on the right shows the effects of the same ITP plasma in a splenectomized person. Note that the ITP plasma dose that did not produce thrombocyto- penia in the splenectomized person was greater than the dose that produced marked thrombocytopenia in the normal individual.
of the hostile environment for platelets and leads to per- manent remission with no further treatment required in 15% of cases.
Drug-induced ‘splenectomy’ is also effective. Vinca alkaloids, either in the form of vincristine or vinblastine,
Table 1. Postulated mechanisms of action of measures used in ITP’
Therapy Antibody Macrophage Related mechanisms production function
Splenectomy removal of hostile cells and micro-environ- ment
Gluco- .1 4.1 lymphocytotoxicity corticoids Azathioprine 5. 4 .1 lymphocytotoxicit y
(proliferating cells) Cyclo- 4 . 1 .1 lymphocytotoxicity phosphamide (both resting and pro-
Vinca alkaloids $ J.1 selective drug delivery: liferating cells)
elution of antibody from platelets
Colchicine .1 selective drug delivery Danazol .1 .1 restoration of suppres-
Tamoxifen & .1 restoration of suppres-
Plasmapheresis removal of antibody
sor T cell function
sor T cell function
and immune com- plexes
WIG 4.1 (transient)
Reprinted with permission from Ahn et al. [3].
administered intravenously, bind selectively to platelet tubulin. These platelets, then phagocytosed, poison mac- rophages. Alternatively, allogeneic platelets reacted in vitro with vinca alkaloids may be transfused into patients with ITP. The patient’s autoantibody will program the platelets for phagocytosis by macrophages, which in turn will be either destroyed or functionally impaired. Treat- ment with vinca alkaloids is effective, but must be repeated frequently. Vinca has no known mutagenic potential; however, vinca alkaloids are expensive and may produce toxic side effects. Colchicine acts like vinca in that it binds to platelets and reacts with macrophages. It is inexpensive, has no known mutagenicity, and may be administered repeatedly. Colchicine is less effective than vinca alkaloids, however. There are other treatments for refractory ITP. Plasmapheresis, however, is not of lasting value in patients with chronic disease.
Androgens were first used in humans about 30 years ago, after their effects on transplanted lymphomas were studied in animals. Although their value was undeniable in humans, the side effects proved especially distressing

20 Harrington
to female patients. However, they clearly had antilym- phocytic effects. Androgens, then, are generally used only for acute, short-term management of ITP, as most patients affected with ITP are female. They produce a fairly prompt response and ultimately decrease antibody production, but they cause masculinization, hirsutism, weight gain, and acne. Danazol, another agent used to treat ITP, is an attenuated androgen with minimal mas- culinizing effect. It decreases the amount of circulating antibody and restores the T cell helper/suppressor ratio to normal, It is effective and has few side effects, making it well-suited for treatment of male and female patients with refractory ITP; however, it is expensive. Azathioprine and cyclosphosphamide are less effective than vinca alka- loids, take longer to act, and are oncogenic and mutagen- ic. Therefore, they are not considered agents of choice for treating a benign disease such as ITP. Intravenous immu- noglobulin (IVIG) may be administered to evoke a fairly prompt increase in platelets (platelet counts up to 50,000 or 60,000/mm3), especially before slow infusion of vinca alkaloid. In addition, IVlG is used in ITP for emergen- cies, such as intracranial bleeding or during labor. It is presumed that IVIG acts by competing with the ITP autoantibody for the Fc receptors on macrophages. These methods of treatment are summarized in table I.
Thrombotic Thrombocytopenic Purpura
Thrombotic thrombocytopenic purpura (TTP) is a usually fatal disease characterized by the presence of microthrombi (composed of platelets) in small blood ves- sels.
In 1978, a group in Cleveland proposed exchange transfusion, an approach that had been used successfully in 1 patient about 20 years earlier. It was thought that some putative toxin would be removed. Dr. Byrnes in our group found that, rather than removing a toxin, the nor- mal plasma provided a factor missing in TTP, a disaggre- gator of platelets. It was subsequently thoroughly studied by Dr. Lian in our group. Apparently, a globulin in nor- mal plasma may be responsible for promoting dissocia- tion of the microthrombi.
Transfusions and the Allosensitized Patient
Platelets have a normal lifespan of 8- 10 days. If plate- lets are repeatedly transfused, however, the recipient eventually becomes alloimmunized to platelet alloanti-
gens. The infusion of HLA-compatible platelets may def- er alloimmunization, but even so, incompatibility of platelet-specific alloantigens remains.
Drs Ahn and Junghans, also in our group, treated a patient with thrombocytopenia and alloimmunization to both HLA- and platelet-specific antigens. The patient had massive gastrointestinal bleeding due to an arteriovenous malformation of the small bowel. IVIG, given 1 h before infusion of 9 units of platelets, increased platelet half-life from 3 min to 3 h, enabling surgical resection of the small bowel with minimal operative blood loss.
Conclusion
The use of IVIG is now extensively documented in the treatment of thrombocytopenia of childhood, a generally self-limiting condition. Infusion of immunoglobulin is recommended as an emergency treatment for refractory ITP in adults and may have value in TTP and bleeding states brought about by allosensitization.
References
1 Aster, R. H.: Pooling of platelets in the spleen: role in the patho- genesis of ‘hypersplenic’ thrombocytopenia. J. clin. Invest. 45:
2 Karpatkin, S.: Autoimmune thrombocytopenic purpura. Blood 56: 329-343 (1 980).
3 Ahn, Y . S.; Harrington, W. J.; Mylvaganam, R.; Allen, L. M.; Pall, L. M.: Slow infusion of vinca alkaloid in the treatment of ITP. Ann. intern. Med. 100: 192 (1984).
645-657 ( 1 966).
Questions and Answers
Question: In terms of the poison theory, what functions may be impaired that might contribute to platelet survival?
Harrington: The difference in platelet survival time before and after splenectomy in ITP - between a platelet count of 5,000/mm3 and one of 500,000/mm3 in a patient with ITP - is only a matter of a day or so. Vinca-loaded platelets are able to achieve this critical difference. In addition, loaded platelets that are programmed with ITP antibody and administered to patients with monocytic leukemia (macrophage-like) dramatically decrease the white blood cell (WBC) count. Vinca-loaded platelets programmed with ITP antibody also correct hemolytic anemia. If vinca-loaded platelets programmed with ITP antibody are incubated with macrophages, the macrophages appear to disintegrate when examined with electron microscopy. In vinca-loaded platelets alone are exposed to macrophages, the macro- phages are not adversely affected.
Comment: We are currently using cyclosporine to treat patients with aplastic anemia who cannot receive bone marrow transplants, are elderly, or don’t have donors.

Hematologic Disorders 21
Because most of our patients are highly alloimmunized, they cannot tolerate platelets. These patients are being treated in an attempt to induce remission of the aplastic anemia. About 50% of these patients respond favorably. Interestingly, those patients who do not respond are now able to tolerate random platelets. and their antiplatelet antibody completely disappears. Three patients devel- oped antibodies and should do well with random normal platelets. Cyclosporine has also been effective in patients who experience difficulty with cyclophosphamide or vincristine, are cushingoid, or have very low WBC counts. One year after treatment, several of these patients are doing well and have no apparent bleeding problems.
Question: If IVIG works mainly by inducing ‘dyspepsia’ of the macrophage system, how is the efficacy of vinca alkaloids enhanced by IVIG?
Harrington: The probable, but still unproven, mechanism is the overloading of Fc receptors. For example, in thrombocytopenia, with a platelet count of 40,000 or 50,000/mm3, platelets will still be destroyed after IVIG administration. Therefore, the use of IVIG does not totally obliterate the ability of the macrophage to destroy the platelets. By raising the platelet count with IVIG, however, there are more platelets to be loaded in vivo.
Question: What percentage of adults with chronic thrombocyto- penia spontaneously recover? What percentage of splenectomized adults develop sepsis?
Harrington: Of nearly 2,000 of our patients with ITP, 10% recov- ered completely, either spontaneously or, more often, following a period of weeks or months of medical therapy. The situation seems similar to the development of the first episode of rheumatoid arthri- tis: most ofthose affected will develop a chronic condition unless the process is interrupted.
To answer the second question, very few splenectomized adults have a problem with infection unless they have Hodgkin’s disease or lymphocytic lymphomas or leukemias and are thus already compro- mised. In those cases, the incidence of infection is greater.
William Harrington, MD, Center for Blood Disorders, University of Miami Hospital, 1475 NW 12th Avenue, Miami, FL 33101 (USA)