Health Protection Stocktake IFF Meeting 20April2011
18
Health Protection Stocktake Workshop Engaging a Changing World 20 April 2011, Victoria Quay, Edinburgh, 10.00 – 16.00 Introduction and Summary This is the record of an all day workshop held at Victoria Quay on 20 April 2011 for the Health Protection Stocktake Group with support from a range of officials working on Scottish resilience. The day was designed and facilitated by International Futures Forum (a non- profit specialising in tackling complex, messy problems in business, government and communities). Using the IFF World Model, participants spent the first half of the day considering health protection in Scotland in the context of a fast-changing, interconnected world. The second part of the day assessed the implications for health protection in the short and long term. The day generated three substantial pieces of content to feed in to the Stocktake. The first session identified possible health protection issues for Scotland resulting from current global trends and discontinuities. The next moved to take a systemic view of health protection and identified possible sources of brittleness or vulnerability in the present system and also ideas for building greater resilience. The final session was organised around the themes of ‘community skills’, ‘widening the scope of health protection’ and ‘designing flexible resilient health protection’ that had emerged from the morning session. It identified a range of measures to take to fix what is not working, to innovate for improvement, and a set of long term principles to guide the evolution of the health protection system to make it more flexible and resilient in the future. Welcome Margaret Hannah, NHS Fife, welcomed participants and performed introductions, including Tony Hodgson and Graham Leicester from International Futures Forum . A full list of participants is included in the Appendix. Graham Leicester explained that the purpose of the workshop was to allow the Health Protection Stocktake Group to expose their emerging thinking to what we know about a fast- changing, interconnected world. This would involve using the IFF world model as a framework. Broadly speaking the morning would be given over to engaging with the world, and the afternoon to considering the practical implications for a more robust health protection strategy.
-
Upload
roanne-dods -
Category
Documents
-
view
216 -
download
0
description
Introduction and Summary This is the record of an all day workshop held at Victoria Quay on 20 April 2011 for the Health Protection Stocktake Group with support from a range of officials working on Scottish resilience. The day was designed and facilitated by International Futures Forum (a non- profit specialising in tackling complex, messy problems in business, government and communities). 20 April 2011, Victoria Quay, Edinburgh, 10.00 – 16.00
Transcript of Health Protection Stocktake IFF Meeting 20April2011

Health Protection Stocktake Workshop Engaging a Changing World
20 April 2011, Victoria Quay, Edinburgh, 10.00 – 16.00
Introduction and Summary This is the record of an all day workshop held at Victoria Quay on 20 April 2011 for the Health Protection Stocktake Group with support from a range of officials working on Scottish resilience. The day was designed and facilitated by International Futures Forum (a non-profit specialising in tackling complex, messy problems in business, government and communities). Using the IFF World Model, participants spent the first half of the day considering health protection in Scotland in the context of a fast-changing, interconnected world. The second part of the day assessed the implications for health protection in the short and long term. The day generated three substantial pieces of content to feed in to the Stocktake. The first session identified possible health protection issues for Scotland resulting from current global trends and discontinuities. The next moved to take a systemic view of health protection and identified possible sources of brittleness or vulnerability in the present system and also ideas for building greater resilience. The final session was organised around the themes of ‘community skills’, ‘widening the scope of health protection’ and ‘designing flexible resilient health protection’ that had emerged from the morning session. It identified a range of measures to take to fix what is not working, to innovate for improvement, and a set of long term principles to guide the evolution of the health protection system to make it more flexible and resilient in the future. Welcome Margaret Hannah, NHS Fife, welcomed participants and performed introductions, including Tony Hodgson and Graham Leicester from International Futures Forum. A full list of participants is included in the Appendix. Graham Leicester explained that the purpose of the workshop was to allow the Health Protection Stocktake Group to expose their emerging thinking to what we know about a fast-changing, interconnected world. This would involve using the IFF world model as a framework. Broadly speaking the morning would be given over to engaging with the world, and the afternoon to considering the practical implications for a more robust health protection strategy.
2
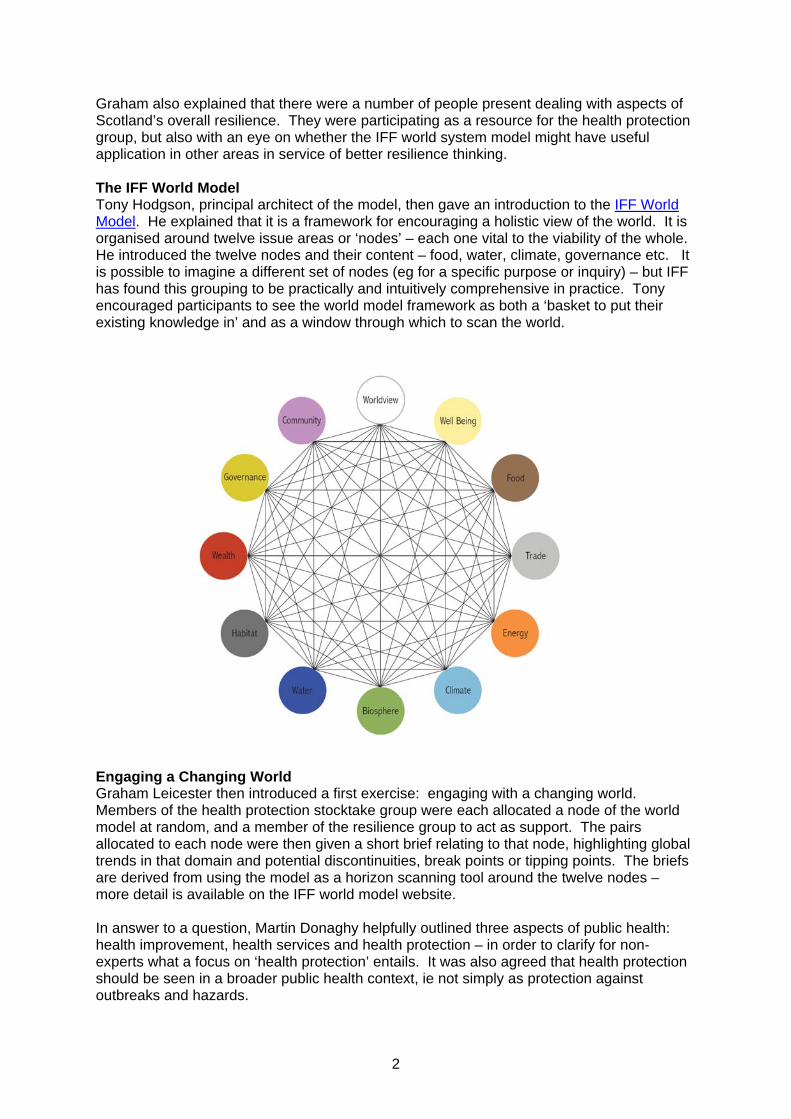
Graham also explained that there were a number of people present dealing with aspects of Scotland’s overall resilience. They were participating as a resource for the health protection group, but also with an eye on whether the IFF world system model might have useful application in other areas in service of better resilience thinking. The IFF World Model Tony Hodgson, principal architect of the model, then gave an introduction to the IFF World Model. He explained that it is a framework for encouraging a holistic view of the world. It is organised around twelve issue areas or ‘nodes’ – each one vital to the viability of the whole. He introduced the twelve nodes and their content – food, water, climate, governance etc. It is possible to imagine a different set of nodes (eg for a specific purpose or inquiry) – but IFF has found this grouping to be practically and intuitively comprehensive in practice. Tony encouraged participants to see the world model framework as both a ‘basket to put their existing knowledge in’ and as a window through which to scan the world.
Engaging a Changing World Graham Leicester then introduced a first exercise: engaging with a changing world. Members of the health protection stocktake group were each allocated a node of the world model at random, and a member of the resilience group to act as support. The pairs allocated to each node were then given a short brief relating to that node, highlighting global trends in that domain and potential discontinuities, break points or tipping points. The briefs are derived from using the model as a horizon scanning tool around the twelve nodes – more detail is available on the IFF world model website. In answer to a question, Martin Donaghy helpfully outlined three aspects of public health: health improvement, health services and health protection – in order to clarify for non-experts what a focus on ‘health protection’ entails. It was also agreed that health protection should be seen in a broader public health context, ie not simply as protection against outbreaks and hazards.

3
To perform an initial scan, each pair assigned to an individual node was invited to study the brief and then identify for their node:
‐ Worrying developments in the global situation ‐ How these might show up in Scotland ‐ Most pressing health protection concern (bearing in mind the public health
context)
Each pair then fed back their answers on these points to paint a rich picture of the emerging global situation, the ways in which that might impact Scotland, and the health protection implications. The results were captured on a series of hexagons and mapped on to the world model – so as to provide a visual rich picture (see below). Water Global: Demand outstrips supply. Leading to mass migration, civil unrest and war, famine, inequality – loss of capacity to export from some nations. Scotland: Migration increases along with the level of demand in the population. Exploitation of scarce water: private supplies, rackets. Rising inequalities and social unrest. Health Protection: Migrant population bring in and suffer from disease. Flooding leads to disease. Poor water quality: need to use treated water? General hygiene suffers. Wealth Global: the £ and the € are not stable, and there is no stable reserve currency. Pursuit of wealth leads to deforestation, over-fishing etc. Possible Japanese slump? And an economic system that is ungovernable. Scotland: Dependency on financial services impacts wealth as these fail. Rising inequalities. Less money for NHS. Health Protection: Lack of resources for NHS, vaccines etc. Less attention to health and safety issues, clean cars, clean industry in a cost-cutting environment. ‘Risk society’ ready to take more risks because outlook is bleak anyway. Planning more difficult.

4
Energy Global: Fossil fuels running out, but demand growing. Higher risk of resource wars and conflicts in developing world. Scotland: Long term dependence on fossil fuel. But switch to renewables should be good for Scotland. Even so, big issues re transport and remote communities. Health Protection: Need to risk assess new energy sources. Be aware of potential knock on impacts of damage to energy infrastructure. Worldview Global: Religious and political conflicts. Islam vs Christianity, Fossil vs Nuclear, Dictators vs Democracy. Scotland: Terrorist events. Riots, more crime. Media coverage interprets and amplifies beyond the ‘facts’. Loss of trust across society. The 6 Ds: death, disease, disorder, dissatisfaction, destitution, discomfort. Health Protection: Should we prepare for the worst case or the most likely? Prepare for CBRN vs chemical release, emergent infection. How to think about HP: Direct/Indirect impact; Expected/ Unexpected; Affordable/ Unaffordable.. Climate Global: Abrupt discontinuity of some sort. Scotland: Extreme water events impact availability of drinking water. Heatwaves more frequent. Health Protection: Infectious diseases associated with water shortages. More immigration. HP function needs to stay good: against vector, food borne and imported infection. Governance Global: Terrorism. Breakdown of effective governance. Revolutions. National governments less powerful. Scotland: Increased migration. Disruption of essential supplies. Terrorism. More infections from abroad. Health Protection: More CBRN incidents. Inability to respond across communities. Too many balls to keep an eye on: we may be surprised. Community Global: Cultural homogenisation blurring communities. Rising inequality and tension. Scotland: Poor uptake of services from marginalised communities. Public health education more difficult, eg re self-help and resilience. Health Protection: Difficult to identify people – eg not registered with GP. There will be new biohazards emerging. Doctors need to be trained for these challenges. Wellbeing Global: Costs of closing the gaps: between wealth and wellbeing and between rich and poor. Scotland: Affluenza – stress, long hours of work. More crime because of rising inequality. Health Protection: Physical and mental health impacts of dissatisfaction. Changing demographic exposes population to different risks. Biosphere Global: Land transformation. No time for regeneration. Supply not meeting demand. Wealthy countries have too large a footprint. Scotland: Greater connectivity with global events. Dependence on goods depleting ecosystems in other countries. Scotland becomes a nation of gardeners. Health Protection: Water contamination. Food chain contamination. Air quality falls. Public experience increased ‘perceived risk’.
5
Food Global: Food shortages and obesity: twin trends. Distribution an issue. Use of GM foods and intensive farming increase. Scotland: Large scale migration from depleted areas. Change in land use. Health Protection: Impacts of migration – rising HIV, TB, pressure on services. More waste to take care of. Zoonoses (animal diseases spread to humans). Trade Global: More migration from south to north. Increased illegal drugs trade. Vulnerability in supplies. Biotech trade raises ethical issues. Movement of people to find jobs. Scotland: More inward migrants and mobile population. Drugs more available, and feeding on poverty. Discontinuities of supply. Increased costs for intervention raising ethical issues. Health Protection: HIV, TB increase. ‘Under the radar people’ makes surveillance difficult. Contamination of drugs and other goods. Increased demand for services we can’t supply. Greater need to collaborate with eg World Health Organisation and European Centre for Disease Control. Habitat Global: Population outstripping infrastructure around the world (in urban areas). Scotland: Edinburgh and Glasgow become slum cities. Health Protection: Lose capacity for surveillance in dense cities. Resurgent diseases – TB, diphtheria. Synchronous Failure After a short break the group regathered for a second exercise. Tony explained that the world model is not only about the nodes, but also about the connections between them. Every node is connected to every other node – in other words, developments in one part of the world system inevitably have consequences in other parts. Troubles do not come singly. In a tightly coupled interconnected world there is a high risk of what the Canadian security analyst Thomas Homer-Dixon calls ‘synchronous failure’. Any event can trigger a cascade of consequential events: as recently in Japan with the earthquake, tsunami and nuclear incident. Or a major disease outbreak might coincide with energy shortages or extreme weather or a financial crash, for example. Graham explained that the next exercise would begin to move into a deeper engagement with a fast-changing, interconnected world. Four groups of three nodes had been selected producing just four snapshots out of a much greater range of permutations of plausible worlds of synchronous failure in which the concerns voiced for individual nodes in the first exercise now occur together. He invited the pairs responsible for each node to team up in small groups as follows:
‐ community, water, biosphere ‐ trade, food, habitat ‐ water, wealth, energy ‐ governance, worldview, climate
At this stage each group was also given briefings on these three nodes that mirrored the earlier briefs on global trends and discontinuities but prepared (by experts within and without government, compiled by the resilience team) especially for Scotland. The task for each group was to imagine themselves into this world of synchronous failure in Scotland and to start to consider the implications for health protection.

6
Brittleness and Resilience Once the groups had begun to inhabit these plausible but challenging future worlds, Tony introduced a short presentation on brittleness and resilience. A resilient system is able to flex under challenge and ‘bounce back’. The opposite is a ‘brittle’ system. Brittleness becomes exposed when:
‐ Disruption occurs in highly interconnected infrastructure ‐ “just in time” becomes “right out of stuff” ‐ Emergency services become the biggest emergency ‐ People expect “the authorities” to fix the impossible ‐ Society rapidly runs out of options
Growth and efficiency alone can often lead ecological systems, businesses and societies into fragile rigidities, exposing them to turbulent transformation. And the ways in which we tend to run our system, for economic efficiency, tend to make the system overall less resilient. The ‘resilience premium’, the slack in the system needed to cope with uncertainty and challenge, is too often taken as profit.
On the other hand, a resilient system has the following characteristics (which can be explored in more detail eg at www.resalliance.org ):
‐ the ability to absorb disturbances ‐ to be changed and then to re-organise and still have the same identity ‐ the ability to learn from the disturbance ‐ resilience shifts attention from purely growth and efficiency to needed recovery
and flexibility

7
Following this introduction, each group was encouraged to consider two questions in the context of the challenging worlds they had started to imagine in Scotland’s future:
‐ What brittleness might these challenges reveal in the Health Protection system?
‐ What are the implications for building a more resilient Health Protection
capacity? Potential Brittleness in Health Protection Systems In view of the challenges a changing world might pose for the health protection system in Scotland, the group identified the following potential weaknesses or vulnerabilities in the current system:
‐ Pandemics – planning doesn’t match risk o Unpredictability o Overreacting, vaccines, stockpiling
‐ Perception vs reality: self diagnosis, ‘informed public’, difficult to manage perceived risk
o eg air pollution in suburban areas
‐ Affluence increases air pollution with a disproportionate effect on different parts of the country
‐ Some areas of Scotland developing increasing problems not accommodated in
existing NHS structures or funding patterns
‐ Added urban problems due to fragility of infrastructure eg water and sewage
‐ ‘Learned helplessness’ – culture of dependency
‐ Need to monitor environmental activity from a public health perspective – may be dropped due to resource constraints
‐ Food borne disease etc caused by food miles etc
‐ Strain on numbers and staff
‐ Intelligence gathering and analysis is patchy, eg migration, energy, wealth
‐ Too narrow in our concept of Health Protection
‐ Balance between prevention and reaction?
‐ Interruption of supplies, services
‐ Responding to increased demands nationally and in many localities
‐ Capacity under strain: people, money, medicines, communications infrastructure
(IT), transport
‐ No mutual aid?

8
‐ Less capacity for command and control
‐ Inadequate (differential) response to varied patterns
Building Resilience in Health Protection Systems In view of the potential brittleness of the system, the group identified the following as areas in which to build the resilience of the health protection system:
‐ Broaden range of issues for planning to include those outwith control of HP
‐ Consider how best to ramp up for emergencies
‐ Cost of resilience: resources, staff etc. Need to balance with routine activity ie prevention
‐ Flexibility of response
‐ Specialist workforce vs wider public health workforce
‐ Address reputational risk so that advice is followed: eg lack of take up of MMR,
swine flu vaccine in pregnant women
‐ National level agreement on priorities and a different resource split to support it
‐ Building community resilience and protection
‐ Gap between health protection and health improvement should be addressed: more cohesion/ integrated approach to resources.
o eg food miles – food borne disease – obesity links, and environmental impacts on health
‐ Expand staffing base eg use existing resource differently with the inclusion and
coordination of voluntary sector
‐ Adopt wider lenses – horizon scanning
‐ Develop workforce skills (multi-skilling)
‐ Pool resources, multi-agency collaboration
‐ Practise the 4 C’s: command, control, coordination, communication
‐ More money
‐ Trained people – locally deployed
‐ Resilient structures
‐ Resilient communities (which are already changing, eg generational shifts, self help culture)
‐ Scottish identity

9
‐ Access external support (UK, EU) Advice for Health Protection from the Future Graham explained that the whole morning had been an exercise in immersing the group in a variety of plausible but challenging futures, all based on a fast-changing global context that will inevitably impact Scotland. First the group had explored this on the basis of individual nodes, then combinations threatening synchronous failure. This is not to say that these scenarios will happen – but all are based on existing phenomena in the world today… so they are at least plausible. In effect the morning had been a journey into the future. And in order to gain as much insight as possible from the journey before returning to the present (after lunch) Graham invited everyone as individuals to reflect on their experience and to write a single piece of new advice to the Health Protection Stocktake Group dealing with these issues in 2011 – ie not something they knew before taking the journey, but an insight gained from contemplating the future. ‘Knowing what you now know’, he suggested, ‘what single piece of new advice would you give a group working on these issues today?’ Everybody then posted their advice on a hexagon on the wall before leaving for lunch. Identifying Themes for Further Exploration After lunch Tony explained how he and the facilitation team had clustered the pieces of advice into seven broad thematic groups, as follows: 1. Community Preventive and Rebound Capacity
‐ Don’t rely on the centre, enable the local to respond ‐ Skilled local personnel remain very important ‐ Develop local community support and response to health protection threats
2. Positive Resilience
‐ Keep calm, smile a lot, keep an open mind, be flexible ‐ It is not personal even if it feels like it is! ‐ It might never happen! ‐ It’s not all about disaster: imagine the positive
3. Be Able to Act
‐ 4 C’s: command, control, coordination, communication. Works in any discipline ‐ Sometimes we just need to get on with it and deal with what we can

10
4. Health Protection in a Wider Context
‐ Need to have expanded view of health protection and its implications, ie not just ‘medical’ issues to be considered
‐ Don’t forget wider implications – ie not just health protection ‐ Think of local health protection in a global context ‐ Think wider than own organisation
5. Inclusive Resource Planning
‐ Think multi-agency. Non-health people have an input ‐ Enhanced HPS workforce: flexibility, capacity ‐ Think about how to use all our collective resources ‐ Establish a health protection strategy group involving all HP stakeholders to identify:
HP provision and needs (met and unmet and where we are now); aims (where we want to get to); actions (how to get there); taking into account Scotland-wide skills and resources and local variation in community/partner expectations and service delivery. Done on an annual basis and limited to 5 pages
6. Flexibility Designed In
‐ You can’t solve every issue. Don’t try planning for everything ‐ Flexibility of systems, people ‐ Plan for flexibility ‐ Integrated, flexible approach ‐ Ensure resource flexibility
7. Towards a New Level of Health Protection Resilience
‐ Health depends on society working well: influence economic and political issues, don’t look inwards any more
‐ Revisit and exploit the joint nature of public health: improvement increases protection increases improvement etc
‐ Learn what we can from countries beyond Europe about future health risks ‐ Impacts will be greatest on the have nots – could be huge health inequalities issue,
so prevention measures, helping people to help themselves, essential Following discussion these were grouped together into three overall themes to be explored: Community Skills
‐ Community Preventive and Rebound Capacity ‐ Positive Resilience ‐ Be Able to Act
Widening the Scope of Health Protection
‐ Health Protection in a Wider Context ‐ Inclusive Resource Planning
Designing Flexible Resilient Health Protection
‐ Flexibility Designed In ‐ Towards a New Level of Health Protection Resilience
Three groups formed around these themes, with individuals joining whichever group now included their piece of pre-lunch advice. Each group was invited to think about how to improve health protection in relation to their specific theme and to address three perspectives on ‘improvement’:
11
‐ What needs fixing? ‐ What needs innovating? ‐ What long term principles should guide us?
Feedback The three groups generated a large number of suggestions for improvement based on these three perspectives and recorded their ideas on flipcharts as follows: Community Skills Needs Fixing:
‐ Rigidity of structures ‐ Community education (Councillors, decision-makers) ‐ Links between different agencies/ offices (drawing on whole organisation)
Needs Innovating:
‐ Mechanisms – formal and informal - for introducing additional players (eg voluntary sector)
‐ Effective (skilled) mutual aid ‐ Robust escalation processes (agreed criteria)
Long Term Principles
‐ Public Health Act: joint planning ‐ Cooperative environment ‐ Shared values: honesty, mutual respect ‐ Learning from experience: organisational memory, telling the story ‐ Balancing experience, science, evidence and judgement ‐ Effective communications (new media)
Widening the Scope of Health Protection Needs Fixing:
‐ Too inward looking ‐ Is the title wrong? Narrow focus on health hazards? ‐ Lack of flexibility, too focussed ‐ Better understanding needed of how global influences affect local delivery ‐ Tension between national and local ‐ Academic endeavours underpinning health protection activity ‐ Links with Health Protection Agency, eg on chemical and radiation
Needs Innovating:
‐ Insist on joint working in planning/ response/ exercises and training ‐ Address balance of care in health service and partners (both nationally and locally,
including multi-skilling) ‐ Make sure academic endeavour is applied
Long Term Principles:
‐ Common goals: health protection seen as part of a wider whole ‐ Collaboration ‐ Don’t let structures get in the way ‐ Establish common principles and standards, including about responsibility ‐ Have regard to UK context ‐ Appreciation of capabilities and role responsibilities

12
Designing Flexible Resilient Health Protection Needs Fixing:
‐ Capacity: maximising this in event of an incident. ‐ Health protection vs health improvement balance. ‐ Health protection staff in boards are thin on the ground
Needs Innovating:
‐ Expanding mutual aid: internally and internationally ‐ Raise visibility of health protection ‐ Centralised HP or regional boards? – need integrated approach to resources, use of
voluntary sector (eg meningitis trust) including for public communication ‐ Exploring more external resources ‐ Increase secondments: cross pollination (eg for a month), international exchanges ‐ IT systems should be fit for purpose: lose the compatibility issues, make them
functional ‐ Training issues: cross-functional coaching and mentoring ‐ Review how funding is allocated, ie not just by head of population ‐ Make greater use of health improvement agenda to support health protection issues
Long Term Principles:
‐ Consistent set of standards across Scotland ‐ Don’t limit horizons ‐ Practice in benign times what you would do in a crisis eg international exchange ‐ Think global act local
A Strategic View: Three Horizons of Health Protection Finally, rather than have a simple round of each group’s work, Tony presented the ‘three horizons’ framework for thinking about longer term strategic change (see IFF website for more detail). He explained that the first horizon is business as usual, the dominant system – under pressure as the world changes. The second horizon is about innovation, reacting to changes in the world in order to keep business as usual running or to improve it. The third horizon is more visionary – and eventually comes through over time to provide the new ‘business as usual’, much better suited to a very different world. See the graphic below.
increasing synchronous
failure
Increasing challenge to ‘bounce back’
Radically n
ew ideas
with bett
er fit to ne
w
environm
ent new context for
proven policies
new capacities to
absorb shocks and bounce
back
new resilience paradigm
innovation in
health
protection
strategies
FUTURE
THE TURBULENT TRANSITION
HORIZON 1
HORIZON 2
HORIZON 3
HEALTH
NOW
radically different operating
environment
increasing synchronous
failure
Increasing challenge to ‘bounce back’
Radically n
ew ideas
with bett
er fit to ne
w
environm
ent new context for
proven policies
new capacities to
absorb shocks and bounce
back
new resilience paradigm
innovation in
health
protection
strategies
FUTURE
THE TURBULENT TRANSITION
HORIZON 1
HORIZON 2
HORIZON 3
HEALTH
NOW
radically different operating
environment
13
In some ways the three questions posed to the groups, about what needs fixing, what needs innovating and long term principles, were hinting at this three horizons framework. And so the final act of the day was to take feedback from the group as a whole mapped on to the three horizons. The intention is to make visible a broad strategy: what needs to be done now to ‘keep the plane in the air’, what are the principles that should guide long term development and direction, and what is the nature of the innovations needed in the transition between the first and third horizons. Broadly feeding back in reverse order – starting with long term principles, then innovations, and finally things that need fixing – the following comments were made by members of the group. These were also captured in headlines and mapped on to the three horizons framework as shown below (see also the full page version in the appendix).
‐ We need to continue to learn from experience, preserve the organisational memory etc. But that does not mean just recording the science alone: that must be balanced by judgement and experience. This is a long term principle, not respected as much as it should be today.
‐ We would like to see a consistent set of standards across Scotland. At the moment
there is a lot of difference between Board areas. But who should establish the standards? And can we leave room for local flexibility once they are established?
‐ We talked about having equity of outcome across Scotland.
‐ The danger is that we just modify the edges of what we do now. We need to keep an
eye on the emergent future, and the way the world is changing.
‐ Our take on ‘consistency’, from a group with more of a focus on localism, was more about agreeing shared values rather than overarching systems. That would leave more room for local autonomy.
‐ The difference between major incidents and run of the mill public health events is
often difficult to articulate and escalation processes are confused. It would be good to have a set of clear criteria for that.
‐ The public health act requires joint health protection plans. So the more inclusive
framework is already there. But at the moment this is more of a ‘cobbling together’ of existing information rather than anything fundamentally new. Some are finding the guidance constraining, ticking some boxes, rather than encouraging a new, more creative, locally autonomous process [the author of the guidance pointed out that this was precisely what it had intended – but probably needed to be more about process than content]. There needs to be some innovation in the way we use guidance so that it is more about enabling the future than satisfying the reporting demands of the first horizon.
‐ This relates to the broadening of the scope of health protection. There is a crossover
between health protection and health improvement. We need to expand our definition of ‘health protection’.
‐ Mutual aid is a big issue. There is a lot of talk about it, but it is not effectively utilised
across the country. The island boards are more used to receiving support from the mainland. We should also consider this across the pathway of care, even within a board area. And to look beyond Scotland: there is mutual aid to be had from the international arena. But there is a general unwillingness to ask for help, or to admit to the need for help. It would help for relationships to be established before the need

14
and before a crisis: short secondments, establish relationships, run exercises etc. It is much easier to pick up existing relationships than establish them in a crisis. And it is possible to practice mutual aid by giving it rather than receiving it.
‐ Mutuality seems to be coming through as a principle at all levels. And it should not
be confined to health.
‐ There is a cost involved in establishing relationships, mutual aid etc. None of this will be easy in a climate of big cuts.
‐ The principles of cooperation and coordination work for the SCGs and should apply
across the whole system.
‐ We need to pay more attention to social media and the way communities use it to share information. We need to become more savvy in social media use as responders.
‐ There needs to be a renewed commitment to national issues and the national
situation. We have moved towards board level autonomy and thinking.
‐ The culture in the NHS suggests that it is a sign of weakness to ask for help. We need to get over that for a resilient future. Insisting on joint working at all stages – planning, resourcing, exercises etc is a way to tackle that. And the question of capacity is a standing agenda item in SCGs.
‐ There is a need for academic respectability and intellectual endeavour around these
issues. There are always plenty of reasons for not changing. We need to build the evidence base for something beyond incrementalism.

15
‐ There is a tendency to revert to the mean. What needs fixing is to free ourselves from the principle that ‘it’s always been that way’.
‐ IT systems need improving, so that they are compatible.
‐ Soften the boundaries between Health Protection Scotland and the Boards,
interchange between the two etc. Could be done quickly. Don’t assume that ‘everything national is HPS, everything local is for the Boards’. We need parity of esteem… and no assumption that the expert on a national issue is necessarily in a national institution. Understand that there is a human system too, and run it that way.
Final Reflections Once the larger three horizons picture had emerged, Graham Leicester offered some brief observations on the whole. He suggested that the picture showed a clear shift from the first to the third horizon away from rigid centralised structures towards a more flexible system, enabling governance, sharing of resources, blurring of organisational boundaries. That will release the human system that lurks inside the institutional one. The real practice of mutual aid came up as a significant focus of the conversation – suggesting that this might contain the seeds of the shift (willingness to ask for help, ability to provide it, willingness to experiment with a wider conception of the health protection system beyond Scotland and even beyond UK, blurring of national and local, mutual respect, identification of expertise across the system etc). The big policy dilemma that emerges from the story is about how best to combine ‘consistency’ across the country and flexibility for local autonomy. One strand suggested agreeing consistent national standards and applying them across the country. But what scope would that leave for local autonomy? It smacks a little of the first horizon system seeking control and uniformity (there was an exchange about guidance that suggested even well intentioned attempts to shift the culture are still interpreted as if they were about compliance rather than freedom). A second approach seemed to suggest agreement on ‘shared values’ or on a set of ‘common goals’ or outcomes (equity of outcome rather than equity of input as a compass direction?) that would then allow for maximum flexibility and autonomy at a local level. It is not clear that these two approaches are compatible: so this may be the central policy dilemma going forward. Fortunately the third horizon suggests that a more resilient system will need a balance of ‘experience, judgement and evidence’ – which may be just the qualities required to resolve the policy dilemma and transition to the third horizon. There is a lot in the story about working towards common standards and outcomes, trying things out, flexing the human system – providing the space for that evolution to take place. And the journey certainly seems to be worth the effort: from big cuts to big possibilities. In conclusion, the Chair of the Health Protection Stocktake Group, Jim Brown, thanked IFF for the day: it had provided plenty of useful food for thought at a pivotal moment for the group. For that he was very grateful. Graham Leicester Director International Futures Forum 26 April 2011 www.internationalfuturesforum.com

16
Appendix: Participants Health Protection Stocktake Group Jim Brown, Chair Lesley Wilkie, NHS Grampian Dona Milne. NHS Lothian Roland Salmon, Public Health Wales Andrew Blake, West Lothian Council Jackie Hyland, NHS Martin Donaghy, HPS Garrick Smythe, COSLA Jayne Leith, NHS Grampian - attendance TBC Joyce Whytock, Scottish Government Jacqueline Campbell, Scottish Government Andrew Riley, Scottish Government Malcolm McWhirter, Scottish Government Lorna Willocks, Scottish Government Resilience Group Andrew Elliott Ralph Thorp Marie Stevens Derek Smith Margaret Nicoll Suzanne Wilkie Allan Todd Kerry Jardine Lynda Nicholson Steven Woodhouse Colin McGowan International Futures Forum Graham Leicester Tony Hodgson Margaret Hannah Thanks also to contributions for the Scottish Briefs compiled by Colin McGowan for Scottish Resilience Unit, as follows: Biosphere Mary Christie Scottish Natural Heritage Governance John Curtice Strathclyde University Worldview Alison Elliot Centre for Theology and Public Issues
Habitat Deepak Gopinath Dundee University Water Jim O’Connor Scottish Water Wellbeing Margaret Hannah NHS Fife

17
Food David Thomson Scottish Government Enterprise & Development Trade Joe Brown Enterprise & Tourism Division Business Division Scottish Government Energy Bobbie Ronnie Scottish Government Critical National Infrastructure (CNI) Resilience
Climate James Simpson Scottish Government Climate Change Adaptation Wealth Alistair Brown Deputy Director of Finance, Scottish Government Community Laura Ross Employability and Tackling Poverty Division Scottish Government

time
prevalence
Three Horizons of Health Protection: 20 April 2011
© International Futures Forum 2007 www.internationalfuturesforum.com
H3
H2
H1
Support from academia too weak
Mutual aid
HP staff thin on the ground at local level
Inhibition caused by cost
Get rid of local/national or centre/ periphery mindset
Refresh the evidence base
Constrained by boundary issues
Facing big cuts
Fix the IT systems
Academia: bright people regress when kept in silos
Reversion to the old norm
Agree how to set national standards
Encourage self-helpSoften boundaries between HPS and boards
Soften the rigid boundaries
Mutual aid: start now, building links in UK and internationally
Practise mutual aid: start by offering it
Health protection with health improvement
Allow for radical change, emergent futures
Joint health protection planning
Greater internal resilience, secondments
Insist on joint working in planning, response, exercises
Broaden scope for cooperation across Scotland
Consistent set of standards across Scotland
Pathways of care: balance for resilience
Potential role of social media
Orientation towards outcomes for the population
From prescription to enabling
Cooperation and coordination principles from SCGs applied to HP
Variety of local implementation
Balance experience, judgement and evidence
Common goal: community planning and health protection
Make best use of pool of experience
Equity of outcome
Problems with the escalation process
Parochial reputation issues
Safe to admit need for help
Consider Scotland as part of UK wide system)
Developing innovative processes)
Guidance is more about enabling than accountability
Shared central values plus local autonomy
These notes record the final session of a workshop run by International Futures Forum for the Health Protection Stocktake. Groups worked in the first half of the day engaging with the potential challenges of a fast-changing world. The second half of the day involved considering how to make the health protection system more robust today and more resilient in the future. The pink post-its highlight issues that need to be addressed today. Possible promising innovations in horizon 2 are
shown on the yellow post-its. And the green record a longer term, principled perspective on the enablers for a resilient health protection system in the future.
BIG CUTS
BIG POSSIBILITIES
Realise the potential in the human system not just institutions