HealthCare Associated Infections in Acute Care Hospitals Data from July 1, 2009 – June 30, 2011...
39
HealthCare Associated Infections in Acute Care Hospitals Data from July 1, 2009 – June 30, 2011 Public Health Council
-
Upload
malcolm-byrd -
Category
Documents
-
view
213 -
download
0
Transcript of HealthCare Associated Infections in Acute Care Hospitals Data from July 1, 2009 – June 30, 2011...

HealthCare Associated Infections in Acute Care Hospitals
Data from July 1, 2009 – June 30, 2011
Public Health Council
Massachusetts Department of Public Health
Reporting Philosophy•To catalyze hospital-specific and statewide initiatives to address the most prevalent preventable infections through surveillance and dissemination of best practices
•To validate that the extensive work conducted across the health system often reduces the rate of preventable adverse health events, and to refocus interventions where such reduction is not seen
•To further inform consumers, policy-makers, and providers on the frequency and setting of adverse events
•To report the occurrence of HAIs as a means to inform improvement as a core measure of hospital quality and safety; these measures are not intended to be punitive
Not all HAIs may be averted. However, our goal remains elimination of all those adverse events which are preventable. The long-term goal of HAI reporting is to minimize the number of these occurrences through increased awareness and development of robust
systems for error trapping and prevention. Therefore, we seek to gain a greater understanding of how preventable infections happen and how they can be prevented in the
future
Massachusetts Department of Public Health
A New Philosophy
•To increase accessibility to consumers, policy-makers, and technical experts alike
•To develop data feedback loops to focus high-yield interventions
•“Not letting the perfect get in the way of the good”

Massachusetts Department of Public Health
HAI Background
• HAI recognized as a critical challenge to patient safety and public health
• Increased attention due to role in escalating healthcare costs, patient and family impact and recognition many are preventable
• Aggressive national and local efforts to address HAI
• Targeted by HHS and CMS for nonpayment
Massachusetts Department of Public Health
HAI Data Overview
• The public presentation of quality and safety data is essential to the DPH commitment to transparency and accountability
• Consumers need reliable data to help make informed healthcare decisions
• Providers need standardized performance measures to support improvement efforts
• Policy makers require access to data to target prevention efforts, promote alignment of incentives and reinvestment in successful strategies.
•

Massachusetts Department of Public Health
Statutory & Regulatory Framework• Massachusetts law provides DPH with legal authority to
conduct surveillance and to investigate and control spread of communicable and infectious diseases• MGL c.111, sections 6 & 7
• HAI regulatory language can be found in 105 CMR 130.000

Massachusetts Department of Public Health
Acknowledgements• Deb Wachenheim (Health Care for All)• Paula Griswold (MA Coalition for the Prevention of Medical Errors)• Deb Yokoe (Brigham & Women’s Hospital)• Ken Sands & Sharon Wright (Beth Israel Deaconess Medical Center)• John Snow Inc. data validation team• Charles Deutsch, Richard Platt, Michael Klompas, Ken Kleinman, Karen
Kieser (Harvard Catalyst)• Al DeMaria, Shauna Onofrey, Johanna Vostok, Nora McElroy, Will Lapsley
(DPH HAI Epidemiology Team)• Eileen McHale (DPH HAI Coordinator) • Karen Boudreau (Institute for Health Care Improvement)• MDPH Healthcare Associated Infection Technical Advisory Group• NHSN staff• Commissioner Auerbach

Massachusetts Department of Public Health
2012 Reporting Goals
• Present objective data using national standardized definitions and scientifically sound analysis
• Provide reports that are useful, accessible and understandable for consumers, providers and policy makers
• Use data to inform policy, drive innovation and quality improvement
Massachusetts Department of Public Health
Process for Improvement
• MDPH leadership commitment to creating change and driving improvement
• Collaboration with a diverse group of stakeholders
• Evaluated multiple options for depiction of data graphics intended to improve understanding of data
• Includes hospital specific summary to be used by facilities as an improvement tool

Massachusetts Department of Public Health
History
Massachusetts Department of Public Health
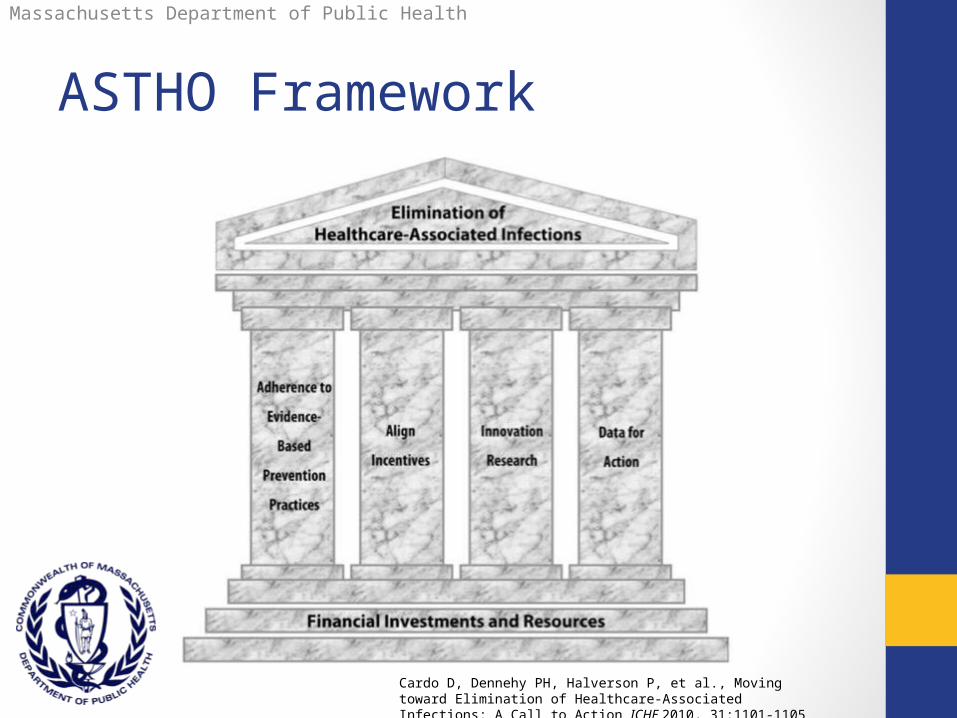
ASTHO Framework
Cardo D, Dennehy PH, Halverson P, et al., Moving toward Elimination of Healthcare-Associated Infections: A Call to Action ICHE 2010, 31:1101-1105
Massachusetts Department of Public Health
How to Use this Report
• “…every member of the health care team, from the doctor to patients and their families, has a role in prevention and elimination of HAIs…”
• Key risk factors – shared responsibility
• Encourages candid communication with providers
• “…many factors contribute to a hospital’s quality of care. The overall quality and safety of a hospital is not determined only by HAI rates…”
• Resources for patients and their families

Massachusetts Department of Public Health
Why HAI?• Among the leading causes of preventable death in U.S.
• 1 in 20 hospitalized patients affected
• 1.7 million infections/99,000 deaths
• 2007, the annual economic burden of HAI in Massachusetts ranged from $200 to $400 million.
• 2009 CDC estimated the U.S. direct medical cost of treating HAI ranges from $35.7 billion to $45 billion annually.
• Adherence to evidence based practices can reduce certain HAIs by as much as 70 percent.
Massachusetts Department of Public Health
Surveillance
• systematic collection, analysis, and interpretation of data on the occurrence of infectious diseases or events
• all healthcare facilities reporting data must use the same definitions • National Healthcare Safety Network.
• Extensive data validation (JSI)
Massachusetts Department of Public Health
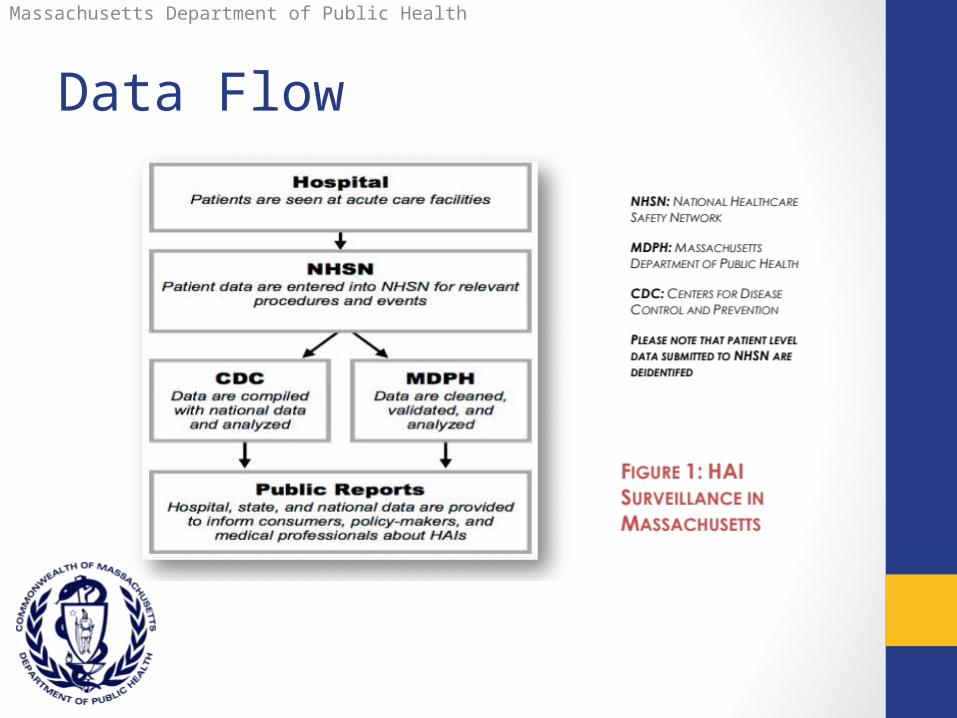
Data Flow
Massachusetts Department of Public Health
CLABSI
• Central Line Associated Blood Stream Infections• “The CDC defines a CLABSI as recovery of a pathogen
from a blood culture (a single blood culture for organisms not commonly present on the skin and two or more blood cultures for organisms commonly present on the skin) in a patient who had a central line at the time of infection or within the 48-hour period before development of infection”
• 12,000 to 28,000 per year. Each episode costs ~$16,550
• Use of central lines directly correlated to infections rates

Massachusetts Department of Public Health
SSI• Surgical Site Infections:
• hysterectomy (abdominal and vaginal), knee and hip arthroplasty, coronary artery bypass graft
• more than half of SSIs are not identified until patients are discharged from the hospital and patients with infection do not always return to the same hospital where the original surgery was performed.

Massachusetts Department of Public Health
Risk Adjustment & Stats• Many factors may contribute to infections, including prior
health history, age, complications of a procedure, smoking, obesity, and others.
• Models used attempt a correction for some degree of risk, they likely do not entirely eliminate differences between facilities that may result from this risk.
• CLABSI: state and national baselines• SSI: national baseline only (smaller sample size)
Massachusetts Department of Public Health
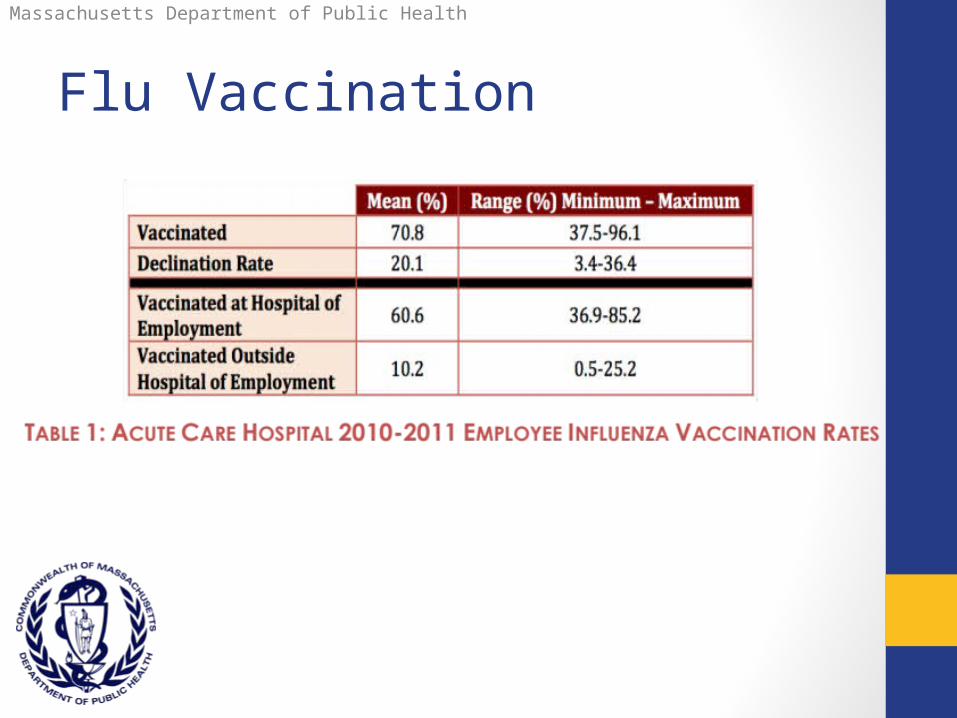
Flu Vaccination
Massachusetts Department of Public Health
Data Highlights• Summarizes HAI rates in acute care hospitals for
the reporting period of July 1, 2009 – June 30, 2011
• New - Hospital specific “Summary Sheets” (handout)
• Describes prevention activities and initiatives
• Improved graphics and readability

Massachusetts Department of Public Health
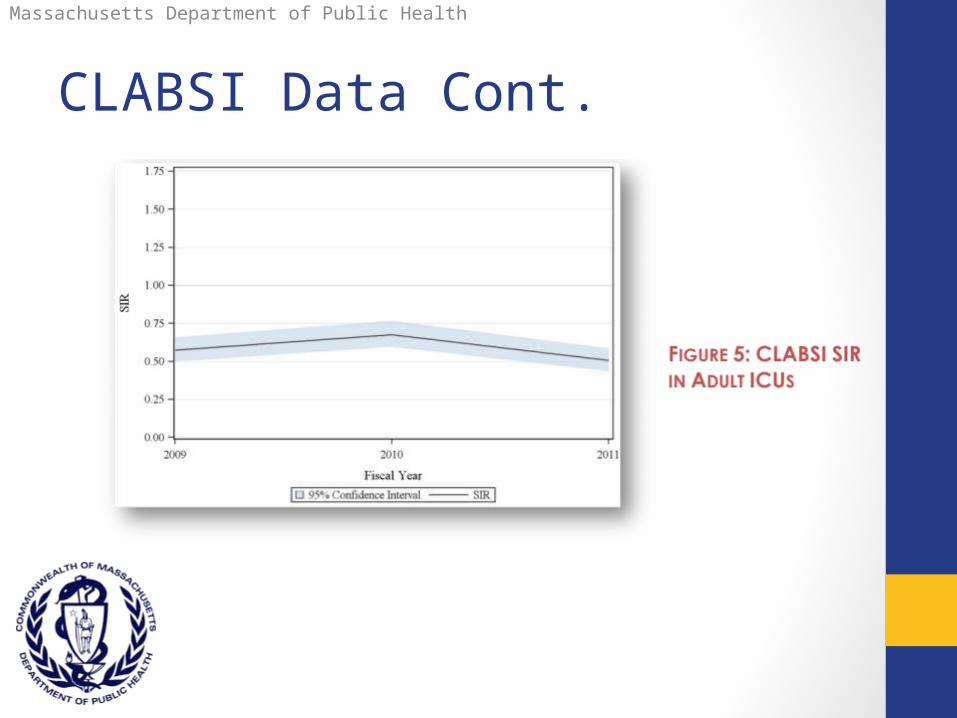
CLABSI Data• Massachusetts acute care hospitals reported 199 CLABSIs
during FY11, an overall decrease in SIR of 24% from FY10
• SIR in all ICU types was statistically the same or lower than predicted compared with both state and national baselines.
• Compared with state baseline, SIR of medical ICUs in major teaching hospitals and SIR of NICUs for babies 751-1000g were statistically significantly improved FY10 FY11.
• Central line utilization only modestly decreased.

Massachusetts Department of Public Health
CLABSI Data cont.
Massachusetts Department of Public Health
CLABSI Data Cont.

Massachusetts Department of Public Health
CLABSI Data Cont.

Massachusetts Department of Public Health
Central Line Utilization

Massachusetts Department of Public Health
CLABSI Pathogens
Massachusetts Department of Public Health
Surgical Site Infections• Hip arthroplasty statistically significantly lower than
predicted
• Vaginal hysterectomy statistically significantly higher than predicted
• Knee arthroplasty, abdominal hysterectomy, and CABG as predicted
• Primary barrier to good data is high variability of post-discharge surveillance capacity; reliance on admin data provides limited insights.

Massachusetts Department of Public Health
SSI Data
Massachusetts Department of Public Health
Vaginal Hysterectomy• Statistical high-outlier in FY10 and FY11
• Further investigation is needed to determine causes • though it may in part be due to coding inconsistencies by
which hysterectomies with an abdominal incision but a vaginal extraction are counted as vaginal hysterectomies.
• Not mandated nationwide therefore smaller pool for national baseline
• DPH is assembling a small working group of key stakeholders/outliers to assess etiology and disseminate best practices

Massachusetts Department of Public Health
SSI Pathogens

Massachusetts Department of Public Health
SSI Outliers (high and Low)

Massachusetts Department of Public Health
One-Pagers
Caution Page
(description of statistical
limitations)
Overview Page
(explanation of how to read
hospital-specific one
pagers)

Massachusetts Department of Public Health
One-PagerTemplate
Massachusetts Department of Public Health
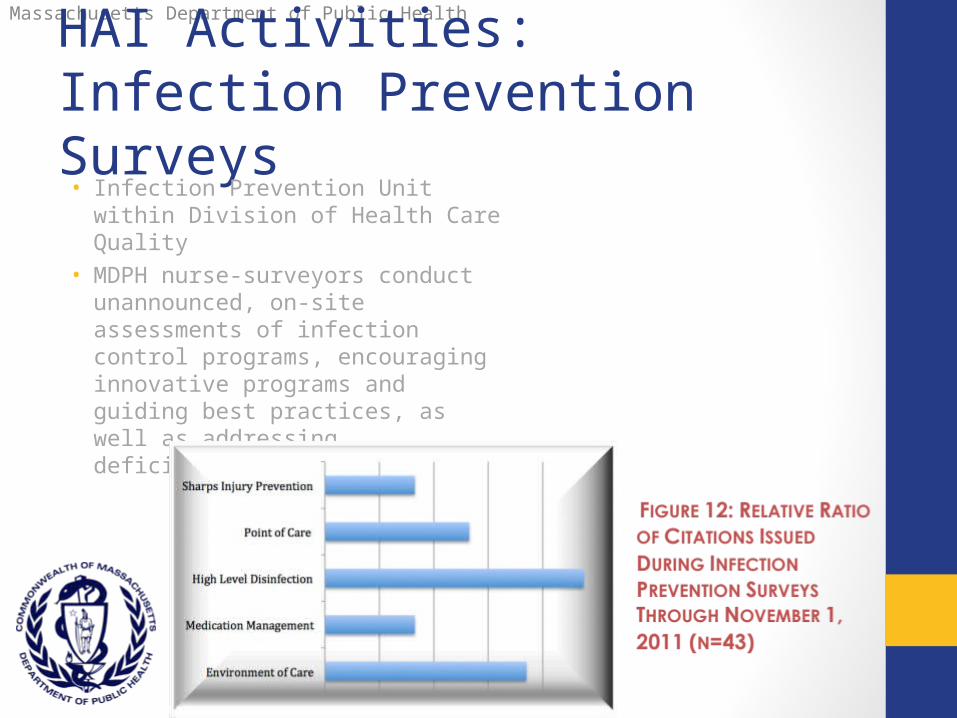
HAI Activities: Infection Prevention Surveys• Infection Prevention Unit within Division
of Health Care Quality
• MDPH nurse-surveyors conduct unannounced, on-site assessments of infection control programs, encouraging innovative programs and guiding best practices, as well as addressing deficiencies or concerns

Massachusetts Department of Public Health
ARRA Funding
• Coordination and Reporting of State HAI Prevention Efforts
• Detection and Reporting of HAI Surveillance Data
• Establishing a Prevention Collaborative (C. difficile)

Massachusetts Department of Public Health
Collaboratives• 2009 -2011: CDC, MDPH, MA Coalition, Masspro
• C. difficile Infection Prevention in Hospitals
• 2011- July 2012: CDC, MDPH, MA Coalition, Mass Senior Care, Masspro
• C. difficile Infection Prevention Partnerships in Hospitals and Skilled Nursing Facilities
• Expansion of HAI prevention to additional settings of care – Long Term Care. 17 acute care hospital teams and 74 long term care facilities participating
• Evidence based CDI prevention recommendations• Expanding professional social networks• Teaching and encouraging use of QI methods,
focusing especially on small tests of change• Teaching and encouraging use of adaptive
strategies for front line staff engagement.
• 2009 -2011: CDC, MDPH, MA Coalition, Masspro• C. difficile Infection Prevention in Hospitals
• 2011- July 2012: CDC, MDPH, MA Coalition, Mass Senior Care, Masspro
• C. difficile Infection Prevention Partnerships in Hospitals and Skilled Nursing Facilities
• Expansion of HAI prevention to additional settings of care – Long Term Care. 17 acute care hospital teams and 74 long term care facilities participating
• Evidence based CDI prevention recommendations• Expanding professional social networks• Teaching and encouraging use of QI methods,
focusing especially on small tests of change• Teaching and encouraging use of adaptive
strategies for front line staff engagement.

Massachusetts Department of Public Health
Report Dissemination PLan• This report is an important step in promoting transparency
for healthcare consumers and motivation for hospitals to continue to prioritize HAI prevention but much remains to be done to accelerate progress towards the goal of HAI elimination
• MDPH has contacted CQOs (or CMOs) in high and low outliers prior to public release
• Over time MDPH will continue to refine and enhance data presentation
• MDPH will continue to work with hospitals and additional state and national organizations in a comprehensive effort to address these largely preventable infections.
Text report will be posted online today. Hospital-specific fact sheets will be posted by Friday

Massachusetts Department of Public Health
• Facilitating continuous QI.
• Moving towards consumer self-assessment of risk to inform decision making.
• Make the reported HAI data easily actionable & readily available so that reports may be used to more rapidly drive improvements.
• Developing thresholds for action and recommended next steps if these thresholds are reached.
• Benchmarking our state not against national averages, but against high-performers in the 80th percentile and higher.
• Dual focus on clinical and surveillance data.
Looking to the Future
Massachusetts Department of Public Health
Thank you
Massachusetts Department of Public Health
Bureau of Health Care Safety & Quality
Office of Emergency Medical Services
99 Chauncy Street, 11th Floor
Boston, MA 02111
617.753.8000
For Further Information, Please Contact
Iyah Romm, Special Assistant to the Director