Health information, health treatment, and worker productivity: Evidence from Nigeria Andrew Dillon...
43
Health information, health treatment, and worker productivity: Evidence from Nigeria Andrew Dillon Michigan State University Jed Friedman The World Bank Pieter Serneels University of East Anglia October 2013
-
Upload
kody-phinney -
Category
Documents
-
view
216 -
download
1
Transcript of Health information, health treatment, and worker productivity: Evidence from Nigeria Andrew Dillon...

Health information, health treatment,
and worker productivity:
Evidence from NigeriaAndrew Dillon
Michigan State UniversityJed FriedmanThe World Bank
Pieter Serneels University of East Anglia
October 2013

MotivationHealth largely seen as critical input to economic
development … but economic gains from health investment difficult to measure
Yet economic gains from health investment important for policy decisions
Agricultural productivity is key for growth in low income countries, but productivity increasing investments (irrigation) may increase exposure to vector borne illnesses.
Does investment in health increase productivity and income, and by how much?

MotivationMalaria remains a significant illness worldwide, especially for
sub-Saharan Africa Estimated 210 million infections and ~1 million deaths per year
20% of estimated malaria cases worldwide are found in Nigeria
51% of households in Nigeria reported at least one episode of malaria (NLSS 2003/4) – in endemic settings, “malaria” often becomes a general term for illness/fever
Estimated cost of malaria from previous work: direct cost of treatment absenteeism from work (‘indirect cost’) is estimated between 1-
5 days per episode

Motivation Existing micro-economic evidence suggests
substantial effects of health on income and labor outcomes in low income countries
Disease affects labor outcomes Reduction in malaria exposure at an early age increases
income later in life (Cutler et al. 2010 and Bleakley 2010)
HIV/AIDS reduces labour supply in Kenya, Botswana (Fox et al 2004;Thiruthmurti et al 2006;Habyarimana et al 2010)
Schistomosiasis reduces labor supply in Mali (Audibert and Etard, 1998)
Pollution reduces worker output in US (Zivin 2010)

Some micro-estimates of cost per malarial episode
Study Country Direct cost
(% of total cost)
Indirect cost
(% of total cost)
Morel et al. Vietnam US$ 0.7 (6%) US$ 11.09 (94%)
Akazili et al. Ghana US$ 1.87 (29%) US$ 4.52 (71%)
Deressa et al. Ethiopia US$ 1.60 (28%) US$ 4.08 (72%)
Cropper et al. Ethiopia US$ 1.60 (7%) US$ 22 (93%)
Sauerborn et al. Burkina Faso US$ 1.85 (31%) US$ 4.11 (69%)
Ettling & Shepard Rwanda US$ 0.63 (28%) US$ 2.25 (72%)
Asenso-Okyere &
Dzator
Ghana US$1.81 (21%) US$ 6.87 (79%)
Indirect costs (absenteeism) is highest, but estimates derive from self-reports, valued at average wages, not including on-the-job costs. Furthermore, all based on observational data.

Motivation for current study design
Existing empirical evidence suffers from problems with:Omitted or unobserved variables
E.g. endowment effects: worker’s initial health condition, physical work capacity
Reverse causality Are healthier workers more productive or more productive workers
healthier? Or both?
Measurement of productivityNeed a measure at the individual worker levelNeed uniform measure, so consider homogenous activities

Empirical questionsDoes access to workplace based malaria testing
and treatment affect income, labor supply, and productivity?
If malaria treatment leads to higher income, is this because of its effects on labor supply, productivity, or both?
Are there other benefits from workplace testing and treatment for malaria?

Study siteOne large 5,700 hectare sugarcane plantation in
rural Nigeria
Employs ~800 sugarcane cutters who work throughout the season
Workers are organized into work groups, managed by a supervisor and headmen
Workers are paid (piece rate) 2.04 naira per “measured rod” of sugarcane they cutA “measured rod” is a physical standard carried by
every gang leader

Study siteThe plantation records for each worker the daily
amount cut, days worked, and earnings
Workers are paid monthly, and keep careful track of their earnings to verify payments
At the start of every work day, workers can select into cane-cutting or scrabbling:Scrabbling pays fixed wage (500 Naira/day) and is
less arduous, involves collecting and bundling cut cane, most workers cut cane but many scrabble for a small proportion of days
Harvest work is seasonal: December – March and relatively lucrative

Worker’s decision theoryWorker’s output is a function of ability and effort.
Effort may be influenced by wage, health self-perception, individual motivation, etc.
Worker’s earnings are determined by both labor supply and their productivity when working.
Worker’s choose not only how much to work but which occupation, cutting for a piece rate or scrabbling for a lower average fixed rate. This choice depends on the worker’s willingness to supply
effort.

Experimental design A mobile health clinic visits the workforce during
working hours
Every sugarcane cutter is tested for malaria and, if positive, treated with ACT over the course of an 8 week period
But the temporal order of worker testing and treatment determined on a random basis …
… potentially inducing exogenous variation in worker health over study period
Conducted at peak of harvest season (Jan, Feb) in 2010

Experimental design (cont.)
Each week, 2-3 randomly selected gangs visited by study team, and random subset of workers assessedStudy design: blocked by work group, assessment
temporally randomized across workers within work group
Small survey team administers work and health questionnaire
Mobile health clinic tests for malaria (RDT and blood slides)
All parasitemic positive workers treated with ACT

A health team visit…

Health tests after clearing a field…

Experimental design: validation
In principle randomization guarantees valid counterfactual but in reality:8 work groupsOver 1 harvest season~800 workers
Need to explore balance of worker characteristics within work group over time

Worker characteristics and importance of work group strata

Within work group balancing test across survey week, by round
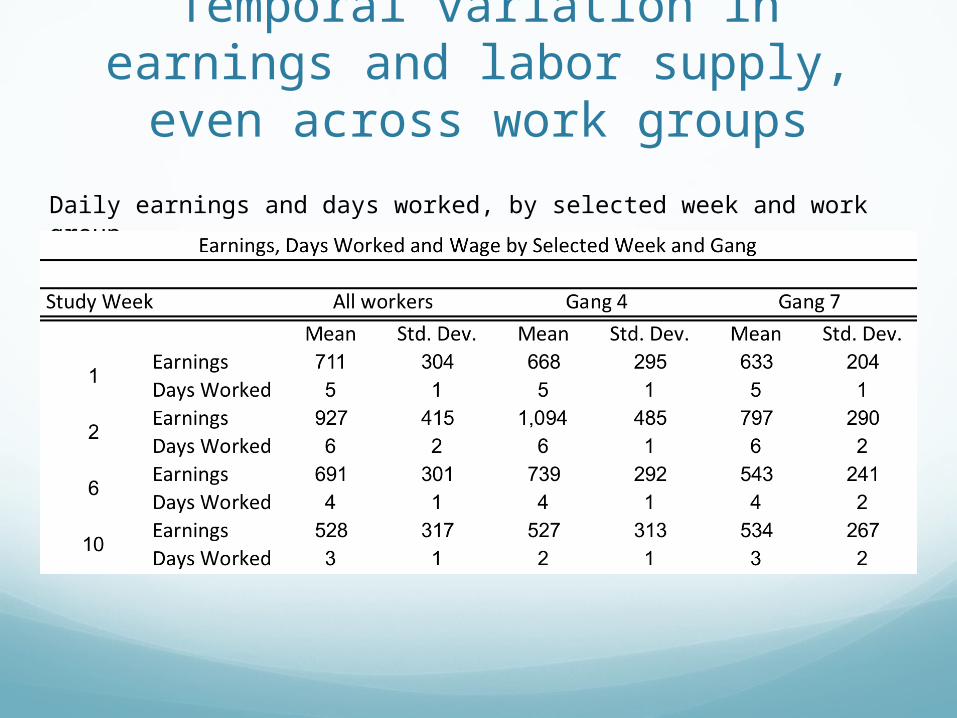
Temporal variation in earnings and labor supply, even across
work groups
Daily earnings and days worked, by selected week and work group

Measurement and diagnosis of malaria
Diagnosis follows the WHO standard of microscopy from thick blood smear, independent validation
Results in 3-day lag between specimen collection and diagnosis:Metric is number of parasites observed in 5
randomly selected blood field, MOH cut-off is 3 parasites

Data structure overview

Impact estimation strategyWorkers grouped by week of interview (and
work group) to identify windows of potential impact

Econometric strategy overview
We start with an intent to treat effect (ITT) ITT: compares outcomes for workers who were
offered access to testing and treatment with outcomes for those who had not yet been offered access to testing and treatment
Stratification by work group, and temporal variation within work group, indicates importance of gang-week FE
Where Wt- is set of all workers assessed before observation period t

ITT results
11-13% gain in earnings from treatment over 2-3 weeks, due in roughly equal measure to increased labor supply and increased productivity

Robustness of ITT
Results likely unaffected by externalities from treatment:most malaria transmission occurs in evening or night
when workers are off plantationsymptoms usually begin 12-25 days after infection
Inclusion of worker observables (BMI, hemoglobin, education, etc.) does not affect results

Summary so farA temporally randomized work site regimen of
malaria testing and treatment indicates significant increase in earnings (~10%)
Increase is due in roughly equal proportions to: Increased labor supply Increased earnings per day

Treatment on the treatedWe can also attempt to estimate the ToT with an
additional assumptionToT: compares outcomes for parasitemic positive
workers who received ACT with outcomes for workers who were sick during the same period, using information from future positive tests

Treatment on the treated
An earnings effect of roughly same magnitude as ITT, mostly through labor supply response.
Here the estimated 3-week earnings benefit ~$9
Compliance protocolValidity of ToT estimates is predicated (in part) on
compliance with treatment
Workers who tested positive were visited by the health supervisor on:Day 2 of their ACT prescription The day after their prescribed treatment endedWorkers were given a small incentive (50 Naira) to
return the medicine container and asked follow-up questions to confirm proper compliance with treatment and to identify any adverse effects

Treatment on the treated (cont.)
What may account for similar magnitudes of ITT and ToT estimates, given 36% positivity rate?Our counterfactual for the “ill” is noisy – TOT
estimates are comparing recovering workers with some proportion of healthy ones (and not all sick ones as necessary). Very difficult to correct for this with existing data
The intervention is a combination of two “treatments”:Health information on malaria statusMalaria treatment if sick
Might workers also be responding to the first component?

‘TOUT’ on malaria negative workers
Similar in earnings magnitude to ITT estimates, increases largely coming through increases in daily wage

Reductions in scrabbling greater for malaria negative
workersFurthermore it appears that gains for negatives at least
in part due to switch into piece-rate from scrabbling

Gains to negative workers not solely due to decreases in
scrabblingCan restrict estimates to worker-weeks with no
scrabbling

So what is happening here?
Does good health news lead to higher worker participation and productivity? New health information has been known to affect subsequent
behavior, at least in the case of HIV, where learning positivity status leads to safer practices (Thornton (2008, 2012))
But little literature concerning health status learning effects of communicable diseases
Theory may tell us (i.e. Gong 2013) that only surprises from new information should affect behavior – i.e. a change in expectations
TOT for malaria negative workers

Suggestive findings consistent with good health news leading to change in expectations of productivity
Are there other explanations/possible channels? A “meaning response” a la Moerman (2002) who examines
the placebo effect and argues the “meaning” given to placebo is what induces benefits. Can a healthy diagnosis in endemic setting by medical professional convey sufficient meaning to alter subjective perception of well-being and actually increase productivity?
Gift exchange a la Akerlof (1982) – gratitude for health test leads to higher morale and greater effort. Unlikely in piece-rate setting and this plantation context.
TOT for malaria negative workers

Conclusions Clear that the malaria testing and treatment increases the
labor supply and productivity of the average worker
Earnings responses for both the malaria positive, who receive medication, and malaria negatives
Gains among the sick largely due to increased labor supply, and greatest gains observed among the sickest. At prevailing wages, estimated $9 benefit from treatment
Gains among the healthy apparently in part due to change in earnings expectations (shift out of scrabbling). Estimated $11 benefit from receiving good news.
Example of workplace based health program that likely pays for itself

CodaThanks for listening!

AppendixExternal validity: one firm, one particular group
of workers (prime age males) Very low % of workers miss a whole week of work, but
perhaps we miss the “sickest of the sick”

Compliance statistics

Are these gains the “productivity costs” of malaria infection?
Only a fraction of workers have malaria, what is the expected gain from treatment for them?
35.9% of workers tested positive and given treatmentWald estimator [ITT estimate over proportion
treated] is one take at a TOT
Substantial gains from treating malaria!3 week gain approximately $30, while cost of ACT = $7
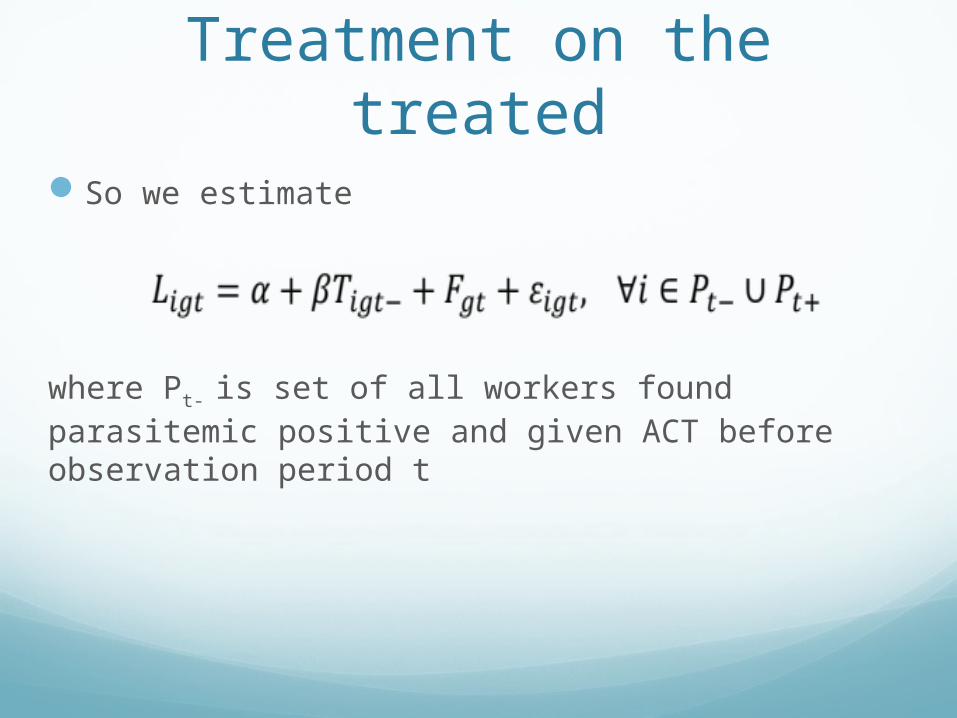
Treatment on the treatedSo we estimate
where Pt- is set of all workers found parasitemic positive and given ACT before observation period t

Designing Evaluations of Workplace Based Programs
Time varying access to intervention facilitates the construction of treatment and control groupsNot all types of interventions can use this strategy
(treatments with potential spillovers)Resolves ethical dilemmas
Measurement of productivityAcross firms worker productivity may be highly
variablePiece rate wage systems are idealRecording system of worker output is essential

If parasite presence, even at low levels, affects subjective health and expectations, then perhaps those with parasites more subject to surprise:
Evidence on upside surprise

We can also stratify by subjective perception of work capacity: whether worker feels tired at end of day
Evidence on upside surprise