
Health Facilit y Guidelines Australasian · PDF fileThis Health Planning Unit ... The term...
27
Australasian Health Facility Guidelines Part B - Health Facility Briefing and Planning 0540 - Paediatric / Adolescent Unit Revision 6.0 07 June 2016
Transcript of Health Facilit y Guidelines Australasian · PDF fileThis Health Planning Unit ... The term...

AustralasianHealth Facility Guidelines
Part B - Health Facility Briefing and Planning0540 - Paediatric / Adolescent Unit
Revision 6.007 June 2016

Australasian Health Facility Guidelines
Index
01 INTRODUCTION 401.01 Preamble 401.02 Introduction 401.03 Policy Framework 401.04 Description 5
02 PLANNING 602.01 Operational Models 602.02 Operational Policies 702.03 Planning Models 802.04 Functional Areas 802.05 Functional Relationships 9
03 DESIGN 1003.01 Access 1003.02 Parking 1003.03 Disaster Planning 1003.04 Infection Prevention and Control 1003.05 Environmental Considerations 1003.06 Space Standards and Components 1103.07 Safety and Security 1103.08 Finishes 1203.09 Fixtures, Fittings & Equipment 1303.10 Building Service Requirements 13
04 COMPONENTS OF THE UNIT 1404.01 Standard Components 1404.02 Non-Standard Components 14
AX APPENDICES 19AX.01 Schedule of Accommodation 19AX.02 Functional Relationships / Diagrams 26AX.03 Checklists 27AX.04 References 27
ATTACHMENTS 28Attachments 28
Part B - Health Facility Briefing and Planning Page 30540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
01 INTRODUCTION
01.01 Preamble
This Health Planning Unit (HPU) has been developed for use by the design team, project mangers and endusers to facilitate the process of planning and design.
The Paediatric / Adolescent Unit HPU was originally developed for NSW Health and issued for Australasianuse in 2006. This revision has been informed by an exstensive consultation process and included clinicalexperts and consumers.
01.02 Introduction
This HPU addresses Paediatric / Adolescent Units that are part of a general health service and not those indedicated children’s hospitals. Even so, the components of the Inpatient Unit, as described in the Scheduleof Accommodation, may be used as a 'building block' for major centres.
Paediatric intensive care services are only provided in designated children’s hospitals and requirements forthis service are described in HPU 360 Intensive Care Unit – General.
Paediatric specific facilities in emergency departments are described in HPU 300 Emergency Unit.
The term ‘family’ has been used throughout this HPU. This term refers to parents, relatives and other carers.
This document should be read in conjunction with AusHFG generic requirements including StandardComponents described in:
• Part A - Introduction and Instructions for Use;
• Part B - Section 80- General Requirements and Section 90 – Standard; Components, Room Dataand Room Layout Sheets;
• Part C - Design for Access, Mobility, OHS and Security;
• Part D - Infection Prevention and Control; and
• Part E - Building Services and Environmental Design.
01.03 Policy Framework
Prior to undertaking a project, planners and project staff should familiarise themselves with state and territoryspecific policies (as detailed in the Further Reading section of the Appendices), and with the followingpublications:
• Association for the Wellbeing of Children in Healthcare and Children’s Hospitals of Australasia,Charter on The Rights of Children and Young People in Healthcare Services in Australia;
• Association for the Wellbeing of Children in Healthcare, Policy Relating to the Provision of Play forChildren in Hospital, 2002;
• National Public Health Partnership, Healthy Children – Strengthening Promotion and PreventionAcross Australia. National Public Health Strategic Framework for Children 2005 – 2008, 2005;and
• Royal Australasian College of Physicians, Association for the Wellbeing of Children in Healthcareand Children’s Hospitals of Australasia, Standards for the Care of Children and Adolescents inHealth Services, 2008.
Part B - Health Facility Briefing and Planning Page 40540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
01.04 Description
DEFINITION OF A PAEDIATRIC / ADOLESCENT UNIT
The Paediatric/ Adolescent Unit describes a range of facilities to support the care of babies, toddlers,children and adolescents usually up to 16 years.
The Unit described in this document includes both inpatient and ambulatory/ day stay facilities. Thecollocation of these service components ensures a critical mass of skilled staff is provided and careenvironments suit the particular needs of children/ adolescents and their families.
The trend towards ambulatory care and shorter hospital stays for children has impacted on the configurationof Paediatric/ Adolescent Units. Inpatients are generally sicker and more dependent, requiring higher levelsof nursing care and observation.
There has been increasing recognition of the physical and psychological needs of children in hospital withhealth services seeking to provide an environment which, as far as possible, normalises their stay. Even sickchildren can be quite active and need continuing opportunities for play and education.
NEEDS OF THE POPULATION
The needs of children and adolescents in hospital differs from those for adults. It is a misconception topresume that because children are smaller they will need less space. In fact, a greater amount of space isrequired to accommodate activities such as family centred care and play by and between children.
Factors specific to paediatric/ adolescent care which will influence space utilisation include:
• the mix of beds, cots and bassinets will vary constantly. All rooms must be sized to accommodatea bed. There must be adequate and easily accessible storage;
• bed rooms should be large enough to allow recreation space for the child, space for patientequipment such as walking aids and space for parents to remain with the child. This includesspace for one parent to stay overnight with their child;
• special belongings such as toys and drawings should be readily accessible and visible from thechild's bed;
• additional single bed rooms due to a higher incidence of infectious disease among children;
• recreational play spaces to support the developmental needs of differing age groups. This willideally include access to outdoor areas;
• systems and resources to support the ongoing educational needs of school aged children;
• storage to accommodate strollers, playpens and mobile toys;
• the need for observation of patients by nursing staff is greater, especially of infants and toddlers;
• the need for family/patient education and counselling; and
• a separate treatment room so that painful or stressing procedures do not occur in the child’s bedroom.
Part B - Health Facility Briefing and Planning Page 50540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
02 PLANNING
02.01 Operational Models
MODEL OF CARE
Children and adolescents should be cared for in environments that support their physical and psychologicalneeds.
Ideally, services for paediatrics and adolescents will be collocated. These services may include overnightinpatient beds, short stay beds for monitoring and observation and ambulatory care facilities. Collocationmay promote opportunities for new models of care such as direct referral from a GP. Models will bedependent on the scale of paediatric/ adolescent services and alternate models may be required whereservice volumes are low (e.g. paediatric safe beds within a general inpatient unit).
Participation of parents is regarded as an important principle of paediatric inpatient care. As described inthe Charter on the Rights of Children and Young people in Healthcare Services in Australia, children andadolescents have the opportunity to ‘be nurtured by their parents and to have family relationships supported’while receiving care. This model is referred to as family centred care.
The Charter also promotes participation in ‘education, play, creative activities and recreation, even if this isdifficult due to their illness or disability’.
It is assumed that every Unit will have formal intra-area links as well as a formal relationship with aChildren’s Hospital within a network.
MANAGEMENT OF PATIENTS WITH MENTAL HEALTH CONDITIONS
Where an admission to manage a mental health condition is needed, children under 12 years of age willroutinely be managed in a Paediatric Unit, close to home.
Adolescents with mental health conditions may be managed in a Paediatric/ Adolescent Unit or a specialistChild and Adolescent Mental Health Unit to better manage specific conditions (e.g. early psychosis). Thesafety of the adolescent, and that of others, will be considered.
Where children and adolescents are admitted to a general Paediatric/ Adolescent Unit, they will bemanaged in a standard inpatient bed room. Staff should conduct a risk assessment to determine operationalresponses that will be needed to support the safe care of the patient in the acute inpatient environment.Operational responses may include removing equipment from the bedroom, locating the patient in a bedroom near the staff station, or ‘specialling’.
MANAGEMENT OF SHORT STAYS
When children, after initial treatment, need a period of observation prior to discharge or a decision to admitis uncertain, the allocation of short-stay/ assessment beds within a Paediatric/ Adolescent Inpatient Unitcan support these activities. This avoids children being cared for with adults in short stay units attached toemergency departments.
PROVISION OF SERVICES TO CHILDREN IN HEALTH SERVICES WITHOUT A DEDICATEDPAEDIATRIC/ ADOLESCENT UNIT
In many smaller health facilities, a dedicated Paediatric/ Adolescent Unit may not be possible owing tolow volumes of activity. In such cases, a paediatric ‘safe bed’ model may be an alternative. An example ofcriteria used to provide this type of service is detailed in NSW Health PD2010_033 Safety and Security ofChildren and Adolescents in NSW Acute Health Facilities, June 2010.
Part B - Health Facility Briefing and Planning Page 60540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
02.02 Operational Policies
GENERAL
Operational policies have a major impact on design requirements as well as capital and recurrent costsfor health care facilities. Operational policies should be established at the earliest stages in planning withconsideration given to local jurisdictional policies.
Unit specific operational policies are detailed below; a list of general operational policies is available fromAHIA, 2010, AusHFG Part B: Section 80 General Requirements.
HOURS OF OPERATION
Inpatient services will operate 24 hours a day, seven days per week. Operating hours for short-stay andambulatory care services will vary according to local requirements.
FORMULA PREPARATION AND MILK STORAGE
Many health services may provide a central milk preparation service or provide pre-made formula. Theseproducts will be delivered and stored on the Unit.
Where formula is prepared on the Unit, this will be undertaken in a formula preparation room. This room maybe shared with an adjacent service (e.g. special care nursery).
Dedicated monitored refrigeration may also be needed if mothers are providing expressed breast milk. Thismilk will be stored in a secure room.
HIGH OBSERVATION CARE
Children requiring a higher level of care acutely will be referred to a clinician in a regional or tertiary hospital.A neonatal/paediatric retrieval coordination service, using ground or air transport, may be used especiallyif intensive or high dependency care is anticipated. The care of the patient while awaiting transfer shouldbe discussed with the neonatal/paediatric retrieval service and referral hospital clinician. The most suitableinterim location for care may not be the room in the paediatric inpatient unit and options for temporary caremay include:
• a high-observation area within the Paediatric/ Adolescent Unit; and
• transfer to a higher acuity area of the hospital such as the emergency department.
Each hospital should establish operational policies to manage these situations considering local and regionalresources.
To facilitate consultation between hospitals or a retrieval service, the following resources should beprovided:
• a telephone with direct access to the retrieval services;
• a hands-free cordless handset to allow clinicians to move between patient and support areas;
• the ability for clinical data and images to be reviewed by networked centre; and
• telemedicine technology (e.g. Vision for Adolescent Life). This is likely to be a mobile solution in aPaediatric Unit.
MANAGEMENT OF BARIATRIC (SEVERELY OBESE) PATIENTS
It is important to ensure that one bedroom and ensuite can accommodate a larger bed if necessary and easyuse of lifting equipment for bariatric patients. Space allocations may also need to consider that the parent ofa child may be obese.
STAFFING
The Unit will be staffed by a multidisciplinary team including medical, nursing, allied health and other supportstaff. The staffing profile will be determined by the size and role delineation. Office space and staff amenitieswill reflect this profile.
Part B - Health Facility Briefing and Planning Page 70540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
SCHOOLING
The average age of the Unit’s occupants and average length of stay should be carefully assessed whendetermining the need, if any, of facilities for education. Education can be provided using a model where theteacher comes to the child and uses a mix of hard copy resources and electronic learning tools. Alternatively,recreation spaces may be used flexibly across the day to provide both play and education. Newer modelsinclude online forums so the child can keep connected with their own school.
02.03 Planning Models
LOCATION
The Unit should have direct access to a secure and adequately sized outdoor play area, whether on theground floor or an upper level of the building.
02.04 Functional Areas
FUNCTIONAL ZONES
Functional zones may include:
• entry/ reception/ waiting areas;
• paediatric ambulatory care areas;
• inpatient areas for both paediatrics and adolescents, including recreation areas and parentfacilities;
• clinical support areas; and
• staff areas including office space, meeting rooms and staff amenities
ENTRY/ RECEPTION/ WAITING
Where a critical mass of paediatric/ adolescent services is provided, a dedicated reception will provide awayfinding point for visitors accessing ambulatory care services and possibly the inpatient unit. This waitingroom will also support both services but mainly be used to support ambulatory care services. The receptioncounter should be able to view the entrance to the Unit and observe those in waiting areas.
AMBULATORY CARE AREA
Ambulatory care areas will be grouped so that clinical support and staffing can be shared with the inpatientunit and easily accessible. Facilities may include consult, interview and treatment rooms.
Families should have direct access to this area from the entry/ reception/ waiting room.
INPATIENT AREAS
Inpatient areas will be organised so the majority of patient rooms can be observed. Depending on the agesof children and adolescents being managed on the Unit, it may be possible to cohort two groups of beds andassociated recreation space for children and adolescents. Beds located between these two groups of bedswould ‘swing’ as demand from one group increases or decreases.
Parents and visitors will have direct access to inpatient areas from the entry. A family lounge, and relatedamenities, will be located within this area so parents can have some separation yet remain close to theirchild.
CLINICAL SUPPORT AREAS
Clinical support areas will include staff stations, utilities, a formula room, storage (for a range of clinicalconsumables, equipment, toys and educational resources), beverage room and a cleaners room. Clinicalsupport space may be shared with ambulatory care areas if provided.
Part B - Health Facility Briefing and Planning Page 80540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
Rooms will be arranged so they are easily accessed by staff. Equipment such as resuscitation trolleys mayneed to be stored in lockable cupboards or a room so they cannot be accessed by children.
STAFF AREAS
These areas will include staff offices, meeting rooms and amenities.
02.05 Functional Relationships
The Paediatric/ Adolescent Unit should be located with ready access to the emergency departmentoperating unit, critical care areas and medical imaging. It should be located to avoid the need for throughtraffic.
In small units, collocation with an adult ward with 'swing beds' may facilitate management in times of highoccupancy.
Part B - Health Facility Briefing and Planning Page 90540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
03 DESIGN
03.01 Access
EXTERNAL
Parents may need access to nearby drop-off and parking areas so that children with disabilities can safelyaccess clinical services.
INTERNAL
Internal access to the Unit needs to be controlled to prevent unauthorised access.
03.02 Parking
For information relating to staff parking, refer to Part C, Clause 790 of these Guidelines for furtherinformation.
03.03 Disaster Planning
Refer to AusHFG Part B Clause 80 General Requirements and Part C Design for Access, Mobility, OHS andSecurity for further information.
03.04 Infection Prevention and Control
Additional single bed rooms may be required owing to a higher incidence of infectious disease amongchildren. Both standard isolation and negative pressure isolation rooms may be needed.
Alcohol based hand rub dispensers should be fixed in a location that is not accessible to small children.
Toys used within the Unit should be cleanable.
Also refer to AusHFG Part D Infection Control & Prevention for further information.
03.05 Environmental Considerations
ACOUSTICS
Babies, toddlers and children are naturally boisterous at play and noisy when distressed. The sounds ofchildren crying or in pain, the noise of unfamiliar equipment or, conversely, extreme quiet are all anxiety-provoking.
Finishes and materials must be selected to absorb and soften sounds in all patient and related areas. Thismay be achieved by acoustic ceiling tiles, absorbent panels, curtains, upholstered furniture and the selecteduse of carpet.
The treatment room will require maximum acoustic containment to prevent the sounds of distressed childrenreaching other patient care areas.
NATURAL LIGHT
Natural light is required to all bed rooms, recreation spaces and the family lounge.
Part B - Health Facility Briefing and Planning Page 100540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016
Australasian Health Facility Guidelines
PRIVACY VERSUS OBSERVATION
Design should allow nursing staff to have optimal observation of all patient areas and for children to be ableto see the staff in order to feel reassured and safe.
The need for observation and the safety of children must be balanced to ensure that privacy of children andtheir families. This can be achieved using curtains on windows and other glazed panels and the use of bedscreens.
INTERIOR DECOR
It is important within the Paediatric/Adolescent Unit to use decor to create a positive environment that is asnon-institutional as possible.
Psychological reassurance will be provided by scaling the environment to the size of the child as far aspossible (e.g. tables and chairs in play rooms). Culturally significant images may also provide reassurance.
Graphics provide distraction for children and visitors and can make areas more interesting and inviting. Theycan be used in all patient and common areas including corridors, waiting areas, treatment rooms, play room,recreation rooms, bed rooms and lounges. The décor of areas may need to be suitable for differing agegroups noting that adolescents generally prefer a very different environment.
Wall decorations should be at a height visible by children lying supine in bed and also some low enough fortoddlers to see. Ceiling decoration or sensory walls may also be considered.
Also refer to AusHFG Part C Design for Access, Mobility, OHS and Security.
03.06 Space Standards and Components
ERGONOMICS
Refer to AusHFG Part C Section 730 Human Engineering for information.
HUMAN ENGINEERING
Refer to AusHFG Part C Section 730 Human Engineering for information.
ACCESS AND MOBILITY
Refer to AusHFG Part C Section 730 Human Engineering for information.
WINDOWS
The height of the windows in bed rooms should enable children in their cots/beds to see activity outside. Alow and wide internal window ledge will be well used by children.
Refer to AusHFG Part C Section 730 Human Engineering for further information.
DOORS
Refer AusHFG Part C Clause 710 Space Standards and Dimensions for information.
03.07 Safety and Security
SAFETY
The design of the Unit should aim to reduce safety risks while facilitating the natural curiosity of children.This will be informed through risk assessment.
Design and layout will prevent access by children to areas containing equipment or material likely to beharmful to them, including:
• beverage bay and heated food trolleys;
Part B - Health Facility Briefing and Planning Page 110540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
• utility rooms, cleaners rooms, storage rooms, linen bays;
• resuscitation trolley;
• disposal room;
• treatment room;
• clean utility medication room; and
• inpatient unit exits.
In order to prevent injury and improve safety:
• surface finishes, furniture and glazing must be designed and materials appropriate to their use(e.g. rounded edges on furniture at low levels, safety glass in patient areas);
• cupboards should be designed to be out of reach of small children or fitted with child-proof locks;
• barriers and balustrades will be designed so they are non-non-scalable but can be seen throughby toddlers;
• non-scalable safety fencing of adequate height around external play areas should be providedespecially where this is not located at ground level;
• locate services and fixtures such as power points, medical service panels, call systems, handhygiene products and door handles out of reach of small children; and
• bed rooms to have doors with high and low vision panels and handles. These will be sized andpositioned so staff can see a small child on the other side.
As far as possible, safety measures should not cause avoidable inconvenience nor impair efficiency.
SECURITY
Egress points must be secured and should be monitored to minimise and contain the risk of a child'sunaccompanied egress or abduction from the Unit and prevent interference from unauthorised persons.
Security measures may include:
• video intercoms and access control at the entrance to the Unit;
• direct staff observation;
• restricted window openings;
• ‘tagging’ of babies and toddlers so they can be tracked; and
• high level door latches.
03.08 Finishes
WALL PROTECTION
Refer to AusHFG Part C Design for Access, Mobility, OHS and Security for information.
FLOOR FINISHES
Refer to AusHFG Part C Design for Access, Mobility, OHS and Security for information.
CEILING FINISHES
If patients with eating disorders are managed within the Unit care should be taken with regard to use ofceiling tiles as hide food.
Part B - Health Facility Briefing and Planning Page 120540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
03.09 Fixtures, Fittings & Equipment
DOOR HARDWARE
Door hardware must be designed so as not to trap small fingers.
Refer to part C of these Guidelines and to the Room Data Sheets (RDS) and Room Layout Sheets (RLS) forfurther detailed information.
03.10 Building Service Requirements
INFORMATION COMMUNICATIONS TECHNOLOGY
In addition to the usual hospital communication systems (such as point of care systems), the Paediatric/Adolescent Unit has particular needs.
Communication systems may include:
• closed-circuit television monitoring where this is necessary to ensure adequate observation ofaccess/egress points;
• televisions in all bedrooms;
• dedicated Wi-Fi internet access children and their families to support their own devices; and
• staff to staff communication devices such as DECT phones.
Increasingly IT system may support a patient’s own devices providing access to the internet via wirelessarrangements.
In addition, smaller health care facilities may need to communicate with their networked service regardingurgent patient care issues. To facilitate this communication the following equipment may be needed:
telephone with direct access to a retrieval service;
• an office area equipped with a hands-free cordless phone and PC for viewing/ sharing imagesand clinical data; and
• telemedicine technology. In most inpatient environments, a mobile solution is suitable.
DURESS ALARM SYSTEM
Duress alarms will be located at receptions and staff stations. Should a paediatric / adolescent ambulatorycare service be collocated, fixed duress points are usually included in consult and interview rooms.
Part B - Health Facility Briefing and Planning Page 130540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
04 COMPONENTS OF THE UNIT
04.01 Standard Components
Rooms / spaces are defined as:
• standard components (SC) which refer to rooms / spaces for which room data sheets, roomlayout sheets (drawings) and textual description have been developed;
• standard components – derived rooms are rooms, based on a SC but they vary in size. In theseinstances, the standard component will form the broad room ‘brief’ and room size and contentswill be scaled to meet the service requirement;
• non-standard components which are unique rooms that are usually service-specific and notcommon.
The standard component types are listed in the attached Schedule of Accommodation. The current StandardComponents can be found at: www.healthfacilityguidelines.com.au/standardcomponents
04.02 Non-Standard Components
Non-standard components are unit-specific and provided in accordance with specific operational policiesand service demand. These non-standard components for a Paediatric/ Adolescent Unit are detailed below.
1 BED ROOM – PAEDIATRIC
Description and Function
The 1 Bed Room will be broadly consistent with the standard component for a 1 Bed Room. In the paediatricinpatient context, the bed room will be sized to accommodate an overnight bed to be used by a parent.Patient entertainment will be needed at each bedspace including access to a patient entertainment system.
Considerations
Options for an overnight parent bed may include:
• a sofa chair that can be converted to a bed or mobile fold-away bed in the case of generalpaediatric services; or
• a more permanent solution in a children’s hospital (built-in or pull down unit).
Should a fold away option be used, storage space will be needed. This approach to planning will beconsidered for all 1 bed rooms including isolation and bariatric rooms.
BATHROOM - PAEDIATRIC
Description and Function
The bathroom has adjustable height paediatric peninsula bath, shower, hand basin and toilet facilities toattend the hygiene and treatment needs of babies, toddlers and older children.
A baby bath is required and should be bench-set, a baby change bench / table and baby and adult scales.
Functions include:
• bathing of patients for treatment purposes;
• weighing and height measuring on admission; and
Part B - Health Facility Briefing and Planning Page 140540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
• Unaccompanied patients may not have access to this room.
Location and Relationships
Centrally located to the bed rooms, with good visual observation and quick access from the staff station.
Considerations
Space may also store:
• mobile patient lifter;
• baby clothes and nappies;
• baby care supplies;
• bath cleaning equipment; and
• Effective ventilation is needed.
The room may be designed for use by more than one small child at a time while preserving visual privacy.
PLAY ROOM - INTERNAL
Description and Function
The play room provides an area where children may go for play, recreation, education and remedialactivities. The following designated area may be provided within the space allocation:
• dining for small children;
• television; and
• reading / playing board games.
It is envisaged that parents and siblings will accompany their children at times.
Functions and activities will include:
• structured and unstructured play activities;
• reading;
• watching television;
• drawing (whiteboards and paper);
• board games;
• meals, snacks, drinks for patients;
• remedial therapy activities; and
• education.
The patients may be:
• ambulant/ crawling;
• in bed/ cot/ bassinet;
• in a stroller/ pram;
• on crutches or in a wheelchair;
• in a playpen; and
• needing therapy or treatment such as oxygen, IV therapy or traction.
Location and Relationships
Access must allow for a bed with orthopaedic fittings.
Part B - Health Facility Briefing and Planning Page 150540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
Direct access to the outside play area (where provided).
Good observation from staff station and general nursing circulation areas required.
Considerations
The following are required:
• natural light;
• bright and cheerful décor;
• acoustic absorption; and
• means of restricted window opening for natural ventilation when required.
Corridor wall and door to be glazed to allow observation of patients.
Dividing walls may be glazed to a height suitable to allow observation of patients.
Storage (not necessarily within the play area) required for:
• hospital-provided toys and games;
• books, education material and CDs / DVDs;
• chairs - stacking - several sizes;
• high chairs;
• tricycles;
• playpen (fold-away);
• strollers and prams; and
• computers.
If paints are to be used, a small sink should be fitted.
Consider a toddler-height hand basin for use before and after meals / snacks.
TREATMENT ROOM
Description and Function
This room will generally be consistent with the standard component. Procedures may include inhalationsedation.
Location and Relationships
Centrally located to bed rooms.
Considerations
The space should be planned to accommodate procedural sedation as staff will move the bed away from thewall and supervise sedation at the bedhead. Staff will still need to move around the foot of the bed.
PLAY ROOM - EXTERNAL
Description and Function
An outdoor area where children may go for play, recreation, remedial activities and family visiting.
Functions and activities include:
• structured and unstructured play activities;
• remedial therapy activities; and
• family interaction and quiet time.
Location and Functional Relationships
Part B - Health Facility Briefing and Planning Page 160540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
Observation from the staff station.
Direct access to / from inside play area.
Consideration should be given to external access for maintenance purposes.
Considerations
Threshold should facilitate ease of manoeuvring for:
• patients in wheelchairs;
• patient beds/cots/bassinet; and
• those who have difficulty in walking.
Requires protection from extreme weather conditions including suitably rated sun shared and otherprotected undercover area.
Ground area may be covered with outdoor carpet or pavers but not loose materials such as gravel orwoodchips.
Non-scalable safety fence high enough to prevent removal of children is required for the surrounding area.
Access and egress should only be form the inpatient area.
RECREATION ROOM
Description and Function
An indoor area where adolescents can use to meet with their peers/ friends, watch TV, listen to music or playgames. Requirements include:
• TV;
• docking station for MP3 players;
• other equipment such as an air hockey table or pool table; and
• lounge chairs, beanbags and sofas.
Location and Functional Relationships
Locate near adolescent bed rooms, where designated.
Considerations
Wireless internet will allow adolescents to use their own devices within this area.
QUIET STUDY ROOM
Description and Function
An indoor area used by adolescents to undertake study or other quiet activities.
Considerations
Locate away from noisy rooms but nearby adolescent bed rooms.
Options may include desk space and /or lounge chairs. GPOs and wireless internet will allow adolescents touse hospital provided PCs or their own devices.
It will be possible to use this room for alternate uses when not in use by adolescents (e.g. small meetings).
Part B - Health Facility Briefing and Planning Page 170540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016
Australasian Health Facility Guidelines
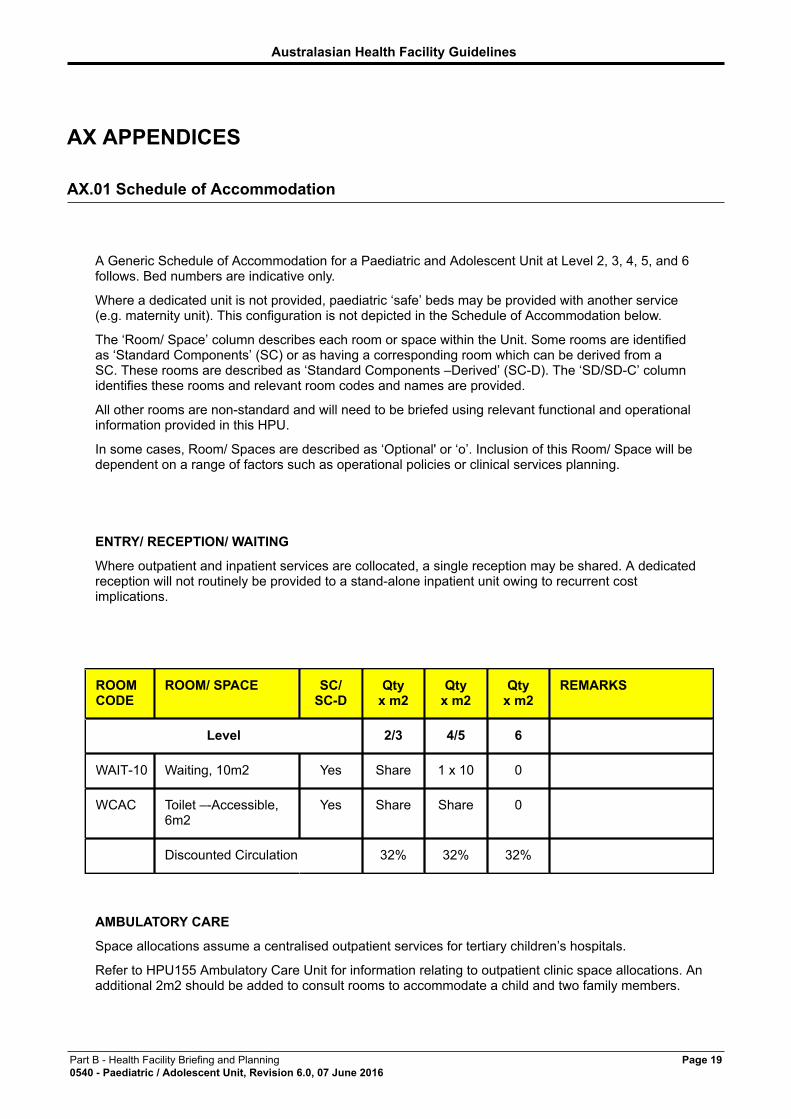
AX APPENDICES
AX.01 Schedule of Accommodation
A Generic Schedule of Accommodation for a Paediatric and Adolescent Unit at Level 2, 3, 4, 5, and 6follows. Bed numbers are indicative only.
Where a dedicated unit is not provided, paediatric ‘safe’ beds may be provided with another service(e.g. maternity unit). This configuration is not depicted in the Schedule of Accommodation below.
The ‘Room/ Space’ column describes each room or space within the Unit. Some rooms are identifiedas ‘Standard Components’ (SC) or as having a corresponding room which can be derived from aSC. These rooms are described as ‘Standard Components –Derived’ (SC-D). The ‘SD/SD-C’ columnidentifies these rooms and relevant room codes and names are provided.
All other rooms are non-standard and will need to be briefed using relevant functional and operationalinformation provided in this HPU.
In some cases, Room/ Spaces are described as ‘Optional' or ‘o’. Inclusion of this Room/ Space will bedependent on a range of factors such as operational policies or clinical services planning.
ENTRY/ RECEPTION/ WAITING
Where outpatient and inpatient services are collocated, a single reception may be shared. A dedicatedreception will not routinely be provided to a stand-alone inpatient unit owing to recurrent costimplications.
ROOMCODE
ROOM/ SPACE SC/SC-D
Qtyx m2
Qtyx m2
Qtyx m2
REMARKS
Level 2/3 4/5 6
WAIT-10 Waiting, 10m2 Yes Share 1 x 10 0
WCAC Toilet –-Accessible,6m2
Yes Share Share 0
Discounted Circulation 32% 32% 32%
AMBULATORY CARE
Space allocations assume a centralised outpatient services for tertiary children’s hospitals.
Refer to HPU155 Ambulatory Care Unit for information relating to outpatient clinic space allocations. Anadditional 2m2 should be added to consult rooms to accommodate a child and two family members.
Part B - Health Facility Briefing and Planning Page 190540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
Alternatively, assessment/ day stay beds and associated isolation rooms may instead be collocated withother inpatient beds. This will be dependent on critical mass and the most efficient use of nursing staffacross the two areas.
ROOMCODE
ROOM/ SPACE SC/SC-D
Qtyx m2
Qtyx m2
Qtyx m2
REMARKS
Level 2/3 4/5 6
4BR-ST-A 4 Bed Room,42m2
Yes 1 x 42
(o)
42 0 Assessment/ DayStay. May be used forshort term holding ofchildren and / or forday stay procedures
1BR-ST-A 1 Bed Room,15m2
Yes 1 x15 (o)
A standard isolationroom to manageconditions such asgastroenteritis oroncology cases.Assumes day-onlycare
ENS-ST-A1
Ensuite, 5m2 Yes 1 x 5
(o)
2 x 5 0 Include secondensuite if singlebedroom is provided.
CONS Consult Room 1 x 14
(o)
14 0 Larger size forchildren. Numberof rooms will bedependent onanticipated occasionsof service
INTF Interview Room Yes 1 x 12
(o)
1 x 12 0
BLIN Bay - Linen Yes SharedwithIPU
1 x 2 0
Staff Base / CleanUtility
1 x 5 1 x 10 0
Discounted Circulation 32% 32% 32%
Part B - Health Facility Briefing and Planning Page 200540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
INPATIENT AREAS
The bed numbers and bed room types are indicative only. Numbers and configuration will be based onservice planning and jurisdictional policies. Overnight accommodation is assumed.
ROOMCODE
ROOM/ SPACE SC/SC-D
Qtyx m2
Qtyx m2
Qtyx m2
REMARKS
Level 2/3 4/5 6
1BR-ST-A 1 Bed Room Yes 4 x 18 8 x 18 15x 20
Bed/chair for parent.For management ofairborne infectionssuch as chickenpox.
1BR-IS-N 1 Bed Room -Isolation NegativePressure
Yes 0 1 x 18 1 x 18 Bed/chair for parent.Class N IsolationRooms
2BR-ST-A 2 Bed Room Yes 3 x 31 2 x 31 4 x 31 For older children
4BR-ST-A 4 Bed Room Yes 0 1 x 42 1 x 42 For babies andtoddlers. May alsobe used for highobservation at Levels4 / 5
ENS-ST-A1
Ensuite, 5m2 Yes 4 x 5 12 x 5 22 x 5
WCPT Toilet – Patient,4m2
Yes 0 1 x 4 1 x 4 Assumes each 4 bedroom has an ensuiteand toilet
ANRM Anteroom Yes 0 1 x 6 2 x 6 For Class N IsolationRooms
BHWS-B Bay -Handwashing -Type B
Yes 2 x 1 4 x 1 6 x 1
Discounted Circulation 32% 32% 32%
Part B - Health Facility Briefing and Planning Page 210540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016
Australasian Health Facility Guidelines
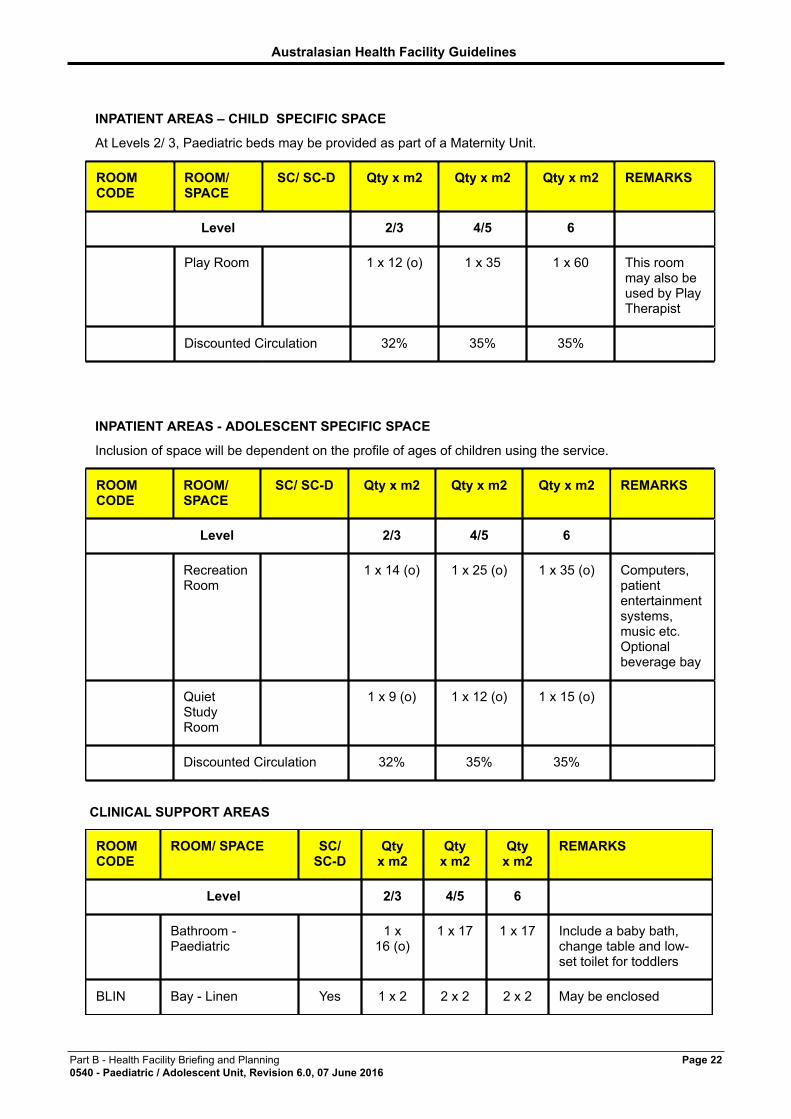
INPATIENT AREAS – CHILD SPECIFIC SPACE
At Levels 2/ 3, Paediatric beds may be provided as part of a Maternity Unit.
ROOMCODE
ROOM/SPACE
SC/ SC-D Qty x m2 Qty x m2 Qty x m2 REMARKS
Level 2/3 4/5 6
Play Room 1 x 12 (o) 1 x 35 1 x 60 This roommay also beused by PlayTherapist
Discounted Circulation 32% 35% 35%
INPATIENT AREAS - ADOLESCENT SPECIFIC SPACE
Inclusion of space will be dependent on the profile of ages of children using the service.
ROOMCODE
ROOM/SPACE
SC/ SC-D Qty x m2 Qty x m2 Qty x m2 REMARKS
Level 2/3 4/5 6
RecreationRoom
1 x 14 (o) 1 x 25 (o) 1 x 35 (o) Computers,patiententertainmentsystems,music etc.Optionalbeverage bay
QuietStudyRoom
1 x 9 (o) 1 x 12 (o) 1 x 15 (o)
Discounted Circulation 32% 35% 35%
CLINICAL SUPPORT AREAS
ROOMCODE
ROOM/ SPACE SC/SC-D
Qtyx m2
Qtyx m2
Qtyx m2
REMARKS
Level 2/3 4/5 6
Bathroom -Paediatric
1 x16 (o)
1 x 17 1 x 17 Include a baby bath,change table and low-set toilet for toddlers
BLIN Bay - Linen Yes 1 x 2 2 x 2 2 x 2 May be enclosed
Part B - Health Facility Briefing and Planning Page 220540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
BRES Bay - ResuscitationTrolley
Yes Shared 2 x 1.5 2 x 1.5 Assumes one forinfants, one foradolescents. Securelocation needed.
PTRY Pantry Yes Shared 1 x 8 1 x 8 This room will alsobe used to storesnacks for children andadolescents.
BMT-4 Bay – Meal Trolley Yes Shared 1 x 4 1 x 4
BMEQ-4 Bay – MobileEquipment, 4m2
Yes Shared 1 x 4 2 x 4
FORM Formula Room Yes 1 x 7
(o)
1 x 7
(o)
1 x 7
(o)
May be located inNICU/SCN or MaternityUnit in Level 2/3.
SSTN-14 Staff Station, 14m2 Yes Shared 1 x 14 1 x 14
OFF-CLN
Office - ClinicalWorkroom
Yes Shared 1 x 12 1 x 15
STPS-8 Store - Photocopy /Stationery, 8m2
Yes Shared 1 x 8 1 x 8 May be collocated withoffices
CLUR-12 Clean Utility/Medication Room
Yes Shared 1 x 12 1 x 14 Includes medicationstorage
PROC-16 Procedure Room,16m2
Shared 1 x 16 1 x 16
DTUR-10 Dirty Utility Yes Shared 1 x 10 1 x 12 May need 2 roomsdepending on IPUlayout
DISP-8 Disposal Room,8m2
Yes Shared 1 x 8 1 x 8
INTF Interview Room Yes Shared 1 x 12 1 x 12 May also be usedas a quiet space forbreastfeeding
Therapy /Multipurpose Room
0 1 x 20 1 x 20
ST-EQ-14
Store - Equipment Yes 1 x 12 1 x 20 1 x 30 Beds and cots
STEQ-20 Store - Equipment Yes Shared 1 x 20 1 x 25 General equipment
STGN-9 Store – General,9m2
Yes Shared 1 x 9 1 x 9 Clinical consumables
Part B - Health Facility Briefing and Planning Page 230540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
CLRM-5 Cleaner's Room,5m2
Yes Shared 1 x 5 1 x 5
LNPA-12 Lounge - Parent Yes 1 x 9
(o)
1 x 12 1 x 18 May include sofa bed
BBEV-OP
Bay – Beverage,
Open Plan
Yes 0 1 x 3 1 x 3 Collocate with ParentLounge
OVES Overnight Stay -Ensuite
Yes 0 1 x 4 1 x 4 Provided for parents
Discounted Circulation 32% 35% 35%
STAFF AREAS
Office space is indicative only. Requirements will be based on jurisdictional office policies and staffingprofiles. Where outpatient services are collocated, it is likely that additional clerical support may beneeded.
ROOMCODE
ROOM/ SPACE SC/SC-D
Qtyx m2
Qtyx m2
Qtyx m2
REMARKS
Level 2/3 4/5 6
OFF-S12
Office – SinglePerson, 12m2
Yes 1 x 12 1 x 12 Director
OFF-S9 Office - SinglePerson, 9m2
Yes 1 x 9 1 x 9 1 x 9 NUM
OFF-2P Office – 2 Person,Shared, 12m2
Yes 1 x 12 1 x 12
Office – Workstation- 0 5.5 5.5 No. dependent on localarrangements andoffice policies. Mayinclude education,administration andresearch staff
MEET-L-15
Meeting Room Yes Share 1 x 18 1 x 20
SRM-15 Staff Room Yes Share 1 x 15 1 x 18
PROP-2 Property Bay - Staff Yes Share 1 x 2 1 x 3
WCST Toilet – Staff, 3m2 Yes Share 2 x 3 2 x 3
Part B - Health Facility Briefing and Planning Page 240540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
SHST Shower – Staff, 3m2 Yes Share 1 x3 (o)
1 x3 (o)
Discounted Circulation 20% 30% 30%
Part B - Health Facility Briefing and Planning Page 250540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
AX.02 Functional Relationships / Diagrams
A functional relationship diagram is shown below.
Part B - Health Facility Briefing and Planning Page 260540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
AX.03 Checklists
A Security Checklist is contained below. Refer also to Part C of these Guidelines for general requirements.
AX.04 References
• Association or the Wellbeing of Children in Healthcare and Children's Hospitals of Australia,Charter on the Rights of Children and Young People in Healthcare Services in Australia;
• Association for the Wellbeing of Children in Healthcare, Policy Relating to the Provision of Play forChildren in Hospital, 2002;
• National Public Health Partnership, Healthy Children – Strengthening Promotion and PreventionAcross Australia. National Public Health Strategic Framework for Children 2005 – 2008, 2005;
• Royal Australasian College of Physicians, Association for the Wellbeing of Children in Healthcareand Children’s Hospitals of Australasia, Standards for the Care of Children and Adolescents inHealth Services, 2008; and
• NSW Health PD2010_033 Children and Adolescents – Safety and Security in Acute CareSettings, June 2010.
FURTHER READING
• NSW Health Guidelines for Networking of Paediatric Services in NSW, 2002
• NSW Health PD2005_157 Emergency Paediatric Referral – Policy, January 2005
• NSW Health PD2010_034 Children and Adolescents – Guidelines for Care in Acute CareSettings, June 2010
• NSW Health PD2010_030 Critical Care Tertiary Referral Networks, June 2010
• NSW Health PD2011_016 Children and Adolescents with Mental Health Problems RequiringInpatient Care, March 2011
Part B - Health Facility Briefing and Planning Page 270540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
ATTACHMENTS
Attachments
SECURITY ISSUES TO BE CONSIDERED IN PAEDIATRIC AND ADOLESCENT UNIT
GENERIC SAFETY AND/OR SECURITYRISKS
POTENTIAL SOLUTIONS
Entry by all relevant hospital personnel visitingor working within the health service.
CCTV monitoring of inpatient entry and exitdoorways
After-hours remote switch and intercom installed atentry
Use of reed switches on all external doors andentries. Swipe card readers may be required toboth sides of internal doors to allow accessed byauthorised staff.
SPECIFIC SAFETY AND/OR SECURITYRISKS
POTENTIAL SOLUTIONS
Relatives/ visitors Good visibility from staff stations to patient areaswithin the inpatient unit
Manage relative/ visitor admittance in the area byrestricting visiting hours and/or number, of visitors
Furniture fittings and equipment includingcomputers, office and medical equipment
Non-removable 'Asset No.' on all equipment above apredetermined value.
Keep equipment in lockable areas
Hospital personnel safety Staff working in this area to have knowledge ofwhere the fixed duress system is located and/or usesa mobile duress pendant.
Design shape of interview rooms and location ofdesks in such a way that minimises risk to healthpersonnel.
Provide storage and store items not in constant usethat could be used as weapons. (Operational Policy).
Minimise furniture that can be used as a weapon.
Staff personal effects Provision for lockers in staff areas and lockable deskdrawer to keep small personal effects.
Drug storage Drugs safe to be located in area that can bemonitored by staff
Part B - Health Facility Briefing and Planning Page 280540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016

Australasian Health Facility Guidelines
SECURITY CHECKLIST – PAEDIATRIC AND ADOLESCENT UNIT
FACILITY: DEPARTMENT: Paediatric and Adolescent Unit
RISK ISSUE DESIGN RESPONSE
How is ‘after hours' access provided forpatients and parents and how is this accesspoint monitored?
Do staff have access to both fixed duresssystems?
Is access to patient records restricted to staffentitled to that access?
Is a system implemented to prevent theft ofequipment, files, personal possessions, etc?
Are drug safes installed in accordance withcurrent regulations?
How is after-hours access provided for staff?
How are offices secured during and afterhours?
Is there a lockable storage area available forspecialised equipment?
Is lockable furniture provided for storage ofstaff personal effects?
What system has been implemented to preventthe illegal removal of children?
Are interview rooms appropriately designedwith specific reference to staff egress,furniture selection, furniture location, provisionfor storage of equipment, etc.
What surveillance/monitoring system will beimplemented to monitor access to rooms?
DESIGN COMMENTARY I NOTES DESIGN SIGN-OFF
Name:__________________________________
Position:________________________________
Signature:_______________________________
Date:___________________________________
Name:__________________________________
Position:________________________________
Signature:_______________________________
Date:___________________________________
Name:__________________________________
Position:________________________________
Signature:_______________________________
Date:___________________________________
Part B - Health Facility Briefing and Planning Page 290540 - Paediatric / Adolescent Unit, Revision 6.0, 07 June 2016


















