Health Disparities in Diabetes Jim Holt, MD February 11, 2009.
22
Health Disparities in Health Disparities in Diabetes Diabetes Jim Holt, MD Jim Holt, MD February 11, 2009 February 11, 2009
-
Upload
loren-williams -
Category
Documents
-
view
212 -
download
0
Transcript of Health Disparities in Diabetes Jim Holt, MD February 11, 2009.

Health Disparities in Health Disparities in DiabetesDiabetes
Jim Holt, MDJim Holt, MD
February 11, 2009February 11, 2009

PollPoll
• Consider your patients in the clinic. In Consider your patients in the clinic. In what ways is their health adversely affected what ways is their health adversely affected by--by--
1) The prevailing culture? Does the 1) The prevailing culture? Does the Appalachian area accept more: sedentary Appalachian area accept more: sedentary lifestyles/obesity, poor diets, smoking, and lifestyles/obesity, poor diets, smoking, and ignorance of general health ignorance of general health recommendations?recommendations?
2) Inability to access all needed care?2) Inability to access all needed care?3) Inadequate resources for care?3) Inadequate resources for care?4) Other factors?4) Other factors?

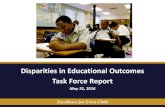
County-level Estimates of Diagnosed Diabetes for Adults aged ≥ 20 years: United States 2005


Unsubstantiated Local Unsubstantiated Local DataData
• 100,000 diabetics in East Tennessee region100,000 diabetics in East Tennessee region• Average HbA1c 9.4% vs. national 7.8%Average HbA1c 9.4% vs. national 7.8%• Average BMI of East TN diabetics: 34Average BMI of East TN diabetics: 34• There are 3 pediatric endocrinologists in the There are 3 pediatric endocrinologists in the
East TN region. Half of the children they East TN region. Half of the children they saw in 2007 have Type 2 diabetes. In 1992, saw in 2007 have Type 2 diabetes. In 1992, 10% of the children they saw had Type 2 10% of the children they saw had Type 2 DM.DM.
• Data from a Knoxville pediatric Data from a Knoxville pediatric endocrinologistendocrinologist

CDC Co. Prevalence DataCDC Co. Prevalence Data
CountyCounty PrevalnPrevalncece
Lower Lower CLCL
Upper Upper CLCL
SDSD
SullivanSullivan 13.9%13.9% 11.8%11.8% 16.3%16.3% 1.2%1.2%
WashngWashngtntn
9.5%9.5% 7.5%7.5% 11.8%11.8% 1.1%1.1%
HawkinHawkinss
11.8%11.8% 9.0%9.0% 15.4%15.4% 1.7%1.7%
CarterCarter 10.4%10.4% 7.8%7.8% 13.8%13.8% 1.5%1.5%
UnicoiUnicoi 11.3%11.3% 8.2%8.2% 15.2%15.2% 1.8%1.8%
JohnsonJohnson 9.7%9.7% 7.0%7.0% 13.1%13.1% 1.5%1.5%
GreeneGreene 10.7%10.7% 8.3%8.3% 13.7%13.7% 1.4%1.4%
HancocHancockk
10.5%10.5% 7.5%7.5% 14.5%14.5% 1.8%1.8%

TN 2007 County Health TN 2007 County Health SnapshotSnapshot
County County MeasureMeasure
SullivanSullivan WashingtonWashington
Yrs of Pot Life Yrs of Pot Life LL
9,841: Rank 9,841: Rank 56/9556/95
9,148 9,148 (33/95)(33/95)
% Poor/Fair % Poor/Fair HlthHlth
20.9% 20.9% (30/95)(30/95)
22.9% 22.9% (70/95)(70/95)
No Hlth InsurNo Hlth Insur 13.7% R 13.7% R (40/95)(40/95)
19.0% R 19.0% R (75/95)(75/95)
Doctors per Doctors per capcap
372/100K 372/100K (6/95)(6/95)
540/100K(3/9540/100K(3/95)5)
Pneumovax Pneumovax VacVac
31.8% Reg 31.8% Reg (1/95)(1/95)
27.4%R 27.4%R (12/95)(12/95)
Influenza VacInfluenza Vac 44.8% R 44.8% R (1/95)(1/95)
34.5%R 34.5%R (53/95)(53/95)
DM Eye DM Eye ExamsExams
52.2% 52.2% (28/95)(28/95)
51.0% 51.0% (37/95)(37/95)
DM Lipid DM Lipid EvalEval
77.1% 77.1% (52/95)(52/95)
75.6% 75.6% (64/95)(64/95)
DM HbA1c’sDM HbA1c’s 90.1% 90.1% (6/95)(6/95)
85.4% 85.4% (59/95)(59/95)

Sullivan & Washington Sullivan & Washington Cos.Cos.
Cig SmokingCig Smoking 22.4%R 22.4%R (18/95)(18/95)
29.9%R 29.9%R (75/95)(75/95)
SedentarySedentary 36.8%R 36.8%R (95/95)(95/95)
35.3%R 35.3%R (88/95)(88/95)
Overwt/ObeseOverwt/Obese 67.7%R 67.7%R (60/95)(60/95)
64.8%R 64.8%R (18/95)(18/95)
3 Fruit 3 Fruit &Veg/day&Veg/day
72.8%R 72.8%R (2/95)(2/95)
67.6%R 67.6%R (30/95)(30/95)
Binge EtOHBinge EtOH 8.8%R 8.8%R (81/95)(81/95)
4.3%R 4.3%R (25/95)(25/95)
Teen Birth Teen Birth RateRate
50/1K 50/1K (30/95)(30/95)
37/1K 37/1K (9/95)(9/95)
HS HS Graduation RtGraduation Rt
81.2% 81.2% (67/95)(67/95)
87.7% 87.7% (34/95)(34/95)
%18-64 w HS %18-64 w HS DipDip
80.4% 80.4% (20/95)(20/95)
82.8% 82.8% (11/95)(11/95)
UnemploymeUnemploymentnt
4.5% 4.5% (13/95)(13/95)
4.5% 4.5% (13/95)(13/95)
Overall Overall HealthHealth
(43/95)(43/95)
(36/95)(36/95)



Other Regional CountiesOther Regional Counties
MeasMeas..
HawHawk.k.
CartCarterer
UnicUnicoioi
John.John. GrneGrne..
HancHanc..
Yrs Yrs LsLs
67/967/955
45/945/955
30/930/955
72/972/955
35/935/955
91/991/955
Pr Pr Hl*Hl*
70/970/955
70/970/955
70/970/955
70/970/955
70/970/955
70/970/955
-- -- Ins*Ins*
75/975/955
75/975/955
75/975/955
75/975/955
75/975/955
75/975/955
MDpMDpcc
70/970/955
52/952/955
34/934/955
56/956/955
21/921/955
80/980/955
PnvxPnvx**
12/912/955
12/912/955
12/912/955
12/912/955
12/912/955
12/912/955
FluvxFluvx**
53/953/955
53/953/955
53/953/955
53/953/955
53/953/955
53/953/955
DmeDmeyeye
67/967/955
66/966/955
87/987/955
95/995/955
41/941/955
94/994/955
DmliDmlipp
32/932/955
85/985/955
81/981/955
66/966/955
74/974/955
68/968/955
HA1cHA1c 22/922/955
93/993/955
87/987/955
82/982/955
58/958/955
43/943/955

Adjacent Counties Adjacent Counties (Cont.)(Cont.)
MeasMeas..
HawHawk.k.
CartCarterer
UnicUnicoioi
John.John. GrneGrne..
HancHanc..
Cigs*Cigs* 75/975/955
75/975/955
75/975/955
75/975/955
75/975/955
75/975/955
SedeSeden*n*
88/988/955
88/988/955
88/988/955
88/988/955
88/988/955
88/988/955
ObesObes**
18/918/955
18/918/955
18/918/955
18/918/955
18/918/955
18/918/955
--fr/--fr/v*v*
30/930/955
30/930/955
30/930/955
30/930/955
30/930/955
30/930/955
BingBinge*e*
25/925/955
25/925/955
25/925/955
25/925/955
25/925/955
25/925/955
TeenTeenBB
28/928/955
32/932/955
16/916/955
62/962/955
47/947/955
88/988/955
HSgrHSgrtt
87/987/955
37/937/955
5/955/95 42/942/955
39/939/955
49/949/955
GradGradss
41/941/955
49/949/955
38/938/955
93/993/955
48/948/955
91/991/955
--jobs--jobs 46/946/955
21/921/955
53/953/955
67/967/955
85/985/955
74/974/955

““Double Disparity”Double Disparity”
• Groups which are disadvantaged in Groups which are disadvantaged in general settings might suffer from general settings might suffer from additional hardship in areas experiencing additional hardship in areas experiencing health disparities.health disparities.
• Example: the documentary Example: the documentary “Conocimiento”, a brief film produced by “Conocimiento”, a brief film produced by an interdisciplinary team at ETSU in an interdisciplinary team at ETSU in 2006, notes particular hardships Mexican 2006, notes particular hardships Mexican mothers faced in complicated deliveries mothers faced in complicated deliveries at local hospitals with inadequate at local hospitals with inadequate availability of Spanish translators.availability of Spanish translators.

Other DisparitiesOther Disparities
• Higher obesity rates in AppalachiaHigher obesity rates in Appalachia• Higher tobacco smoking ratesHigher tobacco smoking rates• Sedentary activity much more Sedentary activity much more
prevalentprevalent• Insurance coverage trend to lower Insurance coverage trend to lower
percentagepercentage• Higher hospitalization rate for DM2 Higher hospitalization rate for DM2
in SW VAin SW VA


Small Group Activity Small Group Activity
• Count off for groups of 4 or 5Count off for groups of 4 or 5• Each group takes 1 caseEach group takes 1 case• May have 2 groups working on the May have 2 groups working on the
same casesame case• Answer questions within 15 minutesAnswer questions within 15 minutes• Select spokesperson, to report to the Select spokesperson, to report to the
large grouplarge group

Questions for CasesQuestions for Cases
• Which disparities are most relevant in Which disparities are most relevant in this case?this case?
• What barriers exist to optimal care of the What barriers exist to optimal care of the DM?DM?
• What are the group’s recommendations to What are the group’s recommendations to significantly improve the patient’s care?significantly improve the patient’s care?
• What additional resources would improve What additional resources would improve this patient’s care, or the care of similar this patient’s care, or the care of similar patients?patients?

Disparities in Diabetes Case Disparities in Diabetes Case # 1# 1
• PC is a 52 year-old white female who presents PC is a 52 year-old white female who presents to Diabetes Clinic. She reports onset of Type 2 to Diabetes Clinic. She reports onset of Type 2 Diabetes at age 31, when her sugars remained Diabetes at age 31, when her sugars remained abnormal following the birth of her second abnormal following the birth of her second (and last) child. PC reports great difficulty (and last) child. PC reports great difficulty controlling binge eating, and consistently poor controlling binge eating, and consistently poor blood sugar readings over the course of her blood sugar readings over the course of her illness. She has burning pain and numbness in illness. She has burning pain and numbness in her legs constantly, up to the thighs. She’s her legs constantly, up to the thighs. She’s had a small MI in the past year, and a “TIA” 3 had a small MI in the past year, and a “TIA” 3 years ago, which left her with mild weakness years ago, which left her with mild weakness in the left hand. Her vision is “only fair”. She in the left hand. Her vision is “only fair”. She is 61 inches tall, and 185 lbs.; her BMI is 35.is 61 inches tall, and 185 lbs.; her BMI is 35.

Disparities in Diabetes Case Disparities in Diabetes Case # 2# 2
• LB is a 12 year-old white female with a 4 LB is a 12 year-old white female with a 4 year history of Type 1 Diabetes. She initially year history of Type 1 Diabetes. She initially presented to the office with F/U care on a presented to the office with F/U care on a Salter I fracture of her ankle; after 2 visits of Salter I fracture of her ankle; after 2 visits of mother requesting pain meds, suspicion of mother requesting pain meds, suspicion of drug abuse by mother is confirmed by DCS. drug abuse by mother is confirmed by DCS. Father is in prison, but a release date is Father is in prison, but a release date is approaching. LB presents to Diabetes Clinic, approaching. LB presents to Diabetes Clinic, reporting resentment of her twin sister’s reporting resentment of her twin sister’s ability to live “normally”. LB admits to daily ability to live “normally”. LB admits to daily binge eating, with blood sugars ranging from binge eating, with blood sugars ranging from mid-100’s to mid-400’s nearly every day.mid-100’s to mid-400’s nearly every day.

Disparities in Diabetes Case Disparities in Diabetes Case # 3# 3
• RF is a 56 year-old white male with DM2 for 12 RF is a 56 year-old white male with DM2 for 12 years, HTN for 25 years, and OSA diagnosed years, HTN for 25 years, and OSA diagnosed concurrently with COPD 2 years ago. He concurrently with COPD 2 years ago. He tolerates CPAP poorly, and often doesn’t wear tolerates CPAP poorly, and often doesn’t wear it. He stays sleepy and sluggish most of the it. He stays sleepy and sluggish most of the time. He has gained 50 lbs. in the past 26 time. He has gained 50 lbs. in the past 26 months; during that time, his diabetic control months; during that time, his diabetic control has deteriorated from HbA1c’s in the 7 to 8% has deteriorated from HbA1c’s in the 7 to 8% range, to 13.5% today. He is still gaining range, to 13.5% today. He is still gaining weight. He presents to the Diabetes Clinic weight. He presents to the Diabetes Clinic saying, “I don’t really see the point of trying saying, “I don’t really see the point of trying too hard to control this disease. It’s pretty too hard to control this disease. It’s pretty obvious to me that I’m going to die soon.”obvious to me that I’m going to die soon.”

Disparities in Diabetes Case Disparities in Diabetes Case # 4# 4
• DE is a 61 year-old white male from Elizabethton, DE is a 61 year-old white male from Elizabethton, who presents to Diabetes Clinic. He is “tired”, who presents to Diabetes Clinic. He is “tired”, since he walked from Elizabethton: his truck is since he walked from Elizabethton: his truck is old and not running, and he can’t afford to get it old and not running, and he can’t afford to get it fixed. He has no income and no prospects; he fixed. He has no income and no prospects; he gets food through church charity programs. His gets food through church charity programs. His food is usually canned vegetables and fruits, and food is usually canned vegetables and fruits, and a large block of cheese monthly. He loves the a large block of cheese monthly. He loves the cheese, so he eats it 3 times/day until it runs out cheese, so he eats it 3 times/day until it runs out in 2 weeks. His blood pressure is 130/80, his in 2 weeks. His blood pressure is 130/80, his BMI is 29%, but his HbA1c is 14%. Talking to BMI is 29%, but his HbA1c is 14%. Talking to him, you get the impression that he may have him, you get the impression that he may have mild mental retardation.mild mental retardation.

Possible Approaches to Possible Approaches to Addressing DisparitiesAddressing Disparities
• EMR with functional registry (apparently EMR with functional registry (apparently rare) and prevention/CDM promptsrare) and prevention/CDM prompts
• Case managementCase management• Group classes Group classes • Use of chronic care model: planned Use of chronic care model: planned
visits, EBM at point of care, improved visits, EBM at point of care, improved systems of care delivery in the 3 systems of care delivery in the 3 programs/”lean thinking”, support for programs/”lean thinking”, support for self-management by patients, and tap self-management by patients, and tap into community systems--effective into community systems--effective programsprograms