
Health Reform: Why, What, How … Liz Baxter May 18, 2013 [email protected].
38
-
Upload
mervyn-skinner -
Category
Documents
-
view
213 -
download
1
Transcript of Health Reform: Why, What, How … Liz Baxter May 18, 2013 [email protected].


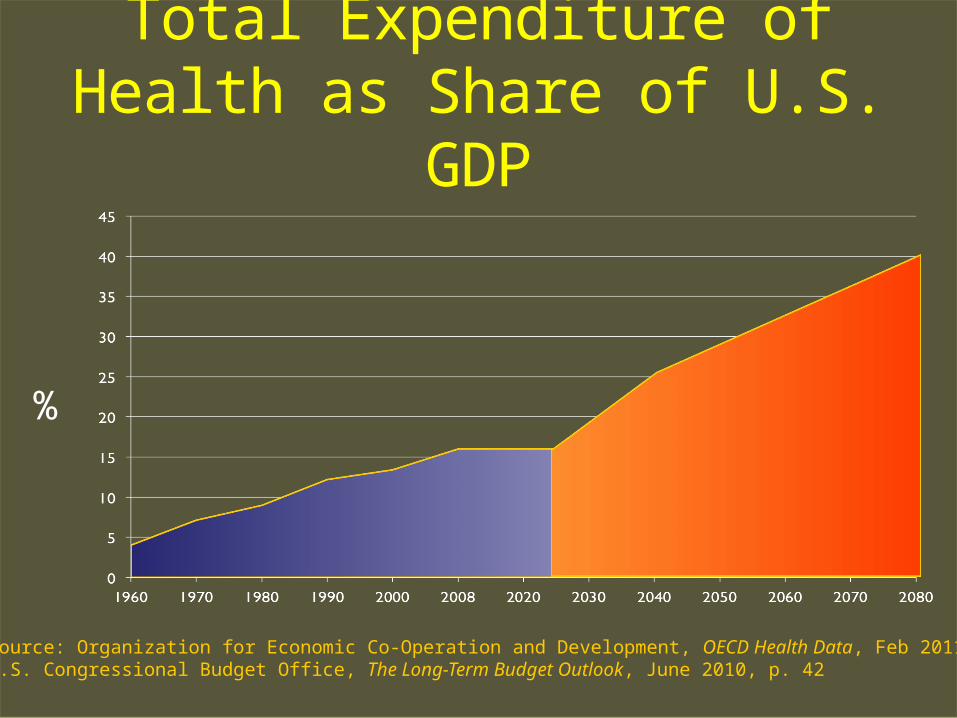
Total Expenditure of Health as Share of U.S. GDP
Current Projected
Source: Organization for Economic Co-Operation and Development, OECD Health Data, Feb 2011;U.S. Congressional Budget Office, The Long-Term Budget Outlook, June 2010, p. 42
%
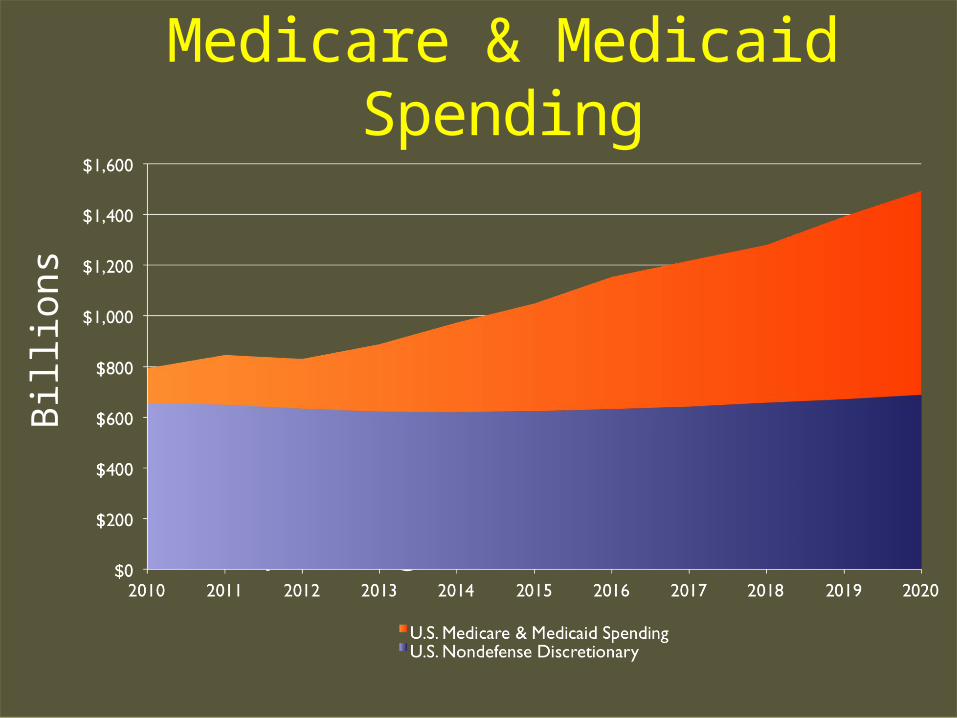
Medicare & Medicaid Spending
Medicare & Medicaid Spending
U.S. Nondefense Discretionary Spending
Bill
ion
s

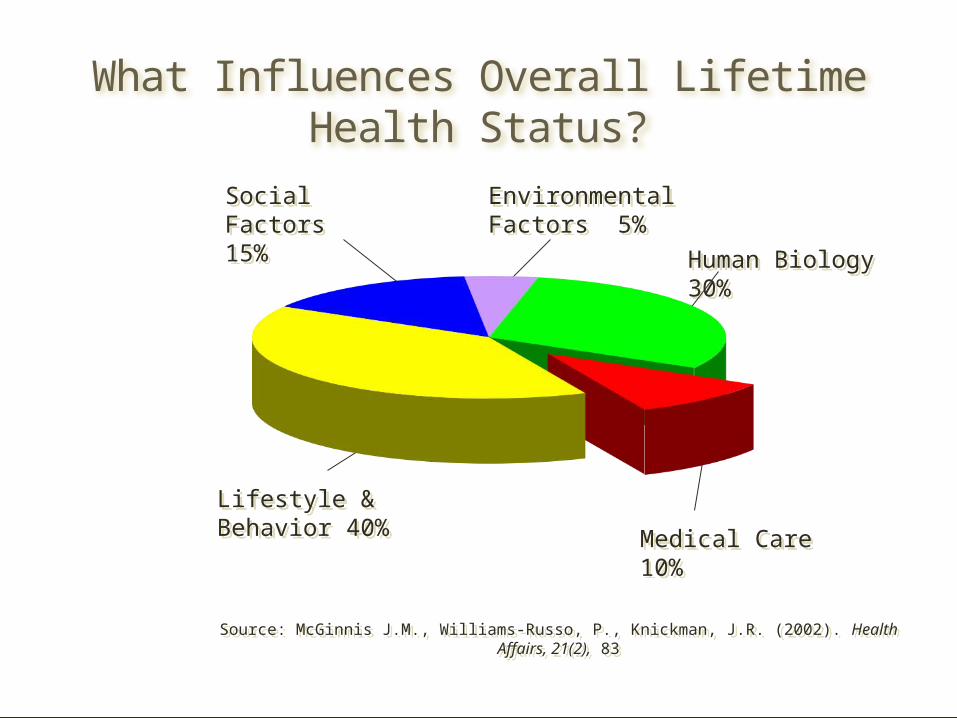
What Influences Overall Lifetime Health Status?
Source: McGinnis J.M., Williams-Russo, P., Knickman, J.R. (2002). Health Affairs, 21(2), 83
Source: McGinnis J.M., Williams-Russo, P., Knickman, J.R. (2002). Health Affairs, 21(2), 83
Lifestyle & Behavior 40%Lifestyle & Behavior 40%
Human Biology 30%Human Biology 30%
Medical Care 10%Medical Care 10%
EnvironmentalFactors 5%EnvironmentalFactors 5%
Social Factors 15%
Social Factors 15%
IJFALTIJ CABF RFFQPM
IJFALTIJ CABF RFFQPM
The Triple Aim①Improved Health②Lower Cost③Better Experience of Care
Traditional Approach to Balancing Budgets
• Cut reimbursement• Cut services• Cut people
Major Elements of Reform
• Expansion of Medicaid eligibility
• Delivery System Reform• Health Insurance Exchange
Medicaid Expansion
• Traditional Medicaid• State and federal
partnership• Oregon Health Plan• Raising Income Eligibility
Oregon Health Plan
50% of babies born in Oregon
16% of Oregonians
85% of Oregon providers
11% percent of total state budget
40% are people of color
23
OR: Changing How Care is Delivered
Coordinated Care Organizations (CCOs)
• Reduce waste• Accountable for health
outcomes• Local decision-making• Align financial incentives• Create fiscal sustainability• Reduce disparities• Better coordination of care
Health Insurance Exchange
• Created by OR Legislature in 2011
• Public Corporation• 9 member board of directors• State option under
Affordable Care Act• Cover Oregon
(coveroregon.com)
Mission of Cover Oregon
Improving the health of all Oregonians by providing health coverage options, increasing access to information, and fostering quality and value in the health care system
ONE HOUSE ONE DOOR
IndividualsandFamilies
SmallEmployers
PORTAL
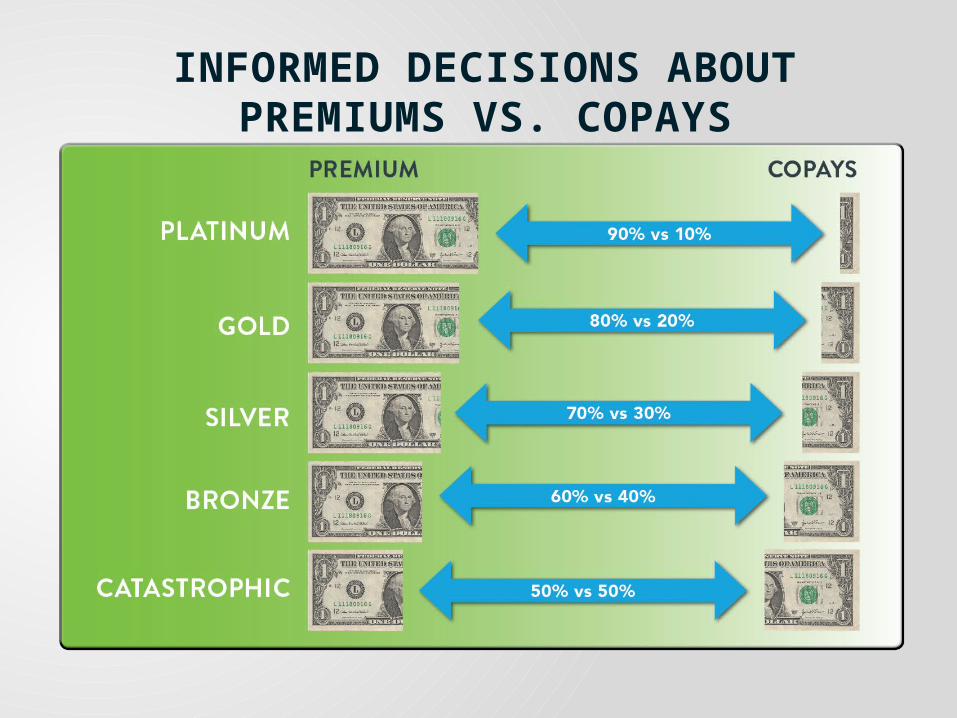
INFORMED DECISIONS ABOUT PREMIUMS VS. COPAYS
• No one can be denied, no lifetime limits
• Carriers must spend 80% of premiums on care
• Health plans held accountable for quality
• Essential health benefits: Ambulatory patient services
Emergency services
Hospitalization
Maternity and newborn care
Mental health and substance use disorder services, including behavioral health treatment
NEW HEALTH COVERAGE RULES
Prescription drugs
Rehabilitative and habilitative services and devices
Laboratory services
Preventive and wellness services, and chronic disease management
Pediatric services, including oral and vision care
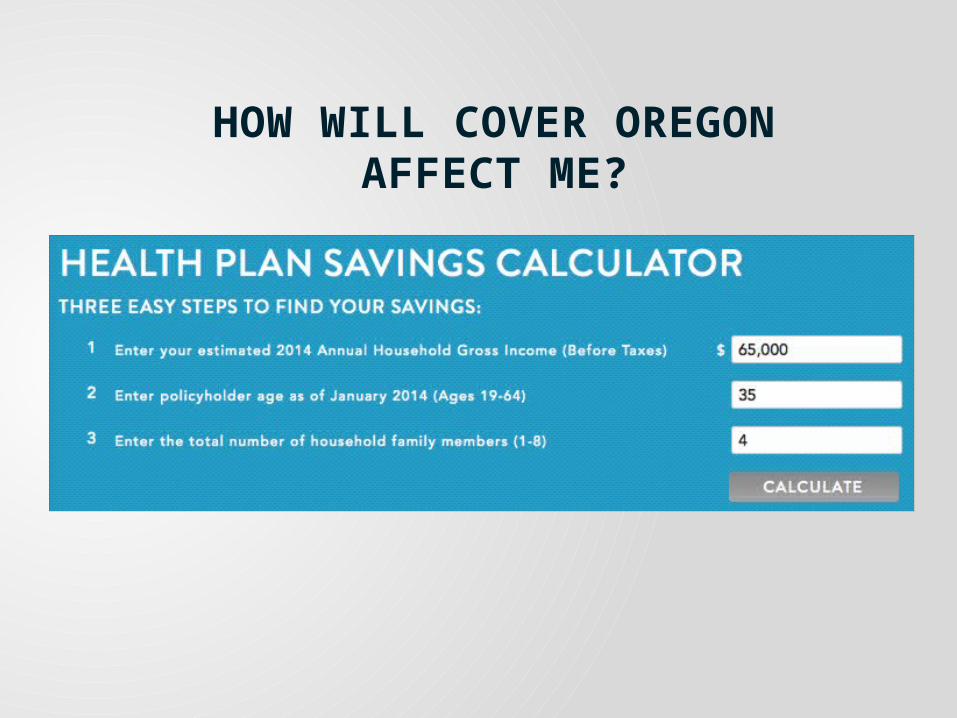
HOW WILL COVER OREGONAFFECT ME?
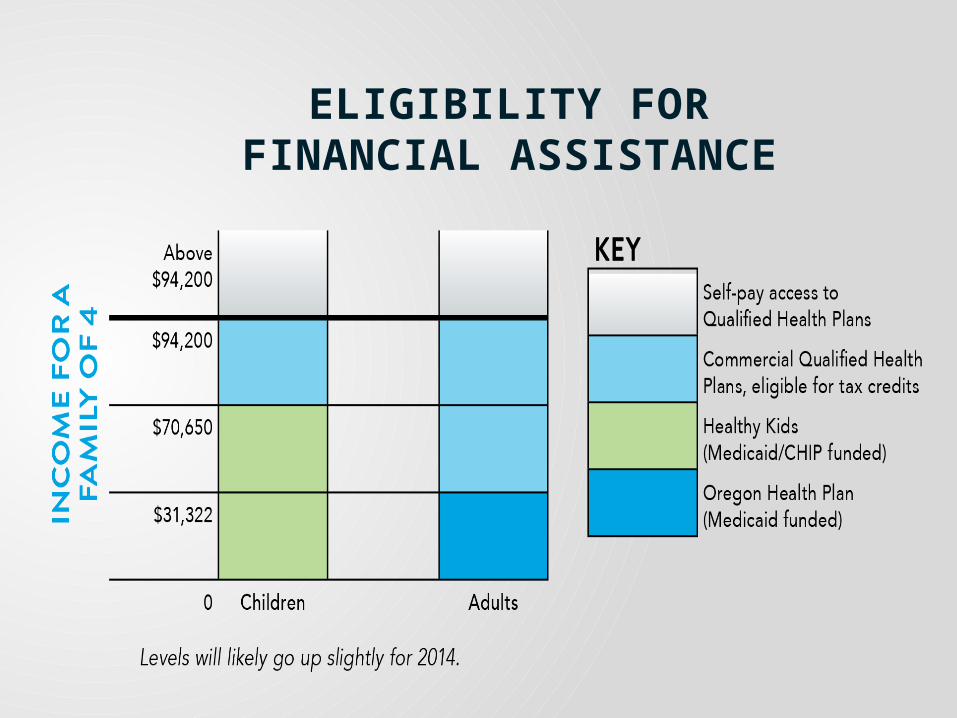
ELIGIBILITY FORFINANCIAL ASSISTANCE
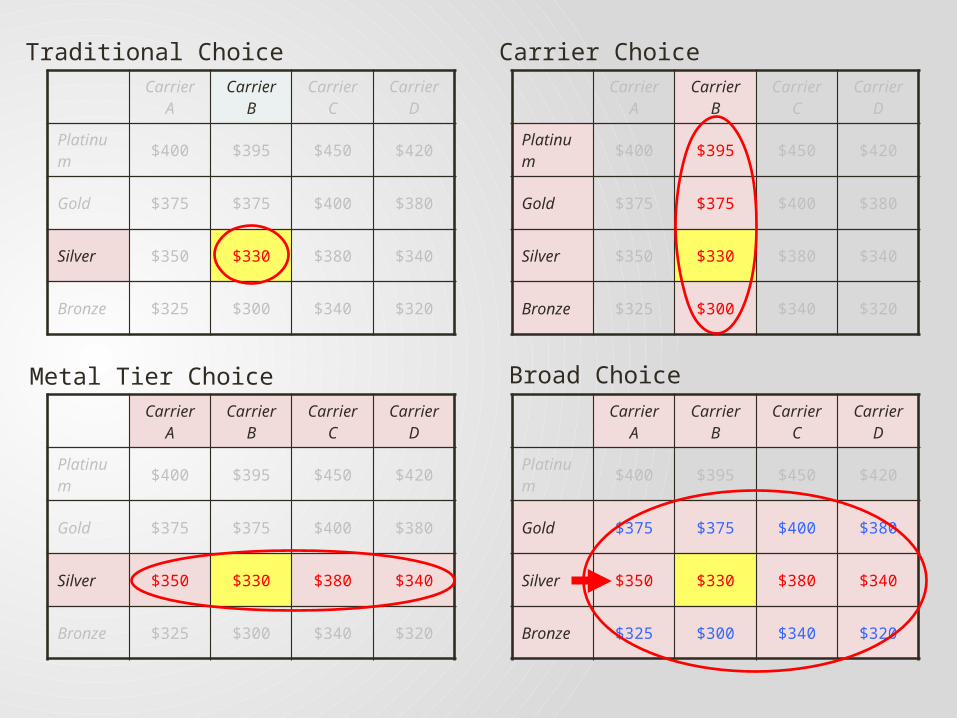
Carrier A
Carrier B
Carrier C
Carrier D
Platinum $400 $395 $450 $420
Gold $375 $375 $400 $380
Silver $350 $330 $380 $340
Bronze $325 $300 $340 $320
Carrier A
Carrier B
Carrier C
Carrier D
Platinum $400 $395 $450 $420
Gold $375 $375 $400 $380
Silver $350 $330 $380 $340
Bronze $325 $300 $340 $320
Carrier A
Carrier B
Carrier C
Carrier D
Platinum $400 $395 $450 $420
Gold $375 $375 $400 $380
Silver $350 $330 $380 $340
Bronze $325 $300 $340 $320
Carrier A
Carrier B
Carrier C
Carrier D
Platinum $400 $395 $450 $420
Gold $375 $375 $400 $380
Silver $350 $330 $380 $340
Bronze $325 $300 $340 $320
Traditional Choice Carrier Choice
Metal Tier Choice Broad Choice
LONG-TERMVISION
• Larger employers
• Additional products
• Coordinated care models
• Quality and value
• Buying power
The doctor of the future will give no medicine, but will interest her or his patients in the care of the human frame, in a proper diet, and in the cause and prevention of disease.
--Thomas Alva Edison


Thank You
• [email protected]• Healthreform.kff.org• Health.Oregon.gov• Oregon.gov/oha/oei/• CoverOregon.com











![FOR THE DISTRICT OF NEW JERSEY BAXTER … THE DISTRICT OF NEW JERSEY BAXTER HEALTHCARE CORPORATION, BAXTER INTERNATIONAL INC., and ... 1684.] 4 Although Baxter purports to seek construction](https://static.fdocuments.in/doc/165x107/5b0a073a7f8b9aba628b8749/for-the-district-of-new-jersey-baxter-the-district-of-new-jersey-baxter-healthcare.jpg)




