Healthy Urban Planning in European Cities

of 9
Transcript of Healthy Urban Planning in European Cities
-
7/30/2019 Healthy Urban Planning in European Cities
1/9
Healthy urban planning in European citiesHUGH BARTON1*, MARCUS GRANT1, CLAIRE MITCHAM2 andCATHERINE TSOUROU31WHO Collaborating Centre for Healthy Cities and Urban Policy, School of Built and NaturalEnvironment, University of the West of England, Bristol, United Kingdom, 2Baker Associates, Bristol,United Kingdom and 3Consultant, Padua, Italy*Corresponding author. E-mail: [email protected]
SUMMARYThis article describes the WHO healthy urban planning
(HUP) initiative as it has developed through the labora-
tory of the Healthy Cities movement and evaluates the
degree to which applicant cities successfully developed
plans for HUP. The paper provides a brief historical per-
spective on the relationship of health and planning and an
overview of the ways in which urban spatial development
affects health. It then turns to the WHO European
Healthy Cities Network (WHO-EHCN) and explains the
evolution of the HUP programme through Phase III
(19982002) of the Healthy Cities Project, showing how
the programme has grown from experimental beginnings
to being mainstreamed in Phase IV (20032008). Each
city wishing to join the WHO-EHCN in this latter phase
produced a programme for further development of HUP,
and these were assessed by the Bristol Collaborating
Centre. The paper presents the overall results, concluding
that a significant progress has been made and the most
advanced cities have much to offer municipalities every-
where in the best practice for integrating health into urban
planning.
Key words: Healthy Cities; urban planning; healthy environment
INTRODUCTION
Health and urban planning are natural allies.Modern town planning has its roots in theunhealthy industrial cities of the nineteenthcentury: endemic problems of poor watersupply, sanitation, light and air triggered aresponse in terms of not only infrastructure
engineering but also urban design. The codes ofstreet and building layout were designed tobanish forever the dank houses and airlessstreets.
It is ironic, then, that the connection betweenhealth policy and urban planning becametenuous in the twentieth century. The originalhealth objectives of clean air and water aredeeply entrenched in planning and buildingcontrol systems, but contemporary diseases of
civilization have been ignored in many ways.Indeed, planning policies have facilitated if notactually fostered the powerful trends towardscar-dependent, sedentary and privatized life-styles, with their negative effects on health.
This paper highlights the important work ofthe Healthy Cities movement in seeking toreintegrate health and planning. The first
section sets out the nature of the link and theproblem of separation; the second section sum-marizes the evaluative methods used. Theresults are in two parts: an examination of theevolution of the WHO healthy urban planning(HUP) initiative, from inception, through pilotprojects, to mainstreaming, and an evaluation ofthe progress made by the cities over Phase III(19982002) as evidenced by their applicationsfor Phase IV (20032008). Subsequent
Health Promotion International, Vol. 24 No. S1
doi:10.1093/heapro/dap059
# The Author (2009). Published by Oxford University Press. All rights reserved.
For Permissions, please email: [email protected]
i91
-
7/30/2019 Healthy Urban Planning in European Cities
2/9
discussion points to five key elements in anideal health-integrated planning system, con-cluding that health is a powerful motivator,capable of cutting across sectional interests inthe process of city planning.
URBAN PLANNING AS ADETERMINANT OF HEALTH
The environment has long been recognized as akey determinant of health (Lalonde, 1974;Whitehead and Dahlgren, 1991; Marmot andWilkinson, 1999). The health-related professionsincreasingly recognize that promoting healthsolely through programmes of changing the be-haviour of individuals or small groups is notvery effective, reaching only a small proportionof the population and seldom being maintained
in the long term (McCarthy, 1999; Lawlor et al.,2003). What is needed is a more fundamental,social, economic and environmental change.
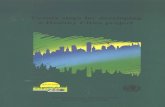
Urban planning as a mechanism of environ-mental control influences health in systematicways. Figure 1 sets out a settlement health map,showing the various spheres of social and econ-omic life and the wider environment that areaffected by the spatial planning of settlements(Barton, 2005; Barton and Grant, 2006). It wasinspired in part by Whitehead and Dahlgrensfigure (Whitehead and Dahlgren, 1991), of the
determinants of health, and in part by the eco-system model of human habitats (Duhl andSanchez, 1999). The sphere of direct planninginfluence is the built environment: here definedbroadly to mean the physical form and manage-ment of places: the buildings, spaces, streets andnetworks that make up human settlements. This
sphere affects all the others to a greater orlesser extent, helping to shape some of theoptions that are open to individuals, socialgroups, businesses and state agencies. Forexample, through the provision (or lack of pro-vision) of appropriate space, it influences whatcan take place and how accessible those activi-ties are to different groups in the population.
Each outer sphere affects the health and well-being of people, represented by the inmostsphere (Whitehead and Dahlgren, 1991;Marmot and Wilkinson, 1999; McCarthy, 1999;Lawlor et al., 2003)the natural environment,for example, through the cleanliness of air andwater; the built environment through the avail-ability, convenience, safety and attractiveness ofpedestrian and cycling facilities, parks andplaying fields, and hence the propensity to takehealthy exercise; local economy throughinequalities in access to work and income; com-munity through supportive social networks (ortheir lack). The model can be used therefore tohelp understand the relationship between healthand planning.
Many of the urban development trends pro-
moted by the market and facilitated by planningauthorities are pandering to our unhealthyinstincts (Barton et al., 2000; National HeartForum, Living Streets and CABE, 2007).Despite more than a decade of official advocacyof sustainable development, many conventionsof the development industry remain trapped ina pre-Rio time warp. Across Europe, theexpanding peripheral city areas exhibit a patternof low-density, use-segregated, car-based devel-opment that not only uses land profligately butreduces the viability of local services, makes
walking impractical because of distance anddeters cycling. The fashionable office, retail andleisure parks that spring up in the wake of roadinvestment typically rely on 90 95% car use.The segregation of land uses is undermining thepotential for integrated neighbourhoods andlocal social capital. Unsustainability is literallybeing built into our cities.
In this context, health is a casualty. Thedecline in regular daily walking and cycling is
Fig. 1: Human ecology model of a settlement.Source: Barton and Grant (2006).
i92 H. Barton et al.
-
7/30/2019 Healthy Urban Planning in European Cities
3/9
resulting in increased obesity and risk of dia-betes and cardiovascular diseases (Franklinet al., 2003). Social polarization of opportunityis exacerbated. People tied to localityelderlypeople, children, young parents, unemployedpeople and immobile peopleare increasinglyvulnerable. The decline in local facilities, the
reduction in pedestrian movement and neigh-bourly street life all reduce opportunities forthe supportive social contacts so vital formental well-being (Halpern, 1995). Health pro-blems are being accumulated for the future,which will make the present problems of healthservice delivery look trivial by comparison.
Given that the quality of the urban environ-ment is important for human health, it is puz-zling that direct assessments of the linksbetween the built environment and physicalactivity as it influences health are still rare(Handy et al., 2002). The research literature isdivided between that focused on health out-comes (Halpern, 1995; Aicher, 1998) and thatfocused on planning interventions and behav-iour (Hedicar and Curtis, 1995; Cervero andKockelman, 1997; Williams et al ., 2000).Articles that make the connection explicit stillpromote the idea as innovative and newsworthy(Dube, 2000; Jackson et al., 2003; Barton et al.,2003a, b).
This lack of progress is in part because of thedifficulty in disentangling the influence of thebuilt environment from related social, economic
and personal variables in a rigorous way.Nevertheless, the evidence of the interconnec-tions is steadily building. In relation to physicalactivity, for example, we can now say with confi-dence that incidental foot and bike trips (to get tosomewhere for a specific purpose) are affected bya number of spatial variables: distance, density,form and layout; and recreational physical activityis influenced by the accessibility of parks andother facilities, the provision of pavements/bike-ways and the perceived aesthetic quality of theneighbourhood (Handy, 2005; National Heart
Forum, Living Streets and CABE, 2007). We canlink rising asthma levels generally to traffic-derived pollution (ozone), with some startlingspecific findings: in Atlanta when vehicle trafficwas kept artificially low during the Olympics in1996, traffic counts dropped by 22.5%, peak dailyozone levels by 27.9%, asthma emergencymedical events by 41.6%, whereas other emer-gency events were much the same as usual(Jackson and Kochtitzky, 2001).
Rather tardily, the research community isembarking on a more cross-cutting research inthis field. Its current relative paucity does notmean that health and planning have not beenlinked in practice. But normally this link isimplicit, not explicit, lacking a systematic orcomprehensive approach.
METHOD
There are three stages to the evaluation of pro-gress made towards a comprehensive approachto integrating health and planning in the WorldHealth Organization European Healthy CitiesNetwork (WHO-EHCN). The first is throughparticipant observation in the development ofthe HUP programme over a number of years.In addition, self-identified cities reported onprogress were interviewed individually and eval-uated through discussion as part of a mutuallearning exercise. Some of the results and con-clusions were set out in earlier publications(Barton et al., 2003a, b).
The second stage, in late 2005, involved theevaluation of 52 city applications for Phase IVof the Healthy Cities project. The raw materialof this evaluation was the written applicationssupplied to the Bristol Collaborating Centre bythe WHO Regional Office for Europe. Theyessentially show how far the cities had comeduring Phase III and by the start of Phase IV.
The applications were, on occasion, sup-plemented by telephone calls to applicants toclarify particular statements. Where feasible,the accuracy of the written material was com-pared with the personal or reported knowledgeof the applicant city and their programmes.With certain exceptions, there was consistencybetween the applications and reality. Wherethere was discrepancy, the actual performancewas invariably better than the applicationsuggested. Some applicant cities where Englishwas not their native tongue had problems in
conveying complex ideas with clarity. Overall, itis therefore likelygiven the number of citiesparticularly in eastern Europe where no exter-nal check was availablethat the results under-play the actual quality of the work going on.
The assessment of the applications involvedthree specific tests: the apparent level of under-standing of HUP; the degree of involvement ofplanning agencies; and the quality of the pro-gramme to strengthen HUP. The way these
Healthy urban planning in European cities i93
-
7/30/2019 Healthy Urban Planning in European Cities
4/9
were assessed by the researchers is explainedlater.
The third stage is the evaluation of progressmade by the end of Phase IV. This is thesubject of another paper presented at theInternational Healthy Cities Conference inZagreb in Autumn 2008 (Barton and Grant,
2010).
THE DEVELOPMENT OF THE WHO HUPINITIATIVE
The WHO HUP initiative was borne out of agrowing conviction that urban planning andrelated activities significantly influence thedeterminants of health (Duhl and Sanchez,1999). Healthy Cities projects throughoutEurope have sought, with limited success, toinvolve urban planners in their work since thelate 1980s. The baseline was established in 1998through a questionnaire survey. Respondentswere the heads of urban planning departmentsin 38 cities participating in Phase II (1993 1997) of the WHO-EHCN. The survey foundthat regular cooperation between planningdepartments and health agencies occurred inonly 25% of cases. Nearly one-third of planningheads considered that planning policies wereactually incompatible with health in certainwaysespecially rigid standards of zoning anddesign. Other anti-health issues highlighted
were excessive levels of motorized traffic, thefocus on private profit and public budgets,social segregation and the lack of attention tothe everyday needs of citizens (Barton andTsourou, 2000).
The foundations for the HUP initiative werelaid in the mid-1990s with the participation ofthe WHO-EHCN in the European SustainableCities and Towns Campaign. The links betweenhealth and sustainable development formed animportant element in the work of the Campaign(Price and Dube, 1997) and provided an oppor-
tunity to begin to explore the relationshipbetween health and urban planning.Meanwhile, urban planners across Europe werebecoming increasingly aware of the importanceof sustainable development, which emphasizesthe need to tackle social, environmental andeconomic issues in a coordinated way. Theirwork in this area led planners to reconsiderissues of the quality of life, well-being and, ulti-mately, health in cities.
In 1998, WHO began to work with urbanplanning practitioners and academics fromacross Europe in a more concerted way. A firststep was to publish Healthy Urban PlanningAWHO Guide to Planning for People (Bartonand Tsourou, 2000). It makes the case forhealth as a central goal of urban planning
policy and practice, highlighting the role ofplanners in tackling the environmental, socialand economic determinants of health. It dis-cusses the relevance of the Healthy Citiesmovement to urban planners, drawing attentionto the principles of equity, sustainability, inter-sectoral cooperation, community involvement,international action and solidarity. The booktranslates concepts and principles into practicalideas. It was produced in cooperation with anumber of cities and academics who met todiscuss the content at a seminar in Milan, Italyin October 1999 (WHO Regional Office forEurope, 1999). The group agreed 12 key healthobjectives for planners. The list provides a closeparallel with the 12 goals of sustainabledevelopment:
(i) promoting healthy lifestyles (especiallyregular exercise);
(ii) facilitating social cohesion and supportivesocial networks;
(iii) promoting access to good-quality housing;(iv) promoting access to employment
opportunities;
(v) promoting accessibility to good-qualityfacilities (educational, cultural, leisure,retail and health care);
(vi) encouraging local food production andoutlets for healthy food;
(vii) promoting safety and a sense of security;(viii) promoting equity and the development of
social capital;(ix) promoting an attractive environment with
acceptable noise levels and good airquality;
(x) ensuring good water quality and healthy
sanitation;(xi) promoting the conservation and quality ofland and mineral resources; and
(xii) reducing emissions that threaten climatestability.
Urban planning, in this light, is seen as a keymeans of promoting health and well-being.Equivalently, human health, well-being andquality of life are seen as central purposes ofurban planning.
i94 H. Barton et al.
-
7/30/2019 Healthy Urban Planning in European Cities
5/9
The meeting and the book provided themomentum for the formation of the WHO CityAction Group (CAG) on Healthy UrbanPlanning. The city of Milan agreed to lead andsupport the work of this group and hosted thefirst meeting at the Politecnico di MilanoTechnical University in June 2001 (WHO
Regional Office for Europe, 2001). Seniorurban planners and HC co-ordinators from 11cities across Europe attended the meeting,making a commitment to begin a process tointegrate health issues more fully into theirwork. The initial membership of the groupincluded cities from all parts of Europe:Gothenburg (Sweden), Horsens (Denmark),Sandnes (Norway), Belfast and Sheffield (UnitedKingdom), Milan (Italy), Seixal (Portugal),Vienna (Austria), Geneva (Switzerland), Zagreb(Croatia) and Pecs (Hungary).
From 2001, this group of cities, working withspecialist WHO advisors, was the focus forWHOs developing work on HUP (WHORegional Office for Europe, 2001; WHORegional Office for Europe, 2002; Barton et al.,2003a, b). Group meetings provided a forum forsharing knowledge and experience of exactlywhat HUP implies in practice and how it affectsday-to-day planning processes and outcomes.These planners developed understanding notjust of each others differences and unique per-spectives but of their common situation and ofhow many European cities can draw on the
experience of one city. The CAG provided thegroundwork for subsequent expansion of theHUP programme. In Phase IV (20032008) ofthe WHO-EHCN, HUP was one of the fourcore themes for cities to develop. The otherthree were health impact analysis, physicalactivity and healthy ageing. HUP is still a newdeparture for many municipalities. The nextsection evaluates how far the whole networkhad learnt through Phase III and rose to thechallenge of Phase IV.
PROGRESS MADE BY THE START OFPHASE IV
By the end of 2005, 52 cities had been assessedfor the membership of Phase IV. Each city wasjudged according to what improvements itplanned above and beyond what had alreadybeen achieved. In some cases, cities had littletradition of land use planning (as in Seixal,
reported earlier) and therefore started from alow level. In others, there was a well-developedplanning system but no established HealthyCities programme which might already havebuilt bridges between planning and healthagencies. In a few, especially in Scandinavia,there were both appropriate legal systems for
planning settlements and established planning/health links. It was possible for cities in any ofthese groups to perform well according toassessment criteria referred to in the Methodssection.
UNDERSTANDING
The level of understanding of HUP wasassessed by three tests, each of which relied ondifferent parts of the application and thushelped to check on the significance andreliability of any particular facet:
the range of relevant planning policy areasthat were identified for action (using the listgiven earlier in this paper);
the nature of the activities promised underthe HUP heading: were they expressly aboutpromoting change in the built environment,with health as an explicit driver for thatchange?;
the degree of explicit linkage between HUPand the other main themes: for example, was
HUP seen as part of the healthy ageingagenda?
All the cities were, of course, completely awarethat their plans for the development of HUPwere to be scrutinized. However, they did notknow exactly how this would happen, so theopportunity for game-playing was reduced. Thecharacter of the answers generally suggests thatapplicant cities made a direct and honestresponse to the cues in the application form.
In relation to the first criteria, the applicantswere not formally asked to reflect the full range
of health objectives in their application, butspecific aims and programmes might beexpected to cover a number of relevant areas.The range encompassed helps to show theunderstanding of the multi-faceted nature of thehealth-planning relationship. Forty per cent ofapplicant cities mentioned at least half of the 12WHO-ECHN objectives referred to earlier.However, 30% mentioned no more than 2 outof the 12. Housing quality and accessibility to
Healthy urban planning in European cities i95
-
7/30/2019 Healthy Urban Planning in European Cities
6/9
services were the objectives most commonlyidentified. Objectives of employment, food andclimate change were all conspicuous by theirabsence from the vast majority of applications(Figure 2).
General understanding of HUP was judgedby the degree to which applicants conveyed rec-ognition of the integrated nature of land use/transport systems and the impact on health.
Most of the cities giving a good coverage ofobjectives also demonstrated a good overallunderstanding. Conversely, those identifyingfew objectives demonstrated poor understand-ing; the most common limitation was that theyhad not made the jump from a view of publichealth as purely about the co-ordination of ser-vices and campaigns, to one which was about
the creation of a healthy urban environment.Twenty-five per cent of the cities showed weakor very weak understanding. The strongest citiesnot only demonstrated a coherent and well-developed understanding, but also linkedtogether the three Phase IV themes: i.e. HIAwas seen as a tool which could expressly beused to promote HUP, whereas HUP was seenas a process which could assist healthy ageing.Thirty per cent of cities showed a good or excel-lent level of understanding.
INVOLVEMENT
Healthy Cities units in most municipalities areoff-shoots of health departments and staffed bymedical or public health practitioners. Planningagencies have not traditionally been involved.Phase IV acted as an incentive to broaden themanagement of the Healthy Cities programme.Without proper representation of planning
agencies at a senior decision-making level in theprogramme, it is very difficult to achieve
health-integrated plans.A significant proportion of Healthy Citiessteering groups had no obvious representationof planning agencies (Figure 3). This includesall the weakest group of cities, as identified inthe assessment of understanding. However, afew of the strongest cities also lacked represen-tation. It may be that in some cities, effectivepower resides with the officers at the coal-face(and at that level, there is effectiveco-operation) rather than with the steeringgroup or management group (who may follownot lead).
THE PROGRAMME
The programme for promoting HUP is the cruxof the assessment. However, the evaluationprocess is not simple. The good applications,with relevant and coherent programmes andclear mechanisms for further building mutualunderstanding between health and planningprofessionals, are straightforward to assess. The
poor applications, with no coherent approach,are also straightforward. But between lie manyapplications, over half of the total, whichdisplay some appropriate ideas without beingsufficiently clearly argued or illustrated to judgetheir real merit. A majority of cities do havespecific projects with a strong HUP dimen-sionin relation in particular to the topics ofhousing, accessibility, open space, regenerationand/or walking and cycling.
Fig. 2: HUP objectives identified in theapplications.
Fig. 3: Analysis of the involvement of planningagencies and officers.
i96 H. Barton et al.
-
7/30/2019 Healthy Urban Planning in European Cities
7/9
Although some of these projects are positiveand innovative, others are not sufficiently tunedto a broad view of health. They appear splicedinto the programme: perhaps from otheragencies, without integrating the health angle.For example, some open-space projects arefocused on issues of wildlife habitat preser-
vation (valuable as that is) and do not addresshuman recreational needs (with the accompany-ing health benefits) in any systematic way.
About a third of cities have gone the extrastep and are integrating health objectives intotheir spatial strategies. Some cities have explicitbottom-up programmes of community plan-ning or public involvement in policy-making,enhancing social capital/empowerment. A verypositive feature is that many cities have coher-ent programmes for the training and awareness-raising of staff, sometimes across organizationaldivides.
OVERALL ASSESSMENT
The 52 Phase-IV applications can be dividedinto five groups (Figure 4).
Seventeen applications are very strong. Theseare from cities with a good understanding ofHUP who also put forward an innovative,impressive or comprehensive programme.Sixteen applications are of good quality but arefrom cities with a less complete apparent
understanding of HUP. However, they showother strengths, such as a very good understand-ing in specific areas or they demonstrate theknowledge of their weaknesses, and their pro-posed activities address these. Others may lackcurrent understanding but have demonstrated agood start in joining the WHO-EHCN and are
pointing in the right direction.Nineteen applications range from poor tovery weak. These cities have been unable todemonstrate a real understanding of HUP inthe application. Representation of planners inthe core group is usually lacking, and the propo-sal may be vague or inadequate. The cities inthis group usually do not display awareness ofthese weaknesses and consequently provide noremedy.
The development of the cities in the HUPCAG in Phase III provides insights into the waycities can progress from a weak one to a strongone. Three lessons stand out. The first isthe critical importance of cross-sectoralco-operation. Collaboration between health andplanning agencies is the starting point, butneeds also to embrace transport, housing, regen-eration, economic development and recreation.In Gothenburg, for example, a health group wasestablished within the City Planning Authorityto consider the health implications of planningproposals, drawing on expertise from otherdepartments. In Milan, a pilot process wasundertaken to introduce an intersectoral
approach to developing three regeneration pro-jects in the city, linking social and environ-mental interventions systematically.
The second lesson is the importance of pro-ducing a health-integrated spatial plan whichinvolves the wider community in the issues. InSandnes, health was fully integrated into thenew municipal comprehensive plan (the mainmanagement document for all municipal activi-ties). Health represented one of the three keythemes of the plan, and is being implementedthrough a range of practical initiatives, with a
focus on citizen participation. In Horsens,health was a central objective of all municipalactivities and was integrated into urban plan-ning processes. Neighbourhood regenerationand community empowerment activities haveprovided an important vehicle for implementingthe health-oriented goals of the general munici-pal plan.
The third lesson is about the potential forradical change. In Belfast, where planning andFig. 4: Categorizing the city applications.
Healthy urban planning in European cities i97
-
7/30/2019 Healthy Urban Planning in European Cities
8/9
health have been institutionally divorced, theNorthern Ireland Office of the United KingdomGovernment Department of the Environmentand Belfast Healthy Cities made a jointapproach to promote and integrate health into awide range of local and regional plans and pol-icies. Tools such as strategic environmental
assessment and a quality of life matrix weredeveloped to assist this process. In Seixal,Portugal, there was little experience of townplanning. Health provided a new motivation topromote it, and an interdepartmental workinggroup was established to guide the integrationof health into the emerging development planand to implement this concept on a practicallevel.
CONCLUSION
The WHO-EHCH HUP initiative provides aclassic example of the development of a newprinciple, triggered by top-down encouragementand spread by networks of mutual support. Forthose municipalities that have only recentlyembarked on the journey, health is proving apowerful motivator for addressing planningissues that have not previously been faced,drawing in new constituencies of politicalsupport. For example, in Seixal, the healthagenda has encouraged planning policies toprotect allotments from development and to
tackle problems of social exclusion (and relatedhealth inequalities) on isolated estates.Nevertheless, in many cities, there are difficultiesbecause vertical departmental remits deter colla-borative workingas one planner commented:There are a lot of islands in this municipality.Some municipalitiesespecially in northernEuropehave had health embedded in planningpolicy-making for some years. In these situ-ations, interagency cooperation is the rule andnot the exception, and the main planning docu-ments reflect health priorities not only in their
context but in decision-making processes thatplace a premium on building social capital.
Both the more experienced and the lessexperienced cities agree that health-integratedplanning is valuable. Healthy opportunities arecreated. Planning policies become better, moreresponsive to community needs and morestrongly supported.
An ideal health-integrated planning systemhas five key elements. The first is acceptance of
interdepartmental and interagency collabor-ation so that health implications can be properlyexplored and integrated solutions pursuedacross institutional remits. The second is strongpolitical backing, which helps to ensure a con-sistent approach and the resources needed. Thethird is full integration of health with environ-
mental, social and economic concerns in themain statements on land-use planning, trans-port, housing and economic developmentpolicy: placing health at the heart of plan-making. The fourth is the active involvement ofcitizens and stakeholders in the private, publicand voluntary sectors in the policy process. Thefifth is a toolbox of planning techniques thatfully reflects health objectives and makes themexplicit: quality-of-life monitoring, healthimpact assessment, strategic sustainabilityassessment, urban potential studies.
The WHO-EHCN experiment in HUP is notalone. Other cities around Europe are progres-sing in the same direction. Health argumentsare increasingly being made explicit in planningpolicy debate (Breeze and Lock, 2001; Jones,2002). Practitioners are grappling with the diffi-culties of assessing health effects (Morgan andMahoney, 2001). But the WHO-EHCN doesdemonstrate both the power of the idea in chan-ging minds and opening new avenues and thenecessity of a sustained, progressively more sys-tematic approach. Health is a powerful motiva-tor, capable of cutting across vested interests in
a way that sustainable development may not beable to.
FUNDING
This article is based on an evaluation commis-sioned by the WHO Regional Office forEurope.
REFERENCES
Aicher, J. (1998) Designing Healthy Cities: Prescriptions,Principles and Practice. Krieger Publishing Company,Malabar, FL.
Barton, H. (2005) A health map for urban planners:towards a conceptual model for healthy sustainablesettlements. Built Environment, 31, 339355.
Barton, H. and Grant, M. (2006) A health map for thelocal human habitat. Journal of the Royal Society for thePromotion of Health, 126, http://www.euro.who.int/healthy-cities/Documentation/20020514_1 (last accessed17 September 2003).
i98 H. Barton et al.
-
7/30/2019 Healthy Urban Planning in European Cities
9/9
Barton, H. and Grant, M. (2010) Healthy Cities Phase 4Review. Journal of Urban Health, in press.
Barton, H. and Tsourou, C. (2000) Healthy UrbanPlanningA WHO Guide to Planning for People.E&FN Spon, London.
Barton, H. (ed.) (2000) Sustainable Communities: ThePotential for Eco-Neighbourhoods. Earthscan, London.
Barton, H., Mitcham, C. and Tsourou, C. (eds) (2003a)Healthy Urban Planning in Practice: Experience of
European Cities. Report of the WHO City ActionGroup on Healthy Urban Planning. WHO RegionalOffice for Europe, Copenhagen.
Barton, H., Handy, S., Boarnet, M., Ewing, R.,Killingsworth, R., Jackson, R. et al. (2003b) Healthycities. Urban Design Quality, 87, 15 36.
Breeze, C. and Lock, K. (eds) (2001) Health ImpactAssessment in Strategic Environmental Assessment: AReview of Health Impact Assessment Concepts, Methodsand a Practice to Support the Development of aProtocol on Strategic Environmental Assessment to theEspoo Convention, Which Adequately Covers Health
Impacts, November 2001. WHO Regional Officefor Europe, Copenhagen, http://www.euro.who.int/docu-ment/e74634.pdf (last accessed 17 September 2003).
Cervero, R. and Kockelman, K. (1997) Travel demand andthe 3Ds: density, diversity and design. TransportationResearch Part D, 3, 199 219.
Dube, P. (2000) Urban health: an urban planning perspec-tive. Reviews on Environmental Health, 15, 249265.
Duhl, L. J. and Sanchez, A. K. (1999) Healthy cities andthe city planning processa background document onlinks between health and urban planning., WHORegional Office for Europe Expert Group on the UrbanEnvironment, Copenhagen.1996 European SustainableCities. European Commission, Brussels.
Franklin, T. et al. (2003) Walkable streets. New UrbanFutures, 19, 57.
Halpern, D. (1995) Mental Health and the BuiltEnvironment. Taylor and Francis, London.
Handy, S. (2005) Rebuilding the Environment to PromotePhysical Activity. Presentation at the WHO HealthyCities and National Networks Business Meeting inBursa, September 2005, Turkey.
Handy, S., Boarnet, M., Ewing, R. and Killingsworth, R.(2002) How the built environment affects physicalactivity: views from urban planning. American Journalof Preventive Medicine, 23, 64 73.
Hedicar, P. and Curtis, C. (1995) Residential Developmentand Car-based Travel: Does Location Make aDifference? Oxford School of Planning, Oxford BrookesUniversity, Oxford.
Jackson, R. and Kochtitzky, C. (2001) Creating a HealthyEnvironment: The Impact of the Environment on PublicHealth. Centre for Disease Control and Prevention,National Centre for Environmental Health, USA.
Jackson, R. (2003) The impact of the built environment onhealth: an emerging field. American Journal of PublicHealth, 93, 13821384.
Jones, G. (2002) Planning for health could reap rewards.Planning, 1491, 1617.
Lalonde, M. (1974) A New Perspective on the Health ofCanadians. Healthy and Welfare Canada, Ottawa.
Lawlor, D. et al. (2003) The challenges of evaluatingenvironmental interventions to increase populationlevels of physical activity: the case of the UK NationalCycle Network. Journal of Epidemiology andCommunity Health, 57, 96101.
Marmot, M. and Wilkinson, R. (eds) (1999) SocialDeterminants of Health. Oxford University Press, Oxford.
McCarthy, M. (1999) Transport and health. In Marmot, M.and Wilkinson, R. (eds), Social Determinants of Health.Oxford University Press, Oxford.
Morgan, R. and Mahoney, M. (2001) Health impact assess-ment in Australia and New Zealand: an exploration ofmethodological consensus. Promotion and Education, 8,
811.National Heart Forum, Living Streets and CABE (2007)
Building Health: Creating and Enhancing Places forHealthy Active Lives. National Heart Forum, London.
Price, C. and Dube, C. (1997) Sustainable Development andHealth: Concepts, Principles and Framework for Action
for European Cities and Towns. WHO Regional Officefor Europe, Copenhagen, http://www.who.dk/document/e53218.pdf (last accessed 8 September 2003).
Whitehead, M. and Dahlgren, G. (1991) What can we doabout inequalities in health? Lancet, 338, 10591063.
WHO Regional Office for Europe (1999) Healthy UrbanPlanning: Report of a WHO Seminar. WHO RegionalOffice for Europe, Copenhagen, http://www.who.dk/eprise/main/who/progs/hcp/UrbanHealthTopics/20020604_1 (last
accessed 8 September 2003).WHO Regional Office for Europe (2001) First Meeting of
the City Action Group. Report on a WHO Meeting,Milan, Italy, 2425 June 2001, WHO Regional Office forEurope, Copenhagen.
WHO Regional Office for Europe (2002) Second Meetingof the WHO City Action Group on HealthyUrban Planning. Report on a WHO Meeting, 23 24May 2002, Milan, Italy, WHO Regional Office forEurope, Copenhagen.
Williams, K. et al. (2000) Achieving Sustainable UrbanForm. E&F Spon, London.
Healthy urban planning in European cities i99