
Heart and Circulation: Dysfunction (PHSI3008)
18
Heart and Circulation: Dysfunction (PHSI3008) Table of Contents 1. Developmental defects 2. Tumour angiogenesis 3. Haematological disorders 4. Neurogenic regulation of blood pressure 5. Stress 6. Cardiorespiratory and neurotransmitters 1 7. Cardiorespiratory and neurotransmitters 2 8. Muscular dystrophy 9. Cellular mechanisms of remodeling and hypertrophy 10. Hypertension 1 11. Hypertension 2 12. Hypertension 3 13. Obesity 14. Diabetes 15. Atherosclerosis 1 16. Atherosclerosis 2 17. Atherosclerosis 3
Transcript of Heart and Circulation: Dysfunction (PHSI3008)

Heart and Circulation: Dysfunction (PHSI3008)
Table of Contents
1. Developmental defects 2. Tumour angiogenesis 3. Haematological disorders 4. Neurogenic regulation of blood pressure 5. Stress 6. Cardiorespiratory and neurotransmitters 1 7. Cardiorespiratory and neurotransmitters 2 8. Muscular dystrophy 9. Cellular mechanisms of remodeling and hypertrophy 10. Hypertension 1 11. Hypertension 2 12. Hypertension 3 13. Obesity 14. Diabetes 15. Atherosclerosis 1 16. Atherosclerosis 2 17. Atherosclerosis 3

Dysfunction: Developmental Defects
The most common developmental abnormalities of the cardiovascular system are
• Vascular malformations e.g. HHT • Congenital heart defects e.g. Sudden Cardiac death
Hereditary Haemorrhagic Telangiectasia (HHT)
• Genetic disorder • Haemorrhagic= the integrity of the vessel is not strong enough
to cope with the pressure so gaps form and blood cells leak out into the tissue.
o Leads to abnormal blood vessel formation in a range of organs, skin, mucosa, lungs, liver, brain.
• Telangiectasias are small vascular malformations. Are small dilated blood vessels near the surface of the skin or mucous membranes (spider veins)
o Can lead to nosebleeds, red spots appear on the tongue, lips, nose and fingers.
o Can extend to larger vessels in critical organs like the brain, kidneys and heart.
o Patients often have arteriovenous malformations- Arteriovenous malformations (AVM)
• Hard to pick what is an artery and what is a vein • Usually develop as a complex mass of disorganised arteries and
veins – distorted, abnormal. Sometimes they lead to nowhere and then the blood builds up.
• The arteries and veins are directly connected to each other without capillaries joining them
• Most commonly found in the brain and spine • But can found throughout the body including in the thorax liver
and other organs. Genetic defects in HHT
• Monogenetic mutations (mutation in one gene alone) in either Endoglin or Alk 1 genes have been linked to HHT.
• Endoglin is a cell surface protein expressed on endothelial cells (angioblasts in embryo), some hematopoietic cells (some blood

cells) and also smooth muscle cells (that line the blood vessels to maintain integrity) during heart development.
Endoglin (TGF-b receptor 3) signalling
• Endoglin interacts with receptors for TGF b to stabilise the interactions between the receptor and growth factor. Endoglin doesn’t actually bind TGFb receptors.
• There two types of TGFb receptors. • TGFb hormone binds to either
o One has Alk5 and TbR-2 (TGFbeta receptor 2 chain) o The other has ALK1 and TbR-2
• Endoglin stabilises the whole complex • Endoglin is not completely essential for TGFbeta signalling but it
is extremely supportive of it. • If you have a mutation in endoglin, endoglin wont interact with
the complex and everything that happens downstream (growth and proliferative signals) of it is slightly reduced (not completely reduced)- it is controlling the volume of the signal.
• Mutations in ALK1 do not result in a complete loss of ALK1, it results in ALK1 being slightly less effective
Once TGFbeta is bound, it will result in phosphorylation of proteins like SMADs which move to the nucleus to switch on a whole lot of genes.
Systemic vascular problems in HHT

• You end up with vessels that are not sure what they are supposed to be, where they are supposed to end and what they are supposed to be connecting with
• In HHT patients the artery could be directly connected to the veins (seen in red in the diagram)= problem with patterning
o They are exposed to much higher pressure than they are built for- venules rupture and you get nose bleeds etc. Blood pressure much lower in the veins than the arteries and so cannot cope with it.
• End up with high blood pressure. • In lungs- Post capillary pulmonary hypertension (PCPH): blood
coming from a major artery into a vein. Weakens the vessels and they have more problems
o Normal system in black.
If you do actually wipe out endoglin
• The embryos will die at mid-gestation from vascular defects • (but in patients they are only slightly reduced) • Vasculogenesis appears normal • The next event is angiogenesis- in this disease, defects are in
blood vessel re-modelling. o Aorta is very small. TGFbeta is not making it grow or
proliferate and stretch. Endothelial cells are confused. Smooth muscle cell defects in endoglin knockout mice
• Vascular smooth muscle cells stabilise blood vessels, expand and contract with blood pressure

• Smooth muscle cells are missing in knockout mice – the aorta doesn’t have ANY muscles anymore. The aorta needs heaps of support so you don’t get haemorrhages.
• TGFbeta signalling regulates vSMC differentiation. • Lack of Endoglin reduces TGFbeta signalling, affects vSMC
differentiation and disrupts angiogenesis • Problem of integrity. = the disease is problem of integrity plus problem of patterning
Treatment for HHT • Surgery: Some of the vessels you want to snip out and get rid
of. Very dangerous though • Could give patients a drug called Thalidomide: it 1. Stops
abnormally growing vessels from growing. 2. Will stimulate mural cells (smooth muscle cells) and give them growth signals.
o Thalidomide is famous for birth defects- stops morning sickness. Also produced problems with limb development (shortened limbs).
• Bevazicimub: o It is an antibody against VEGF-A. VEGFA bind to receptors
on endothelial cells and induces proliferation. The receptor for VEGF receptor is still switched on in the bad vessels (cos they haven’t gotten the good growth factors, on all of the other normal vessels it is switched off). Give antibody that will block VEGFA and will block the proliferative signal in the AVM and will calm down the vessel.
• Give them more TGF-Beta1. Congenital Heart Defects
• Defects in the heart and major blood vessels connecting the heart present at birth
• The most common birth defects in humans, 2 in 100 live births have congenital heart defects
• Leading cause of non-infectious newborn deaths

Causes • 40% are unknown • some of them are due to infection during embryonic
development • Teratogens in the environment (makes the embryo terrible e.g.
the weed and cyclops) • Chromosomal abnormalities
What types of congenital heart defects (CHD) can you have?
• Hypoplasia: underdevelopment of the heart. • Obstruction defects: problems blocking any point in the heart
and the vessels around the heart • Septal defects:
o atrial and ventricular chambers are not appropriately partitioned. Atrial septal defects occur in 1 in 1500 live births.
• Cyanotic defects: o defects where the pumping of myocardium is not effective
enough to get all of the oxygenated blood out that we require.
o Classic sign is cyanosis= blue lips. Deoxygenated blood. Transcription factors
• NKx2.5= Tin man. It comes in again and interacts with other transcription factors to form specific chambers- atrial versus ventricle myocytes. Important in Atrial Septal Defects, AV block, Ventricular septal defects VSD, TOF (Tetralogy of Fallot- cyanotic heart defect

Nkx-2.5 is mutated in some CHD patients • Doesn’t wipe out the whole thing- you wouldn’t be born • During embryogenesis blood flows through a hole in the septum
primum • This hole (foamen ovale) is closed shortly after birth
• Nkx2.5 is important in AV node formation
• In some patients with Nkx2.5 point mutations this hole is not
closed. After birth- blood from right atrium to left atrium- mixing of oxygenating and deoxygenated blood
o The mutations are in the DNA binding homeodomains of the Nkx-2.5 and lead to haploinsufficiency
§ = only one gene works (the other copy is inactivated by the mutation)
o Nkx2.5 is a transcription factor- some bits are binding directly to the actual DNA. Other parts of it are forming the architecture that allows it to bind to DNA.
o So this is a problem with the DNA binding domain itself
• Another mutation could affect which part of the DNA it binds to o E.g. 6 year old with abnormal ECG. Required a pacemaker
by the age of 14 o Even with a pacemaker, he still unexpectedly died of late
stage heart failure. o Many of his family in Oregon had inherited atrial septal
defects Specific mutation of Nkx-25 within the ventricular cardiomyocytes leads to CHD
• Conditional deletion of nkx2-5 by Cre excision • Ventricular specific promotor-MIC2v drives Cre expression
= Floxed Nkx2-5 is deleted only in the ventricular cardiomyocytes
o rest of the heart developed normally o This lead to cardiac hypertrophy o When the Nkx2-5 is deleted, ventricular cardiomyocytes
proliferate and form more trabecular o Disrupts heart function and can lead to sudden cardiac
death The trabecular come out of the base of the left and right ventricle. Connect to the valves and help push the blood out
• BMP10 is a soluble growth factor in the TGFb family. • Absolutely essential for trabecular formation • Expressed in the trabecular myocardium of the ventricles and
atria o BMP10 knockout mice die in utero o BMP10 deficient hearts exhibit rhythmic contraction but at
a significantly slower rate compared to normal. Don’t get as much oxygen (43 beats/min verus normal 96 beats per min)
What’s the link?

• Sectioned through the hearts of Oregon family. The Nkx2.5 mutant has such a constricted ventricle that the space the blood will flow through is coming smaller and smaller
• Nkx 2.5 normally switches off the expression of BMP10 (represses it)
o BMP10 is expressed at a huge level and controls trabeculation and just kept going from embryogenesis onwards. Because there is no repression.
So problems they get when there is a nkx-2.5 deficiency
• Hole in the heart needs to be fixed • Irregular heart beats- need a pacemaker • Excess trabeculation/ excess cell proliferation (BMP-10) • Septal defects • Outflow tract defects • Hypoplasia of the left heart • Hypertrophy of the left ventricle • Arrhythmias • Cardiomyopathy • Complete knockout of nkx is lethal.

Tumour Angiogenesis
Vasculogenesis: • The initial formation of the vascular plexus via de novo (from
scratch) production of endothelial cells Angioblast:
• Endothelial progenitor cell- can form vessels and proliferate. In the embryo. Can be reactivated in the adult in disease
Angiogenesis: • the formation and re-modelling vasculature to develop new
vessels. Ateriogenesis:
• specification and generation of the arteries Lymphangiogenesis:
• formation of lymphatic vessels Lymphatic vessels
• Unidirectional • Does not rely on the heart • Tissue fluid gets squeezed out when blood cells flow through • Pours it all into the subclavian vein. • Tumours also hijack neighbouring blood vessels
Vasculogenesis
• Groups of angioblasts arise from the mesoderm • These angioblasts form a basic structure called the primary
vascular plexus. • Only happens in the embryo
Angiogenesis • Generation of novel blood vessels from pre-existing vessels

• Re-modelling of pre-existing vessels via sprouting and branching. • Can happen in the embryo, childhood, wound healing and other
diseases. Formation of a closed vascular system
• Within microcapillary networks, there will be cells that were veins that have decided to be lymphatic vessels.
• Attracted supporting cells to come in – pericytes (aka mural cells aka vascular smooth muscle cells all pretty much the same).
Growth factors are crucial in angiogenesis
Angiogenesis also occurs during embryogenesis but can be re-activated in adults
• Wound healing:

o Angioblasts appear and add themselves to the local vessels and push them into the wound to bring oxygen into the wound to heal it.
• Pregnancy-placenta development o Angiogenesis in pregnant mother. o Placenta huge sponge of vascular network on child’s side
and mothers side. • Inflammation
o Angioblasts enter sites of inflammation to set up new vessels and bring in oxygenated blood in
• Diabetic retinopathy o Blindness in diabetic patients
• Tumour development and growth Tumour Angiogenesis
• Cancer will only reach a dangerous size (needs to be bigger than 1 square centre meter) if it can hijack and create a closed circulatory system. Concept was first proposed by Judah Folkman in 1971.
• Large tumours are highly vascularised. Tumours= an organ. o Avascular tumours fail to expand and rapidly become
necrotic internally. If there is a mutated oncogene but it fails to recruit a vascular system, then it could form a harmless microscopic tumour. It needs Angiogenesis to go down the lethal tumour pathway. This is the “Tumour angiogenic switch”
• Universal target for therapies as all large tumours needed to develop a vasculature to expand- not dependent on the cell type of origin of the tumour (can use it on any type of cancer- liver, bone)
Tumours form a vasculature to get
• Important growth requirements (oxygen, nutrients). All tumours require nutrients from the host for survival and expansion
• Dispose of waste products

• Tumours initially get nutrients from absorbing it via simple diffusion. However to grow beyond the size of 1mm diameter it needs vessels.
• The more microvessels feeding the tumour- the worse the outcome for the patient.
• On one side you have the tumour cells with a big mass • Driven by hypoxia, the tumour gives off a series of growth
factures o VEGF which induce endothelial cells to proliferate and to
come towards a targeted area (chemotactic signal) o produce PDGF: platelet derived growth factor. Good at
inducing pericytes or vascular smooth muscle cells to proliferate, expand and cover a blood vessel.
o bFGF: basic fibroblast growth factor- mitogen encourages cells to proliferate and attracts cells. Induce expression of molecules that cause endothelial cells to sprout off the main artery and come towards it.
• Inflammatory cells support angiogenesis- mast cells, neutrophils etc.
• Hypoxia turns on the angiogenic factors.

Tumour angiogenesis requires a range of different cell types
• Stromal cells- fibroblasts around it. It will support the endothelial cells. Tricking fibroblasts to produce more angiogenic factors.
• Pericytes: attracted to area. • Macrophages are associated with tumours- can help or hinder
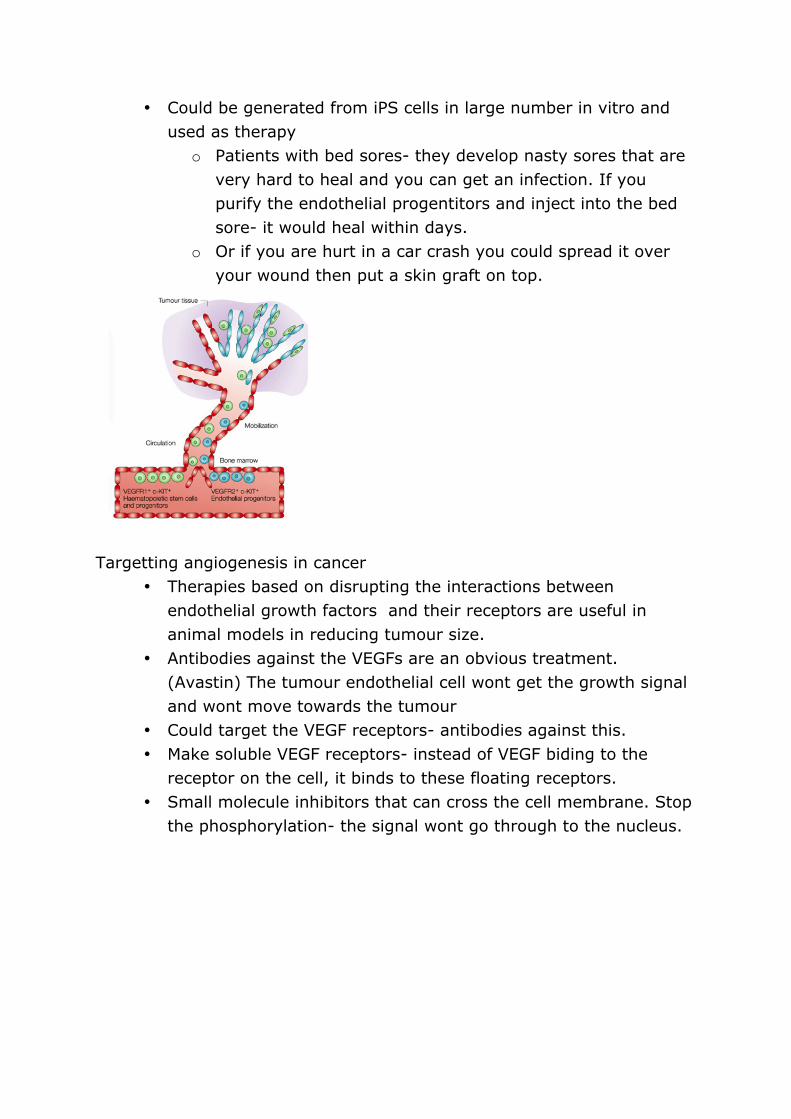
blood vessels • Platelets • Endothelial progenitor cells are released from the bone marrow,
circulate, home into areas where the new vessels are being produced and the tumour grabs them and incorporates them.
• SDF-1 is a potent chemokine “hey youre a cell that has a receptor for me, come here” good way of attracting a sprouting endothelial cell to come towards it.
Endothelial progenitor cells
• Released during wound healing and pregnancy. • Very proliferative • Very rare circulating cells- usually in the bone marrow • Capable of contributing to new blood vessels • Can be purified and expanded in vitro in a dish. You can give
them back to a patient when you need it.
• Could be generated from iPS cells in large number in vitro and used as therapy
o Patients with bed sores- they develop nasty sores that are very hard to heal and you can get an infection. If you purify the endothelial progentitors and inject into the bed sore- it would heal within days.
o Or if you are hurt in a car crash you could spread it over your wound then put a skin graft on top.
Targetting angiogenesis in cancer
• Therapies based on disrupting the interactions between endothelial growth factors and their receptors are useful in animal models in reducing tumour size.
• Antibodies against the VEGFs are an obvious treatment. (Avastin) The tumour endothelial cell wont get the growth signal and wont move towards the tumour
• Could target the VEGF receptors- antibodies against this. • Make soluble VEGF receptors- instead of VEGF biding to the
receptor on the cell, it binds to these floating receptors. • Small molecule inhibitors that can cross the cell membrane. Stop
the phosphorylation- the signal wont go through to the nucleus.

You can also target Lymphatic vessels for cancer therapies
• Lymphatic vessels are the main route for metastatic dissemination of tumour cells
o No lymphatics= the tumour would be stuck there. • Tumour cells produce soluble factors to attract lymphatic
endothelial cells • Targeting lymphatics can reduce tumours • Target- block VEGF-C so it cant be used by lymphatic vessels. Or
target the receptor. • Tumours ride on the lymphatic highway to move around and get
to the lymph nodes.

Targets for anti-angiogenic therapies Endothelial cells
• Growth factor receptors • Chemo-attractant receptors • Adhesion molecules • Transcriptional regulators • Hypoxia helps tumours
Other cell types • Angiogenic growth factors • Chemo-attractants • Growth factors regulating supportive cell types • Adhesion molecules
Targeted anti-angiogenesis therapies for Diabetetic Retinopathy (DR)
• DR is the leading cause of blindness of adults • Too many endothelial cells proliferating over the retina,
obscuring vision • VEGF is over-expressed in the proliferating diabetic retina • You can use anti-angiogenic therapy to treat it: Narrow needle,
inject through the sclera into the vitreous humour (intra-vitreal injections) and it will heal completely (no hole left).
• Changes in glucose in the circulation sets off angiogenesis over the retina. There are normal amount of blood vessels + way too many more. The old ones no longer need VEGF.

Also useful for macula degeneration- excess buildup of blood vessels over the retina. Anti-VEGF treatment. Pro-angiogenic therapies
• Angiogenic factors can be used in diseases where there is poor, damaged or abnormal blood vessel formation
• Cardiovascular disease treatment: assist in the disease such as coronary artery disease
o Help rejuvenate the coronary arteries- give them a growth signal to proliferate and go back to normal structure.
• Treatment of ischaemic damage • Bed sores: VEGF injections significantly improve healing.
o Can inject VEGF into the bed sore and it will heal. PHSI 3008: Find a way to stop the vessels getting in to the cancer. Target the FGF, angiogenic factors, chemoattractants. Use something that will only be active in embyros. Cos the normal shouldn’t have it.


















