
Heart disease: Getting international collaboration right Chris Gale [email protected] Associate...
37
Heart disease: Getting international collaboration right Chris Gale [email protected] Associate Professor, Honorary Consultant Cardiologist University of Leeds, UK
-
Upload
stuart-henry -
Category
Documents
-
view
214 -
download
0
Transcript of Heart disease: Getting international collaboration right Chris Gale [email protected] Associate...
Heart disease:Getting international collaboration right
Chris Gale
Associate Professor, Honorary Consultant Cardiologist
University of Leeds, UK

Risk
of i
n-hs
pita
l all-
caus
e m
orta
lity,
odd
s ra
tio
Year of admission to hospital
Gale CP. Eur Heart J. 2012 Mar;33(5):630-9

Global cardiovascular careWesternised Rapid westernisation Developing
North America China AfricaWestern Europe India South America
High survival Resistant mortality High mortality
Guideline adherence Brisk implementation Primary preventionMedication adherence Organisational culture Secondary careNovel technologies Systems Ecological saturation
Care deficits Premature cardiovascular death
Lancet. 2012 Dec 15;380(9859):2095-128

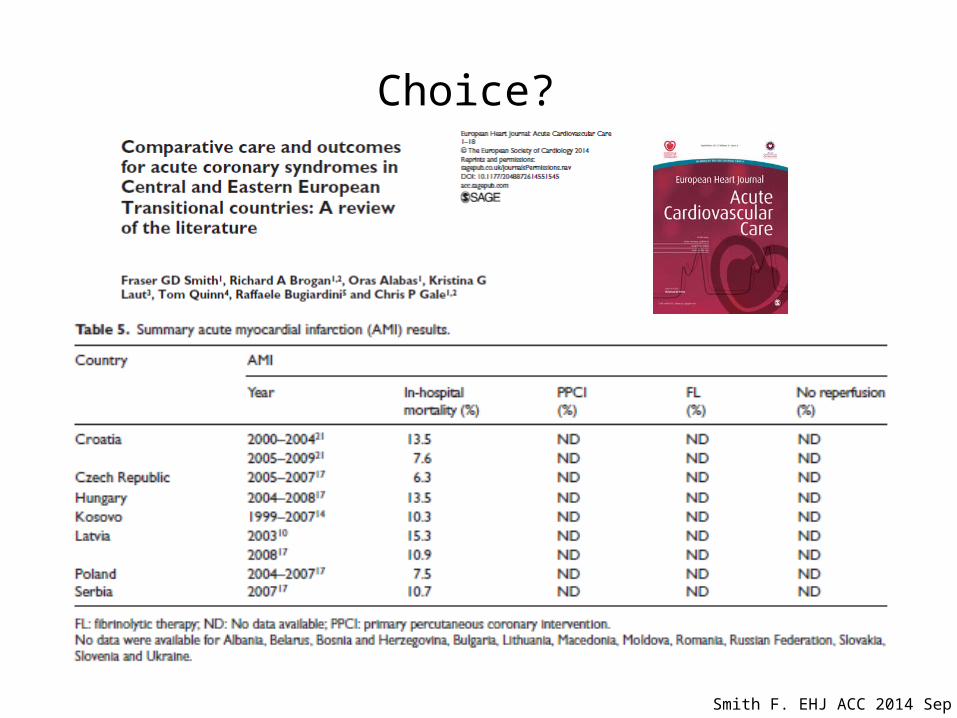
Smith FG. Eur Heart J Acute Cardiovasc Care. 2014 Sep 11
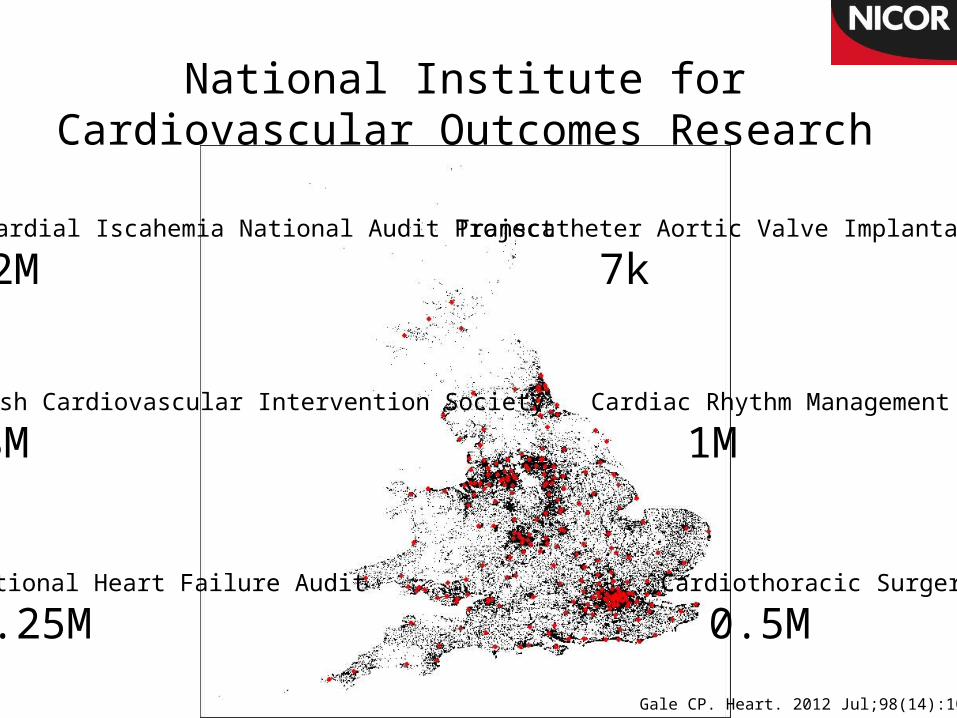
Myocardial Iscahemia National Audit Project
1.2MTranscatheter Aortic Valve Implantation
7k
National Heart Failure Audit
0.25M
British Cardiovascular Intervention Society
0.8M
Cardiothoracic Surgery
0.5M
Cardiac Rhythm Management
1M
National Institute for Cardiovascular Outcomes Research
Gale CP. Heart. 2012 Jul;98(14):1040-3

DTN times approximately constant throughout the day
PCI peak DTB at 0800 and trough at 1800
Eur Heart J. 2011 Mar;32(6):706-11
Door to treatment times, over 24 hrs
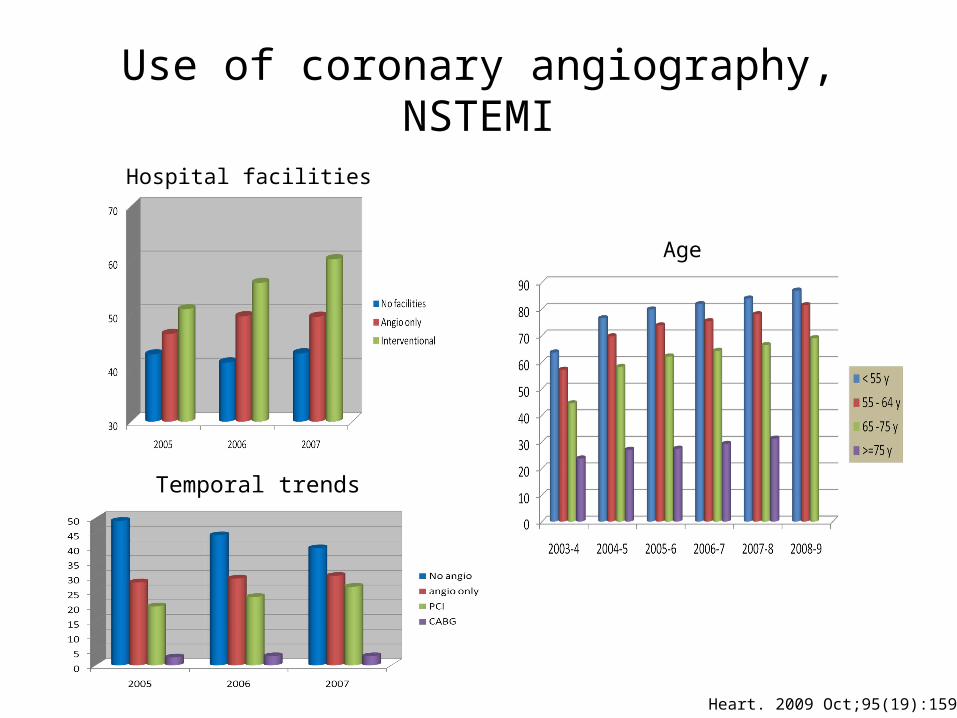
Use of coronary angiography, NSTEMI
Age
Hospital facilities
Temporal trends
Heart. 2009 Oct;95(19):1593-9

Old and new
Eur Heart J. 2011 Mar;32(6):706-11

More is less…..
Eur Heart J. 2011 Mar;32(6):706-11

……..is better
Eur Heart J. 2011 Mar;32(6):706-11

Reduced inequalities?
In-h
ospi
tal r
isk
of d
eath
, odd
s ra
tio
Year
30-
day
risk
of d
eath
, odd
s ra
tio
West RM. Eur Heart J. 2012 Mar;33(5):630-9Gale CP. Heart. 2014 Apr;100(7):582-9Alabas O. Age Ageing. 2014 Nov;43(6):779-85Gale CP. Int J Cardiol. 2013 Sep 30;168(2):881-7

Phenotype independent mortality
? System dependent mortality
Gale CP. Heart. 2011 Dec;97(23):1926-31

Cumulative missed opportunitiesProfile of each missed opportunities along the pathway of STEMI care, by CMOC group for patients eligible for all nine care opportunities.
Simms A. Eur Heart J Acute Cardiovasc Care. 2014 Sep 16.
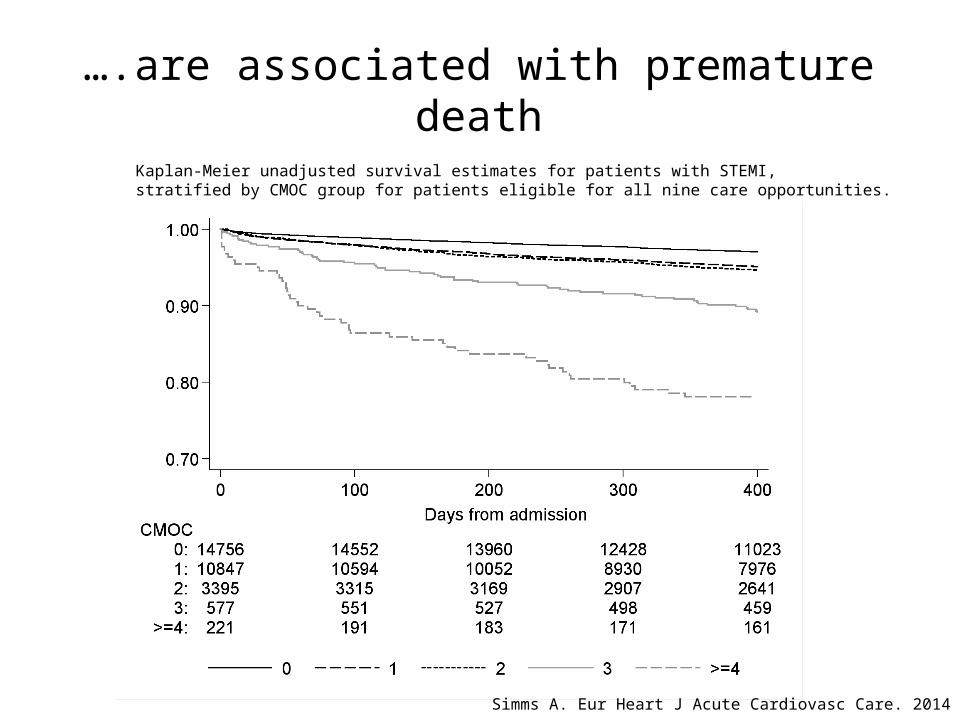
….are associated with premature death
Kaplan-Meier unadjusted survival estimates for patients with STEMI, stratified by CMOC group for patients eligible for all nine care opportunities.
Simms A. Eur Heart J Acute Cardiovasc Care. 2014 Sep 16.

International missed opportunities
Gale CP EuroIntervention. 2013 Aug 22;9(4):469-76Gale CP Int J Cardiol. 2013 Apr 19
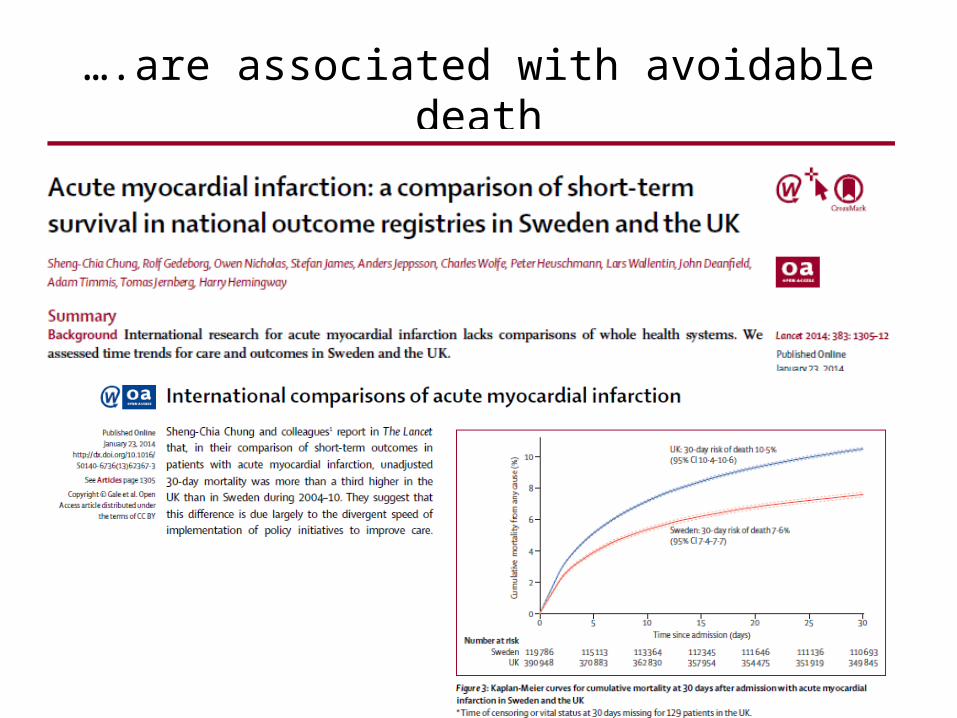
….are associated with avoidable death

Start (and finish) with the data
Lilford. Lancet 2004;363:1147

Missing by choice and chance

Chance?
• Complete case analysis may bias estimates
Spatial variation in missing data
Gale CP. Heart. 2011 Dec;97(23):1926-31
% missing data in key fields

So, what can we do?
Cases
Countries
Quality
Care
Facilities
Outcomes
Observational dataRetrospective – registriesProspective – snap shots
Randomised dataRCTRRCT

Big Data
MINAP
HFA
CRM
BCIS
CTS
NACR
Others
Gale CP. Heart. 2012 Jul;98(14):1040-3
Big Data
Big Data

Big Data
Big Data

Big Data
Big Data

Big Data

Big Data
Big Data

Big Data

EMMACE: data resolution
Electronic Health Record Linkage:
Acure coronary syndrome: MINAP
Status and cause of death: ONS
Hospital data: facilities questionanire
Health data: HES
Primary Care: The Phoenix Partnership
EMMACE-3
Admission One m
Six m One year
Consent into studies
Death
One year
Questionnaires: Admission / One month / Six months/ One year Drug adherence/compliance: Morisky Medication Adherence, Single Question Medicine Adherence, Beliefs about Medicine, The Adherence Estimator and Problems with Taking medications, Satisfaction with Information about Medicines Scale (SIMS), List of Medications Health Related Quality of Life: EQ-5D
Questionnaires: Admission / One month / Six months/ One year Drug adherence/compliance: Satisfaction with Information about Medicines Scale (SIMS), List of Medications Patient reported experience measure: Care Quality Commission Picker Inpatient -15Health Related Quality of Life: Brief Illness Perception (BIP), EQ-5D
Questionnaires: Annual Drug adherence: MacNew
Health Related Quality of Life: EQ-5D
Six months
One month
Annual
EMMACE-3X
EMMACE-4
Alabas O. BMJ Open 2014 in press

Pyramid of evidence
validitybias
-to determine the optimal approaches to healthcare interventions and delivery
cmRCT High validityLow bias

Cohort multiple RCT
Regular outcome measurement
Large observational cohortEligible patients identified
Remaining patients
Randomised to intervention
Usual care
Relton C. BMJ. 2010;19:340

GRACE RRCT
Data collection: MINAP, survey survey, NICOR, ONS

Acknowledgements
• Funders:– British Heart Foundation– National Institute for Health Research
• Institutions:– University of Leeds– National Institute for Cardiovascular Outcomes
Research, UCL• Team: