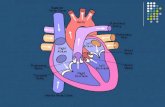
Heart
23
Emily Moore Calle Linden The Dinh Thi FACTORS THAT INFLUENCE A CHANGE IN BEHAVIOUR TO INCREASE THE HEALTH OF HEART FAILURE PATIENTS
-
Upload
emilymoore27 -
Category
Health & Medicine
-
view
433 -
download
2
Transcript of Heart

Emily MooreCalle LindenThe Dinh Thi
FACTORS THAT INFLUENCE A CHANGE IN BEHAVIOUR TO
INCREASE THE HEALTH OF HEART FAILURE PATIENTS

FACTORS INFLUENCING SELF-CARE
No opportunities to teach patients
Not sufficient knowledge to teach patients
Nurse´s responsibilities
Insufficient self-care
Hard to change habbits
See no reason
Fatigue
Easily tired
Don’t know what to do
Don’t know how to do
Have difficulty learning
Decreased memory
Motivation Knowledge
Barriers

Cost-eff ective way to treat patients Decreased risk for readmission Shorter stay at hospital
Improve situations in everyday lifeProvide the patients with active decisions
Gives the patient a feeling of control Improving compliance to treatments
Better understanding for treatments gives an improved compliance
WHY SELF-CARE?

Removing barriers Chronic degradation Physical exercise may reduce symptoms
6MW
Organizational improvements/Nurse´s responsibiliti es Heart failure receptions Individual assessment of opportunities
Improving motivation
FACTORS INFLUENCING SELF-CARE

Telephone-delivered education Individual with follow up The patient can be at their home
Significant improved knowledge (Baker, Darren 2011).
Web-based education Increases patients access to knowledge and possibility to
share information Requires close to non experience using computers
TOOLS FOR IMPROVING PATIENTS KNOWLEDGE

Video educations Patients are free to choose whenever they wish to learn
Improved compliance to self-care (Albert, Buchsbaum & Li, 2007)
Education session at hospital Ensure the patient receive information prior to discharge
Reduced the risk for readmission (Krumholz et al., 2002)
TOOLS FOR IMPROVING PATIENTS KNOWLEDGE

Helping patients change behavior is an important role for family physicians
Change interventions are especially useful in addressing lifestyle modification for disease prevention, long-term disease management and addictions.
The concepts of “patient noncompliance” and motivation often focus on patient failure.
Understanding patient readiness to make change, appreciating barriers to change and helping patients anticipate relapse can improve patient satisfaction and lower physician frustration during the change process.
MODEL OF IMPROVEMENT

1. What change are we testing - what is the objective of the test?
2. Who is included in the test - who will be involved in the testing process (nurses, QI team, staffi ng) and on whom will the test be conducted (patients with urinary incontinence)?
3. When are we testing (start and end date)?4. Where are we testing?
PLAN

To change behavior, the patient must understand what to do and how to do it. The patient needs enough knowledge to adjust the treatment or prevention regimen in response to changing circumstances.
Learning relies heavily on the educator's ability to adapt teaching strategies to the individual and on the patient's ability to process information. Because poor glycemic control and cognitive dysfunction are associated, it is among the numerous factors that can aff ect the ability of the patient with diabetes to process information.

Doing the test. Collecting data for analysis - complete the chart audits,
collect whatever data is needed to help complete the quality picture.
Carrying out the Change - work the plan. Documenting problems - note any problems encountered
along the way. This will assist you in analyzing this cycle and in avoiding problems in the future.
Collecting Data - what information are you finding as you work the plan?
Beginning Analysis - make observations and begin analyzing the findings and continue to document expected and unexpected observations along the way.
DO

In this phase an organization should study the data and determine what was learned.
List out problems, successes and surprises specifically so that you can substantiate your conclusions and have the list as a resource for future QI cycles.
STUDY

It is important at this stage to set up a specific plan with detailed action steps that will help maintain or hold any gains and that improvements continue over time.
In the ACT stage, organizations also should establish a new plan for next PDSA cycle and begin the cycle over again. (continue to explain patient motivation of techniques that have been developed for influencing patient behavior.)
ACT

Ten success characteristics 1. LeadershipSetting and reaching collective goals, and to empower individuals autonomy and accountabil ity• Ask -- raise the issue• Advise -- increase awareness of risk and benefi ts related to behaviour• Assist -- help the patient to identify a negotiated SMART (specifi c, measurable, achievable, realistic, t imed) goal related to behaviour change and signpost if appropriate.
2. Organizational supportThe larger organization looks for ways to support the work of the Microsystem3. Staff focusExpectations of staff are high regarding performance, continuing education, professional growth, and networking
CLINICAL MICROSYSTEMSCLINICAL MICROSYSTEM TOOL

4. Education and TrainingOff ering training and education courses on the management and proper treatment of heart failureProcesses to change lifestyle5. Interdependence The interaction of staff is characterized by trust, collaboration, willingness to help each other, appreciation of complementary roles, respect and recognition that all contribute individually to a shared purpose.6. Patient FocusThe primary concern is to meet all patient needs – caring, listening, educating, and responding to special requests,

7. Community and Market FocusEstablish innovative relationships with the community; The Microsystem is a resource for the community; the community is a resource for the MicrosystemInitiatives in the community8. Performance ResultPerformance focuses on patient outcomes, avoidable costs, streamlining delivery, using data feedback9.Process ImprovementLearning and redesign is supported by the continuous monitoring of care, use of benchmarking, frequent tests of change10. Information and Information TechnologyTechnology facilitates eff ective communication

NICE- National Institute for Health and Clinical Excellence. Let's Get Moving initiative 2007-recommendations for health professionals on interventions for patientse.g.• learning to spot things that trigger or reinforce the unwanted behaviour• setting goals and planning how to achieve them• building confidence to make important and wanted changes• self-monitoring• creating SMART action plans• building social support through signposting• rewarding success.

Four commonly used methods to increase physical activity
Brief interventions – advice delivered by GPs and other non-hospital-based health professionals.
Exercise referral schemes – referral to a tailored physical activity programme.
Pedometers – use of a device to measure how far you have walked.
Walking and cycling schemes

Strömberg, A. (2005). The crucial role of patient education in heart fai lure. The European Journal of Heart Fai lure, 7, 363–369
Koell ing, T. , Johnson, M., Cody, R. & Aaronson, K. (2005). Discharge education improves cl in ical outcomes in patients with chronic heart fai lure. Journal of the American association, 18 , 179-185.
Krumholz, H., Amatruda, J . , Smith, G., Mattera, J . , Roumanis, S. , Radford, M. et al. (2002). Randomized Trial of an Education and Support Interventions to prevent Readmission of Patients With Heart Fai lure. Journal of the American College of Cardiology, 39, 83-89.
Kwok, T., Lee, J . , Woo, J . , Lee, D. & Griffi th, S. (2008). A randomized control led tr ial of a community nurse-supported hospital discharge programme in older patients with chronic heart fai lure. The author journal compilation, 17, 109-117
Ricard, Camarda, R., Foley, L. , Givertz, M., & Cahalin, L. (2011). Case report: exercise in a patient with acute decompensated heart fai lure receiving posit ive inotropic therapy. Cardiopulmonary Physical Therapy Journal, 22(2) , 13-18.
Mårtensson, J . , Strömberg, A., Fr idlund, B. & Dahlström U. (2001). Nurse-led heart fai lure cl inics in Sweden. European Journal of Heart Fai lure, 3, 139-144.
REFERENCES

Shearer, N., Cisar, N., Greenberg, E. (2007). A telephone-delivered empowerment intervention with patients diagnosed with heart failure. Heart & Lung, 36, 159-169.
Baker, D., Dewalt, D., Schillinger, D., Hawk, V., Ruo, B., Bibbins-Domingo, K. et al. (2011). The eff ect of Progressive, Reinforcing Telephone Education and Heart
Failure Symptoms. Journal of Cardiac Failure, 17 , 789- 796.Domingues, F., Clausell, N., Aliti, G., Dominguez, D., Rabelo, E. (2011). Arq Bras Caridol. Brasilien
Lindén, C. et al. (2011). Web-based patient education for patients with heart failure.
Albert, N., Buchsbaum, R., Li, J. (2007). Randomized study of the eff ect of video education on heart failure healthcare utilization, symptoms, and self-care behaviors. Patient Education and Counseling 69, 129- 139.
Krumholz, H., Amatruda, J., Smith, G., Mattera, J., Roumanis, S., Radford M., Crombie, P., Vaccarino, V. (2002). Journal of the American College of Cardiology
REFERENCES

Carole Lannon, MD MPH. Jacqueline Dunbar- Jacob, PhD, RN, FAAN. Models for
Changing Patient Behavior: Creating successful self-care plans
Eraker SA, Kirscht JP, Becker MH. (1984)Understanding and improving patient compliance. Ann Intern Med, 100:258-268
Michelle A. Dart. (2011). Motivational Interviewing in Nursing Practice: Empowering the Patient
REFERENCES

NICE. (2006). Four commonly used methods to increase physical activity. Retrieved from http://publications.nice.org.uk/four-commonly-used-methods-to-increase-physical-activity-ph2Huber, T.P., Kurtin, P., & Seid, M. (2006). Clinical microsystem assessment diagnostic.Retrieved from http://www.dhcs.ca.gov/provgovpart/initiatives/nqi/Documents/MSAssessmentFinal.pdfHayes, S. (2010). Brief interventions to change behaviour. Practice Nurse, 39 (6). Retrieved from http://web.ebscohost.com.dbgw.lis.curtin.edu.au/ehost/detail?vid=5&hid=17&sid=8517c172-8956-48cb-b335-ed8caca8b5dd%40sessionmgr13&bdata=JnNpdGU9ZWhvc3QtbGl2ZQ%3d%3d#db=rzh&AN=2010612148
REFERENCES

Looked at the problems in our previous presentation-nursing knowledge-patient knowledge-lifestyle behavioursChose lifestyle behaviours as the main focus as the
other two factors also tied into this problemUsed university library data bases and government
websites
SEARCH PROCESS

We each were allocated a tool and applied it to behavioural changes
Calle and The both presented in previous presentations, Emily will present today
Each member did their own powerpoint slides, Emily produced the final product
COLLABORATION PROCESS