Health literacy and consumer-centred care: at the brink of change?
33
Health literacy and consumer-centred care: at the brink of change? The Ian Webster Health for All Oration to the annual forum of the Centre for Primary Health Care and Equity Leanne Wells, Chief Executive Officer, Consumers Health Forum of Australia Thank you for the opportunity to give the Ian Webster Health for All Oration. It is an honour to give this talk in recognition of an individual like Emeritus Professor Ian Webster and his commitment to ‘health for all’. What his work and that of this Centre demonstrates is the fundamental importance of robust knowledge and debate giving rise to good public health policy to shape better lives in Australia. Right now we are at a crossroads in health where we need the sort of leadership Ian Webster and many of his contemporaries has shown over many decades. We are at a point of flux in health policy decision-making where we need fresh thinking to tackle the paradox of these times: …..contemporary health care’s enormous potential to preserve and extend life at a time of avoidable disparity in health outcomes.
-
Upload
consumers-health-forum-of-australia -
Category
Healthcare
-
view
668 -
download
1
Transcript of Health literacy and consumer-centred care: at the brink of change?

Health literacy and consumer-centred care: at the brink of change?
The Ian Webster Health for All Oration to the annual forum of the Centre for Primary Health
Care and Equity Leanne Wells, Chief Executive Officer, Consumers
Health Forum of Australia
Thank you for the opportunity to give the Ian Webster Health for All Oration. It is an honour to give this talk in recognition of an individual like Emeritus Professor Ian Webster and his commitment to ‘health for all’. What his work and that of this Centre demonstrates is the fundamental importance of robust knowledge and debate giving rise to good public health policy to shape better lives in Australia. Right now we are at a crossroads in health where we need the sort of leadership Ian Webster and many of his contemporaries has shown over many decades. We are at a point of flux in health policy decision-making where we need fresh thinking to tackle the paradox of these times: …..contemporary health care’s enormous potential to preserve and extend life at a time of avoidable disparity in health outcomes.

We are at a point where we need to rejuvenate health policy thinking. When you think about it, apart from Medicare’s introduction, there’s really only three or so other real game changers that have been introduced by the Commonwealth over the last three decades that have really boosted the primary health care system and made a difference for consumers – at least that part of it that the Commonwealth leads or invests in. That’s one per decade on average. The first is the advent of divisions of general practice – Australia’s version of the regional ‘meso’ organisation. Even though we have seen some changes and medico-politics as divisions have moved to Medicare Locals and then to PHNs, the essential construct of a regionally based, clinically and community led organisation to respond to local need and support a connected system remains intact. The second is the Enhanced Primary Health care items. While we might reserve judgement on how successful they have been, they did, for the first time, provide public subsidies for team care arrangements and allied health service provision…. …..they recognised through our public health insurance scheme the growth in chronic disease and the need for multidisciplinary team care arrangements. And the third is the reforms to primary care psychiatry – the Better Access and Better Outcome in Mental Health Care – which have been attributed by independent evaluation to have changed the mental health landscape. Arguably the Indigenous Chronic Care Package is a fourth.

Critically, all have had bipartisan support which perhaps explains their success and longevity. But in the face of the consensus spearheaded by Barbara Starfield’s seminal work that tells us that the globe’s highest performing health systems have strong primary health care sectors, we’ve been stalled for too long. We face too many challenges to remain so. We need a modern, fit-for-purpose health system that serves our needs now, not as they were thirty or so years ago when Medicare was first designed. And that means primary health care access for all including the most vulnerable and disadvantaged in our society. A perfect storm? Ironically the ill-fated GP co-payment was the shot in the arm that health policy needed. It reinforced for all of us that good policy stems from the basic question: what problem are we trying to solve? There’s no doubt it jolted all the health players into renewed, vigorous debate about our aspirations for our health care system. We’ve had almost a decade of inquiry and review through the forums such as the National Health and Hospital Reform Commission and Nicola Roxon’s Expert Reference Group. All produced extensive reports steeped in equally extensive consultation.

Now we’ve got the new Minister’s ‘Healthier Medicare’ which includes a review of the Medicare Benefits Schedule to consider how services can be aligned with contemporary clinical evidence and improve health outcomes for patients And we’ve got a Primary Health Care Advisory Group - of which I am a member – looking at how to provide better care for people with complex and chronic conditions, Looking at innovative care and funding models, Ways to better recognise and treat mental health conditions, And how we can achieve greater connection between primary health and hospital care. In other words, how to design a better system for these consumers and those who care for them.


Consultations in all states and territories and regions are underway now on the Discussion Paper released by the Group. There are several avenues for input and consumer focus groups and a dossier of the patient experience of primary health care will also feed in to the case for change. The cynics might well say ‘here we go again’. The cynics might also say ‘this is all about GPs: what they do and how they are paid’. Well, to a large part, it has to be. We’d all agree that fee-for-service funding does not serve the management of complex, chronic disease at all well. But that doesn’t mean that it is the only place we put the spot light. We need systems thinking. We need to take a holistic approach look and analyse what works and doesn’t work about primary health care in Australia… …we need to focus on the way that its constituent parts interrelate, how the system works over time and how it fits within the context of even large systems. A framework I particularly like that promotes system thinking is
the ten building blocks of high performing primary care.
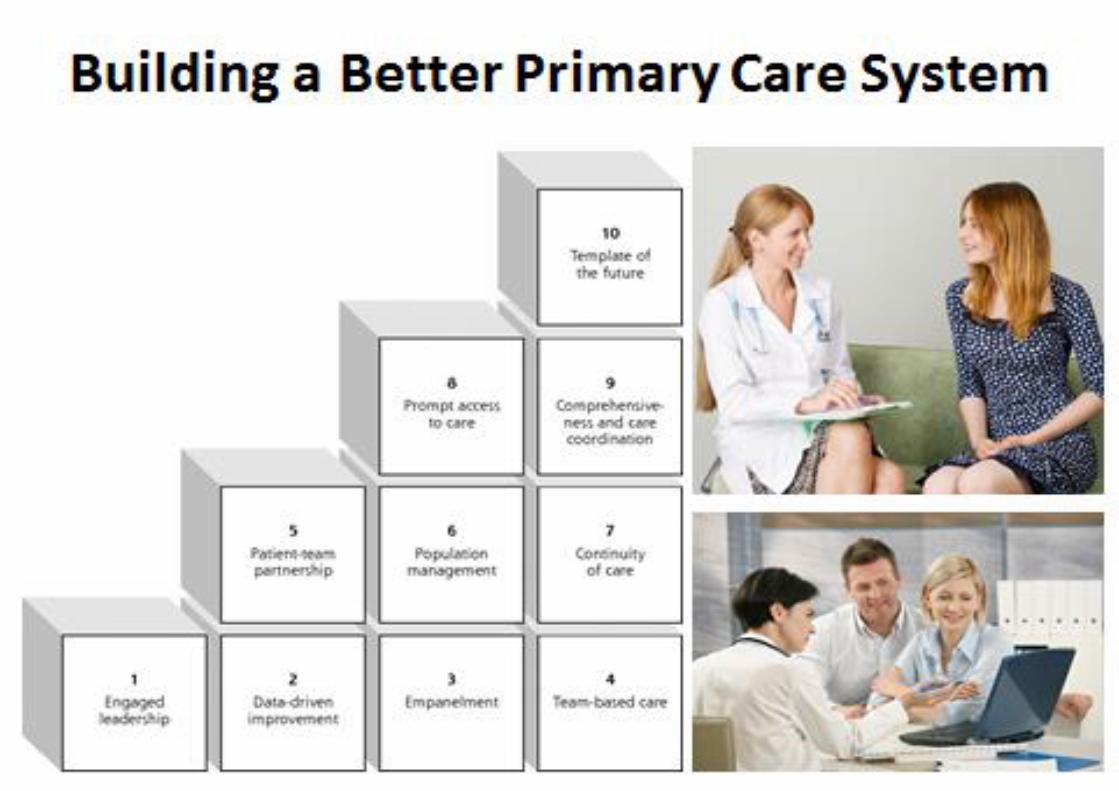

Its whole premise is how to gear the system to be more patient centred – how to reach those quadruple aims of health reform:
better health,
improved patient experience,
more affordable costs, and
a motivated sustainable workforce. And it makes it clear that active engagement of patients is a common thread through all building blocks, whether it be enrolment in a health care home; consumer peer workers as part of the health care team; or data-driven improvement that includes measures of patients’ experience. So granted, the current PHCAG process is about GP financing. It needs to be - but not exclusively. But the other certainty is that, without doubt, it will be a lost opportunity if any future primary health care strategy lacks solid investment in health literacy, self-management and patient activation programs so that consumers can take their rightful place as partners in care – as the directors of their care. That patients should be partners in care… that we should have primary health care policy and system that gives people greater control of their health and care so that services will have to adapt and reform around their needs and aspirations should not negotiable. Consumer health literacy and empowerment is not the soft underbelly. It is not the optional extra. Patient participation, health literacy and empowerment must be a main theme in the PHCAG report and the government’s response.

How can we guard against it getting forgotten by policy makers? We need to keep bringing it back to system thinking and what’s in the best interests of consumers: their equity of access, their experience of care and their health outcomes. That needs to be our compass.


So back to ‘Healthier Medicare’ and our current medico-political climate. It seems to me that this time around – after over a decade of reviews and reports - we have somewhat a perfect storm. We have factors aligning where previously they didn’t. There are the looming big shifts and wicked problems of which we are all too well aware:
Mounting evidence that focusing the health system on the
patient improves outcomes, is more effective, more cost
efficient and more satisfying for both patient and clinician
Growth in the prevalence of chronic disease often
requiring less acute medical care but more coordinated care,
not necessarily involving the doctor, opening the way, and
demand for, more individualised packages of care
Modern information technology shifting the system from
care arrangements based on one-size-fits-all to individually-
tailored solutions
Personal health care monitoring systems that enable
individuals to check their own health status…these
consumer-centred devices have the potential to
revolutionise routine checks and treatment of chronic and
aged care, contributing to the rise of self- managed care
Growth in consumerism and the informed patient

Trends towards choice, control and self-directed
approaches to human service delivery, spearheaded by the
NDIS
Consumers facing a fragmented, complex and increasingly
unaffordable healthcare system
And, not least, the ballooning cost of health care to individuals and governments
To put these costs and their drivers into sharper relief:
o Around 50% of Australians have at least one chronic
condition, and 20% have two or more
o The cost of chronic disease to Medicare has more than
doubled from about $10 billion to almost $20 billion over
the past decade
o Risk factors for chronic conditions such as obesity are
already at high levels and increasing
o There is a potentially preventable hospitalisation for
chronic disease every 2 minutes – now isn’t that an
astounding statistic?
o Nearly a quarter of people who visit an emergency
department felt their care could have been provided by a
GP.
We’ve known about these drivers for a while. What are the main differences this time around? What are the factors contributing to our perfect storm?

We’ve got central agencies (PM&C, Treasury and Finance) giving unprecedented focus to primary health care as a key solution to arresting the spending trajectories foreshadowed by the most recent Intergenerational Report. We got First Leaders recognising that primary health care is the main game in a statement after their most recent retreat. We’ve got a Health Minister who is on record as wanting to act. We’ve also got a consumer sector that is rapidly growing in maturity and positioning itself to be a serious policy actor. We’ve got a clinical community – notably GPs – recognising the case for change and actively canvassing new ways in which they should work and be funded. The RACGP’s Vision for Health paper has been out for comment for some time. In all of this, the case for the empowered consumer is compelling. Several commentators and researchers agree that as the need for efficiency and deriving better value from the healthcare dollar grows, the key is to get patients with chronic illnesses to manage more of their own care That’s why I want to focus today on the role health literacy and consumer-centred care are playing - and will increasingly play - as a pivotal influence in the way health care transforms in the next decade and beyond. What do Australian health consumers want? But first, let’s get back to basics. Let’s frame this discussion by thinking about what Australian health consumers want.

What fundamental needs and wants underpin consumer activism today? What experiences of healthcare do they value and rate highly? Any other industry setting out to invest in research and development efforts to redesign itself and its services would start with this fundamental question about their market…. ….so should health policy makers and administrators. After conducting extensive market research, NAB Health recently formulated a set of design principles to underpin what they call a future health “ecosystem”.

NAB’s design principles included:
Make life easier and more convenient for me
Let me take ownership and empower me
Include and respect me in the relationship
Keep me informed
Enable transparent access to my information
Give me the best care you can
Reduce my costs
By any standards, these sound like a pretty good set of wants to me – a good litmus test for any new policy. And they tell us that if Australia is to advance health there will need to be quite fundamental changes. There are, by our standards, radical changes happening or being proposed in countries like the UK and US, yet little real sign of serious debate about such changes here in Australia. Health literacy and consumer-centred care are concepts where Australia, despite a lot of talk has, with some exceptions, shown little progress in systematically advancing. This is at least partly due to the way the combination of Medicare and fee for service funding regimes has stifled better practices in this area. But the growing knowledge of what makes an effective consumer-clinician relationship and the revolution in information and technology now makes it more pressing than ever for us to exploit the benefits of health literacy, the activated patient and consumer-centred care in the way programs and services are designed and delivered. We are an informed group here today but let me just briefly cover what I mean by these two terms.

Health literacy is the ability to obtain, understand and use healthcare information … ….to make appropriate health decisions and follow instructions for treatment.
In a broader sense health literacy is also where the individual is
exposed to those influences which promote wellness, help
them understand their medical treatment and elements of a
healthy lifestyle.
A national report on health literacy agreed by Health Ministers
last year states that the complexity of the health system is
challenging for everyone and contributes to poor quality and
unsafe care.
Low health literacy also hits the bottom line with the report
saying it may be associated with 3 to 5 per cent extra cost to
the health system.
It goes on to say about only 40 per cent of adults have a level
of individual health literacy needed to meet the complex
demands of everyday life.
That means only 40 per cent of adults can follow health
messages and will be able to make right choices based on a
thorough understanding of those choices.

The literacy deficit: why empowerment matters?
So, what to do about this troubling literacy deficit?
The national statement suggests three ways to improve health
literacy.
Supporting effective partnerships between consumers,
healthcare providers and managers is one of these.
Consumers themselves have long recognised the benefit of
empowerment to their experiences of care and to setting and
achieving their health care goals in partnership with their
clinicians.
Yes clinicians will say that, of course, they are focused on the patient in front of them.
But too often it is the system which triumphs over the individual’s needs.
The consumer and patient is subject to the system rather than vice-versa.
Patients want and need professionals who see them as more than just the ‘vessel’ of a disease to be cured, or a problem to be solved. Patients want to be recognised for who they are: unique individuals with their own unique lives.
That might sound an obvious point. But CHF has found that the biggest drivers of complaints and dissatisfaction with the health system is almost always that consumers feel they aren’t being respected as individuals, and partners, in their own health care decision-making.

Our message to the policy makers and health workforce is for them to take a patient-centred approach to setting policy and providing care: not disease-centred, not system-centred, but patient-centred.
So, if that’s the case what do we need the system to reflect:
Clinicians’ education and continuing professional development that promotes patients as partners in care
Consumers involved in health care research
Self management programs embedded in primary care
Consumer participation recognised in national safety and quality standards and associated accreditation
Consumer participation in the governance and values of health organisations
Models of care where, as Janne said, there’s a team of professionals looking after the consumer, sharing information and contributing to a common care plan
Care in place – by that I mean but we need to move away from thinking that hospitals or clinics are the only care settings. Health professions should be prepared to meet the consumer where it’s convenient for the consumer. For primary care, this might mean expanding services in pharmacies, having better after-hours services, making better use of telemedicine, coming into consumers’ homes and offices or in-reaching to supported accommodation and crisis homelessness services

clinicians open to working across the traditional clinical boundaries. The future for specialists may be beyond the hospital’s four walls.
Recent work by the UK think tank, the King’s Fund, contemplates new ways of working for hospital physicians whereby they work much more closely with their primary and community care colleagues in non-hospital settings as advisers.
So it’s all these things like this that add up to what I would say is a consumer-centred system. And let’s be frank, it’s not money that is not necessarily the big
barrier here. It is that much more challenging hurdle: human
behaviour.
So much of the benefits that come with a consumer – focused
system are much less to do with cost than with changing the
way we do things.
Time for alternative approaches So given the largely clinician-directed nature of our health system, don’t we need to consider alternative approaches? I think it starts with culture change and challenging the prevailing orthodoxy. There are highly talented health care thinkers who are pointing towards a brave new world of consumer-centred, individualised health care that lies within our reach right now.


Eric Topol, the medical innovator and cardiologist recently published a book entitled The Patient Will See You Now:.. The Future of Medicine is in Your Hands. Topol specialises in arresting conventional thought … but he is no couch commentator. He was the first physician to raise the alarm earlier this century about a new arthritis drug associated with high rates of heart attacks. It’s fair to say he probably raises the pulse of many conventional doctors with his arresting book titles. Recently he tweeted a table showing the contrast in culture and practices between what he calls “Old Medicine” and “New Medicine”. So the Old Medicine is:
“Population-based”… --- while the New Medicine is “individualised”.
The old is “One-off, doctor’s office”… --- The new is real-time streaming, in the real world
Doctor-ordered data makes way for… --- patient-generated data
Unshared doctor’s notes become … … Our notes, patient-edited
Information owned by doctors and hospitals becomes…

--- information owned by rightful owner
And data goes from “limited”… --- to “panoramic”.
We see in those contrasting terms a striking shift away from the paternal doctor-passive patient stereotype to the two-way relationship that involves a dialogue and information sharing between clinician and consumer… To the sort of health literacy and consumer-centred care that Janne described. And we see the same sort of principles emerging elsewhere, this time in proposed new rules for the coming healthcare era emerging in the US. The Commonwealth Fund recently published this list proposed by the Institute of Healthcare Improvement. The Institute’s recipe for what they describe as a “radical redesign of health care delivery” includes precepts such as:
Change the balance of power – to encourage patients and families to take a leading role in their care
Standardise what makes sense and make it easy – streamline processes and use technology to facilitate team work so patients with complex conditions are not asked to repeat tests and medical histories
Customise to the individual so services are designed to meet needs of patients rather than the providers and payers
Collaborate and cooperate

Eliminate walls – encourage partnerships between health care, social agencies et all to address social and economic issues that impede good health
Assume abundance – to encourage cooperation that makes the most of existing resources
Return the money – share savings between patients, employers and communities to ensure affordable care and to promote health or invest in other sectors like education
Move knowledge, not people – to deliver relevant knowledge to patients and providers whenever and wherever they need it.
So that list shows just how far moves towards individualised, personal-tailored approaches to health are being proposed in the US, albeit conveying the optimism of the USA, particularly admirable given its history of a costly, highly inequitable health system. And in England, the health world there too is deeply embroiled in debate about pressure for change to the NHS. Giving people choice and control over their health and care and shifting away from a system where decisions that impact most on patients are still taken by clinicians, commissioners and policy makers are seen as a key part of the solution. Again, it is the individually-targeted approach that is being proposed as a centrepiece for change according to former (Labour) Health Secretary and leading commentator Alan Milburn.

In a report titled ‘Powerful People’ by the Institute for Public Policy Research in the UK, Milburn and collaborator Stephen Dorrell have written in their foreword that the NHS needs to be transformed and that money be “put directly in people’s hands by accelerating the spread of personal health budgets”. They say these payments should be an entitlement for all those with long-term conditions by 2020. They write about “devo-health” where power should be devolved down to local areas and to frontline professionals so that they are better able to redesign services around people’s needs. Consumer centred care seems reasonably subscribed to in the UK, at least by lead commentators and clinicians. Even so, Milburn and Dorrell’s commentary suggests that, despite political emphasis on empowering patients, empowerment remains at the margins rather than the centre of the UK system. Equally so, they say their agenda would require a profound change to clinical and healthcare cultures. Their report argues for giving citizens greater control over their own health and care, so that services are redesigned around their needs, “to improve health outcomes and to save money by supporting people better to manage their conditions themselves”. I guess it’s that last point on costs which tends to focus the mind on the idea that perhaps better care - a more responsive system - can save costs, and/or generate more available cost-effective care.

What’s happening in Australia? So what’s happening in Australia in the way of patient-focused systems? Not nearly enough CHF would say. But there’s promise on the horizon. The NSW Clinical Excellence Commission’s “patient-based care challenge” is one such examples. Earlier this year the Commission’s Karen Luxford and co-author Stephanie Newell published in the British Medical Journal about this project.
The aim of the program introduced across NSW Health districts
was to make patient centred care more broadly recognised as
everyone’s responsibility from the executive through to
clinicians and staff.
Developed in collaboration with a patient advisory committee,
this project highlights the importance of engaging with patients
right through: at the bedside and in health service governance
and strategic decision making.
The leadership challenge proposed 26 possible strategies
ranging from starting each board meeting with a story of patient
care, related by the patient or read by staff, and including
requirements that the board spend 25 per cent of meetings on
quality of care issues, regular board and executive visits to the
ward.

The strategy also embraced the mission “the patient at the
centre --- every patient, every time”, encouraged staff to view
patients, family and carers as care team members, and sought
to use patient feedback to drive change. That might include
getting patient family advisers to survey patients in waiting
rooms or work with junior medical staff to conduct a patient
shadowing project.
By October last year, after about two years, 13 districts had
adopted an average of 19 of the 26 strategies.
The authors say that as the project uptake was in the early stages it was hard to judge whether it has been a success. Whatever the final results, the important feature is that we are seeing significant steps to promote the concept of consumer-focused health care championed by an organisation whose core business is to lead safety and quality improvement in a public health system. Like the Commission, Primary Health Networks, as regional system stewards, are well placed to take up this mantle. Health Minister Ley has said that patients will have the
opportunity to have their say, with community advisory
committees to advise PHN boards “from the patient
perspective”.
But success will depend on whether PHNs have got consumer
and patient perspectives as integral and on the same footing
as input from clinicians.

It will depend on PHN’s appetite for investing in patient
leaders as much as they invest in clinical leaders, and the
sophistication with which they involved patients and consumers
in all steps of the commissioning cycle.
And in that respect, we are seeing some hope-stirring
particularly in the directions being set by the Federal Health
Minister Sussan Ley.
The PHCAG Discussion Paper I mentioned earlier makes the point that Medicare is failing to meet the challenge of chronic care. It says patients often experience a fragmented system, uncoordinated care, difficulty finding the right care, low uptake of eHealth and technology to overcome these barriers…. It acknowledges that patients feel disempowerment, frustration and disengagement. A heartening feature of the Paper is the acknowledgement of the idea of the “patient as a partner in care”. It recognises that patients have different levels of understanding, skills and capacity to self-manage their conditions. Targeted education, training and motivational support, the report says, has been shown to enable patients more effectively to self-manage their health and wellbeing. Furthermore, the report states “health workforce training --- beginning at the undergraduate level --- must include the principles of the patient as a partner in care”. This is a central requirement, we believe, for the development of health literacy and consumer-centred care.

As the report states, care co-ordinators could help patients better understand their needs and make an assessment of their self-management and self-advocacy. The coordinators could support patient participation, engagement and self-management and build health literacy, either directly or in conjunction with practice nurses, community nurses and Aboriginal and Torres Strait Islander health practitioners. Putting patients first: the ultimate disruptive innovation?
So in conclusion, right now, putting patients first is more an aspiration than a systematic program of action. We have promising sentiments in high level policy documents and some promising practice but it is in pockets and not widespread. What should we be doing so that patients can climb the health care ladder?


We need broad changes in behaviour and culture including:
Acknowledgement and support by clinicians to treat the patient as an individual with individual needs and not as another passive recipient at the mercy of an uncoordinated system
Educating the health work force to encourage informed and engaged health consumers
Funding clinicians to give the time and attention to informing and supporting patients to better manage their health
Shifting from a fee for service system to a system that rewards wrap-around, team-based care rather than one-off episodic services, particularly for those with chronic and complex conditions
And not least, providing effective funding for the education and training of health consumer representatives --- like Janne Graham in the video --- to guide both patients and health institutions towards more effective care
These suggested changes are pretty modest I would suggest, given the perfect storm we are facing of rising costs and a disempowering primary health system. We remain hopeful that Australia takes up the opportunity to be exemplars: to be leaders rather than followers of world’s best practice in consumer participation and leadership in primary health care. Such an approach would exploit the growing evidence in
Australia and abroad of the value of having active consumer
involvement in both design and delivery of health services.
The Australian Commission on Safety and Quality in
Healthcare reminds us of the research that demonstrates that
patient-centred care improves the patient experience and
creates public value for services.

As Alan Milburn and several other commentators also remind us, there is a straightforward moral case for empowering people in health and care as well as an instrumental case. Empowerment can produce better health outcomes, more satisfied citizens and much needed financial savings. Rather than being seen as a warm and fuzzy option, consumer health literacy, empowerment and better self-management should be central to a modern health system. Patients have been described as the health system’s untapped resource. They have been described as powerful agents of change. The empowered consumer could just well be the disruptive innovator we have been looking for.