Healthcare Epidemiology, the Hospital Epidemiologist: Rationale and Responsibilities
54
Healthcare Epidemiology, the Healthcare Epidemiology, the Hospital Epidemiologist: Hospital Epidemiologist: Rationale and Responsibilities Rationale and Responsibilities Disclosure: Grant: Sage, Advisory Board: Disclosure: Grant: Sage, Advisory Board: Theradoc, GSK, BioMerieux, Data Monitoring Theradoc, GSK, BioMerieux, Data Monitoring Board: Cadence Pharmaceuticals, Honoraria: Board: Cadence Pharmaceuticals, Honoraria: 3M, Pfizer, BioMerieux 3M, Pfizer, BioMerieux Trish M. Perl, MD, MSc Trish M. Perl, MD, MSc Hospital Epidemiologist, Johns Hopkins Hospital Hospital Epidemiologist, Johns Hopkins Hospital Professor of Medicine, Johns Hopkins University Professor of Medicine, Johns Hopkins University 13 13 th th Annual Fellows Course Annual Fellows Course July 7, 2009 July 7, 2009
description
Healthcare Epidemiology, the Hospital Epidemiologist: Rationale and Responsibilities. Trish M. Perl, MD, MSc Hospital Epidemiologist, Johns Hopkins Hospital Professor of Medicine, Johns Hopkins University 13 th Annual Fellows Course July 7, 2009. - PowerPoint PPT Presentation
Transcript of Healthcare Epidemiology, the Hospital Epidemiologist: Rationale and Responsibilities

Healthcare Epidemiology, the Hospital Healthcare Epidemiology, the Hospital Epidemiologist: Rationale and Epidemiologist: Rationale and
ResponsibilitiesResponsibilities
Disclosure: Grant: Sage, Advisory Board: Theradoc, GSK, Disclosure: Grant: Sage, Advisory Board: Theradoc, GSK, BioMerieux, Data Monitoring Board: Cadence Pharmaceuticals, BioMerieux, Data Monitoring Board: Cadence Pharmaceuticals,
Honoraria: 3M, Pfizer, BioMerieuxHonoraria: 3M, Pfizer, BioMerieux
Trish M. Perl, MD, MScTrish M. Perl, MD, MScHospital Epidemiologist, Johns Hopkins HospitalHospital Epidemiologist, Johns Hopkins HospitalProfessor of Medicine, Johns Hopkins UniversityProfessor of Medicine, Johns Hopkins University
13 13thth Annual Fellows Course Annual Fellows CourseJuly 7, 2009July 7, 2009

A patient with meningococcal meningitis was A patient with meningococcal meningitis was admitted last night. Nobody wore masks? admitted last night. Nobody wore masks? Who was exposed and needs prophylaxis?Who was exposed and needs prophylaxis?
You see 5 MRSA surgical site infections on GI You see 5 MRSA surgical site infections on GI surgery when you go on service. The surgery when you go on service. The infections occurred over 3 weeks? What do infections occurred over 3 weeks? What do you do? Is this an outbreak?you do? Is this an outbreak?
The influenza vaccination rate among HCWs The influenza vaccination rate among HCWs is only 40% what do you do?is only 40% what do you do?
QuestionsQuestions

To review the roles and responsibilities of a To review the roles and responsibilities of a hospital or healthcare epidemiologistshospital or healthcare epidemiologists
To review the primary tools used by To review the primary tools used by healthcare epidemiologists and infection healthcare epidemiologists and infection control practitioners to prevent and control control practitioners to prevent and control HAIHAI
To review some of the barriers and To review some of the barriers and challenges with programs or healthcare challenges with programs or healthcare epidemiology interventionsepidemiology interventions
ObjectivesObjectives

Healthcare associated infections (HAIs)Healthcare associated infections (HAIs)
Infections that develop as a result of Infections that develop as a result of medical or surgical care and are not medical or surgical care and are not incubating on admission to the health care incubating on admission to the health care systemsystem
Encompasses resistant and Encompasses resistant and epidemiologically significant organisms epidemiologically significant organisms that are acquired, develop or transmitted that are acquired, develop or transmitted in the healthcare settingin the healthcare setting

What Do We Do?What Do We Do?

A person (usually MD trained in Infectious A person (usually MD trained in Infectious Diseases and Epidemiology) who supervises a Diseases and Epidemiology) who supervises a Hospital Epidemiology and Infection Control Hospital Epidemiology and Infection Control Program. They are responsible for preventing Program. They are responsible for preventing and controlling adverse events among patients and controlling adverse events among patients and healthcare workers (patient safety). and healthcare workers (patient safety).
Their focus of prevention and Their focus of prevention and control goes beyond the health control goes beyond the health of the individual patient or of the individual patient or healthcare worker and oftenhealthcare worker and oftenconsider the population.consider the population.
What is a Hospital (Health Care What is a Hospital (Health Care Epidemiologist?Epidemiologist?

The study of events (infectious or non-The study of events (infectious or non-infectious) that occur in hospitalized patients infectious) that occur in hospitalized patients as a result of being hospitalized, having as a result of being hospitalized, having surgery or other surgical procedure, or of surgery or other surgical procedure, or of receiving a treatmentreceiving a treatment– Nosocomial or healthcare associated infectionsNosocomial or healthcare associated infections– Resistant or epidemiologically important organismsResistant or epidemiologically important organisms– Unexpected exposure to communicable diseases in health Unexpected exposure to communicable diseases in health
care settingscare settings– OutbreaksOutbreaks
What is Hospital or Healthcare What is Hospital or Healthcare Epidemiology?Epidemiology?

WeWe• evaluate rates and use population based methodsevaluate rates and use population based methods• use traditional epidemiologic methods and use traditional epidemiologic methods and
molecular epidemiologic methods to evaluate risk molecular epidemiologic methods to evaluate risk factors and determine causalityfactors and determine causality
• focus on infection but recently have expanded to focus on infection but recently have expanded to study non-infectious outcomes of carestudy non-infectious outcomes of care
• measure complications and process of care measure complications and process of care measuresmeasures
• implement and collaborate with interventionsimplement and collaborate with interventions
What Specifically Do We Do in Hospital What Specifically Do We Do in Hospital or Healthcare Epidemiology?or Healthcare Epidemiology?

• Intervene to prevent transmission of resistant Intervene to prevent transmission of resistant organisms & infections (includes surveillance)organisms & infections (includes surveillance)
• Implement guidelines and research findingsImplement guidelines and research findings• Develop policies and procedures e g., to decrease Develop policies and procedures e g., to decrease
selection and transmission of resistant organismsselection and transmission of resistant organisms• Educate healthcare workers Educate healthcare workers • Conduct research or evaluate best practice--risk Conduct research or evaluate best practice--risk
factors, outcomes, interventionsfactors, outcomes, interventions• Help manage mass infectious diseases casualty Help manage mass infectious diseases casualty
situationssituations
Primary Functions of Healthcare or Primary Functions of Healthcare or Hospital EpidemiologyHospital Epidemiology

Competing interestsCompeting interests
EpidemiologicalEpidemiologicalpopulation-orientedpopulation-orientednon-maleficencenon-maleficenceconfidentialityconfidentialityinvestigate/reportinvestigate/reportjusticejustice
MedicalMedicalperson-orientedperson-orientednon-maleficencenon-maleficenceconfidentiality confidentiality privacyprivacyautonomyautonomy
Herwaldt and Kaldjian, Ethical Aspects of Infection ControlHerwaldt and Kaldjian, Ethical Aspects of Infection ControlThe Practical Guide to Hospital EpidemiologyThe Practical Guide to Hospital Epidemiology


What Is the Problem and its What Is the Problem and its Impact?Impact?

A Sobering Letter from a Family A Sobering Letter from a Family MemberMember
““Today would have been my beloved Today would have been my beloved wife’s birthday. She died in your wife’s birthday. She died in your hospitalhospital.”….”……“…“I witnessed many gross violations of I witnessed many gross violations of the standard "Universal Precautions“ the standard "Universal Precautions“ posted everywhere within the hospital. posted everywhere within the hospital. They were not limited to one building, They were not limited to one building, one floor, or one individual. They were one floor, or one individual. They were widespread.”…widespread.”…

““I witnessed staff with colds coughing I witnessed staff with colds coughing and sneezing in my wife's room and sneezing in my wife's room without masks on, people coming in without masks on, people coming in with gloves on they had just used with with gloves on they had just used with another patient, doctors not washing another patient, doctors not washing their hands upon entering the room, their hands upon entering the room, after touching my wife, after shaking after touching my wife, after shaking my family members' hands, etc.; my family members' hands, etc.; stethoscopes and other equipment stethoscopes and other equipment being universally shared…”being universally shared…”

““Even more shocking, while under Even more shocking, while under quarantine during her various life-quarantine during her various life-threatening infections, many, not just threatening infections, many, not just one or two, staff persons who directly one or two, staff persons who directly touched my wife, her equipment, her touched my wife, her equipment, her waste products, etc. refused to wear waste products, etc. refused to wear either protective masks and/or gloves. either protective masks and/or gloves. This was in direct violation of the This was in direct violation of the quarantine rules posted all over the quarantine rules posted all over the entrance to her room. When I entrance to her room. When I challenged these individuals, they challenged these individuals, they replied that these were simply replied that these were simply "guidelines", and that the staff person "guidelines", and that the staff person could opt to proceed at their own risk, if could opt to proceed at their own risk, if they chose to work without protective they chose to work without protective coverings…..”coverings…..”

A global issueA global issue In the US, they represent a significant portion of In the US, they represent a significant portion of
adverse events/medical errors adverse events/medical errors Affect 2 - 10% of hospitalized patients and more Affect 2 - 10% of hospitalized patients and more
than 2 million pts/yrthan 2 million pts/yr Total excess costs $ 1 billion annuallyTotal excess costs $ 1 billion annually Most costs not reimbursed when DRGs used or if Most costs not reimbursed when DRGs used or if
costs are capitatedcosts are capitated CMS will capitate reimbursement for several CMS will capitate reimbursement for several
healthcare associated infections including CA-BSI, healthcare associated infections including CA-BSI, UTI and mediastinitis.UTI and mediastinitis.
Healthcare Associated Infections Healthcare Associated Infections (HAIs)(HAIs)

Burden of Healthcare-Associated Burden of Healthcare-Associated Infections in the US, 2002Infections in the US, 2002
• 1.7 million infections in hospitals1.7 million infections in hospitals– Most (1.3 million) were outside of Most (1.3 million) were outside of
ICUsICUs– 9.3 infections per 1,000 patient-days9.3 infections per 1,000 patient-days– 4.5 per 100 admissions4.5 per 100 admissions
• 99,000 deaths associated with 99,000 deaths associated with infectionsinfections– 36,000 – pneumonia36,000 – pneumonia– 31,000 – bloodstream infections31,000 – bloodstream infections
Klevens, Edwards, Richards, et al. Pub Health Rep 2007;122:160-6Klevens, Edwards, Richards, et al. Pub Health Rep 2007;122:160-6

Costs of HAIsCosts of HAIs
• PneumoniaPneumonia24,40824,408
• BloodBlood 12,77412,774• SSISSI 7,059 7,059• UTIUTI 3,936 3,936
Medical Care 2008; 46:101Medical Care 2008; 46:101
• VAPVAP 22,87522,875• BloodBlood
18,43218,432• SSI-CABGSSI-CABG 17,94417,944• CAUTICAUTI
1,2571,257
ICHE 2007; 28:1121ICHE 2007; 28:1121

So What Are the Challenges and So What Are the Challenges and PressuresPressures

Perspective - 2009Perspective - 2009• 100,000 deaths from HAIs100,000 deaths from HAIs• Costs over 1 Billion dollarsCosts over 1 Billion dollars• Public reporting of HAI rates in many states in the US, and Public reporting of HAI rates in many states in the US, and
many European countriesmany European countries• Public reporting of MRSA BSI in the UK and Public reporting of MRSA BSI in the UK and C. difficileC. difficile in in
Quebec and OhioQuebec and Ohio• Mandatory MRSA/VRE surveillance cultures on admitted Mandatory MRSA/VRE surveillance cultures on admitted
patients in 5 states in the USpatients in 5 states in the US• Patient safety initiatives-5 million lives, CMS, institutionalPatient safety initiatives-5 million lives, CMS, institutional• JCAHO National Patient safety goalsJCAHO National Patient safety goals• Pay for performancePay for performance• Public interest and visibilityPublic interest and visibility• Medicolegal visibilityMedicolegal visibility

Legislators
Legislators
ConsumersConsumers
Provider
Provider
ss
Professional Professional organizationsorganizations
Forces impacting infection prevention Forces impacting infection prevention and controland control
Regulatory
Regulatory
agencie
s
agencie
sCMSCMSOSHAOSHAJCAHOJCAHO
CDC-guidelines, CDC-guidelines, funding, public funding, public awarenessawarenessAHRQ-guidelines, AHRQ-guidelines, fundingfunding
State legislatorsState legislators
SHEA, APICSHEA, APIC
Leapfrog, BCBSLeapfrog, BCBS
Consumers UnionConsumers UnionNational Public National Public Safety QuorumSafety Quorum
Governme
Governmentalntal

Challenge 1: Resistance/Emerging Challenge 1: Resistance/Emerging OrganismsOrganisms

Antibiotic resistance rates in ICUsAntibiotic resistance rates in ICUs
Antimicrobial-resistant pathogenAntimicrobial-resistant pathogen Pooled mean Pooled mean resistance resistance
rates in 2003 rates in 2003 (%)(%)
Percentage increase Percentage increase (2003 versus 1998 (2003 versus 1998
to 2002)to 2002)
Enterococci resistant to vancomycin (VRE)Enterococci resistant to vancomycin (VRE) 28.528.5 1212Methicillin-resistant Methicillin-resistant S. aureusS. aureus 59.559.5 1111Methicillin-resistant Methicillin-resistant S. epidermidisS. epidermidis 89.189.1 11
E. coliE. coli resistant to 3rd-generation resistant to 3rd-generation cephalosporins or aztreonamcephalosporins or aztreonam
5.85.8 00
Klebsiella pneumoniaeKlebsiella pneumoniae resistant to 3rd- resistant to 3rd-generation cephalosporins or aztreonamgeneration cephalosporins or aztreonam
20.620.6 4747
P. aeruginosaP. aeruginosa resistant to imipenem resistant to imipenem 21.121.1 1515P. aeruginosaP. aeruginosa resistant to quinolones resistant to quinolones 29.529.5 99P. aeruginosaP. aeruginosa resistant to ceftazidime resistant to ceftazidime 31.931.9 2020EnterobacterEnterobacter sppspp resistant to 3rd- resistant to 3rd-generation cephalosporinsgeneration cephalosporins
31.131.1 66
Adapted from the NNIS Report, issued October 2004Adapted from the NNIS Report, issued October 2004
Theuretzbacher U, Toney JH. Current Opinion in Invest Drugs 7(2):158, 2006Theuretzbacher U, Toney JH. Current Opinion in Invest Drugs 7(2):158, 2006

Worldwide prevalence of MRSAWorldwide prevalence of MRSA
Grundmann et al. Lancet 2006; 368: 874-85Grundmann et al. Lancet 2006; 368: 874-85

Community acquired MRSACommunity acquired MRSA• Emergence in patients without established risk factorsEmergence in patients without established risk factors• Skin, soft tissue infections, necrotizing fasciitis & pneumoniaSkin, soft tissue infections, necrotizing fasciitis & pneumonia• Genetically distinctGenetically distinct
– Clonal strains USA 300 and USA 400 by PFGEClonal strains USA 300 and USA 400 by PFGE– Contain Panton-Valentine Leukocidin & other enterotoxins with Contain Panton-Valentine Leukocidin & other enterotoxins with
different SCCdifferent SCCmec mec (type IV a-d) (type IV a-d) • Not multi-drug resistantNot multi-drug resistant
– Resistant to pen, ox; +/- R erythro, quinolones, clindamycin, Resistant to pen, ox; +/- R erythro, quinolones, clindamycin, • Movement into HealthcareMovement into Healthcare
– 132 cases of MRSA BSI -- 2004 (incidence 6.8/1,000 adm)132 cases of MRSA BSI -- 2004 (incidence 6.8/1,000 adm)– 42% met criteria for nosocomial infection42% met criteria for nosocomial infection– 34% USA300 genotype; USA300 accounted for 28% of healthcare- 34% USA300 genotype; USA300 accounted for 28% of healthcare-
associated infections & 20% of nosocomial BSI.associated infections & 20% of nosocomial BSI.
Seybold, et al. Clin Infect Dis. 2006;42:647-56Seybold, et al. Clin Infect Dis. 2006;42:647-56..

The changing face ofThe changing face of C. difficile C. difficile • Increase in incidence and emergence of Increase in incidence and emergence of
community casescommunity cases– 2005 10 peri-partum and 23 community acquired CDAD 2005 10 peri-partum and 23 community acquired CDAD
( 3/5 children hosp) reported in 4 states( 3/5 children hosp) reported in 4 states– 24% no exposure to abx within 3 mo - several in contact 24% no exposure to abx within 3 mo - several in contact
with persons with diarrhea; 9% had <3 doses of abxwith persons with diarrhea; 9% had <3 doses of abx• Designated as NAP1 / BI, Toxinotype IIIDesignated as NAP1 / BI, Toxinotype III• 18 bp deletion in 18 bp deletion in tcdC, tcdC, mechanism may be mechanism may be
increased toxin productionincreased toxin production• Increased resistance to fluoroquinolonesIncreased resistance to fluoroquinolones• Spread -- Europe, Canada, North East, Mid Spread -- Europe, Canada, North East, Mid
Atlantic, MidwestAtlantic, Midwest
McDonald et al. NEJM 2005;353:2433-41.McDonald et al. NEJM 2005;353:2433-41.Warny et al. Lancet 2005; 366:1079-84Warny et al. Lancet 2005; 366:1079-84MMWR 2006; 295:1 25.MMWR 2006; 295:1 25.

r = 0.976, P<.001 for P aeruginosa; r = 0.891, P = .007 for GNR; r = 0.958, P<.001 for years of observation
Fluoroquinolone Use and Fluoroquinolone Use and Resistance Rates in Resistance Rates in P. aeruginosaP. aeruginosa
and GNRand GNR
Neuhauser MM, et al. JAMA. 2003;289:885-8Neuhauser MM, et al. JAMA. 2003;289:885-8..

Does Antibiotic Use increase MRSADoes Antibiotic Use increase MRSA
Monnet et al 2004:10: 1432Monnet et al 2004:10: 1432Wertheim et al 2006Wertheim et al 2006
•MRSA is in addition to other MRSA is in addition to other S. aureusS. aureus infections infections•Traditionally associated with exposure to healthcare Traditionally associated with exposure to healthcare or antimicrobialsor antimicrobials•In Europe, totalIn Europe, totalambulatoryambulatoryantibiotic useantibiotic usecorrelated withcorrelated withMRSA bloodMRSA bloodcultures (R=0.49, cultures (R=0.49, p=0.01)p=0.01)

ResistantResistantOrganismsOrganisms
NativeNativeOrganismsOrganisms
AnimalsAnimals
HumansHumans
EnvironmentEnvironmentAntibioticAntibioticExposureExposure
GeneticGeneticTransfersTransfers
TransmissionTransmissionEmergenceEmergence
EradicationEradication
HealthHealthPolicyPolicy
Hand HygieneHand Hygiene
DecontaminationDecontaminationAntibiotic Antibiotic
ManagementManagementIsolation/Isolation/Barrier Barrier
PrecautionsPrecautions
SurveillanceSurveillance

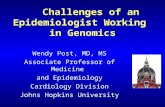
Hand Imprint Cultures After Hand Imprint Cultures After Contact Contact
with Environmental Surfaceswith Environmental Surfaces
0
10
20
30
40
50
60
Environmental cultures growing
organisms (%)
Total S. aureus VRE GNB C. difficileOrganisms
Occupied RoomsCleaned Rooms
Bhalla A, et al. Infect Control Hosp Epidemiol. 2004;25:164-7Bhalla A, et al. Infect Control Hosp Epidemiol. 2004;25:164-7..

Linking the environment to infectionLinking the environment to infection
Hardy et al. Infection Control and Hospital EpidemiologyHardy et al. Infection Control and Hospital Epidemiology 2006;27:127-132 2006;27:127-132

Challenge 2: Knowledge, Attitudes Challenge 2: Knowledge, Attitudes and Behaviorsand Behaviors

N Opportunities N Opportunities ComplianceCompliance
NurseNurse (520)(520) 1875 ( 66 %) 1875 ( 66 %) 52 %52 %Student nurseStudent nurse (48) (48) 131 (4.7 %) 131 (4.7 %) 43 %43 %Nurses' aideNurses' aide (166)(166) 378 378 (13 %) (13 %) 47 %47 %Mid-wifeMid-wife (14) (14) 35 (1.3 %) 35 (1.3 %) 66 %66 %PhysicianPhysician (158) 281 (158) 281 (10 %)(10 %) 30 %30 %Phys/Resp therapist Phys/Resp therapist (23)(23) 48 48 (1.7 %) (1.7 %) 28 % 28 %Radiology TechnicianRadiology Technician (4) (4) 12 12 (0.4 %) (0.4 %) 8 % 8 %OthersOthers (58) (58) 74 74 (2.7 %) (2.7 %) 27 %27 %TOTALTOTAL 2,834 (100 %) 2,834 (100 %) 48 % 48 %
Pittet et al, Ann Intern Med 1999,Pittet et al, Ann Intern Med 1999, 130:126130:126
Compliance and professionCompliance and profession

Beliefs and perceptions affecting physician Beliefs and perceptions affecting physician hand hygiene beliefshand hygiene beliefs
Number of observations (opportunities) = 811; number of physicians = 147Number of observations (opportunities) = 811; number of physicians = 147*95% CI = 95% Confidence Interval*95% CI = 95% Confidence Interval
Psycho-social variablesPsycho-social variables
Pittet et al. Ann Intern Med 2004; 141: 1-8Pittet et al. Ann Intern Med 2004; 141: 1-8

Challenge 3: Public Perception and Challenge 3: Public Perception and ConsumersConsumers


USA Today May 11, 2006USA Today May 11, 2006Atlanta Journal Constitution,Atlanta Journal Constitution, March 14, 2003March 14, 2003

The Baltimore area has a variety of social and economic factors that lead to higher than average MRSA rates in the community….

Challenge 4: Pay For PerformanceChallenge 4: Pay For Performance

CMS No Pay for PerformanceCMS No Pay for PerformanceConditions for 2008Conditions for 2008
– Air EmbolismAir Embolism– Blood IncompatibilityBlood Incompatibility– Catheter-Associated Urinary Tract InfectionsCatheter-Associated Urinary Tract Infections– Pressure Ulcers (Decubitus Ulcers)Pressure Ulcers (Decubitus Ulcers)– Vascular Catheter Associated Blood Stream Infections Vascular Catheter Associated Blood Stream Infections – Surgical Site Infection After Elective Surgery (Orthopedic Surgical Site Infection After Elective Surgery (Orthopedic
and Bariatric)and Bariatric)– Mediastinitis after coronary bypass surgeryMediastinitis after coronary bypass surgery– In Hospital FallsIn Hospital Falls– Postoperative Deep Vein Thrombosis, Pulmonary Embolism Postoperative Deep Vein Thrombosis, Pulmonary Embolism
after Knee and Hip Replacementafter Knee and Hip Replacement– Glycemic Control Complications:Glycemic Control Complications:
Diabetic KetoacidosisDiabetic Ketoacidosis– Objects left in after SurgeryObjects left in after Surgery
Hyperosmolar coma (Diabetic or Hypoglycemic Hyperosmolar coma (Diabetic or Hypoglycemic Coma)Coma)
Conditions considered for 2009 Conditions considered for 2009 – Ventilator-Associated PneumoniaVentilator-Associated Pneumonia– Methicillin Resistant Staphylococcus Aureus (MRSA)Methicillin Resistant Staphylococcus Aureus (MRSA)– Clostridium Difficile-Associated Disease (CDAD)Clostridium Difficile-Associated Disease (CDAD)– Staphylococcus aureus SepticemiaStaphylococcus aureus Septicemia– Legionnaires DiseaseLegionnaires Disease– DeliriumDelirium– Iatrogenic PneumothoraxIatrogenic Pneumothorax

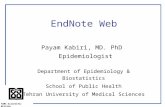
Challenge 5: Public ReportingChallenge 5: Public Reporting

Healthcare Associated Infections Healthcare Associated Infections Reporting Laws: USReporting Laws: US

MRSA reporting laws: USMRSA reporting laws: US

Consequences of HAI Public Reporting Consequences of HAI Public Reporting and Reimbursement Changesand Reimbursement Changes
• Presumed to motivate quality improvementPresumed to motivate quality improvement– Patients, physicians, purchasers select high quality Patients, physicians, purchasers select high quality
physicians or institutionsphysicians or institutions– Motivate physicians and institutions to compete on Motivate physicians and institutions to compete on
qualityquality• May have unintended or negative May have unintended or negative
consequencesconsequences– Also largely unexploredAlso largely unexplored– e.g., Improper utilization of resources, adverse e.g., Improper utilization of resources, adverse
patient selectionpatient selection

PreventionPrevention

Potential Prevention and Control Potential Prevention and Control MeasuresMeasures
• Infection Prevention/ControlInfection Prevention/Control– Hand hygieneHand hygiene– Isolation and barrier precautionsIsolation and barrier precautions– Cohorting or separation of colonized/infected Cohorting or separation of colonized/infected
and non-colonized patientsand non-colonized patients– Control of environmental or other potential Control of environmental or other potential
sourcessources– TechnologyTechnology– ImmunizationImmunization
• Antibiotic stewardship/managementAntibiotic stewardship/management

A patient with meningococcal meningitis was A patient with meningococcal meningitis was admitted last night. Nobody wore masks? admitted last night. Nobody wore masks? Who was exposed and needs prophylaxis?Who was exposed and needs prophylaxis?
You see 5 MRSA surgical site infections on GI You see 5 MRSA surgical site infections on GI surgery when you go on service. The surgery when you go on service. The infections occurred over 3 weeks? What do infections occurred over 3 weeks? What do you do? Is this an outbreak?you do? Is this an outbreak?
The influenza vaccination rate among HCWs The influenza vaccination rate among HCWs is only 40% what do you do?is only 40% what do you do?
Putting the Questions into PerspectivePutting the Questions into Perspective

• What are the facts?What are the facts? What does the literature tell you?What does the literature tell you? Is the intervention evidence based?Is the intervention evidence based?
• Are there regulatory issues?Are there regulatory issues?• What are the medico-legal issues?What are the medico-legal issues?• Are there ethical considerations?Are there ethical considerations?• What are the behavioral considerations (we have What are the behavioral considerations (we have
always done it this way)?always done it this way)?• How do you make your case and advertise--”selling How do you make your case and advertise--”selling
your point of view?your point of view?
How do you make a case for IC How do you make a case for IC interventions and strategies?interventions and strategies?

Considerations for the Healthcare Considerations for the Healthcare EpidemiologistEpidemiologist
• Are we surveying “significant” events? Are we surveying “significant” events? – Willie Sutton ruleWillie Sutton rule
• Are we meeting the regulatory requirements?Are we meeting the regulatory requirements?• Is our surveillance meaningful?Is our surveillance meaningful?
– Defined eventsDefined events– Adequate case-finding strategiesAdequate case-finding strategies– Validated methodology esp with computerized systemsValidated methodology esp with computerized systems– Inter-observer reliabilityInter-observer reliability
• Are we providing to the people who can change Are we providing to the people who can change things in a meaningful waythings in a meaningful way

Evidence-based infection control is... Evidence-based infection control is... ...the ...the explicitexplicit, , judiciousjudicious and and
conscientiousconscientious use of use of current best current best evidenceevidence from infection control from infection control researchresearch
in in making decisionsmaking decisions about the about the prevention and control of infection of prevention and control of infection of
individuals and populationsindividuals and populations..
Focus on the EvidenceFocus on the Evidence

BMJ 327:1459 (2003)

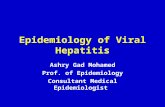
Oh the Places You Can Go--JHH CA BSI Oh the Places You Can Go--JHH CA BSI Rates (1998-2008)Rates (1998-2008)
0.002.004.006.008.00
10.0012.0014.0016.00
19981999200020012002200320042005200620072008
Rate/1000 Catheter Days
JHH SICU7 NNIS Pooled Mean NNIS 90th percentile
Berenholtz, CCM 2004:32(10):2014Berenholtz, CCM 2004:32(10):2014
Surveillance and data feedbackSurveillance and data feedbackExecutive engagementExecutive engagementDevelop policiesDevelop policies
““The bundle”The bundle”•Remove the catheterRemove the catheter•Practice hand hygienePractice hand hygiene•Use CHG skin prepUse CHG skin prep•Wear/use maximal barrier precautionsWear/use maximal barrier precautions•Avoid the femoral site for CVC placementAvoid the femoral site for CVC placement

In SumIn Sum
• Healthcare epidemiologists do public health in the Healthcare epidemiologists do public health in the hospital and their role is to be the hospital and their role is to be the “consciousness” of the institution“consciousness” of the institution
• The public and regulatory atmosphere has The public and regulatory atmosphere has increased the visibility of infection prevention and increased the visibility of infection prevention and controlcontrol
• Fellows have a huge role in 1) understanding the Fellows have a huge role in 1) understanding the population implications of HAIs, epidemiologic population implications of HAIs, epidemiologic significant organisms; 2) knowing the evidence significant organisms; 2) knowing the evidence behind prevention and control strategies; 3) behind prevention and control strategies; 3) identifying clusters; 4) spreading the wordidentifying clusters; 4) spreading the word

Finally—it’s a great job!Finally—it’s a great job!