Health in Your Hands: Lessons from Building Public ...
24
Health in Your Hands: Lessons from Building Public- Private Partnerships for Washing Hands with Soap 33512
Transcript of Health in Your Hands: Lessons from Building Public ...

Health in Your Hands:
Lessons from Building Public-Private Partnerships for Washing Hands with Soap
33512

The World Bank does not accept responsibility for the views expressed herein, which are those of theauthors, and should not be attributed to the World Bank or its affiliated organizations. The findings,interpretations and opinions expressed in this document are the result of a research supported by theBank. The designations employed and the presentation of the material are solely for the convenienceof the reader and do not imply the expression of any legal opinion whatsoever on the part of theWorld Bank or its affiliates concerning the legal status of any country, territory, city, area, or itsauthorities, or concerning the delimitations of its boundaries or national affiliations.
July 2002, 2nd Edition

Contents
Introduction 2
Executive Summary 3
Part 1The Public Private Partnership for Handwash: A Brief History 5
Part 2Why Handwashing? And Why a Public Private Partnership? 6
Part 3The Approach Step-by-Step 9
Part 4Understanding Handwashing with Soap 14
Part 5Future Challenges, Conclusions 19
List of Tables
Partnership Partners 2
Possible incentives and contributions for public/privateplayers in the Handwash Public Private Partnership 8
Handwashing with soap by mothers in Ghana and Kerala 15
List of Boxes
Key Lessons 4
Observed handwashing practices in Ghana and Kerala 15
The soap habit 17
Key Lessons 19
List of Figures
Steps 3
Leading Infectious Killers 7
Role of the partners in the Handwashing Public Private Partnership 14
The pyramid of cleanliness 16
Range of influences on a Kerala village that can potentially be harnessed 18
Lessons from Building Public-PrivatePatnerships for Washing Hands with Soap

Introduction
Washing hands with soap could save a million lives. Eighteen months ago, a small team fromthe Water and Sanitation Program, the World Bank and the London School of Hygiene andTropical Medicine set out to answer the following question:
“Can the expertise and resources of Industry and Governments be coupled to design and deliverlarge-scale, high-impact handwash promotion programs?”
A year and a half on, public-private partnerships for handwashing with soap are in place inGhana and Kerala, and full-scale handwash promotion programs have been designed. Othercountries are set to join the initiative. This document outlines the approach that was taken, andoffers lessons for those interested in setting up such programs in future.
Partnership Partners
International In Ghana In Kerala
■ Water and Sanitation Program
■ World Bank
■ London School of Hygiene &Tropical Medicine
■ UNICEF
■ USAID
■ AED
■ Community Water andSanitation Agency(CWSA)
■ Ministries of Health,Education, Works andHousing, Women andChildren’s Affairs
■ Ministry of LocalGovernment and RuralDevelopment
■ Association of GhanaianIndustries
■ Unilever Ltd, GETTRADE,PZ Cussons
■ UNICEF
■ World Bank
■ Water and SanitationProgram
■ Kerala Rural Water Supplyand Sanitation Agency(KRWSA)
■ Government of Kerala,Government of India
■ Hindustan Lever Ltd.
■ Indian Soap and ToiletriesMakers’ Association(ISTMA)
■ Khadi and Cottage IndustryBoard
■ Ministry of Health, Ministryof Rural Development
■ UNICEF
■ WHO
■ World Bank
■ Water and SanitationProgram
2

Executive Summary
Initiate
Assign focal person
Collect Info
Form steering committee
Execute consumer studies
Design the Handwashing program
Resource the program
Detailed design and test of approaches
Baseline, M&E
Launch
1
Steps
Programs to promote handwashing with soap could be amongst the most effective and cost-effective interventions for reducing infectious diseases in the world today. A million lives couldbe saved each year, if hands were washed systematically with soap.
Whilst public agencies are interested in saving lives, private industry is more interested inselling soap. This is the founding rationale for a public-private partnership to promotehandwashing with soap. However, partnership can bring other benefits; industry enhances itsimage and knowledge whilst the public sector benefits from state-of-the-art communication skillsof private industry.
After 18 months of work, two programs are ready for launch in the state of Kerala, India and inGhana. Building up the partnerships was a slow and resource-intensive process. Success willultimately be judged by carefully measuring the impact of the programs. In the meantime, fourfactors argue for the pursuit of the Public Private Partnership, both in the two trial countries andin expanding the initiative to a limited number of other countries:
• The handwash programs that have been designed are groundbreaking.• Many enquiries on joining the initiative have come from Governments, NGOs and external
support agencies.• Three major global industrial players are in discussions on expanding the initiative.• International interest in handwashing as an intervention has grown in the past two years,
increasing the need for well-documented trials of new approaches.
Many private and public agencies are interested in setting up Public Private Partnerships forHandwashing in their own countries. This document is primarily for them. It is also for decisionmakers in Industry, Government and external support agencies, who need to know if investingin such activities is likely to be worthwhile or not.
Part 1 of this document explores the rationale for handwashing programs and for Public PrivatePartnerships; Part 2 outlines the history of the initiative; Part 3 documents the approach; andPart 4 covers insights about handwashing gleaned from consumer research and the implicationsof the findings for the handwash programs. Part 5 provides conclusions and key lessons.
This document covers the lessons learnt about setting up Public Private Partnerships forHandwashing. A second document will cover operationalizing and monitoring. All programreports, products and materials are posted on our dedicated website at http://www.wsp.org/english/activities/handwashing/
23
4
5
6
7
8
9
10
3

The Public Private Partnership for Handwashing: an idea whose time has come?■ Handwashing with soap could save a million lives.■ Diarrhoeal diseases are losing ground to other health issues on the international agenda:
new programs to promote handwashing provide a rallying point.■ Combining the forces of the public and the private sector to promote handwashing with
soap offers rewards to both.
However, it needs time and effort...■ Few individuals and agencies appreciate the importance of handwashing; advocacy is
needed at all levels.■ Building partnerships is time-consuming and resource intensive. It needs complementary
skills and champions with drive and energy.■ People at the top of key institutions provide the necessary leadership.■ Industry players may be reluctant to work together, but they increasingly see that it makes
sense to increase the market for all. To come on board, small-scale players may need extraassistance.
■ Partnership arrangements should be flexible and open to all who wish to join.
...and insight, understanding and particular skills■ Industry is well placed to design communications programs; they have made huge investments
in developing their own expertise in consumer insight, message design and media planning.■ Consumer studies into handwashing should be carried out by professional market/consumer
research agencies with Industry assistance.■ Communication strategies require detailed trial and testing for effectiveness, otherwise the
investment may be wasted.■ Changing behavior patterns is not easy. According to industry, adopting a new practice
needs at least six effective contacts a month. Drip-drip approaches do not provide a criticalmass of stimulus for habits to change.
■ A champion from each organization at each level is essential. A trusted catalyst that canbring together industry, government and support agencies is also needed.
But much remains to be learnt■ Work is needed to validate indicators of handwashing behavior for baseline monitoring and
evaluation. Trying to monitor the impact of the program on diarrhoeal diseases is a moredifficult task.
■ External support agencies, government and industry have different expectations and timehorizons; figuring out how to satisfy the needs of all partners while retaining innovativeprogramming is a challenge.
■ Further challenges include how to make partnerships deliver new handwash products, andmaking handwashing cheaper for the poorest, possibly via tax incentives.
Finally■ The initiative cannot be evaluated until it has produced results, but the prospects look good
for the continuation and expansion of the Public Private Partnership for Handwashing.
Key Lessons
4

Part 1The Public Private Partnership forHandwash: A Brief History
The Water and Sanitation decade of the 1980ssaw substant ia l improvements in theinfrastructure of environmental health in thedeveloping world. However, diarrhoealdiseases remained amongst the top three killersof children. The realization began to grow thatthe way in which facilities were used might bejust as important as their provision. Growinginterest in hygiene behavior in the 1990s gaveresearchers insight into the context and meaningof hygiene behavior2 and led to thedevelopment of approaches such asPar t ic ipator y Hygiene and Sani tat ionTransformat ion (PHAST) and the socialmarketing of hygiene 3, 4.
However, approaches that could be scaled upto meet the need for improvement in hygieneon a mass scale, similar to vaccinationprograms, were still needed. Consumer studiesin the late 1990s highlighted the complexityof the determinants of hygiene behavior andshowed that simply teaching people abouthealth was not going to lead to substantialbehavior change5. Rather, positive images andpopulation-scale marketing of behavior change,based on insight into the factors that motivateconsumer behavior, were required.
One program at the end of the 1990s was ofparticular interest: the BASICS/EHP CentralAmerican Handwashing Initiative, whichencouraged four private sector companies tolaunch handwashing campaigns in f ivecountries (Guatemala, Costa Rica, El Salvador,Honduras and Nicaragua). The results wereencouraging, and proved that soap companiescould be capable and willing partners for healthpromotion6.
A workshop on Hygiene, organized by theWorld Bank/Water and Sanitation Program(WB/WSP) and the World Bank, with helpfrom the London School of Hygiene andTropical Medicine (LSHTM), in May 2000considered both the results of recent research
into hygiene behavior and the BASICSexperience. This inspired the idea of trying todevelop a new Public Private Partnershipmodel. Over the following year, discussionswere held between WB/WSP and LSHTM, andmanagement consultants McKinsey and Cowere consul ted. They considered theproposition sound, but pointed out the needfor strong leadership and careful planning.
The concept was further developed, and inthe year 2000, two sites willing and able totrial the idea were located in Ghana and thestate of Kerala, India. The objective was to tryto get private industry and the public sector towork together to develop programs to promotehandwashing. We wanted to learn how to setup such programs, and to explore theirfeasibility, acceptability and value. A contractfor technical assistance from the LSHTM for theinitiative was signed with WSP and the WorldBank in March 2001.
After a year in the field the partners have:• Established bases in the Kerala Rural Water
Supply Agency (KRWSA) and theCommunity Water and Sanitation Agency(CWSA) in Ghana.
• Bui l t local par tnerships of indust r yassociations, industrial and small-scalemanufacturers, Ministries, external supportagencies and NGOs.
• Setup national or s tate- level s teeringcommittees and made concerted nationaland international advocacy efforts to explainthe concept.
• Designed, commissioned, and assisted in theexecution and analysis of studies of soapconsumption and the soap market in Ghanaand Kerala.
• Designed communications programs topromote handwashing with non-brandedsoap across the state of Kerala and the wholecountry of Ghana. Commitment to fund theprograms has been for thcoming from
5
“A growing number of business leaders share unease about any form of global economicdevelopment that fails to emphasize the human dimension or that creates a globalization ofopportunity without a corresponding globalization of responsibility” 1

government and external support agencies,whilst the private sector has agreed toprovide technical and managerial skills.
At the same time, at a global level, theteam has:• Suppor ted the documentat ion and
disseminat ion of the BASICS CentralAmerica experience.
• Set up an international advisory group.• Been advocates for the ini t ia t ive in
international fora, the international press
and a dedicated website.• Carried out a brief study of the world market
for soaps.• Carried out a study of the experience of
Public Private Partnerships in the healthsector.
• Worked with three big multinationals onperspectives for wider expansion.
• Raised funds from the Bank-NetherlandsWater Partnership for continuation andexpansion of the initiative.
Why Handwashing? And Why a PublicPrivate Partnership?
Part 2
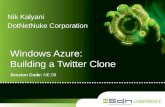
Handwashing with soap couldsave a million livesDiarrhoeal diseases are the second biggestkiller of children in the world today (figure 1).In the same way that the mosquito is the vectorof malaria; transferring the infection from personto person, so hands are the main vector ofdiarrhoeal pathogens; transferring them fromsurface to surface and from person to person.Human excreta is the source of most diarrhoealpathogens and handwashing after contact withhuman excreta is probably the single mostimportant moment at which hands should bewashed with soap7. A recent review of all theavailable evidence suggests that handwashingwith soap could reduce diarrhoea incidence by42-46 percent and save at least one millionlives8.
Though the evidence base is weaker, similararguments apply to Acute Respiratory TractInfections, the number 1 killer of children. Handsare also a vector of ARI transmission. A numberof studies suggest that handwashing could bevery effective in reducing the incidence ofclinical cases of ARI9.
While soap is found in most households, it isoften reserved for washing clothes, dishes andbathing. Handwashing with soap is not commonthough practice varies from country to country.For example, a study in urban Burkina Fasoobserved only one percent of mothers using soapto wash their hands after using the toilet, and
only 18 percent after cleaning up a child’sbot tom10. In rural Niger ia, s t ruc turedobservations by Omotade showed only 10percent of mothers were using soap to wash theirhands after cleaning up a child11. In slums inLucknow, India, 13 percent of mothers wereobserved using soap after cleaning up a childand 20 percent after going outside to defecate.Handwashing practices can also be poor inmore developed countries; one UK study showedless than half of mothers used soap afterchanging a dirty nappy12.
Programs to prevent diarrhoeal diseases havelost momentum over the past years. Whilstmany new initiatives on AIDS, malaria and TBhave been announced, the diarrhoeas remainorphan diseases. There are three main reasons:
• Responsibility for combating the diarrhoealdiseases has been split between Ministriesof Health, Water, Environment and others,and as a result, has been championed bynone.
• Advocacy has been flagging, possiblybecause the diarrhoeal diseases are anunattractive, dirty topic, competing poorlyfor political attention with other hot healthproblems, such as HIV.
• Interventions to prevent Intestinal diseaseshave proven more complex and problematicthan expected.
Control of Diarrhoeal Diseases (CDD)programs in Ministries of Health worldwide are
6

flagging. Participatory methods that arecommonly found associated with water andsanitation programs may be effective atimproving hygiene on a small scale, but areunlikely to provide a feasible approach tocovering large populations. Handwashingneeds to be tackled on the scale of vaccinationprograms, where population coverage isalmost total. For this breadth of reach, socialmarket ing s ty le approaches based onadequate formative research into risk behavior,context and motivation are most appropriate.The skills and resources of both the public andthe private sector are needed if handwashingis to be promoted successfully on a wide scale.
However these issues are not widelyunderstood. The first condition for a successfulPublic Private Partnership for Handwashing isinvestment in dissemination and advocacyamongst decision makers.
Programs to prevent diarrhoea that are not onlydemonstrably effective, and cost-effective, butalso attractive and eye catching, are neededi f more suppor t for eradicat ing thesepreventable killer diseases is to be forthcoming.
Why a Public Private Partnershipfor Handwashing?While the public and private sector havealways worked together in one way or another,the idea of a direct partnership is relativelynew. Governments have contracted out
services to the private sector or handed overresponsibility entirely via privatization, but onlyrecently has the idea of joint programming withjoint responsibility become a reality. Over thelast ten years Public Private Partnerships in thehealth sector have been used to:
1 develop and facilitate access to vaccinesand treatments;
2 promote behaviors and products that reducedisease occurrence and
3 improve health services.
Examples include Roll Back Malaria and GAVI( the Global Al l iance for Vaccines andImmunization). A review of practice in healthPublic Private Partnerships can be found athttp://www.wsp.org/english/activit ies/handwashing/bestpractice.pdf
A partnership should pool resources and riskand provide added value over and above whateach party could achieve alone11. Clearly,partners will only join a partnership if theys tand to gain f rom i t . In the case ofhandwashing, there are obvious benefits toboth sides; industry may sell more soap, whilstGovernment benef i t s f rom the pr ivatesector’s expertise in designing effectivecommunications to improve public health.Table 1 (on page 8) summarizes the potentialincentives and contributions of players in aHandwash Public Private Partnership.
3.0
3.5 Leading Infectious KillersMillions of deaths, worldwide, all ages,1998
Acute respiratoryinfections (including
pneumoniaand influenza)
AIDS*
Dea
ths
in m
illio
ns
Diarrhoealdisease
TB Malaria Measles
2.32.2
Over age five
* HIV positive people who died with TB have been included among AIDS deathsSource: WHO 1998
Under age five
1.5
1.1
0.9
2.5
2.0
1.5
1.0
0.5
0
Fig 1
7
“The primarymotivation for
Colgate-Palmolive isthat a Public Private
Partnership onhandwashing is in
natural harmony withour value systemwhich is three-pronged: care,
continuousimprovement andglobal team work.”
Diana Grina, Global Director,Professional and Government
Relations, Personal CareProducts Colgate-Palmolive,
WashingtonMay 2300
http://wsp.org/english/activities/handwashing/
workshop.pdf

Table 1 Possible incentives and contributions for public/private players in theHandwash Public Private Partnership
Industry Public Sector
Benefit
Contribution
■ Enhanced image as a globalcorporate citizen, enhancing brandequity
■ Staff motivation and retention■ Influence in development and
Government circles■ Insight into future markets■ Access to national and international
research and knowledge■ Access to public infrastructure to
stimulate markets
■ Better services with higher coverageleading to improved health, which,in turn, assists economicdevelopment.
■ Liberation of resources for otherpriorities
■ Learning about consumer research,marketing and communicationmanagement
■ Understanding clients as consumers
■ Professional expertise in:- Marketing- Communications planning- Consumer research- Communication management- Product tracking- Product development
■ Resources
■ Catalyst role■ Legitimacy/Institutional home■ Resources■ Knowledge of target markets■ Facilitate regulatory environment■ Best practices and global vision
There are of course some costs for each partnerin joining a Public Private Partnership. For thepublic sector, these may include loss ofcredibili ty through association with bigbusiness, and potential loss of investment if theprivate partner decides to drop out. Costs tothe private sector are mostly in the diversionof human resources from more immediatelyprofitable activities. As the BASICS review6
points out, program managers in industry arehuman, they make decisions mainly on solidcommercial grounds, but can often be swayedby the desire to ‘do the right thing’.
Public Private Partnerships in the health sectorprobably work best where there is a closealignment between the objectives and activitiesof the two partners (BDP 2002). Selling soapand promoting handwashing are two suchclosely aligned activities.
The soap marketThe world market for soaps and detergents wasworth US$88billion in 2000, having grownby 29 percent since 1996. The market is
dominated by a small number of multinationalcompanies with strong brand identity andenormous adver tising budgets. There iscut throat compet i t ion between thesemultinationals. The top global players includeProcter and Gamble, Unilever, Colgate-Palmolive and Johnson & Johnson. Importantregional players include Beiersdorf in Europe,the Kao Corporation in Asia-Pacific, PatersonZochonis in Africa and Nirma and Godrej inSouth Asia. Procter and Gamble is the world’s21st largest company valued at $116billion,Unilever the 62nd, (worth $56billion) Colgate-Palmolive is the 141st ($31billion), Kao, the405th ($11billion) and Beiersdorf the 454th($10billion) (Financial Times, 10 May 2002).Whilst Johnson & Johnson is the world’s 9thlargest company, soap forms a minor part ofthe portfolio. These companies, along withhuge numbers of medium and small-scale soapproducers, provide soap to almost everyhousehold in the world.
In developed economies, market expansion isat t r ibutable mainly to new product
8
“We are goodcorporatecitizens.”
Procter and Gamblemission statement
http://www.pg.ma/page12.html

developments, such as l iquid soaps forwashing hands and showering, supported byheavy media advertising and promotionalactivity. Because the market for soap productsis largely mature in developed economies anddisplays stagnant growth, global companiesare turning their eyes towards developingcountries or ‘emerging markets’. According tothe director of Unilever, catering to the needsof the poor is going to be a major source offuture market growth.
Factors likely to encourage growth in soapconsumption in developing countriesinclude:• Liberalization of markets and growth in free
trade.
• Phenomenal growth in the reach of massmedia, especially TV.
• Demand driven by the widening gapbetween how consumers l ive and theincreasing visibility of consumption.
• More educated and aware consumers.
• Increasing disposable incomes.
• Increasingly skilled advertising and marketresearch agencies.
• Improvements in t ranspor tat ion andcommunication networks.
• Growth of supermarkets and retail outlets.
• New technology enhancing productivity, makingproducts more attractive and reducing cost.
Soap, soap and more soapThere are many kinds of soap available onworld markets, in bars, flakes, powders, liquidsand pastes – which are used to remove dirtand stains from bodies, clothes, utensils,surfaces and hands. As a rule, the moredeveloped the economy, the more species ofsoap will be found in the cupboards ofconsumers. In an evolved market there is aspecific soap product for every surface, whilstin an emerging market, one bar of laundrysoap, which may be locally or domesticallyproduced, can serve all purposes.
Soap is present in most households in the worldand is a priority purchase, even for thepoorest. In order of impor tance to theconsumer, keeping clothes clean is the first useof soap products, bathing the body the secondand cleaning utensils the third. Handwashingcomes far down the list of priorities.(http://wsp.org/english/activities/handwashing/globalmarketsoap.pdf)
Whilst technically adequate for cleansinghands, bar soap has been largely displacedby liquid soaps for handwashing in Northerneconomies. There may be an equivalent growthpotential in the marketplace for a cheap soapdesigned specifically for handwashing inemerging markets.
The next chapter explores the lessons that werelearnt from the country programs.
Part 3The Approach Step-by-StepOnce the overall concept and vision had beenelaborated and the technical team mobilizedin London and Washington, activities movedto the country level. Seven steps, as set outbelow, were followed in each country. Afurther three steps remain to be taken to reachfull-scale implementation. The process ofpartnership building is similar to that followedby the BASICS initiative in Central America,though in the examples given here thecatalysts were based in quasi governmentinstitutions, whilst in Central America theywere independent). Lessons learnt are shownin italics.
Step 1 InitiationThe Public Private Partnership for Handwashingconcept was presented to potential stakeholdersin Ministries, NGOs, community groups, industrialassociations and external support agencies toraise interest and gauge support. In India, thisprocess began with a one-day workshop, whilea series of meetings were held in Ghana.
• Meetings need to be repeated since not allkey stakeholders can be present. Not allpartners come on board at the same speed.However, agencies that come to the firstmeetings may find follow-up meetings coversimilar ground for the sake of newcomers.
9
“For Unilever,corporate social
responsibility is anintegral part of ouroperating tradition.It is at the heart of
our CorporatePurpose and isreflected in our
Code of BusinessPrinciples. We
believe that thesecommitments are
not just anexpression of our
values, but that inliving them out they
contribute to oursuccess.”
www.unilever.com

• Representatives from Industry may not attendopen meetings but have to be visitedindividually.
• People at the top of key institutions shouldbe approached early on as they legitimisethe participation of their staff.
• Surprisingly few partners had (or voiced)ideological objections to the Public PrivatePartnership. There were, nevertheless, someconcerns that the initiative might appear toprovide ‘easy’ benefits to the private sectorby promoting their products for them.
• The backing by the WB/WSP gave playersconfidence that intentions were serious.
• Other international agencies such asUNICEF and DFID, that had been workingin hygiene promotion, showed interest intying this into their ongoing work.
• Key skil ls required at this stage werepolitical championing from WB/WSP staffand persuas ive communica t ionsconcerning the potential benefits of theinitiative. The involvement of academicshelped validate the case for handwashing.Champions had a l so to be ab le tounderstand both sides sufficiently to beable to ‘translate’ between the differentpublic and private cultures.
Step 2 Assignment of focal personThe local agencies housing the initiative werethe Kerala Rural Water Supply and SanitationAgency and the Communi ty Water andSanitation Agency in Ghana. Both are donorsupported and semi-autonomous. Both have amandate to work on water, sanitation andhygiene and both are struggling to developeffective hygiene promotion programs. The localagencies arranged for the assignment of a keyperson to lead the initiative from within theiragency (Kerala) or as a consultant (Ghana).
• Existing agencies have full workloads:addit ional help to set up a new andsubstantial work program is needed earlyon.
• Management needs to be persuaded of theneed to hire and resource consultants orassign competent staff. This can requirerepeated efforts.
• Key attributes of the focal person are:communications skil ls, familiarity with
government and business s t ructures,knowledge of hygiene promotion, well-regarded professionally, ability to opendoors at a high level, ability to conduct/oversee research and a lot of energy anddrive.
Step 3 Information collectionDevelopment of the initiative requires that it fitwithin the institutional and programmaticenvironment in country. One of the first tasksof the focal person was to identify keystakeholders including industrial players, tradeassociations, ministries, external supportagencies, NGOs, and organizations capableof carrying out consumer and market research.Agencies involved in hygiene promotion werecontacted and briefed about the work.
• Information collection helped identify allpotential partners who could participateand/or benefit from the program.
• The proposal for the Publ ic Pr ivatePartnership was well received by almost allstakeholders.
• A specific directory of contacts for programsshould be created and maintained.
Step 4 Formation of SteeringCommitteesStakeholders from ministries, industry and NGOswere invited to form a steering committee. Thesemet about every four months or at criticaljunctures. They reviewed progress, advised onplans and had a legislative role in monitoringcontracts. In addition, in Ghana a technicalcommittee was formed to help advise onconsultant selection and other technical issues.
• Steering committees confer legitimacy andallow continued advocacy as personnelchange. They help get all stakeholders onboard and keep them involved.
• They offer a forum for public and privateemployees to meet and exchange views.
• They are flexible and informal in thispreparatory stage, but their role may needto be formalized as programs begin.
• In Kerala, a MoU was signed between thesoap industry association (ISTMA) and theGovernment of Kerala to provide aframework under which to operate.
10

Step 5 Design and implementationof studiesTwo studies were commissioned in eachlocation. The first, a consumer study, wasdesigned to provide an understanding ofhandwashing behavior that would help toinform the design of the communicationsprogram. Key questions to be answered were:What is the current rate of handwashing withsoap at cr i t ical t imes? What are thecharacteristics of the target audiences? Whatmotivates handwashing with soap and whatare the barriers to its adoption? What channelsof communication are most appropriate?Secondly, market studies were commissionedto understand the state of the market for soapin each location. The results of these studiesand the technical issues they raise arediscussed in more detail in the next section.
• Consumer studies must be carried out byprofessional market/consumer researchagencies, if their results are to be credibleto industry.
• Some research agencies divide their staffinto commercial and social project teams.In such instances, the commercial teamsshould be preferred, for reasons similar tothe above.
• Industry should be involved in the design ofthe consumer studies from the outset.
• Key skills required were an understandingof hygiene behavior and knowledge offormative research design.
• Studies required a lot of work in briefingand training the agencies as well as indebriefing and collaborating with them inthe production of the final results.
The market studies were commissioned to allowthe public sector to better understand the natureof the soap market. They were designed to findout about total volumes of soap, suppliers andbrands, soap used speci f ical ly forhandwashing and exist ing promotionalstrategies. They aimed to offer the public sectorpartner sufficient insight into the operation ofsoap industry to enable them to negotiate agood deal with industry.
• Again, if they are to be credible, such studiesmust be done by professional agencies withexperience in accessing and interpretingsuch data.
• It is hard to gauge how much artisanal soapis produced, and how much is sold throughunofficial channels without a detailed fieldstudy.
• The results of such studies are only as goodas the brief and the demands from the client.Commissioning such studies requires skills thatmay not be readi ly avai lable. Again,assistance from professionals in industry maybe one solution to getting good design andhence good results.
• Study designs have to take into account theresearch capacity of the professionalagencies, which may not be equal lydeveloped in all countries.
• It remains to be seen whether the publicsector will use the studies as expected.Detailed Market Studies might not beessential for future Handwash Public PrivatePartnerships.
Step 6 Design of the HandwashProgramAn outline design for the handwashingcommunication program based on pastinsight, available data and the consumerresearch, was prepared by industry in Keralaand by the Public Private Partnership team inGhana. While the plans had to be detailedenough to meet the administrative needs ofpotential funders, a great deal of work wasstill required in designing and testing thedetai led communications package. Forexample an effective TV advertisement mightrequire the equivalent of five years of workby senior marketers. Detailed messages andmedia for direct contact have also to bedesigned and tested. Project preparationproceeds iteratively.
Possible steps would be to:1 prepare an outline design;2 secure funds and determine institutional
roles;3 prepare a detailed design using professional
creative teams and agencies;4 proceed to testing of concepts, reframing,
testing again, testing effectiveness;5 finalization of communication package; and
then6 full-scale roll out.
11

Neither program envisages us ing anyestablished brands. However, some form ofnew generic handwash brand may be neededto make the campaign ef fect ive andrecognizable. The par tners would alsowelcome companies piggy-backing their ownindependent branded handwash campaignsonto the partnership initiative if they so wish.
• All communicat ion s t rategies requiredetailed trial and testing for effectiveness,otherwise the investment may be lost.
• Generating a new behavior requires at leastsix effective contacts a month. Drip-dripapproaches are not effective because thecritical mass that can effect a change inhabits is never achieved.
• Key skills needed are marketing, mediaplanning and consumer science, these aregenerally not available in the public sectorand were provided by industry.
• Indust ry is wel l p laced to designcommunications programs; they haveinvested hugely in developing their ownexpertise in consumer insight, messagedesign and media planning.
• There is scope for the private sector tocollaborate and explore the great potentialfor effective communication using publicsector information channels.
Step 7 Resources for the HandwashProgramProject design and financing have to move instep. The outline design for the handwashprogram has to be appropriate to therequirements of potential funders. Whilstindustr y can often make major fundingdecisions on thin documents, external supportagencies and Governments require detailedbackground and justification, complete activityplans, logframes, etc. It may be hard to provideall the detail at this stage because commitmentsof funds are required before the detaileddesign can be produced.
For the Kerala program, both the State andIndian Government were ready to contributevery substantially to the costs of the program.Getting funds committed from external supportagencies has been more difficult, largelybecause they are tied up in existing projects,and the funding cycle can take several years.
• It can be hard to sell an outline design to
potential funders, who may be expecting tosee the full program design.
• However, having access to the results of theconsumer research helps show howprograms are designed to cater to localcircumstances.
• Industry does not have major funds availablefor use in non-branded campaigns. However,their input in communications expertise,access to creative and media planningagencies, methodologies for developing andtesting approaches and in management skillsprogram is critical.
• External support agencies funding may notbe available through existing channels or ina useful period. The project should be offeredto as many donors as possible, and the initialapproach should be to senior decision-makers. Networking with agencies at headoffice level can assist.
• Key skills needed at this stage are insightinto, and access to, the bureaucracy ofGovernment and external support agencies.
• Fund-raising is an on-going process and itmay be necessary to plan a multi-yearintervention and raise funds sequentially asresults are achieved.
• A cost-benefit analysis is useful in marketingthe proposed program to potential funders.Additional preliminary research on theeconomic benefits would also be useful.
Step 8 Baselines and M&EindicatorsThere is no per fect way of measur inghandwashing practices. Many options havebeen tried but all have drawbacks: responsesto direct questions bear little relation to reality,measuring soap use does not distinguish theother uses of soap and structured observationis time-consuming, intrusive and expensive.Never theless, s tructured obser vation isprobably the best tool avai lable13 formonitoring changes of behavior patterns in apopulation. Monitoring soap consumption canprovide additional evidence for programeffectiveness, though any changes detectedmay not be due to the program interventions.Program performance indicators, in terms ofcoverage and audience recall give furtherindicators of progress.
12

As trial programs, these two initiatives will beespecially closely monitored and data collectedfor cost-effectiveness analysis. Preliminarycalculations from Kerala suggest that theprogram will pay for itself in two years bysavings in health care costs. In Ghana, savingsfrom reduced disease will be in the order oftwice program costs.• Work is still needed to find and validate
indicators of handwashing behavior forbaseline monitoring and evaluation.
• Ideally, the consumer study should providean opportuni ty to col lec t basel inehandwashing data. The methodology has tobe watertight enough to provide credibleresults, whatever the circumstances. This ishard to do and requires further work.
• The Monitoring and Evaluation programwould focus on measur ing behaviorimprovements related to handwashing, theeffect iveness of different interventionstrategies, and where adequate data exist,the impact of the program on diarrhoealdisease reduction.
• Given the likely high cost of such programs,data will need to be collected for theevaluation of cost-effectiveness.
Step 9 Detailed design and test ofcommunications approachesThis step is yet to be completed in Kerala andGhana. Once funding and management is inplace in the project cell, detailed programdesign will begin. Creative agencies will bebriefed, and a variety of ads will be sketchedout for radio and TV, as will concepts for postersand kits for schools and health centers, andsupport materials for partners. These will betested on a small scale with samples of the targetaudiences. Those that are deemed most effectivewill be refined and retested. Finally, all printand audiovisual materials will be commissionedand produced for full-scale roll out.
Step 10 Launch and executecampaignsWhen funds are in place and when testing hasbeen carried out, the programs as a wholecan be launched.
The Global PartnershipAt the same time as work was progressing atcountry level, tentative steps were madetowards bui lding a global par tnershipplatform. Interested parties from WSP, WorldBank, UNICEF, USAID, EHP, BASICS and theLSHTM met together four times over the yearand a number of preliminary meetings withglobal soap companies were also held with aview to establishing a global group. Inaddition, annual technical meetings at theWorld Bank have provided opportunities forexperience sharing and dissemination.
• Contrary to expectation of the need for agovernance s t ructure wi th ru les andprocesses, no such role for a globalorganization was identified.
• Meetings of global groups should only beorganized in response to a clear need, asthey are expensive and have opportunitycosts for busy sector professionals.
• One advantage of such meetings is that headoffices of international agencies can leadcountry offices to support the initiative.International media exposure can be helpful,though it is not possible to control exactlywhat will be said. An article on the initiativethat appeared in ‘The Economist’ galvanizeda lot of support but failed to describe theroles of all partners.
• Some partners at the global level who wouldvery much like to be involved in the initiativeare constrained by a lack of resources thattheir agency can bring to the table.
• The role of a global partnership platform willcontinue to be reviewed as the initiativespreads to other countries.
• Annual or biannual technical meetings serveto share experience, advocate anddisseminate the approach.
The approach: Key lessons• Setting up a Public Private Partnerships takes
a great deal of time, and requires majorinvestments in communication at all levels.Partners take time to learn the capabilitiesof each other. For example: industry did notrealize how much Government was capable
13

of in terms of direct contact with thepopulation, Government did not realize thecomplexity and difficulty of behavior changeor that professional marketers had so muchto contribute.
• Building trust is a slow and cumulativeprocess. As money began to be spent bypartners and their backers, confidence in theseriousness of each other’s intentions grew.
• Champions: Committed individuals have
played major roles in getting the PublicPrivate Partnerships off the ground at everylevel. The individuals have to like and respecteach other if motivation and energy levelsare to remain high.
• Time scales differ: Industry can expect tomake a decision and have a program upand running in a matter of months; forgovernment the time horizon may be a year;while for external support agencies thefunding cycle may be three years. Industry,in particular, may not be prepared to wait iffunding negotiations drag on.
Roles of the partners in the Handwashing Public Private PartnershipFig 2
PP P
Government• Health, social welfare
and educationalinfrastructure
• Local-level institutions• Resources and expertise
Scientific community• Defining scope and thrust
of the program• Credibility• Knowledge capture and
dissemination
External SupportAgencies
• Financial resources• Past experience
Private Sector• Crafting communication
for behaviour change• Program design and
control• Optimising resources
across channels andmedia
Understanding Handwashing with SoapPart 4
Handwashing behavior is complex. This factcame as a surprise to some partners whoassumed that getting people to wash theirhands was a simple matter of telling peoplethey would get sick if they didn’t do it. Fourkey questions about handwashing behaviorhave to be answered:
• What are current handwashing practices?• Who should the target audience of the
programs be and what are their characteristics?• What factors motivate, facilitate and hinder
handwashing?
• What channels of communication reachtarget audiences effectively?
The consumer studies were designed to answerthese questions. They used methods drawnfrom social and consumer research, includingstructured observation, in-depth interviews,focus groups and behavior trials. They eachtook around six weeks, cost an average of$35,000 and covered between five hundredand a thousand households, selected torepresent the whole state/country. Mothers,fathers, children and schools were targeted.
14

In Kerala, the Indian Market Research Bureau(IMRB), and in Ghana, Research International(RI) did the detailed design, the fieldwork andthe preliminary analysis, in conjunction withthe client organizations (KRWSA and CWSA).Some assistance was provided by the LSHTMand from industry. Both agencies did well in afield unfamiliar to them, though both requiredconsiderable help and guidance. The studieswere commissioned before industry was fullyon board. More industry input at the designand execution stage could have added valueto the studies.The following give some of the preliminaryfindings from the two studies.
Current handwashing practicesMeasuring handwashing behavior is complexand diff icul t. Both teams used the best
Handwashing withsoap by mothers Ghana Kerala
After usingthe toilet 37 % 42 %
After cleaningup a child 31 % 25 %
Before eating 16 % 11 %
Before preparingfood N/A 10 %
Observed handwashing practices in Ghana and KeralaThe results of the studies proved controversial and highlighted the need for an agreedmethodology, acceptable to all, for measuring handwashing. Closer examination of themethodology adopted in both locations suggests that many non-handwashing events weremissed, for example, when defecation took place away from the house. Structured observationrequires careful introduction so as not to bias results and much patience and supervision.Some of these safeguards may have failed in either or both studies. Alternatively, handwashingwith soap after contact with excreta may actually be higher than was predicted. More carefulmeasures of handwashing to provide a reliable baseline are needed, otherwise changes overthe time of the intervention cannot be measured accurately.
Handwashing at key times other than after defecation and cleaning up a child is poor andthese occasions could also be the focus of attempts to improve handwashing. A weightedaverage of handwashing with soap in Kerala at different critical times suggested that soapwas only used on about 14 percent of these occasions.
In Kerala, hands were washed with soap more often when water was available in the toilet orwhen soap was available in the toilet. In better-off households separate soaps were kept forseparate purposes (bathing, cleaning clothes, for menstrual stains) and all households usedspecial soap, (e.g. Johnsons’ baby soap), for a new baby. Soaps claimed to be used forhandwashing were all beauty soaps, not laundry soaps. Commonest brands mentioned were:Lexus Gold, Nima Rose, Lux and Santoor. The monthly amount claimed to be spent on soapdid not vary much between social classes. In over half of households, the father purchasedsoap, but mothers chose the brand. One hundred percent of households had soap on the dayof the interview.
The Kerala results showed that those who did not use soap to wash their hands after using thetoilet reported diarrhoea five times more often than those who did.
Both studies concluded that poor disposal of children’s stools (often thrown in the yard, on anopen rubbish heap, in a field or drain) could be a source of the faecal pathogens that causechild diarrhoea. One option may be to add this issue to the program at a later date, once thehandwashing message is well established.
15
approach available, structured observations,which required trained observers spendingthree hours in the early mornings watchingwhat happened in courtyards and households.Both teams found higher than expected ratesof soap use by mothers after using the toilet.

Target audiencesBoth s tudies concluded that women ofchildbearing age and children were theprimary target audience; mothers because theywere the principle caretakers of children andpreparers of food, and children, because theywere at an age where handwashing habitscan be inculcated for life. In Kerala, men havealso to be targeted, because they are theprinciple buyers of soap, though womennormally specified the brand. In Ghana,women usually buy the soap but may have tonegotiate a budget with their husband.Previous studies have indicated that life-change events, and particularly the time ofthe arrival of a new baby, are particularlygood opportunities to introduce new habits.
Motivation for handwashingThe qualitative research in Kerala found thatcleanliness was very important to mothers.Figure 3 schematizes how the dirtiest jobs aresaved up until just before the midday bath.Following this, a woman will typically try tostay clean for the rest of the day.
Hands tended to be washed with soap whenthere was a cue. The cue might be a smell;from cutting fish, touching animal dung ordiarrhoeal faeces; something visible such asthe sight of dirt; or a feeling, such as having
been in contact with a poison or an impuritylike non-vegetarian food, or before prayer; ora sense of stickiness. One’s own and one’schildren’s faeces do not bad smell and thereforemay not cue soap use.
The research divided people into habitual usersand non-users of soap after faecal contact.Users seemed to practice what they had alwaysdone since childhood in a mechanical fashion.Habitual users felt dirty if they did not use soapafter faecal contact, whereas non-users did not.Non-users explained that they never had thehabit, they often did not have time, or soapnearby. Another group of users took up thehabit after having a baby. They explained thatkeeping a baby clean nurtures its mental andphysical growth as wel l as i t s heal th.Handwashing with soap is a closeted subject,not seen or talked about, therefore themotivation of social contempt for those withdirty hands is absent.
In Ghana, hands were washed with soap toremove dirt, oil or an unpleasant smell, toprevent diseases and to appear neat. Thedisgust of having been to a dirty public toiletoften cued the use of soap. However, if soapor water was not to hand, hands were lesslikely to be washed. Soap was often storedaway to keep it from being used by others,which made it inaccessible for handwashing.
The pyramid of cleanlinessFig 3
Sweeping courtyard
Cleaning house,vessels, cooking
Cuttingcleaning fish
Handlingcow dung
Cleaninglaterine
Bath
Low dirtNumerous/varied tasks
High dirtspecific tasks
Becoming clean andstaying clean
KRWSA PQR
16

The soap habit
“There are no particular reasons for notwashing hands with soap, it is just thatwe don’t do it” (India Palghat-B-NU)
“Our parents never taught us this”(India Trichur-S-NU)
“Nobody has made us understand thebenefit of washing our hands with soapafter using the toilet” (India Trichur-S-NU)
“How wil l the outside people knowwhether we wash our hands or not?” (IndiaIdd-B-TU)
“My children normally use the soapindiscriminately so I hide it from them andthat saves me money.” (Ghana Ga-rural)
“When we put the Key soap under the bedit makes the soap very hard and it makesit last longer. We also put it there becausewe want to prevent the children fromhaving access to it.” (Ghana Western Region-urban)
“Some of the children tend to eat soapwhen they see it, but if I have hidden itthey could not see it and that will save mefrom trouble.” (Ghana Ga-rural)
“Caring for our children is the mostimportant thing and is of great concern tous as mothers... ...Bathing, cooking andwashing of their clothes is what we meanby caring for our children. You as a mothershould make sure your child dresses neatlyand should be well fed.” (Ghana Ga -rural)
“Looking at things, you see that bothmother and child always look cheerful andheal thy when they are neat.”(Ghana Accra -urban)
“Whenever my child goes on a visit to mysister’s place, his friends do not want himto leave because he is always neat.”(Ghana Accra -urban)
This was especially true in schools. None ofthe rural schools had handwashing facilities.Only one school of 20 sampled had runningwater. The ideal soap for handwashing wassaid to be small enough to handle andpreferably in liquid form to make it easy touse and to restrict its usage to handwashing.
Care for children was one of the strongestmotivators for handwashing in both locations.
Whilst pump-dispensed products are beyondthe reach of poorer consumers in developingcountr ies, cheaper products, designedspecifically for handwashing could have realpotential for growth. (Soap on a rope or in anet to hang in a toilet, small tablets or threadsof soap, tubes or tubs of liquid soap, recyclablecontainers for liquid soap). In Ghana, somemothers even pounded up the soap that wasprovided in behavior trials to make a liquidsoap for hand washing.
Handwashing was not generally hindered bylack of water or soap. However, the problemof where to keep the soap free f rominterference was a major problem in thebehavior trials in Ghana.
Channels of communicationBoth studies were charged with mappingchannels of communication from the householdperspect ive. Combined wi th nat ionalcommercially available figures, this dataprovides the basis for calculating the reach ofthe handwash program when designing themedia mix. Figure 4 (on page 18) shows typicalcommunications routes into a Kerala village.In Kerala while more than half of the householdshad TV, many Muslim women did not watchfor religious reasons. Two thirds of householdshad working radios and over a third readnewspapers and magazines regularly. Whilstdata on mass media use is readily availablefrom national surveys, data on contact with theexisting health system and any other localchannels of communication is often notavailable. In Kerala, the 98 percent success ofthe pulse polio program showed that a programusing the existing health, immunization,anganwadi and education system could havea major impact on target populations.In Ghana 55 percent of urban households and24 percent of rural households had TV. TheKeysoap ad was the most popular TV ad, citedby 38 percent of women. Over a half of womenand three quarters of men listened to the radioevery day.
Complex studies such as these operate at thelimits of the capability of research agencies.There is a temptation to take the opportunitythat such studies offer to add on further issues.
17

However, this can dilute the quality of thewhole exercise. Ways need to be found tosimplify, and certainly not complicate, suchformative research.
ImplicationsThe preliminary results from the studies suggestthat handwashing is a complex practice thatis carried out for a number of reasons. Thesereasons can by physical (‘I see/feel/smell dirton my hands’) and metaphysical (‘I feelunclean/ pol lu ted/ disgusted/ dir ty ’ ) .Cleaning hands with soap serves to refresh,rejuvenate, and contributes to a sense of well-being. Fear of disease and germs may alsoplay a part in the decision to wash hands, butonly a part. Full results will be posted on thewebsi te h t tp://www.wsp.org/engl ish/activities/handwashing/
The outline designs of both programs were builton the preliminary results of the consumerstudies. The detailed design is an on-goingprocess that will revisit the study data for moreinsight into specific issues. Ideas generated byboth studies will be tested with consumers.
The programs wi l l use s tate -of - the -ar tcommunication design approaches and delivermessages via mass media and direct contact
through existing public services. In Kerala, theprogram will target those life change eventswhen new behaviors are most likely to beadopted such as the arrival of a new baby orvaccination. Change will also be enforcedthrough the addition of a handwashingprogram to the midday meals program inprimary schools. Mass media and directcontact together have additive and synergisticeffects. Media will be generic with no companylogos. Interestingly, industry is keen not to beseen to be associated with the handwashinitiative because they expect Governmentsponsored health messages to be more crediblein the eyes of the consumer. However, a newnon-commercial ‘brand’ may have to becreated to add coherence and recognition tothe program.
Calculations for Kerala suggest that 70 percentof households will be reached 43 times a yearvia mass media and 35 percent of householdsnine times a year through the Direct Contactprogram. To achieve this density of contact isexpensive. The initial cost estimate for Keralais $10million spread over three years to coverthe whole state. The outline design for thecommunications program can be viewed athttp://www.wsp.org/english/activit ies/handwashing
Range of influence on a Kerala village that can potentially be harnessedFig 4
Development of womenand child program 51%
Intergrated rural develop-ment program 57%
Community TV 62%
Community centre 40%
Fair price shop 91%
Retail shop 67%
Milk cooperative 67%
Primary school 90%
NGOs
Bank 89%
Local panchayatsAanganwadis 96%
Secondary school 74%
Adult education centre58%
Primary health centre74%
Health sub-centres 79%
Private doctor 88%
Village health guide 38%Traditional birth attendant49%
Post-office 89%
Middle school 87%
Target village
* All India-Rural % - NFHS-2, 98/99
18

■ Handwashing behavior is complex■ Measuring handwashing behavior is difficult■ Formative research study designs should be further simplified to provide a clearer focus,
and training and supervision require substantial international inputs.■ Keys to behavior change are likely to be i) making people feel that they have something
on their hands after defecation; ii) making it easier to wash hands by having soap tohand; iii) targeting life change events.
■ The study results need further detailed analysis, both for the insights they offer into thedesign of each program and to increase the knowledge base about handwashing.
■ To generate a behavior change, industry specialists believe that effective contact with themessage in the mass media has to be made at least six times a month. Drip-drip strategiesdo not provide the critical mass of stimulus needed to change habits.
■ Communications programs will be non-branded and use both mass media and direct contact.■ Industry involvement at the design and execution stage of the studies would have added to
their value.
Key Lessons
Future Challenges, Conclusions Part 5
Future challengesOne year on, the idea of the Public PrivatePartnership for handwashing is well and trulylaunched. However, as we move towardsreplication in other countries, challenges remain:
Single or multiple industrial partnersAs a matter of principle, this Public PrivatePartnership is kept open to all industrial playerswho want to join. All key players in both largeand small-scale soap production were contactedeither directly or via industry associations. InKerala, the partnership remains formally with theindustry association, though we have foundourselves working mainly with just one partner,the dominant player: Unilever. Though small andcottage industry representatives are on thesteering committee, their participation has beenlimited. Full participation is relatively more costlyfor small players. In Ghana, there are threeindustrial partners, two large and one small-scale,and individual companies and industryassociations form part of the steering committee,though Unilever still plays the biggest role. Itshould be noted that the results of all the researchwill be in the public domain and smaller players
will, at least, benefit from this exercise. As TomClasen points out14, multiple partnerships can bedifficult and complex and there are manyprecedents for engaging with single companiesin public-private partnerships. Single partnershipsmight prove the most effective use of publicresources. For the moment, the basic principlesof transparency and openness to all partnersremain non-negotiable as this initiative moves toother countries with other major industrialpartners.
Overall costsPrograms designed to effect behavior change ona mass scale are likely to be expensive, requiringboth mass media and direct consumer contact.Current estimates are in the order of $0.10 perhead of the population per year. However,savings in reduced health costs, and lost workingdays can more than compensate for thisexpenditure. In Kerala, the program will pay foritself after two years; in Ghana likely savingsamount to twice the estimated program costs.Donor agencies may find the idea of spendingmany millions on handwashing surprising, andmay be more amenable to phased approacheswith a year-on-year incremental approach. The
19

private sector needs to see a business plan thatcan reliably change behavior in whole targetedpopulations in a reasonable period if they are toremain interested. Bridging these two perspectivesis difficult, and compromise on the large-scaleobjectives may not be advisable, if the programis to produce measurable results. A further costissue is the contribution that can be expected fromindustry. Industry can contribute only to the extentthat they profit from increased sales of soap,improved Public Relations and new learning.Current contributions in kind of about 25 percentof total program costs may or may not representa ‘fair’ contribution and negotiations continue inboth Kerala and Ghana.
Human resource capacityRecruiting the necessary personnel, bothnationally and internationally, proved verydifficult. People who can span industrial marketingand international public health are a rare breed.Bringing junior members of staff on board earlyand training them up may be one solution.
Measuring resultsMeasuring actual handwashing practice is acomplex task, as we have discussed. We hopethat the partnership with Industry will lead toinnovative new means of measuring the impactof the handwash programs. The Kerala andGhana programs will need to test a number ofapproaches if they are to be able to recommendthe most feasible and reliable. Involving outsideorganizations such as CDC and WHO will addcredibility to any results.
Other tasks for the Public PrivatePartnershipThough most work has been carried out onhandwashing promotion, in the long term greaterhealth benefits might be had through publicsupport for R&D into soaps designed specificallyfor handwashing, or through engagement withgovernments to reduce the unit cost of soap viathe tax burden on raw materials and sales tax. Itremains to be seen if this would translate into aserious price reduction.
A model for sanitation?There are parallels between soap and toilets, bothare consumer goods that are largely providedfor privately and both impact on environmentalhealth. This initiative began with the objective of
promoting both but, for the sake of clarity, thesanitation aim was dropped. However, thisapproach has many lessons to teach about howsanitation might be marketed in future.
Research needsHygiene and handwashing are poorlyresearched. More and better quality data isneeded on the impact of handwashing ondiarrhoeal diseases, respiratory tract and skininfections. Better indicators of handwashingpractice are required, and the learning from thetwo handwashing studies need to be distilled anddisseminated.
ConclusionsFrom a good idea and a vague plan, this PublicPrivate Partnership has found its feet and becomea concrete reality in two countries in one year.This is good progress for a new health programthat is to be delivered via a new paradigm.External champions who were prepared to pushhard were required to get this off the ground, butit still took a long time to do the talking and tobuild up the trust that was needed to forge aneffective partnership.
To be successful, international health programsmust not only be well founded, but also come atthe right time. This program exhibits acombination of:• A novel, attractive and mould-breaking idea• An intervention that should be highly effective,
that could save many lives and that we knewis doable.
• A potential for a win-win partnership of theskills and capacities of industry, Governmentsand external support agencies, at a time whenthe idea of Public Private Partnerships aresweeping into all spheres of public policy.
After a year of exploring the practical implicationsof trying to do such programs, the team is evenmore convinced that Public Private Partnershipsfor Handwashing have huge potential. Agencies,Industry and Governments in many countries areclamoring to join the initiative. The idea has takenon a life of its own and is beginning to influencepolicy beyond our immediate programs. Teamsfrom Industry, Governments, external supportagencies and academia are finding that they havecomplementary roles and skills and can worksurprisingly well together.
20

AED Academy for Educational DevelopmentARI Acute Respiratory Tract Infections
BASICS Basic Support for Institutionalising ChildSurvival
BPD Business Partners for DevelopmentCDD Control of Diarrhoeal Diseases
CWSA Community Water and Sanitation Agency(Ghana)
DFID UK Department for InternationalDevelopment
EHP The Environmental Health ProgramESAs External Support Agencies
IFH International Forum for the Scientific Studyof Home Hygiene
IID Infectious Intestinal DiseasesISTMA Indian Soap and Toiletry Manufacturers
AssociationKRWSA Kerala Rural Water Supply AgencyLSHTM London School of Hygiene and Tropical
MedicineORS Oral Rehydration SaltsORT Oral Rehydration TherapyPPP Public-Private-Partnerships
USAID United States Agency for InternationalDevelopment
WB The World BankWSP Water and Sanitation Program
References1 “Business Partners for Development. Putting Partnering to work.” London: Business Partners for Development, 2001.
2 Almedom A. “Recent developments in hygiene behavior research: an emphasis on methods and meaning.” Trop MedInt Health 1996;1(2):171-82.
3 Pinfold JV, Horan NJ. “Measuring the effect of a hygiene behavior intervention by indicators of behavior and diarrhoealdisease.” Transactions of the royal society of tropical medicine and hygiene 1996;90:366-371.
4 Curtis V, Kanki B, Cousens S, Sanou A, Diallo I, Mertens T. “Dirt and diarrhoea: Formative research for hygienepromotion programs.” Health Policy and Planning 1997;12(2):122-131.
5 Curtis VA. “Hygiene: how myths, monsters and mothers-in-law can promote behavior change.” Journal of Infection2001;43:75-79.
6 Saadé C, Bateman M, Bendahmane. D. “The Story of a Successful Public-Private Partnership in Central America:Handwashing for Diarrheal Disease Prevention.” Washington DC: BASICS, 2001.
7 Curtis VA, Cairncross S, Yonli R. “Domestic hygiene and diarrhoea, pinpointing the problem.” Tropical Medicine andInternational Health 2000;5(1):22-32.
8 Curtis V, Cairncross S. “Could washing hands with saop save a million lives?” submitted.
9 Ryan MAK, Christian R, Wohlrabe J. “Handwashing and respiratory illness among young adults in military training.”American Journal of Preventive Medicine 2001;21(2):79-83.
10 Curtis V, Kanki B, Cousens S, Diallo I, Kpozehouen A, Sangaré M, et al. “Evidence for behavior change following ahygiene promotion program in West Africa.” Bulletin of WHO 2001;79(6):518-526.
11 Omotade OO, Kayode CM, Adeyemo AA, Oladepo O. “Observations on handwashing practices of Mothers andEnvironmental conditions in Ona-Ara local Government Area of Oyo State, Nigeria.” Journal of Diarrhoeal DiseaseResearch 1995;13(4):224-228.
12 Curtis VA, Biran A. “Hygiene in the home: relating bugs to behavior.” Social Science and Medicine in press.
13 Curtis V, Cousens S, Mertens T, Traoré E, Kanki B, Diallo I. “Structured observations of hygiene in Burkina Faso, validity,variability and utility.” Bulletin of the World Health Organisation 1993;71(1):23-32.
14 Clasen T. “The public-private partnership for the Central American handwashing initiative: reflections from a privatesector perspective.” Trop Med Int Health 2002;7(3):197-200.
Acronyms

Water and Sanitation Program
The World BankWater Supply and Sanitation Division
1818 H Street, NWWashington, D.C. 20433
Telephone: (+1202) 4739785Fax: (+1202) 5223313Email: [email protected]: http://www.wsp.org
July 2002, 2nd Edition
Task Managers:Param IyerJennifer Sara
Author:Dr. Valerie Curtis
Contributors:Nana Gabrah-AidooB AshokSandy CairncrossPerry GolloEsther Monier IllouzYuri JainBaby KurianYaw SarkodieEbow SpioAnn ThomasJames Varghese
Created by Green Design AssociatesEmail: [email protected] by PS Press Services Pvt. Ltd.
Picture credit:KRWSA, Kerala, India.CWSA, Ghana.