
Healthcare Vertical Integration and Internal Audit’s Role in Strategic Transactions September...
25
Healthcare Vertical Integration and Internal Audit’s Role in Strategic Transactions September 2014
Transcript of Healthcare Vertical Integration and Internal Audit’s Role in Strategic Transactions September...

Healthcare Vertical Integration and Internal Audit’s Role in Strategic Transactions
September 2014

Page 2
Agenda
I. Healthcare vertical integration
II. Internal Audit’s role in strategic transactions

Page 3
Health industry integration is not black or whiteShades of collaboration exist, although the trend is strongly to the right
Source: www.accountablecarefacts.org
Single MDs; small
groups; single
hospitals
Independent physician
associations, single specialty
groups, hospital chains
Hospital staffs (primary care
physicians employed by
hospitals), some university/faculty
practices
Multispecialty group practices (primary care-
based practices with full
complement of specialty services)
Clinically integrated
delivery systems (multispecialty
groups with hospitals)
Clinically and financially integrated systems
(multispecialty medical groups integrated with hospitals and health plans)
Less integrated or organized systems More integrated or organized systems
Horizontal Vertical
Most ACOs are formed in this space

Page 4
Vertical integration has three primary objectivesPayers and health systems are increasingly willing to accept non-traditional risks to preserve their positions in the healthcare supply chain
Objective Acquirer Target Benefit Risk
1. Strengthen revenue streams
Health System
Physicians Increase referrals and admissions
Provider productivity decline post acquisition, inability to influence physician decisions
Health System
Payer Increase patient volume and reimbursement rates through a restricted network and reduction in payer margin
Financial losses due to under-estimation of member utilization and unit cost
Payer Health System Capture enrollment through health system regional presence and brand
Acquire disproportionately high-cost members due to health system loyalty
2. Improve control of supply costs
Payer Health System,Physicians
Improve ability to manage population health and control medical expense
Capital-intensive investment erodes financial viability and flexibility without improving health cost management
3. Defend against disintermediation or exclusion
Payer Health System Guard against integrated delivery systems contracting directly with employers or government payers as ACOs
Lose network breadth due to reluctance of providers to participate in network of a direct competitor
Health System
Payer Offset potential exclusion from narrow networks
Lose overall managed care volume due to commercial payers unwilling to contract with a direct competitor
Health System
Physicians Avoid disproportionate admissions to competing health systems
Physician unwillingness to modify referral or admission practices

Page 5
Integration activity has come in wavesBeginning in the 1980s, a surge in managed care growth fueled health industry integration, both horizontal and vertical
ElementTrends
1980 – 2000sObservations
Payers- Managed care organizations grew membership and
implemented cost control techniques- Payers consolidated
- Large managed care organizations used their leverage to negotiate lower cost provider contracts
Health Systems- Hospital networks, such as HCA, began to expand by
acquiring other hospitals- Hospitals began to form managed care networks- Health systems formed health plans
- Larger health systems struggled to create economies of scale or reduce cost
- Provider-sponsored health plans initially generated large cash flow; however, months/years later struggled with growth and survival
Physicians
- Physicians tended to operate independently from each other
- Hospitals experimented with employing physicians - Physician groups experimented with starting health
plans
- Care coordination hampered by a lack of communication channels and incentives
- Hospital-physician organizations and physician group-owned HMOs disintegrated over time due to poor management and diverging interests
Reform- No economic or political forces driving for lowering
the cost of care- Expected Clinton-era reforms failed to become a reality
- Providers were not externally incentivized to coordinate care. Revenue could still be driven through volume.
Reimbursement- Fee for service (FFS) reimbursement was the industry
standard
- FFS created an environment where providers and payers existed with inherent, opposing interests
- Providers were not incentivized to reduce the cost of care

Page 6
Vertical integration failure is commonWhile the benefits of integration are appealing, realization has been a challenge for most organizations
1945: Permanente Health Plan (later named Kaiser) opens to the public, providing both health coverage and access to hospitals
20101965
Rise of managed care organizations and new reimbursement methodologies (e.g., DRGs, per diems, case rates, carve outs)
1992: Humana spins off 77 hospitals as Galen Health
Care to focus exclusively on insurance
1972: Humana shifts focus from nursing homes to hospitals, eventually acquiring
77 facilities
Traditional fee for service dominated the market
1947: Group Health Cooperative opens in Seattle Washington as a PSHP
1980: Geisenger Medical Center starts the Geisenger Health
System (a PSHP)
1969: Harvard Community Health Plan opens as a PSHP
2013: Kaiser sells Ohio health plan to
Catholic Health Partners (Health
Innovations Ohio)
2014: North Shore LIJ opens CareConnect
2014: Piedmont Healthcare and Wellstar
Health System start Piedmont Wellstar Plan
2000: Rush University Medical Center sells
Anchor HMO to WellPoint
1971: Rush Univ. Medical Center opens Anchor HMO
1980 1995
1998: UPMC launches UPMC Health Plan
1984: Sentara opens Optima HMO Health
Plan
Passage of the Affordable Care Act
1983: Intermountain Healthcare creates SelectHealth, a non-profit health plan
2002: Piedmont separates from Promina Health, exiting the health plan market
1994: Promina Health founded by Piedmont
Healthcare
2012: Sutter Health
launches Sutter Health Plus
2001: UniHealth divests its
medical and insurance practices
1993: Sutter Health opens
Omni Healthcare Plan
1999: Sutter Health sells Omni Healthcare
to BCBSCA
1986: HealthWest (later UniHealth)
launches CareAmerica
2011: Highmark acquires West Penn Allegheny
Health System
2011: Humana acquires 300 clinic Concentra
Health
2011: UnitedHealth Group acquires 2,300
physician Monarch Healthcare
1990: Cigna acquires majority ownership of Lovelace Health Systems
2002: Cigna sells Lovelace to Ardent Health Services
1998: AHERF files
for bankruptcy
1986: Allegheny Health, Education, and
Research Foundation (AHERF) begins
integration efforts, purchasing physician
organizations and hospitals

Page 7
Strategic, Financial
and Operational
Risk
Vertical integration is fraught with riskEndeavors have failed for myriad reasons, but at the core is typically an under-estimation of the risks to be managed
Limiting financial wherewithal by taking on too much at once
Inadequate physician alignment,
particularly within primary care
Paying for productivity gains that do not align with the acquired entity’s new incentives
Inability to effectively
coordinate care across the
integrated delivery system
Insufficient capability to execute core new functions (e.g., pricing, reserving, practice management)
Not clearly defining each entity’s role within the system
Developing organizational
capabilities too far in advance of
market demand
Optimistic assumptions regarding willingness of business partners to make concessions

Page 8
ElementTrends
2010-2014Observations
Payers
- Slower membership growth due to escalating premiums- Reduced ability to limit risk through underwriting; forced
to manage risk once “in house” - New regulations and taxes negatively impact profitability - Selective vertical integration through medical group or
facility acquisition, or partnerships with health systems
- Pressured to effectively manage medical expense- Working towards ACO-like payment methodologies
(rewarding quality and care coordination)- Increasing member engagement
Health Systems
- Renewed focused on acquisition/merger activity to increase scale
- Rapid EHR adoption driven by financial and care coordination incentives
- Payments increasingly tied to quality metrics- Increasing acceptance of risk through ACOs
- Positioning for inclusion in narrow payer networks and alternative contract arrangements
- Focused on clinical/operational excellence - Patient demand for price transparency - Technological advancement opening new
communication channels for providers and patients
Physicians
- Rapid movement towards health system employment- Physician group consolidation- Primary care shortage - Broader acceptance of evidence-based medicine,
standards of practice and clinical pathways
- Improved ability to coordinate care and control costs
- Gradual movement towards transparency of outcomes
Reform
- ACO and patient centered medical home development- Health Insurance Exchanges provide new forum for
individual and small group market competition- Increasing public acceptance of cost control techniques
(e.g., narrow networks, Medicare Shared Savings Services Program)
- Health Insurance Exchanges increasing patient volume will likely challenge primary care capacity
- Quality programs are necessary core capabilities - Transparency in quality measurements is increasing
consumer driven health care
Reimbursement- Value-based reimbursement models- Shared reward systems (e.g., MSSP)- Compliance contingent reimbursement (Meaningful Use,
Medicare STARS Program)
- Increased provider risk acceptance - Payer and provider incentive alignment- Risk-based payer revenue
The next wave is upon usRegulatory and market changes are prompting both defensive and opportunistic integration moves

Page 9
Integration is being initiated from all directionsHealth systems and payers are both testing new positions along the supply chain
► Provider sponsored health plans– Sutter Health Plus (Sutter Health)– CareConnect (North Shore Long Island Jewish)– Piedmont Wellstar Health Plans (Piedmont and Wellstar Health Systems)
► Health plan hospital/provider acquisitions– West Penn Allegheny (Highmark)– Concentra clinics (Humana)– Diagnostic Clinic Medical Group (Florida Blue)
► Accountable Care Organizations (ACOs)– More than 500 Medicare and Commercial ACOs have formed since 2010– Most are hospital or health system led– More than 10 million members are enrolled in commercial ACOs– Major, national health insurers have announced intentions to significantly
increase their volume of ACO contracts

Page 10
Where to begin?Avoiding the mistakes of the past begins with an assessment of the factors that drive success and failure
Gate 1
Objectives and risk identification
► Clarify strategic intent and desired competitive position within market context
► Identify licensure requirements
► Perform high-level capability analysis– Patient services
and network coverage
– Financial risk management
– Payer or provider operations
► Identify risks and potential mitigation actions
Gate 2
Capability assessment
► Identify the core capabilities required to effectively manage population health to create a positive return on investment
► Determine the level of capability maturity needed to successfully compete in the targeted market
► Identify the capability gaps to be addressed before launching new product or services
Gate 3
Build versus buy analysis
► Evaluate the feasibility and level of effort required to develop required capabilities in house
► Assess the opportunity and associated risks of partnership arrangements
► Determine the costs and advantages of acquiring existing capability providers
► Conduct initial due diligence on acquisition targets
► Develop a recommended approach to obtaining each capability
Gate 4
Business case development
► Determine availability and cost of capital
► Determine start up costs, to include capability investments, capital requirements, talent acquisition and marketing
► Forecast cash inflows driven by patient and premium revenue and investment income
► Estimate cash outflows based on the timing and magnitude of claims payments, operating expenses, interest payments and taxes
► Determine NPV and/or ROI of the health plan investment

Page 11
Agenda
I. Healthcare vertical integration
II. Internal Audit’s role in strategic transactions

Page 12
Background
Strategic transactions like mergers and acquisitions (M&A) and divestitures remain some of the most risk-heavy initiatives that any organization can undertake.
The proactive involvement of Internal Audit (IA) before, during and after the merger, acquisition or divestiture can help management identify issues and opportunities related to the transaction that might not otherwise be addressed.
Acting as an advisor to the program management team, IA is ideally positioned to assess and monitor program management activities, review controls and provide key insights while maintaining independence and objectivity.

Page 13
How IA can help during strategic transactions
► Provide increased visibility into key risks related to strategic transaction changes (e.g., Finance, IT, HR, Operational risks)
► Reinforce that risks and controls are the responsibility of management
► Identify gaps in the integration or separation project management plan
► Suggest opportunities for synergies that would boost the acquisition’s return on investment (ROI) or actions to increase separation-related cost savings
► Highlight the impact that the acquisition and its integration, or the divestiture, may have on other parts of the business
► Identify potential gaps in the internal control structure
► Support management’s prioritization of transition and organizational readiness risks

Page 14
Role of IA during M&A
► There are four key areas where IA can play a crucial role in an organization’s M&A lifecycle:
Throughout the M&A process, IA should form a part of the program
management team so that it can assess and monitor activities and
provide key insights. IA can also audit program management activities
to highlight process gaps and areas of future improvements.

Page 15
Role of IA during M&A: Strategy

Page 16
Role of IA during M&A: Due diligence

Page 17
Role of IA during M&A: Deal approval and close

Page 18
Role of IA during M&A: Integration

Page 19
The role of IA during divestitures
► There are four key areas where IA can play a role in the divestiture lifecycle:
Leading practice calls for IA to be embedded as part of the program
management team and be involved throughout the divestiture life cycle.
Page 20
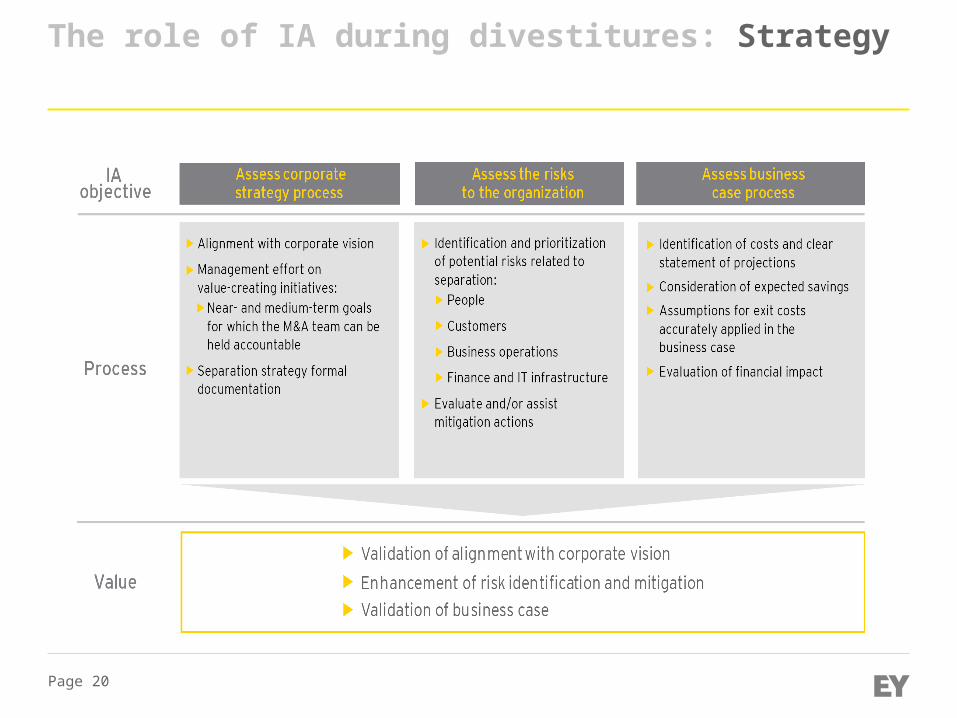
The role of IA during divestitures: Strategy

Page 21
The role of IA during divestitures: Due diligence

Page 22
The role of IA during divestitures: Deal approval and close

Page 23
The role of IA during divestitures: Separation

Page 24
Key benefits
IA provides a critical perspective to strategic transaction deals that many executives may not consider. Without that perspective — right from the start — the organization could find out far too late that the price was not right, or that it has to spend a significant amount of money to fix issues that IA could have identified and helped the organization avoid
► Strategically, IA can determine an organization’s readiness for the transaction
► During due diligence, IA can alert the organization to potential risk, control or regulatory issues that would cause the organization to overpay or undervalue
► Prior to deal close, IA can help prevent deal value leakage
► Post-transaction, IA’s involvement can lead to organizational efficiencies and strengthened control monitoring

Page 25
For further information
► See the full “Internal Audit’s role during the strategic transactions life cycle” report
► For further GRC thought leadership, please refer to our Insights on governance, risk and compliance series on:www.ey.com/GRCinsights
► Please contact:► Sean Lueck, EY Healthcare Advisory (904-505-6572)► Wally Ward, EY Healthcare Advisory (704-331-1907)


















