
Health System Design to Impact Social Determinants...
46
11/23/2015 1 Health System Design to Impact Social Determinants of Health Cory Sevin, IHI Jill Kemper; ICSI Brigid McCaw, Kaiser Permanente Beth Heinz, HealthPartners Tom Blee John Turnipseed, L24 This presenter has nothing to disclose December 6 th 2015 1:00-4:30 ET Orlando, FL #27FORUM Session Objectives Describe how partnerships with community stakeholders broaden the reach and impact of healthcare systems. Identify how unique and impactful partnerships are formed to impact a health issue. Identify 3-5 ideas you can test in your own context. P2 #27FORUM
Transcript of Health System Design to Impact Social Determinants...
11/23/2015
1
Health System Design to Impact Social Determinants of Health
Cory Sevin, IHIJill Kemper; ICSI
Brigid McCaw, Kaiser Permanente
Beth Heinz, HealthPartners
Tom Blee
John Turnipseed,
L24This presenter has
nothing to disclose
December 6th 2015
1:00-4:30 ET
Orlando, FL
#27FORUM
Session Objectives
Describe how partnerships with community stakeholders
broaden the reach and impact of healthcare systems.
Identify how unique and impactful partnerships are
formed to impact a health issue.
Identify 3-5 ideas you can test in your own context.
P2
#27FORUM
11/23/2015
2
Agenda
Welcome and introductions
Health Care Meets People Where They Are - At
Court
Table Work-how does this apply to me?
LIFETeam: Breaking the Cycle of Violence
3:05-3:25 Break
Transforming Health Response to Domestic ViolenceTable Work-how does this apply to me?
4:30 Adjourn
P3
Health Care Meets People Where They
Are – In Court
December 6, 2015
IHI National Forum

11/23/2015
3
• Screening to identify people at risk for developing substance use disorders.
• Brief Intervention to raise awareness of risks and consequences, internal motivation for change, and help set healthier goals.
• Referral to Treatment to facilitate access to treatment and coordinate services between systems for people with higher risk and/or dependence.
SBIRT for Risky Substance Use
5
What do we know?
MN/St. Louis County Data*
• 25,258 DWI arrests in MN (1037 in St. Louis County)
• 60% are first time violators
• Over the last 10 years, 71% of all DWI arrests were first time violators
• 2 out of 3 arrested for DWI never receive a second DWI
*MN Impaired Driving Facts 2014
SBIRT Research*
• Court ordered screening is coercive by nature.
• Target the time when is person most amenable to intervention.
• Design screening as part of brief intervention to increase insight, honesty and motivation.
*Lapham, 2004
6

11/23/2015
4
Hon. Shaun Floerke
7
News clip from KBJR Duluth
Better Approach
"If somebody comes in and they're low risk/low need, and I treat them as though they're high risk/high need, I can actually harm them. I can make them worse.
You're not trying to make them criminalized. You're not trying to pull them deeper into the system.”
- Judge Shaun Floerke
8

11/23/2015
5
Distribution of Alcohol Use
Abstinent/Lo
w risk
Moderate risk High Risk
Primary PreventionBrief Intervention
Specialized Treatment
Disorder
40%35%
20%
5%
Target
Population
Target
Population
9
Core Team– Hon. Shaun Floerke, 6th District Court
– Julie Seitz and Kim Davis, Center for Alcohol & Drug
Treatment
– Greg Anderson and Matt Johnson, St. Louis County
Health & Human Services
– Nicole Korby and Amy Turnquist, Court Administration
– John Walker and Heather Kussatz, Arrowhead Regional
Corrections
– Jill Eichenwald, Public Defense
– Capt. Steve Stromback, MN State Patrol
10
11/23/2015
6
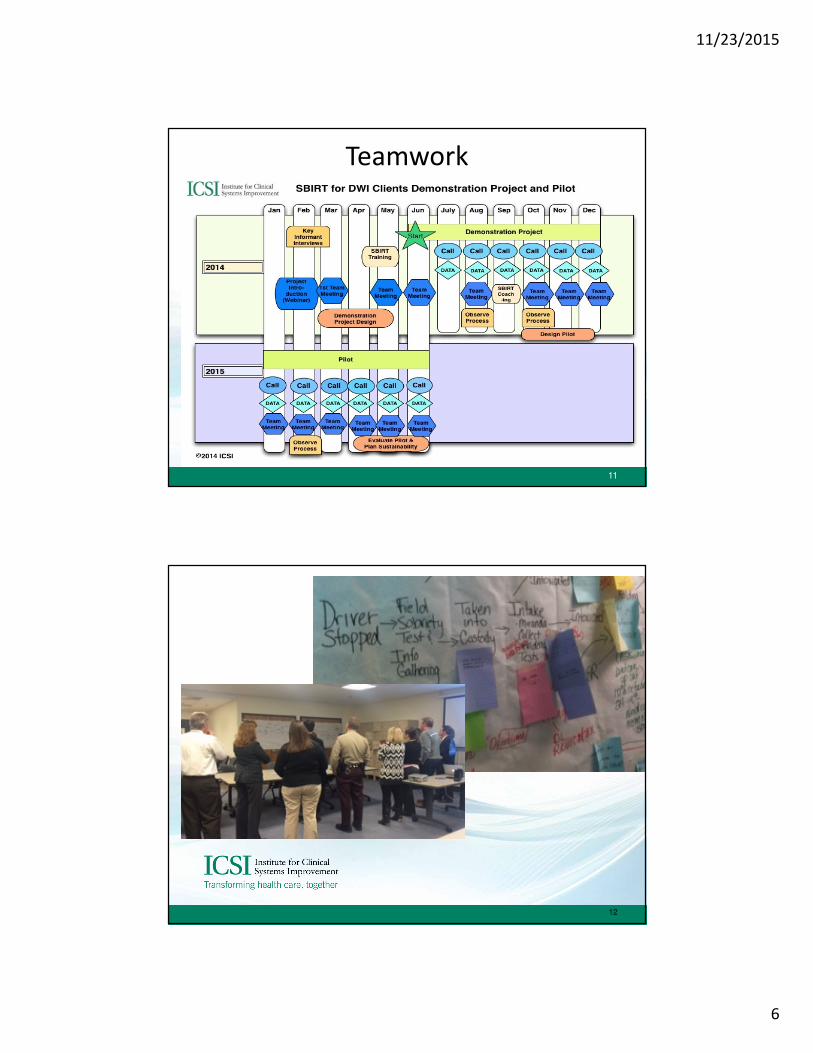
Teamwork
11
12

11/23/2015
7
Process
13
Key Improvements
• Locating interventionists in the courtroom
• Holding Bench meetings and keeping SBIRT
info out of client court file
• Having ARC, PHHS and CADT do the S & BI
• Reducing client fine by $50 when follow-up
appointments were completed
14

11/23/2015
8
24
75
117
175
257
367
14
46
68
110
168
236
716
33 39 4155
0
50
100
150
200
250
300
350
400
Week 1-10 Week 1-20 Week 1-30 Week 1-40 Week 1-50 Week 1-67
SBIRT Screens (data as of 9/17/15)
#Arrests Scheduled in Court
#Screened
#Potential Future Screens
15
16
11/23/2015
9
Client Comments
• “More time to process helps, this isn't just a parking
ticket…”
• “I’m not changing a lot, but I'm more aware of what I
should and shouldn’t do…”
• “This was amazing. I thought I could have 3 drinks and
still drive. This stuff should be taught in high school…”
17
Follow Up
• 3-4 weeks after initial Screening/Brief
Intervention
• Discuss goals/progress
• -Audit- C
• Participation incentive/ reduction in fines
• Exploring alternative options for follow-up
including electronic means.
18

11/23/2015
10
19
20

11/23/2015
11
How Does This Apply To Me?P21
#27FORUM
LIFE Team Helping Hurt People Who Hurt People
Dr. Tom Blee, John Turnipseed, & Beth Heinz

11/23/2015
12
Learning Objectives
Learn about the LIFE
Team program
What disparities do you see
in your community?
Apply learnings to improve the
health of your
community
Who We Are
• Beth Heinz
• Vice President of Operations, Regions Hospital
• Chief Quality Officer, Regions Hospital
• Thomas H. Blee, M.D.
• Assistant Professor of Surgery, University of Minnesota
• Trauma Surgeon, Regions Hospital
• John Turnipseed
• Vice President, Urban Ventures

11/23/2015
13
Health
planMedical
clinics
Dental
clinicsHospitals
Research
&
education
Nonprofit, consumer governed
HealthPartners Integrated Care
Who We Are: Regions Hospital
• Located in St. Paul, Minnesota
• Part of HealthPartners, the largest
consumer governed, nonprofit health
care organization in the nation
• Level 1 Adult and Pediatric Trauma
Center
• 800 Trauma team activations per year
90% Blunt
10% Penetrating

11/23/2015
14
Regions Hospital: Trauma Registry Data
• Average 340 admissions each year for “Assaults”
– 45% Assaults
– 32% Stabs
– 23% Gunshot Wounds
• 84% of patients are male
• 80% of patients are absent fathers
• Dr. Blee’s interaction with repeat
patients
LIFE Team History

11/23/2015
15
What is LIFE Team?Leadership Impacting the Family Environment
• At-risk individuals are identified, and
encouraged to participate in beginning a
positive life transformation
• Multiple intervention techniques focus
on stabilizing lives
– Physically
– Socially
– Economically
– Renewing each individual’s bond to the
community
LIFE Team Process
If the patient meets one or more of the following criteria, refer the
patient to LIFE Team:
• Gang involvement with a desire to get out
• History of perpetrating violence and a desire to change
• History of felonies/legal issues that are impacting ability to secure
employment
• Difficulty securing stable employment and are in a need for
training/interview skill teaching etc.
• History of lack of parental involvement/familial support resulting in
psychosocial issues and the patient could benefit from mentoring
• Need for parental skills training

11/23/2015
16
Community and Hospital Partnership
Case Study
• Surgical complexity
– 5 surgeries in a short period of time
• Stayed about one month on
trauma unit
• Couldn’t eat
• PTSD

11/23/2015
17
Case Study
• The Talk
– Grim discussion
– Needed a miracle
• The Solution: John Turnipseed and
Urban Ventures
• Hope
• Transformation
• Fixing a generational problem
• Health care costs
– Stopped future violence
related visits
Intervention Results

11/23/2015
18
• Direct interventions work best
– Consistency, keep showing up
– Train story
• Most powerful tools
– Rest
– Laughter
• Not every person ready to change
• Model is self perpetuating
Lessons Learned
Conclusions
• Hurt people hurt people
• Most effective when you stay in your strike zone
• Don’t reinvent the wheel, move your resources to
the problem
• The ultimate trauma prevention strategy is to fix
families

11/23/2015
19
Learning Objectives
Learn about the LIFE
Team program
What disparities do you see
in your community?
Apply learnings to improve the
health of your
community
Conclusions
Questions?

11/23/2015
20
Break-Return 3:25P39
Brigid McCaw, MD, MPH, MS, FACP
Medical Director, Family Violence Prevention Program
Kaiser Permanente
December 2015
Transforming the Health Care Response to
Family Violence
#27FORUM

11/23/2015
21
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Objectives
� Learn about an innovative “systems model”
approach and quality improvement processes
that transformed a health care response to
family violence
� Learn about the critical role of linkages
between health care and community services
� Identify 2-3 opportunities to more effectively
address family violence in your setting.
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Ending family violence requires strong partnerships…
Religious
Leaders
Advocates Police
Employers
Health
Professionals
Educators
Friends
Policy Makers
Judges &
Legal
Professionals
…Healthcare has an essential role

11/23/2015
22
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Kaiser Permanente’s Innovative Model
https://youtu.be/uocoMbCg9N8

11/23/2015
23
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
1,0221,663
2,354 2,550 2,8753,466 3,285 3,432
4,036
5,148
6,173 6,2037,106
8,347
12,862
16,062
0
2,000
4,000
6,000
8,000
10,000
12,000
14,000
16,000
18,000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015*
Nu
mb
er
of
Mem
bers
wit
h IP
V D
iag
no
sis
Members Diagnosed with Intimate Partner Violence, 2000-2015*(Women and Men)
*Note: 2015 estimate is based on data from 10/1/14 through 9/30/15
KP Northern California:
Sixteen-fold Increase in IPV Identification
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
0
2,000
4,000
6,000
8,000
10,000
12,000
2000 2001 2002 2003 2004 2005 2006 2007 2008 2009 2010 2011 2012 2013 2014 2015*
Nu
mb
er
of
Mem
bers
wit
h IP
V D
iag
no
sis
*Note: 2015 estimate is based on data from 10/1/14 through 9/30/15
KP Northern California:
Most Identification Occurs in Ambulatory Care
Members Diagnosed with Intimate Partner Violence by Dept Type
2000-2015*
1,022
16,062
{
{
Emergency Dept. & Urgent Care
Mental Health
Primary Care

11/23/2015
24
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
How to transform a health care system’s response to family violence:
Clear goal: DV inquiry and intervention is part of everyday work
Thinking in new ways: Systems-Model Approach
Implementation and dissemination plan
Quality improvement measures
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Making the Case: Why is IPV an important
health care issue?
IPV is extremely common
The health effects are devastating
The health care costs are substantial
IPV impacts future generations
Health care interventions
make a difference

11/23/2015
25
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Affordable Care Act
Screening and counseling for interpersonal and
domestic violence included as part of women’s
preventive health services
Recommends universal screening
for childbearing-age women
IPV screening and counseling
should be core part of women’s
health servicesWomen’s Preventive Health Care Services Committee
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Comparison to other Important
Life-Threatening Conditions
that Affect Women
New cases of breast cancer[1] 211,000
Number of women dying from
cardiovascular disease[2]484,000
Women who are injured from IPV[3] 2,000,000
In the US, each year
1. Breast Cancer Facts & Figures. American Cancer Society: Atlanta, GA. 2005-2006.
2. Heart Disease and Stroke Statistics. American Heart Association: 2006.
3. Extent, Nature, and Consequences of Intimate Partner Violence. U.S. Department of Justice:
Washington, DC. NCJ 181867, 2000.

11/23/2015
26
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
IPV Associated with Many
Health Conditions
Most common cause of injury in women (18-44 yo)
� Headache, fatigue, insomnia, palpitations
� Chronic pain
� Depression, anxiety
� Obstetric and gynecologic conditions
� Poorly controlled chronic conditions
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
IPV and Chronic Health Problems
� 60% more likely to have asthma
� 70% more likely to have heart disease
� 80% more likely to have a stroke
� Twice as likely to be a current smoker
Center for Disease
Control (CDC)
Feb 2008

11/23/2015
27
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Impact on
Future Generations
� Children who witness DV
� May also be victims of abuse
� Higher rates of
� Depression, anxiety
� Substance abuse
� Failure in school
� Becoming victim or
perpetrator
help happens here.
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Intervention Makes a Difference!
Women who talked to their health care provider about the abuse
were nearly 4 times more likely to use an intervention
https://youtu.be/q2GDQMOGQ5E

11/23/2015
28
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Most women end violent relationships
� It takes time: on average 3-5
attempts and about 7 years
� The majority of women do not
have recurrent abusive
relationships
� Clinical intervention helps
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
How to transform a health care system’s response to family violence:
Clear goal: DV inquiry and intervention is part of everyday work
Thinking in new ways: Systems-Model Approach
Implementation and dissemination plan
Quality improvement measures

11/23/2015
29
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Inquiry and
Referral
Supportive
Environment
Leadershipand
Oversight
On-siteServices
Community
Linkages
Member and employee IPV education materials
Ongoing work to establish and promote community
resources
Electronic Medical Record Tools
Clinician training modules
Builds on existing resources in behavioral health, social services,
mental health
Referral Protocols
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Supportive EnvironmentAwareness and Information
What is it?
� Information: restrooms, exam rooms,
on-line, podcasts, health ed classes
� Posters: “Let us know, we can help”
� Reaching patients everywhere they
contact the health care system
� Engaged and informed workforce

11/23/2015
30
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Rooming Alone
Rooming alone allows
for private discussions
of sensitive issues,
including relationship
violence.
Supportive Environment
Privacy Posters
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Supportive EnvironmentEngaged and informed workforce
Stories of courage, survival, and hopekp.org/domestic violence

11/23/2015
31
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Must Address Clinician AND
Patient Concerns
The doctor:� How do I ask about IPV?
� What do I do when the answer is “yes”?
� How can I offer an intervention that is caring, effective, and efficient?
The patient:� If I disclose, what will happen?
� Will I be able to access the next set of resources I need?
� How will this benefit my health?
Inquiry and ReferralMust address patient AND clinician concerns
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Inquiry and Referral
What to do if the answer is “yes”?
Role of the clinician is clear and limited
� ASK
� AFFIRM
� ASSESS
� DOCUMENT
� REFER
“Making the right thing easier to do.”

11/23/2015
32
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Website easily accessible from EHR
Clinical Care Path
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Website easily accessible from EHR
Member Resources Available at Point of Care

11/23/2015
33
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
� Supporting clinicians:� Tools in electronic medical record
� Online clinician training
� Point-of-care online resources
� Engaging patients:� Online information for patients
� Advice Nurses in Call Center
� Apps: Circle of 6, 1 Love MyPlan
Inquiry and Referral
Using Technology to Improve Care
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Comments from a KP Physician
https://youtu.be/KHWCZsXI8Rc

11/23/2015
34
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Improvement in Member Satisfaction“How are things at home?”
0
10
20
30
40
50
60
70
80
90
100
18-34 35-44 45-64 65+
Asked about home life
Not asked
Percent of members rating satisfaction with physician as very good or
excellent (Member Patient Satisfaction Survey)
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
On-site IPV Response
� Triage for other mental health conditions
� Danger assessment
� Safety plan
� Support groups
� Referral to community resources
Social Services & Mental Health

11/23/2015
35
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Customize using local resources
� Local DV agency provides
� on-site advocate
� on-call response to hospital or clinic
� In house DV-trained staff collaborate w/ DV agency
� Private place to access help via phone or on-line
On-site IPV Response
Options for HOW to do this
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
What are they?
� DV advocacy
� 24-hour crisis response, safety planning
� Emergency shelter; transitional housing
�Other services: counseling, legal services, court advocacy
� National DV Hotline, Online Chat, Love is Respect Mobile Texting
� Family Justice Centers
Community Linkages

11/23/2015
36
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Family Justice Center Services
Counseling� Domestic violence and Sexual Assault counseling
� Safety planning
� Self-sufficiency program: computer skills, financial literacy, resume writing
and interviewing skills, ESL
Legal� Restraining orders
� Victims Compensation application assistance
Housing� Shelter and transitional housing assistance
Families� Parenting support
� Childcare while parent or guardian is receiving services onsite
Community LinkagesFamily Justice Center Services
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
How to transform a health care system’s response to family violence:
Clear goal: DV inquiry and intervention is part of everyday work
Implementation and dissemination plan
Thinking in new ways: Systems-Model Approach
Quality improvement measures

11/23/2015
37
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
KP Quality Improvement (QI) Measures
� Uses automated database
� Makes sense clinically
� Actionable
� Linked with national standard
National Committee for Quality Assurance (NCQA):
“QI 11 – Demonstration of a health program showing
continuity and coordination between medical and
behavioral health care.”
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Regional Identification Rate for IPV
5%7% 6% 7%
8%
10%
12% 11%
13%
16%
24%
28%
0%
5%
10%
15%
20%
25%
30%
Percent IPV+ Women Identified
Intimate Partner Violence Identification RateKPNC Women Age 18-652001-2015

11/23/2015
38
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Matching the Performance of the Best
54%
37%
31%28%
27% 26%
20% 19%
15%
0%
10%
20%
30%
40%
50%
60%
A B C REG D E F G H
Intimate Partner Violence Identification Rate
by Medical Center (KPNC Women Age 18-65)
10/1/14 through 9/30/15
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Culture Change
“No one is making you do anything you don’t want. I’m
just saying we’re all headed for Dodge City and we think
you should come along.”

11/23/2015
39
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
How to transform a health care system’s response to family violence:
Clear goal: DV inquiry and intervention is part of everyday work
Thinking in new ways: Systems-Model Approach
Implementation and dissemination plan
Quality improvement measures
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Rapidly Spreading What Works…
…and Sustaining It
� Infrastructure and sponsorship at each medical center
� Step-wise implementation
� Tools for implementation teams� Champion and Team roles
� Templates for referral pathway
� Clinician and patient education
� Regular communication with teams
� Quality improvement measures

11/23/2015
40
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Phases of Implementation
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Step-wise Implementation
Step 1� Form a local multi-disciplinary team with clinician champion
� Develop protocol for patients in urgent and non-urgent situations
� Identify community resources and develop partnerships
Step 2� Visible patient education materials
� Ensure that on-site services are in place
� Choose quality measures and annual goals
Stakeholder communication and engagement

11/23/2015
41
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Step-wise Implementation
Step 3� Clinician training- brief, frequent. Include tools and stories.
� Trend progress over time
� DV resources for employees
Step 4� Leadership training for champion and teams
� Link to other initiatives- electronic medical record, chronic conditions
� Sustain partnerships with community advocacy
� Highlight ‘promising practices’
Stakeholder communication and engagement
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Implementation of IPV Services Underway in Every KP Region
Northern California
Northwest
Southern California
Colorado Mid-Atlantic
Georgia
Hawaii

11/23/2015
42
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Transforming the Health Care
Response to Family Violence
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Transforming the Community
Response to Family Violence
Looking ahead to the next decade…

11/23/2015
43
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Contact Information
Brigid McCaw, MD, MS, MPH, FACPMedical Director, Family Violence Prevention Program
Kaiser Permanente
@BrigidMcCaw
kp.org/domesticviolence
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Appendix
11/23/2015
44
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Clinician Training Resources
How to Ask, How to Respond,
and How to Use HC Tools 14-min Online Training (2010)
Clinician Tipsheet“Communicating with Patients:
Intimate Partner Violence” (2012)
A Provider’s Handbook on
Culturally Competent CareChapter: “Intimate Partner Violence”
(2009)
Making a Difference6 min video (2013)
Abuse & Assault Link Video TipBrief Video Tour of Abuse and
Assault Website (2012)
Abuse and Assault Website Family Violence Prevention Program
Intranet Site
(2005-2014)
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
Descriptions of the
KP Systems-Model Approach
� "Using a Systems-Model Model approach to Improving IPV Services in a Large Health Care Organization". Institute of Medicine. 2011 http://www.iom.edu/Reports/2011/Preventing-Violence-Against-Women-and-Children-Workshop-Summary.aspx“
� “Developing a Health System Response to Intimate Partner Violence,” McCaw, B, and Kotz, K, Intimate Partner Violence: A Health-Based Perspective, C. Mitchell and D. Anglin ed., Oxford University Press 2009
� AHRQ Innovations Solution: “Family Violence Prevention Program significantly improves ability to identify and facilitate treatment for patients affected by domestic violence,” http://www.innovations.ahrq.gov/content.aspx?id=2343
� AHRQ Tool for Assessment of Health System Response http://www.ahrq.gov/research/domesticviol/
� Kaiser Permanente Domestic Violence website kp.org/domesticviolence

11/23/2015
45
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
KP Research Publications on DV
� “A Predictive Model to Help Identify Intimate Partner Violence Using Diagnoses and Phone Calls,” Barghava R, Temkin TL, Fireman BH, Eaton A, McCaw B, Kotz KJ, Amaral D. American Journal of Preventive Medicine, 2011.
� “Mental Health Service Referral and Utilization among Women Experiencing Intimate Partner Violence,” Ahmed A, McCaw B. Am J of Managed Care, 2010.
� “Intimate Partner Violence,” McCaw, B., A Provider’s Handbook on Culturally Competent Care: Women’s Health, Kaiser Permanente National Diversity Council and Office 2009
� “Domestic Violence and Abuse, Health Status, and Social Functioning,” McCaw B, Golding B, Farley, M, Minkoff J. Women and Health, 45(2), 2007.
� “Family Violence Prevention Program: Another Way to Save a Life,” McCaw B, Kotz K.The Permanente Journal 9(1), 2005.
� “Women Referred for On-site Domestic Violence Services in a Managed Care Organization,” McCaw B, Bauer H, Berman W, Mooney L, Holmberg M, Hunkeler E. Women and Health, 35(2-3), 2002.
� “Beyond Screening: A Systems Model Approach to Domestic Violence Services in a Managed Care Setting,” McCaw B, Berman B, Syme L, Hunkeler E. American Journal of Preventive Medicine, 21(3), 2001.
© 2015, The Permanente Medical Group, Inc. All rights reserved. Family Violence Prevention Program.
How Does This Apply To Me?P90
#27FORUM

11/23/2015
46
Thank You!
Links to online stories about these programs:
The LIFETeam: Breaking the Cycle of Violence Program
Translating care for substance abuse from the clinic to
the courtroom
Kaiser Permanente Domestic Violence Prevention
Program
Cory Sevin, RN, MSN
Director, IHI
P91


















