
Heart Valve Replacement with the Björk-Shiley Monostrut Valve: Early Results of a Multicenter...
7
Heart Valve Replacement with the Bjork-Shiley Mbnostrut Valve: Early Results of a Multicenter Clinical Investigation Lars I. Thulin, M.D., William H. Bain, F.R.C.S., Hans H. Huysmans, M.D., Gerrit van Ingen, M.D., Ignatio Prieto, F.R.C.S., Fadi Basile, F.R.C.S., Dan A. Lindblom, M.D., and Christian L. Olin, M.D. ABSTRACT To evaluate the clinical performance of the Bjork-Shiley Monostrut prosthesis, five centers combined their early experience. Between May, 1982, and June, 1985, 537 prostheses were implanted in 486 patients at these cen- ters: 246 patients had aortic valve replacement (AVR), 163 underwent mitral valve replacement (MVR), and 47 had double-valve replacement (DVR). Thirty patients under- went other, more complex procedures. Concomitant car- diac procedures were performed in altogether 25%. Overall hospital (30 days) mortality was 5.1% (3.6% for AVR, 4.3% for MVR, 8.3% for DVR, and 16.6% for other procedures). The patients were followed up at 6- to 9-month intervals from 6 to 48 months (mean follow-up, 33 months). Follow- up was 99.6% complete. Late mortality was 7.2%. The three-year survival rate was 91.0% for AVR, 92.3% for MVR, and 76.2% for DVR. There was no structural failure of the prosthesis. No instances of valve thrombosis and fatal thromboembolism occurred in anticoagulated pa- tients. The three-year incidence of freedom from throm- boembolic events (including TIA) was 89.8% for AVR, 94.9% for MVR, and 90.2% for DVR. Preoperative and postoperative data for the assessment of mechanical hemolysis was available in 60% of the patients. The degree of mechanical hemolysis was low and did not change with time. Although the follow-up is still short, the Bjork- Shiley Monostrut prosthesis appears to represent an im- provement over previous Bjork-Shiley models, particu- larly with regard to durability. Since the introduction of the Bjork-Shiley tilting disk valve in 1969 [l], the prosthesis has undergone progres- sive development to improve its hemodynamic perfor- mance, diminish thromboembolic complications, and to increase its durability. In the latest model, the Bjork- Shiley Monostrut (Monostrut, Shiley, Irvine, California) prosthesis (8-S M), the outflow strut (as well as the inflow strut) has been made an integral part of the cage From the Departments of Cardiothoracic Surgery at Lund University Hospital, Lund, Sweden; Western Infirmary, Glasgow, Scotland; Aca- demic Hospital, Leiden, Holland; HBpital Hotel-Dieu de Montreal, Quebec, Canada; and Karolinska Hospital, Stockholm, Sweden. Accepted for publication Aug 31, 1987. Address reprint requests to Dr. Olin, Department of Thoracic Surgery, Lund University Hospital, S-221 85 Lund, Sweden. [2]. The cage and the struts are machined from a single piece of Haynes 25, a cobalt-based alloy, by a special electromechanical process. The single outflow strut, the "Monostrut," is shaped like a hook and has a broad base to increase its strength (Fig 1). The convexoconcave disk is made of pyrolytic carbon and opens to 70 degrees to decrease resistance to flow. Two types of suture rings are available, Teflon and carbon-coated Dacron. To get a sufficiently large patient sample to study, the early experience of five centers, four European and one Canadian, were combined into a multicenter investiga- tion. Uniform methods of follow-up and definitions of complications were agreed on. Special attention was focused on valve-related complications such as mechani- cal failure, thromboembolism, and prosthesis-induced hemolysis. Patients and Methods The study group comprised 486 patients who under- went valve replacement with the B-S M prosthesis be- tween May, 1982, and June, 1985, at the five centers: 246 had aortic valve replacement (AVR), 163 had mitral valve replacement (MVR), and 47 underwent double- valve replacement (DVR). Thirty patients underwent uncommon or more complex procedures, for which an- other prosthesis (or prosthetic material) was implanted in addition to the B-S M prosthesis. A total of 540 B-S M prostheses were implanted: 309 in the aortic position, 223 in the mitral position, 7 in the tricuspid position, and 1 in the pulmonic position. The B-S M prosthesis was used to replace a natural valve in 96% and a failed prosthesis in 4%. Concomitant cardiac procedures were performed in 25% of the patients, coro- nary artery bypass being the most common (Table 1). Tricuspid valve repair was performed in 8% of those with MVR and in 6% of those with DVR. Preoperative patient characteristicsare shown in Table 2. The mean age of the patients was 56.8 years (age range, 2-78 years). There was a male preponderance in the AVR group and a female preponderance in the MVR and DVR groups. The majority (72%) of the patients were in New York Heart Association (NYHA)Functional Class I11 and IV. Altogether, 19.1% had undergone pre- vious cardiac operations. Preoperative atrial fibrillation was present in 7.4% of the patients with AVR, 58.9% of those with MVR, and 44.7% of those with DVR. Preoperative thromboembolic episodes (TEs) were re- corded in 15.2% of the patients. Ninety-five percent of 164 Ann Thorac Surg 45:164-170, Feb 1988. Copyright 0 1988 by The Society of Thoracic Surgeons
-
Upload
christian-l -
Category
Documents
-
view
214 -
download
2
Transcript of Heart Valve Replacement with the Björk-Shiley Monostrut Valve: Early Results of a Multicenter...

Heart Valve Replacement with the Bjork-Shiley Mbnostrut Valve: Early Results of a Multicenter Clinical Investigation Lars I. Thulin, M.D., William H. Bain, F.R.C.S., Hans H. Huysmans, M.D., Gerrit van Ingen, M.D., Ignatio Prieto, F.R.C.S., Fadi Basile, F.R.C.S., Dan A. Lindblom, M.D., and Christian L. Olin, M.D.
ABSTRACT To evaluate the clinical performance of the Bjork-Shiley Monostrut prosthesis, five centers combined their early experience. Between May, 1982, and June, 1985, 537 prostheses were implanted in 486 patients at these cen- ters: 246 patients had aortic valve replacement (AVR), 163 underwent mitral valve replacement (MVR), and 47 had double-valve replacement (DVR). Thirty patients under- went other, more complex procedures. Concomitant car- diac procedures were performed in altogether 25%. Overall hospital (30 days) mortality was 5.1% (3.6% for AVR, 4.3% for MVR, 8.3% for DVR, and 16.6% for other procedures). The patients were followed up at 6- to 9-month intervals from 6 to 48 months (mean follow-up, 33 months). Follow- up was 99.6% complete. Late mortality was 7.2%. The three-year survival rate was 91.0% for AVR, 92.3% for MVR, and 76.2% for DVR. There was no structural failure of the prosthesis. No instances of valve thrombosis and fatal thromboembolism occurred in anticoagulated pa- tients. The three-year incidence of freedom from throm- boembolic events (including TIA) was 89.8% for AVR, 94.9% for MVR, and 90.2% for DVR. Preoperative and postoperative data for the assessment of mechanical hemolysis was available in 60% of the patients. The degree of mechanical hemolysis was low and did not change with time. Although the follow-up is still short, the Bjork- Shiley Monostrut prosthesis appears to represent an im- provement over previous Bjork-Shiley models, particu- larly with regard to durability.
Since the introduction of the Bjork-Shiley tilting disk valve in 1969 [l], the prosthesis has undergone progres- sive development to improve its hemodynamic perfor- mance, diminish thromboembolic complications, and to increase its durability. In the latest model, the Bjork- Shiley Monostrut (Monostrut, Shiley, Irvine, California) prosthesis (8-S M), the outflow strut (as well as the inflow strut) has been made an integral part of the cage
From the Departments of Cardiothoracic Surgery at Lund University Hospital, Lund, Sweden; Western Infirmary, Glasgow, Scotland; Aca- demic Hospital, Leiden, Holland; HBpital Hotel-Dieu de Montreal, Quebec, Canada; and Karolinska Hospital, Stockholm, Sweden.
Accepted for publication Aug 31, 1987.
Address reprint requests to Dr. Olin, Department of Thoracic Surgery, Lund University Hospital, S-221 85 Lund, Sweden.
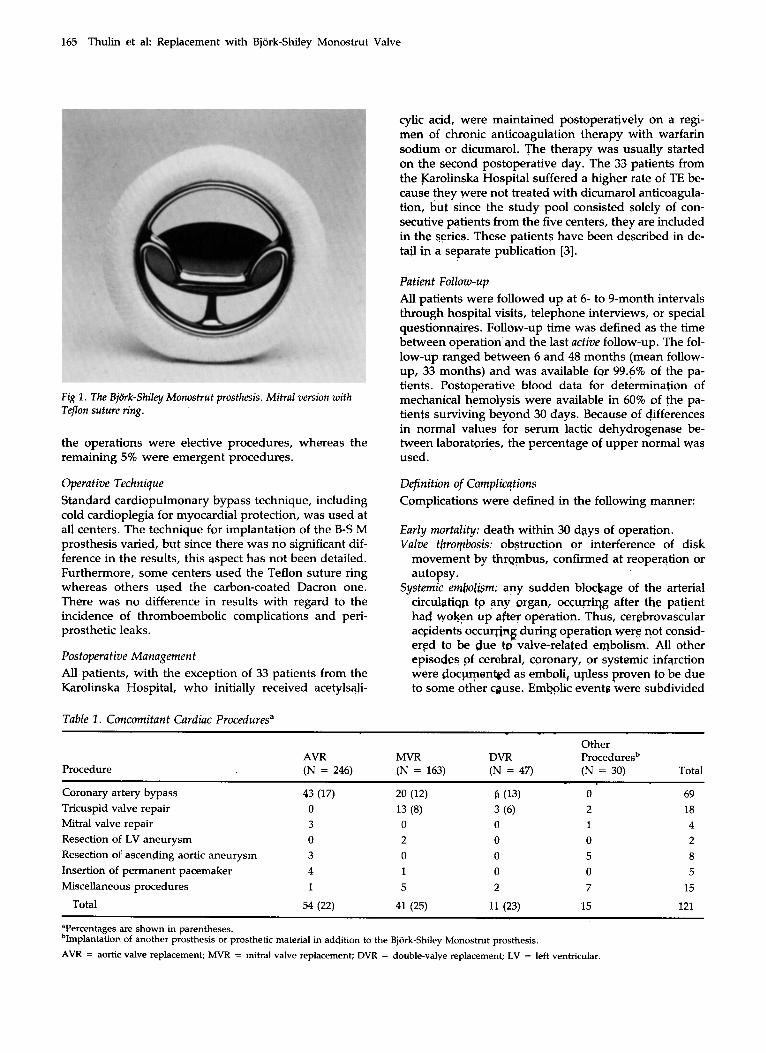
[2]. The cage and the struts are machined from a single piece of Haynes 25, a cobalt-based alloy, by a special electromechanical process. The single outflow strut, the "Monostrut," is shaped like a hook and has a broad base to increase its strength (Fig 1). The convexoconcave disk is made of pyrolytic carbon and opens to 70 degrees to decrease resistance to flow. Two types of suture rings are available, Teflon and carbon-coated Dacron.
To get a sufficiently large patient sample to study, the early experience of five centers, four European and one Canadian, were combined into a multicenter investiga- tion. Uniform methods of follow-up and definitions of complications were agreed on. Special attention was focused on valve-related complications such as mechani- cal failure, thromboembolism, and prosthesis-induced hemolysis.
Patients and Methods The study group comprised 486 patients who under- went valve replacement with the B-S M prosthesis be- tween May, 1982, and June, 1985, at the five centers: 246 had aortic valve replacement (AVR), 163 had mitral valve replacement (MVR), and 47 underwent double- valve replacement (DVR). Thirty patients underwent uncommon or more complex procedures, for which an- other prosthesis (or prosthetic material) was implanted in addition to the B-S M prosthesis.
A total of 540 B-S M prostheses were implanted: 309 in the aortic position, 223 in the mitral position, 7 in the tricuspid position, and 1 in the pulmonic position. The B-S M prosthesis was used to replace a natural valve in 96% and a failed prosthesis in 4%. Concomitant cardiac procedures were performed in 25% of the patients, coro- nary artery bypass being the most common (Table 1). Tricuspid valve repair was performed in 8% of those with MVR and in 6% of those with DVR.
Preoperative patient characteristics are shown in Table 2. The mean age of the patients was 56.8 years (age range, 2-78 years). There was a male preponderance in the AVR group and a female preponderance in the MVR and DVR groups. The majority (72%) of the patients were in New York Heart Association (NYHA) Functional Class I11 and IV. Altogether, 19.1% had undergone pre- vious cardiac operations. Preoperative atrial fibrillation was present in 7.4% of the patients with AVR, 58.9% of those with MVR, and 44.7% of those with DVR. Preoperative thromboembolic episodes (TEs) were re- corded in 15.2% of the patients. Ninety-five percent of
164 Ann Thorac Surg 45:164-170, Feb 1988. Copyright 0 1988 by The Society of Thoracic Surgeons
165 Thulin r:t al: Replacement with Bjork-Shiley Monostrut Valve
Fig 1. The Bjork-Shiley Monostrut prosthesis. Mitral version with Teflon suture ring.
the operations were elective procedures, whereas the remaining S% were emergent procedures.
Operative Technique Standard cardiopulmonary bypass technique, including cold cardioplegia for myocardial protection, was used at all centers. The technique for implantation of the B-S M prosthesis varied, but since there was no significant dif- ference in the results, this aspect has not been detailed. Furthermore, some centers used the Teflon suture ring whereas others used the carbon-coated Dacron one. There was no difference in results with regard to the incidence of thromboembolic complications and peri- prosthetic leaks.
Postoperative Management All patients, with the exception of 33 patients from the Karolinska Hospital, who initially received acetylsaji-
cylic acid, were maintained postoperatively on a regi- men of chronic anticoagulation therapy with warfarin sodium or dicumarol. The therapy was usually started on the second postoperative day. The 33 patients from the Karolinska Hospital suffered a higher rate of TE be- cause they were not treated with dicumarol anticoagula- tion, but since the study pool consisted solely of con- secutive patients from the five centers, they are included in the series. These patients have been described in de- tail ip a separate publication [3].
Patient Follow-up All patients were followed up at 6- to 9-month intervals through hospital visits, telephone interviews, or special questionnaires. Follow-up time was defined as the time between operation apd the last active follow-up. The fol- low-up ranged between 6 and 48 months (mean follow- up, 33 months) and was available for 99.6% of the pa- tients. Postoperative blood data for determination of mechanical hemolysis were available in 60% of the pa- tients surviving beypnd 30 days. Because of differences in normal values for serum lactic dehydrogenase be- tween laboratories, the percentage of upper normal Was used.
Definition of Complicutions Complications were defined in the following manner:
Early mortality: death within 30 days of operation. Valve throrpbosis: obstruction or interference of disk
movement by thrgmbus, confirmed at reoperation or autopsy.
Systemic embolism; any svdden blockage of the arterial circulatiqp to any organ, occurriqg after the patient had woken up after operation. Thus, cerebrovascular accidents occuqjng during operatian were not consid- erFd to be due to valve-related eqbolism. All other episodes of cerebral, coronary, or systemic infqrction were documented as emboli, upless proven to be due to some other cause. Embolic events 'were subdivided
Table 1. Concomitant Cardiac Proceduresa
Other AVR MVR DVR Proceduresb
Procedure (N = 246) (N = 163) (N = 47) (N = 30) Total ~ ~~ ~~~ -
Coronary artery bypass 43 (17) 20 (12) 6 0 3 ) 0 69 Tricuspid valve repair 0 13 (8) 3 (6) 2 18 Mitral valve repair 3 0 0 1 4 Resection of LV aneurysm 0 2 0 0 2
Insertion of permanent pacemaker 4 1 0 0 5
Total 54 (22) 41 (25) 11 (23) 15 121
Resection of ascending aortic aneurysm 3 0 0 5 8
Miscellaneous procedures 1 5 2 7 15
Tercentages are shown in parentheses. bImplantation of another prosthesis or prosthetic material in addition to the Bjork-Shiley Monostrut prosthesis. AVR = aortic valve replacement; MVR = mitral valve replacement; DVR = double-valye replacement; LV = left ventricular.

166 The Annals of Thoracic Surgery Vol 45 No 2 February 1988
Table 2. Preoperative Patient Characteristics
Other AVR MVR DVR Procedures Total
Variable (N = 246) (N = 163) (N = 47) (N = 30) (N = 486)
Age (yr) Mean Range
Male Female
NYHA Class
Sex
I I1
111 IV
Previous cardiac surgery (%) Previous valve replacement (%) Preop. atrial fibrillation (%) Preop. thromboembolic events (%)
58.5 16-78
162 84
10 83
122 31 4.9 3.2 7.4
13.8
55 13-77
59 104
0 31
102 30 28.8 5.5
58.9 18.4
58 22-75
15 31
0 7
32 8
34.0 6.4
44.7 12.8
50 2-69
11 19
2 5
12 11 60 0
43.3 13.3
56.8 2-78
247 239
12 126 268 80 19.1 4.1
28 15.2
~ ~ _ _ _ _
AVR = aortic valve replacement, MVR = mitral valve replacement, DVR = double-valve replacement, NYHA = New York Heart Associahon
into transient ischemic attacks (TIAs), inferring complete recovery within 24 hours, and TEs.
Anticoagulation bleeding: any internal or external bleeding severe enough to warrant hospitalization, blood trans- fusion, or nontrivial outpatient care.
Prosthetic valve endocarditis: postoperative endocarditis occurring de novo confirmed by positive bacterial cul- ture, reoperation, or postmortem examination.
Periprosthetic leakage: any regurgitation occurring around the prosthesis confirmed by catheterization, by reop- eration, or at autopsy.
Hemolysis: any red blood cell destruction resulting in anemia in the absence of periprosthetic leakage or en- docarditis.
Mechanical failure: any intrinsic mechanical or structural failure.
Disk interference: any impairment of the free movement of the disk not attributable to valve thrombosis or me- chanical failure.
Event-free survival: percentage of patients alive and free from any valve-related and anticoagulation-related complications.
Statistical Analyses To estimate survival, incidence of freedom from valve- related complications, and event-free survival, the statis- tical method of Lee was used [4]. The Statistical Analysis System [5] was the base for all computations performed. Chi-square statistics were used to estimate differences between the groups. Differences resulting in a p value of less than 0.05 were considered significant. For analysis of late survival, patients lost to follow-up or later receiv- ing a prosthesis other than the B-S M were withdrawn. For analysis of nonfatal events, the patients were with-
drawn at the time of the first event or at the time of death.
Results Early Mortality There were 25 early deaths (within 30 days of operation), resulting in an early mortality of 5.1%. The early mortal- ity was 3.6% for AVR, 4.3% for MVR, 8.3% for DVR, and 16.6% for other procedures. The causes of early deaths were as follows:
Myocardial failure Myocardial infarction Bleeding Sepsis Cerebrovascular accident Pancreatitis Pneumonia Pulmonary embolism Valve thrombosis
10 4 3 3 1 1 1 1 1
The most common cause of hospital mortality was myo- cardial failure. Factors associated with increased early mortality were concomitant major surgical procedure, NYHA Functional Class IV, and emergent operation.
One patient died 29 days after operation because of valve thrombosis. This was a 56-year-old woman who had undergone aortic valve replacement. She belonged to the early series from the Karolinska Hospital and was discharged without dicumarol anticoagulation.
Late Mortality There were 33 late deaths (later than 30 days), resulting in a late mortality of 7.2%. The causes of late deaths were as follows:
167 Thulin et al: Replacement with Bjork-Shiley Monostrut Valve
80 -
70 -
60-
Cardiac arrhythmia Cancer Bleeding Heart failure Myocardial infarction Sepsis Pseudomembranous colitis Postirradiation pneumonitis Aortic rupture Valve thrombosis Unknown
+ =MVR (92 .3%) . ..---.* =AVR ( 9 1 .O%) \ \ --.A =DVR (76.2%) m
2 3 4 2 3 0 2 2 3 1 9 7 1 6 4 1 3 7 7 9 AVR
1 5 3 1 5 0 144 1 1 2 7 1 5 0 2 0 M V R
4 3 4 1 4 0 3 4 2 0 14 7 D V R
6 6 5 5 3 2 1 1 1 1 2
Cardiac arrhythmia and cancer were the most common causes of death. Four of the 5 late deaths attributed to bleeding were caused or aggravated by the anticoag- ulation therapy. There was no statistical correlation between preoperative patient characteristics and the occurrence of late death.
One patient whose late death was due to valve throm- bosis was a 59-year-old woman who had undergone isolated AVR. Although she was discharged on a regi- men of anticoagulants, this therapy was stopped against the advice of the investigator. The patient died 6 months later, and valve thrombosis was confirmed at autopsy. Since the autopsy rate was not loo%, additional cases of valve thrombosis cannot be excluded among the patients dying late of cardiac arrhythmia or of unknown causes.
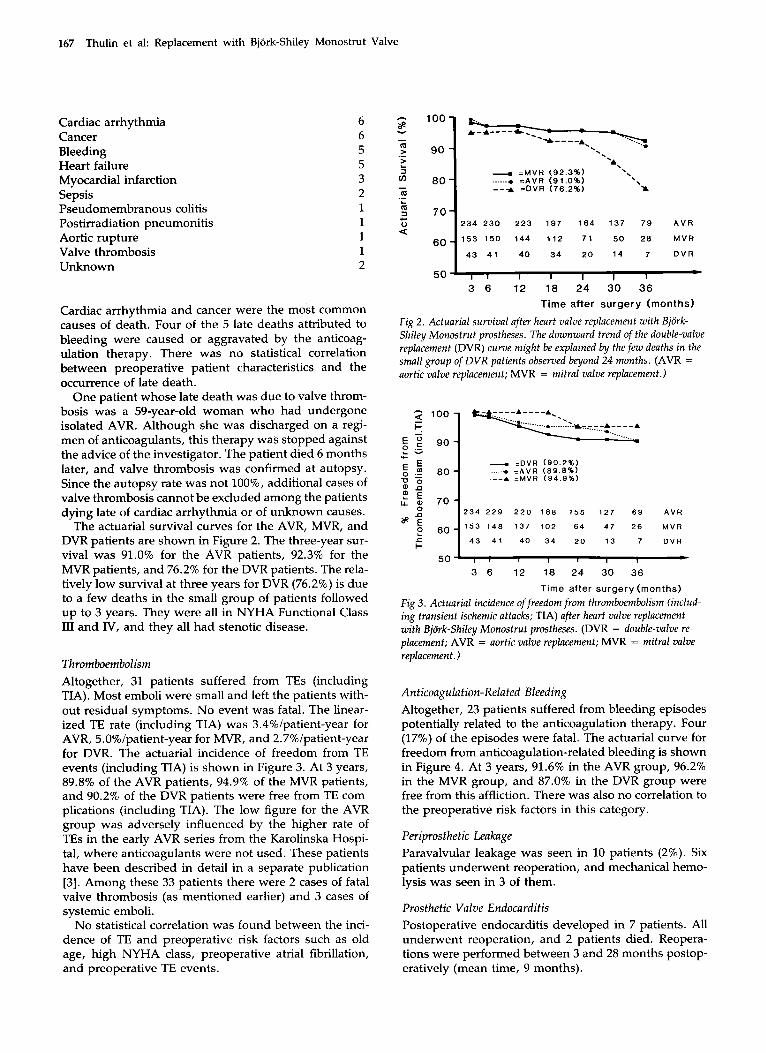
The actuarial survival curves for the AVR, MVR, and DVR patients are shown in Figure 2. The three-year sur- vival was 91.0% for the AVR patients, 92.3% for the MVR patients, and 76.2% for the DVR patients. The rela- tively low survival at three years for DVR (76.2%) is due to a few deaths in the small group of patients followed up to 3 years. They were all in NYHA Functional Class I11 and IV, and they all had stenotic disease.
Thromboembolism Altogether, 31 patients suffered from TEs (including TIA). Most emboli were small and left the patients with- out residual symptoms. No event was fatal. The linear- ized TE rate (including TIA) was 3.4%/patient-year for AVR, 5.0%/patient-year for MVR, and 2.7%/patient-year for DVR. The actuarial incidence of freedom from TE events (including TIA) is shown in Figure 3. At 3 years, 89.8% of the AVR patients, 94.9% of the MVR patients, and 90.2% of the DVR patients were free from TE com- plications (including TIA). The low figure for the AVR group was adversely influenced by the higher rate of TEs in the early AVR series from the Karolinska Hospi- tal, where anticoagulants were not used. These patients have been described in detail in a separate publication [3]. Among these 33 patients there were 2 cases of fatal valve thrombosis (as mentioned earlier) and 3 cases of systemic emboli.
No statistical correlation was found between the inci- dence of TE and preoperative risk factors such as old age, high NYHA class, preoperative atrial fibrillation, and preoperative TE events.
- m m 0
.- L
c
a
Fig 2 . Actuarial survival after heart valve replacement with Bjork- Shiley Monostrut prostheses. The downward trend of the double-valve replacement (DVR) curve might be explained by the few deaths in the small group of DVR patients observed beyond 24 months. (AVR = aortic valve replacement; MVR = mitral valve replacement.)
- 100 9 I-
I- 50
-. =DVR ( 9 0 . 2 % .....+ =AVR ( 0 9 . 8 % 1 .--A LMVR ( 9 4 . 9 % )
2 3 4 2 2 9 2 2 0 1 8 8 1 5 5 127 6 9 AVR
- 1 5 3 1 4 8 137 102 6 4 4 7 2 6 MVR
4 3 4 1 4 0 3 4 2 0 13 7 D V R
I , , I I I c 1
3 6 12 18 24 30 36
Time after surgery (months)
Fig 3. Actuarial incidence offreedom from thromboembolism (includ- ing transient ischemic attacks; TIA) after heart valve replacement with Bjiirk-Shiley Monostrut prostheses. (DVR = double-valve re- placement; AVR = aortic valve replacement; MVR = mitral valve replacement.)
An ticoagulation-Related Bleeding Altogether, 23 patients suffered from bleeding episodes potentially related to the anticoagulation therapy. Four (17%) of the episodes were fatal. The actuarial curve for freedom from anticoagulation-related bleeding is shown in Figure 4. At 3 years, 91.6% in the AVR group, 96.2% in the MVR group, and 87.0% in the DVR group were free from this affliction. There was also no correlation to the preoperative risk factors in this category.
Peripros t hetic Leakage Paravalvular leakage was seen in 10 patients (2%). Six patients underwent reoperation, and mechanical hemo- lysis was seen in 3 of them.
Prosthetic Valve Endocarditis Postoperative endocarditis developed in 7 patients. All underwent reoperation, and 2 patients died. Reopera- tions were performed between 3 and 28 months postop- eratively (mean time, 9 months).

168 The Annals of Thoracic Surgery Vol 45 No 2 February 1988
- = M V R (96 .2%) -..... = A V R ( 9 1 . 6 % ) - - - A = D V R (87 .0%)
2 3 4 2 3 1 2 2 2 1 9 0 157
1 5 3 1 5 0 143 1 1 0 7 1
4 3 4 0 3 9 3 3 1 9
132
4 9
13
7 7
27
6
A V R
M V R
D V R
50' I I
3 6 12 18 2 4 30 36 Time after surgery (months)
Fig 4 . Actuarial incidence of freedom from anticoagulation-related bleeding with Bjork-Shiley Monostrut prostheses. (MVR = mitral value replacement; AVR = aortic valve replacement; DVR = double- value replacement.)
Mechanical Failure N o mechanical failures were observed. Autopsy was performed in two thirds of the patients who died. Valve failure was not suspected clinically in the remaining pa- tients.
Disk lnterference Two patients with MVR underwent reoperation for relief of disk interference. In both patients the disk impinged against the left ventricular wall, possibly because too large a valve had been chosen in relation to the left ven- tricular size. In both patients acute reoperation with reorientation of the valve was performed. One patient, who also had to be reoperated on twice because of bleed- ing, subsequently died. The other patient was asymp- tomatic but continued to have disk interference radio- graphically (disk opening angle reduced to 45-60 degrees). Interestingly, at a follow-up investigation 22 months after operation, when the heart rhythm had re- verted from atrial fibrillation to sinus rhythm, the disk
impingement had disappeared and the disk opened to the expected 70 degrees at all heartbeats.
Hemolysis Four patients had evidence of increased mechanical hemolysis. In 3 patients the hemolysis was associated with a periprosthetic leak. The fourth patient was the first patient described in the preceding section who was reoperated on three times. She received numerous blood transfusions and subsequently suffered from liver insuf- ficiency and hepatitis.
In 295 patients surviving beyond 30 days, preopera- tive and postoperative blood data to assess the degree of prosthesis-induced hemolysis were available (Table 3). With the exception of the 4 patients mentioned in the preceding section, all patients had normal postoperative hemoglobin values. In fact, most patients had a higher hemoglobin value after operation than before operation. Serum lactic dehydrogenase activity and reticulocyte count were only slightly elevated postoperatively, indi- cating that the degree of mechanical hemolysis was low and clinically compensated for in all patients.
Late Complications The overall freedom from late complications is shown in Figure 5. At 3 years, 84.5% of the patients in the MVR group, 81.2% in the AVR group, and 78.4% in the DVR group were free from late complications.
Comment The B-S M prosthesis was introduced in 1982 in an effort to overcome the strut fracture problem associated with some of the previous Bjork-Shiley models. Another ob- ject of the design change was to diminish the resistance to forward flow and to reduce turbulence beyond the valve. These aims were achieved by letting the convexo- concave disk open to 70 degrees and by increasing the relative size of the smaller orifice [6].
Aris and co-workers [7] have recently described the
Table 3 . Blood Data Collected fro& 295 Patients Suroiving Beyond 30 Days Postoperation
AVR MVR DVR
Variable Preop. <1 yr >1 yr Preop. <1 yr >1 yr Preop. <1 yr >1 yr
Hemoglobin (@d; 13.9 14.5 14.6 14.0 14.1 14.3 13.7 14.0 14.0 normal, 13.1- (N = 218) (N = 75) (N = 116) (N = 130) (N = 72) (N = 79) (N = 36) (N = 17) (N = 19) 16.3 gddl )
normal, 0.2- (N = 27) (N = 70) (N = 111) (N = 28) (N = 64) (N = 73) (N = 6) (N = 19) (N = 21) 1.5%)
normal; normal, (N = 177) (N = 75) (N = 112) (N = 129) (N = 69) (N = 79) (N = 39) (N = 23) (N = 20)
keticulocytes (%; 2.16 1.5 1.2 2.73 1.74 1.67 1.7 1.5 1.48
LDH (% of upper 98.7 113.4 103.4 111.1 112.4 117.1 114.9 133.9 144.4
<loo) Haptoglobin 1.37 0.33 0.37 1.46 0.45 0.25 1.4 0.13 0.08
(mg/ml; normal, (N = 44) (N = 64) (N = 91) (N = 31) (N = 61) (N = 58) (N = 9) (N = 15) (N = 16) 0.3-1.8 mg/ml)
= aortic valve replacement; MVR = mitral valve replacement; DVR = double-valve replacement; LDH = lactic dehydrogenase.

169 Thulin et al: Replacement with Bjork-Shiley Monostrut Valve
2 3 4 2 2 9 2 1 8 1 8 2 149 122 6 7
60 1 5 3 1 4 7 1 3 6 100 8 4 4 6 2 5
7 0 1 4 3 4 0 3 8 3 2 18 11 5
A V R
M V R
D V R
50' t I I 1 I
3 6 12 18 24 30 36
Time after surgery (months)
Fig 5. Actuarial incidence of event-free survival after heart valve re- placement with Bjork-Shiley Monostrut prostheses. (MVR = mitral valve replacement; AVR = aortic valve replacement; DVR = double- valve replacement .)
hemodynamic function of the B-S M valve in the aortic position. These authors found a mean resting systolic pressure gradient across the prosthesis of 12.7 * 6.3 mm Hg, which did not increase during exercise. Five pa- tients with a 21-mm prosthesis had a gradient of 15.5 * 8.1 mm Hg at rest.
The main purpose of the present investigation was to study the clinical performance of the B-S M, particularly with regard to durability, thromboembolism, and pros- thesis-related hemolysis. Follow-up was based on hos- pital visits at 9- to 12-month intervals. This method of active follow-up together with a rather wide definition of TEs probably results in a higher incidence of throm- boembolic complications compared with other studies of similar kind.
Table 4. Data from the Literature on Prosthesis-lnduced Hemolysis
In the total sample of 486 patients, with 537 prostheses implanted and observed from 6 months to 4 years, there was no instance of mechanical valve failure. Further in- formation concerning durability can be gained from a survey conducted in Europe in April, 1985, by one of the authors (C. L. 0.). A questionnaire was sent to 106 Euro- pean surgeons who were known to have used the valve. Eight surgeons (7.5%) did not want to participate, and 6 (5.7%) did not answer. Thus, 92 surgeons (86.8%) re- sponded. The survey involved 5,666 prostheses; 3,091 were used for AVR, 2,569 were used for MVR, 15 were used for tricuspid valve replacement, and 1 was used for pulmonic valve replacement. Thrombosis occurred in three implants (0.06%; 2 AVR, 1 MVR). In none of the approximately 5,000 patients observed for up to 3 years had structure valve failure been documented. Although the follow-up is short, it supports the impression that the B-S M valve is a durable prosthesis with a low inci- dence of thrombosis.
Evaluation of the incidence of thromboembolic com- plications was somewhat hampered by the inclusion of the early series of AVRs from the Karolinska Hospital, in which 33 of the patients were discharged without receiv- ing anticoagulants [3]. In this group there was 1 case of fatal valve thrombosis and 3 cases of systemic emboli. A second case of fatal valve thrombosis occurred in a pa- tient who stopped taking anticoagulants against the ad- vice of the investigator. If these cases are excluded, how- ever, no valve thrombosis occurred in the anticoagulated patients and the thromboembolic complication rate was equal to that reported for other comparable series of B-S convexoconcave valves [8].
The low rate of valve thrombosis with the B-S M pros- thesis was further substantiated by the previously
AVR MVR
Variable Preop. Postop. Percent Increase Preop. Postop. Percent Increase
Bjork-Shiley standard prosthesis LDH (% of upper normal) 95 104 9.5 90 91 1.1 No. of patients 184 239
LDH (% of upper normal) 98 138 40.8 88 120 36.4 No. of patients 84 88
LDH (% of upper normal) 96 145 51.0 91 132 45.1
Starr-Edwards prosthesis
Lillehei-Kaster prosthesis
No. of patients 44 53 St. Jude prosthesis
LDH (% of upper normal) 97 105 8.2 90 107 18.9 No. of patients 141 173
Bjork-Shiley Monostrut prosthesis (present series)
LDH (% of upper normal) 99 103 4.0 111 117 5.4 No. of pabents 177 112 129 179
AVR = aortic valve replacement; MVR = mitral valve replacement; LDH = lactic dehydrogenase Source: Adapted from Horstkotte et a1 [ll].

170 The Annals of Thoracic Surgery Vol 45 No 2 February 1988
mentioned European survey. We have chosen to use a rather broad definition of TEs, including TIAs and amaurosis fugax, and we believe that this has given us a truer figure for the overall incidence of TEs [9, 101.
With the exception of the 2 patients with valve throm- bosis caused by the absence of anticoagulation, there were no fatal TEs. Only a few of the patients had perma- nent sequelae. In the present study, there was no statis- tical correlation between the incidence of embolism and such variables as valve location, atrial fibrillation, history of preoperative embolism, and patient age. Further- more, there was no correlation between embolism and the type of suture ring used.
Disk interference was observed in 2 patients after MVR. Both patients were women with mitral stenosis, and both received large prostheses (29 and 31 mm, re- spectively). It is possible that too large a prosthesis was chosen in relation to left ventricular size in these 2 pa- tients. One patient was reoperated on twice, with reorientation of the disk. In addition, she was reoper- ated on twice because of bleeding, and she ultimately died of complications from the many operations and blood transfusions. The other patient was reoperated on once, with reorientation of the valve; thereafter, valve function was normal and she recovered from the opera- tion. Interestingly, a minor degree of disk impingement reappeared six months postoperatively and disappeared again one year later when sinus rhythm returned, offer- ing better ventricular filling.
The degree of mechanical hemolysis in the absence of periprosthetic leakage was low with the B-S M prosthe- sis. Compared with similar data from other types of valve prosthesis, the Bjork-Shiley valve prostheses in- cluding the B-S M valve appear to have a lower degree of mechanical hemolysis (Table 4) [9]. Hemolysis was com- pensated for by a slight increase in red blood cell pro- duction. This result means that DVR or even triple-valve
replacement can be performed safely with this prosthe- sis.
Although longer follow-up will be required to obtain definitive data, our observations suggest that the B-S M valve represents an improvement over the previous Bjork-Shiley models, particularly with regard to dura- bility.
References 1. Bjork VO: A new tilting disc valve prosthesis. Scand J
Thorac Cardiovasc Surg 3:1, 1969 2. Bjork VO, Lindblom D: The Monostrut Bjork-Shiley heart
valve. J Am Coll Cardiol 6:1142, 1985 3. Lindblom D, Lindblom U, Henze A, et al: Three-year clini-
cal results with the Bjork-Shiley Monostrut prosthesis. J Thorac Cardiovasc Surg 94:34, 1987
4. Lee ET: Statistical Methods for Survival Data Analysis. Bel- mont, CA, Lifetime Learning Publications, 1980
5. Helwig I, Council K (eds): SAS User’s Guide. Raleigh, NC, SAS Institute, 1979
6. Bjork VO: The optimal opening angle of the Bjork-Shiley tilting disc valve prosthesis. Scand J Thorac Cardiovasc Surg 15:223, 1981
7. Aris A, Crexells C, Auge JM, et al: Hernodynamic evalua- tion of the integral Monostrut Bjork-Shiley prosthesis in aortic position. Ann Thorac Surg 40234, 1985
8. Sethia B, Turner MA, Lewis S, et al: Fourteen years’ experi- ence with the Bjork-Shiley tilting disc prosthesis. J Thorac Cardiovasc Surg 91:350, 1986
9. McGoon DC: The risk of thromboembolism following val- vular operations: how does one know? J Thorac Cardiovasc Surg 88782, 1984
10. Edmunds LH: Thromboembolic complications of current cardiac valvular prostheses. Ann Thorac Surg 34:96, 1982
11. Horstkotte D, Aul C, Seipel L, et al: Influence of valve type and valve function on chronic intravascular hemolysis fol- lowing mitral and aortic replacement using alloprostheses. Z Kardiol 72:571, 1983


















