Health Disparities in Cardiovascular Disease Paula A. Johnson, MD, MPH Chief, Division of Women’s...
27
Health Disparities in Cardiovascular Disease Paula A. Johnson, MD, MPH Chief, Division of Women’s Health; Executive Director, Connors Center for Women’s Health & Gender Biology, Brigham and Women’s Hospital Brigham and Women’s Hospital
-
Upload
juniper-lucas -
Category
Documents
-
view
217 -
download
1
Transcript of Health Disparities in Cardiovascular Disease Paula A. Johnson, MD, MPH Chief, Division of Women’s...

Health Disparities in Cardiovascular Disease
Paula A. Johnson, MD, MPHChief, Division of Women’s Health;Executive Director, Connors Center for Women’s Health & Gender Biology,Brigham and Women’s Hospital
Brigham and Women’s Hospital

Causes of Death Among U.S. Blacks, 2001
Cancer 22%
All Other Causes
41%
CVD & Stroke
37%
Source: AHA, Heart Facts 2004: African Americans
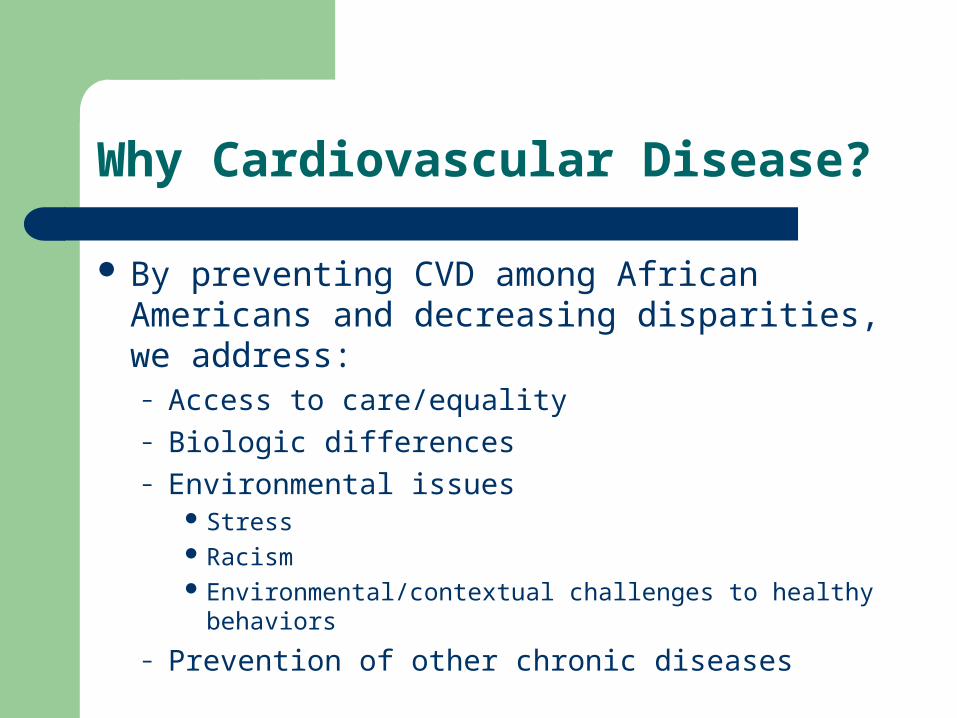
Why Cardiovascular Disease?
By preventing CVD among African Americans and decreasing disparities, we address: – Access to care/equality– Biologic differences– Environmental issues
Stress Racism Environmental/contextual challenges to healthy behaviors
– Prevention of other chronic diseases

Cardiovascular Disease (CVD) in Massachusetts and the United States
CVD, primarily coronary heart disease and stroke, is the leading cause of death for MA blacks and whites, accounting for over 15,000 or about 27% of MA deaths in 2001
In 2001, rates CVD deaths in MA were 18% higher for blacks than whites
Black women tend to develop heart disease at an earlier age and have the highest mortality rate from heart disease of all women
The National Heart Lung and Blood Institute estimates that cardiovascular disease will cost the U.S. $368.4 billion in 2004 in direct and indirect costs
Sources: MDPH, CDC
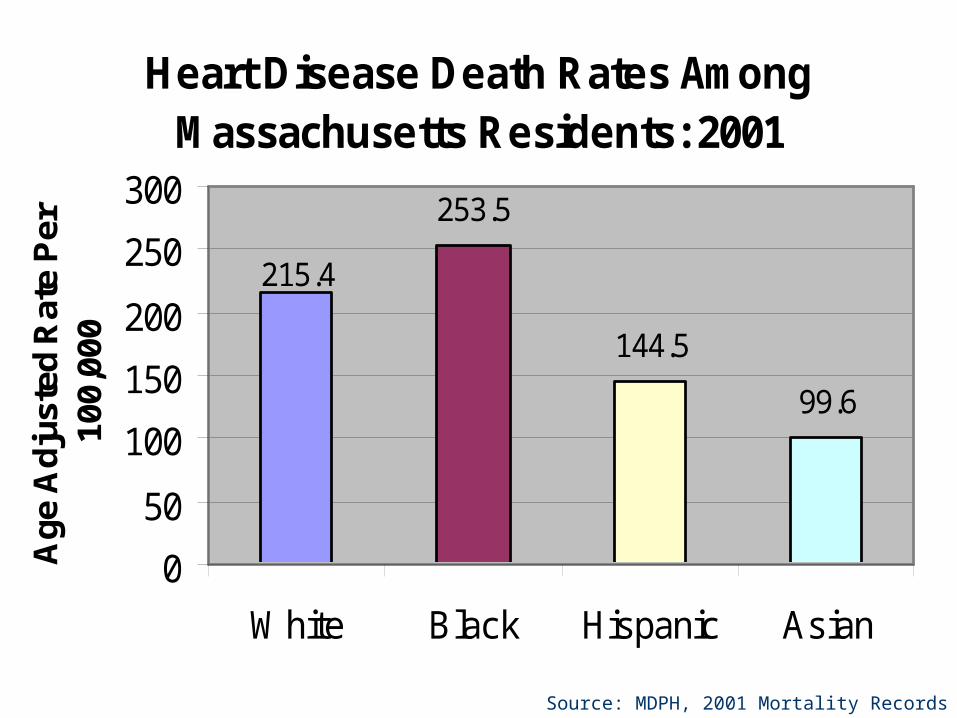
Source: MDPH, 2001 Mortality Records
Heart Disease Death Rates Among Massachusetts Residents: 2001
253.5
144.5
99.6
215.4
0
50
100
150
200
250
300
White Black Hispanic Asian
Age
Adj
uste
d R
ate
Per
10
0,00
0
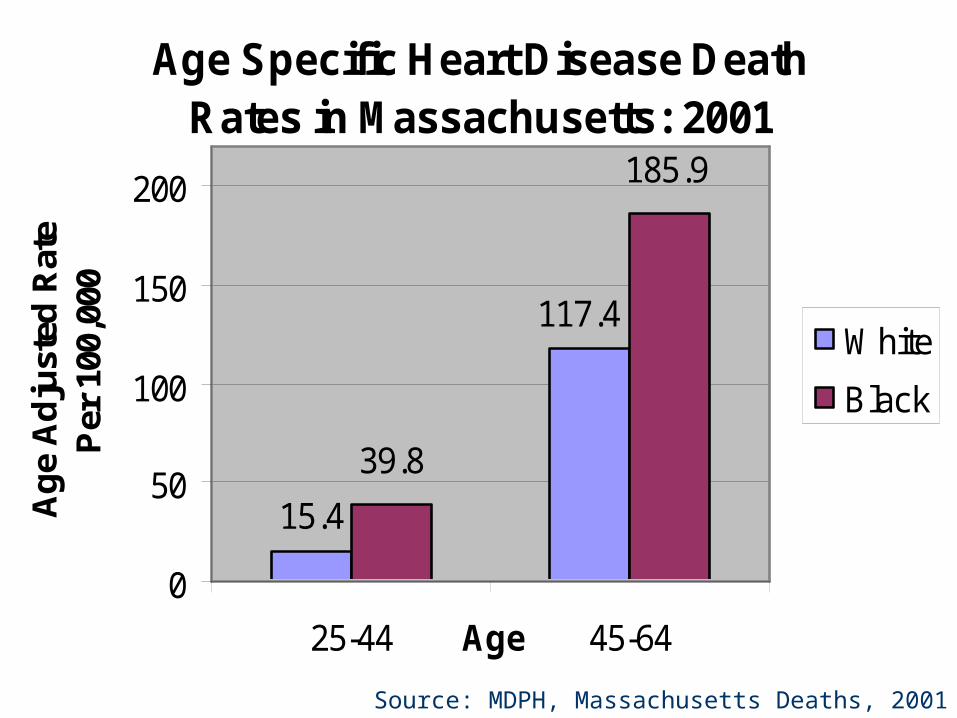
Age Specific Heart Disease Death Rates in Massachusetts: 2001
15.4
117.4
185.9
39.8
0
50
100
150
200
25-44 45-64Age
Ag
e A
dju
sted
Rat
e P
er 1
00,0
00
White
Black
Source: MDPH, Massachusetts Deaths, 2001
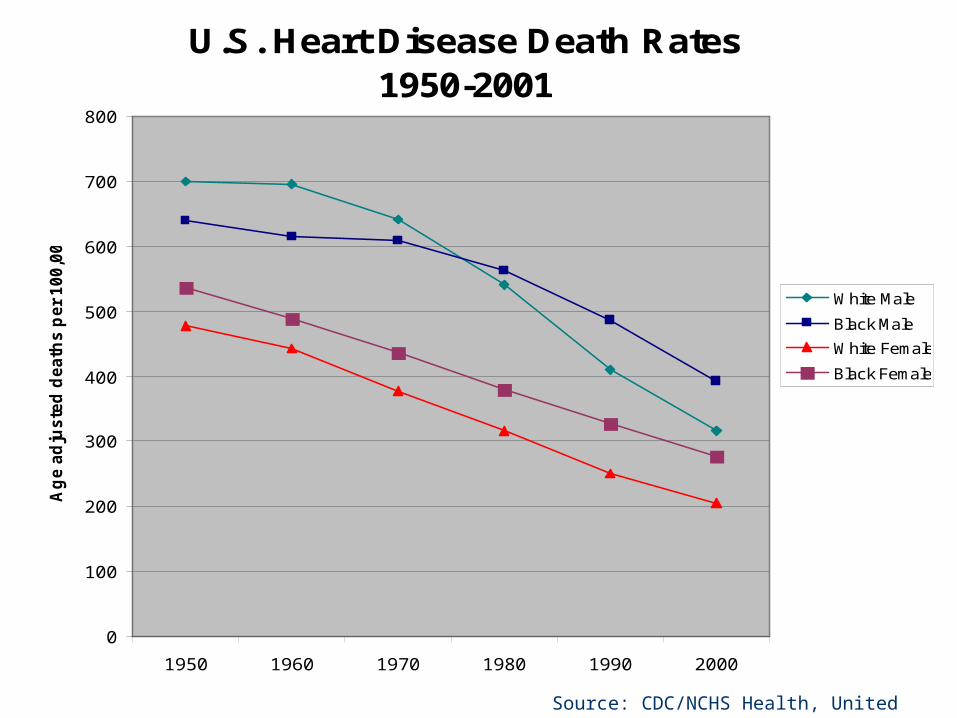
U.S. Heart Disease Death Rates1950-2001
0
100
200
300
400
500
600
700
800
1950 1960 1970 1980 1990 2000
Ag
e a
dju
ste
d d
eath
s p
er
100,0
00
White Male
Black Male
White Female
Black Female
Source: CDC/NCHS Health, United States, 2003
Stroke
Stroke is the third leading cause of death in MA, accounting for 3,534 deaths or about 6% of all deaths in 2001
In 2001, MA blacks were 33% more likely to die of stroke than whites; most of this difference is accounted for by disparities among women, with black women 37% more likely to die from stroke than white women
Source: MDPH, MA Deaths, 2001

Source: MDPH, Massachusetts Deaths, 2001
Stroke Deaths by Race Massachusetts: 2001
36.6
49.2
20.2
65.4
0
10
20
30
40
50
60
70
80
White Black Hispanic Asian
Ag
e-A
dju
sted
Rat
e P
er 1
00,0
00

Source: MDPH, Massachusetts Deaths, 2001
Stroke Deaths by Race and Gender Massachusetts: 2001
52.053.546.3
63.3
0
10
20
30
40
50
60
70
Male Female
Ag
e-A
dju
sted
Rat
e P
er 1
00,0
00
White
Black

Risk Factors
Approximately 80% of cardiovascular disease is preventable.
Risk factors for CVD include:– Overweight and obesity – Physical inactivity – Diabetes – Cigarette smoking – High blood pressure – High blood cholesterol – Family History– Age

Overweight and obesity
Black adults are more likely than all other race/ethnicity groups to be overweight
Significant disparities exist among women; in 2000, black women were 56% more likely to report being obese or overweight than white women in Massachusetts
Factors that are particularly important include physical activity and a healthy diet
The relationship between stress and obesity is being explored and may have particular relevance for the black community
Sources: US DHHS, MDPH BRFSS 2000

Overweight and Obesity by Race/Ethnicity, Massachusetts - 2002
64.3% 62.9%
29.3%
53.8%
0%
20%
40%
60%
80%
100%
White Black Hispanic Asian
17.8%24.7%
6.5%
30.6%
0%
20%
40%
60%
80%
100%
White Black Hispanic Asian
Overweight Obesity
Source: MDPH, BRFSS, A Profile of Health Among Massachusetts Adults, 2002

Consumption of 5 Servings of Fruits & Vegetables/Day Reported By MA Adults: 2002
29.8% 28.4%32.1%
24.2%
0%
10%
20%
30%
40%
White Black Hispanic Asian
Source: MDPH, BRFSS, A Profile of Health Among Massachusetts Adults, 2002

Physical Inactivity
Physical inactivity is more prevalent among African-Americans than whites
In Massachusetts in 2002, blacks were 21% less likely than whites to report physical activity in the previous month

Source: MDPH, BRFSS, A Profile of Health Among Massachusetts Adults, 2002
Any Exercise Reported in Past Month Massachusetts Adults: 2002
82.7%
68.4%73.9%
53.7%
0%10%20%30%40%50%60%70%80%90%
100%
White Black Hispanic Asian

Diabetes
Adults with diabetes are 2-4 times as likely to die of heart disease than those without diabetes
In 2001, Massachusetts blacks were 3.2 times more likely to be discharged from a hospital with a diagnosis of diabetes than whites
The prevalence of diabetes among blacks in the U.S. has quadrupled during the past 30 years, with increasing incidence in black youths
Approximately 2.7 million or 11.4% of all African Americans aged 20 years or older have diabetes, but one-third of them are unaware of their diagnosis
Sources: ADA, CDC

Diabetes By Hospital Discharge Data in Massachusetts: 2001
352.8
248.4
53.0
109.9
050
100150200250300350400450500
White Black Hispanic Asian
Ag
e A
dju
sted
Rat
e P
er 1
00,0
00
Source: MDPH, Massachusetts Hospital Discharge Data, Fiscal Year 2001
Cigarette Smoking
Cigarette smoking rates are similar among white and black residents of Massachusetts
Whites are more likely to quit smoking than blacks
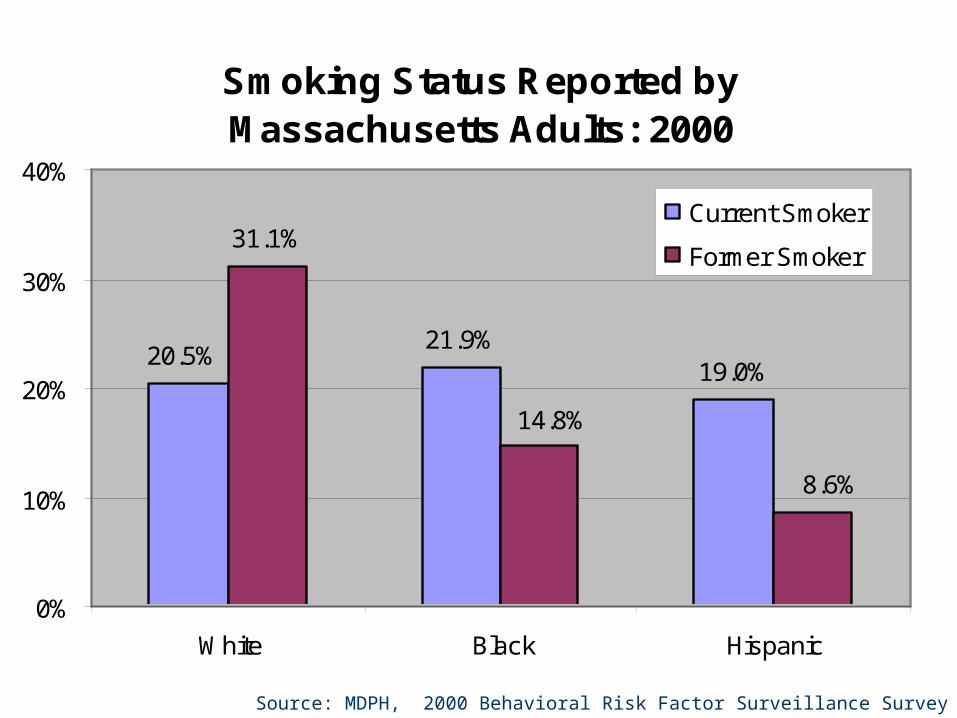
Source: MDPH, 2000 Behavioral Risk Factor Surveillance Survey
Smoking Status Reported by Massachusetts Adults: 2000
21.9%19.0%
31.1%
20.5%
8.6%
14.8%
0%
10%
20%
30%
40%
White Black Hispanic
Current Smoker
Former Smoker
High Blood Pressure (Hypertension)
Those with high blood pressure may have 3-4 times the risk of CHD and 7 times the risk of stroke than those with normal blood pressure
The prevalence of high blood pressure among U.S. blacks is among the highest in the world
Blacks are more likely to develop high blood pressure at an earlier age and to have higher blood pressure than whites
Black women in the U.S. have the highest incidence of hypertension of any race-sex group
Blacks are less likely to have their hypertension controlled than whites, with black women being the least likely (He J et al, Arch Intern Med, 2002;162)
Source: US DHHS
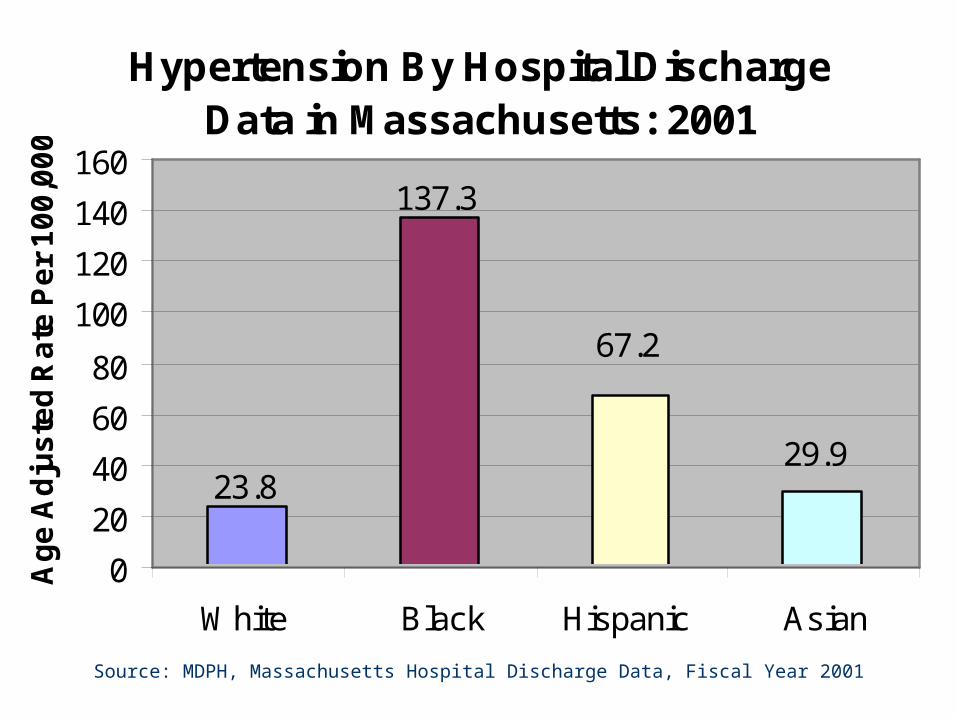
Source: MDPH, Massachusetts Hospital Discharge Data, Fiscal Year 2001
Hypertension By Hospital Discharge Data in Massachusetts: 2001
137.3
67.2
29.923.8
0
20
40
60
80
100
120
140
160
White Black Hispanic Asian
Ag
e A
dju
ste
d R
ate
Pe
r 1
00
,00
0

High Blood Cholesterol
Among African Americans in the U.S., 45% of men and 46% of women have high blood cholesterol
A 10% decrease in total cholesterol levels may result in an estimated 30% reduction in the incidence of coronary heart disease
Blacks tend to have lower blood cholesterol levels than whites

Source: CDC/MDPH, BRFSS 2001
High Cholesterol Reported by Massachusetts Adults: 2001
22.8%
26.9% 27.0%30.6%
20.4%
0%5%
10%15%20%25%30%35%40%
White Black Hispanic Other Multiracial

Screening & Treatment
Blacks are less likely to receive major procedures diagnosing and treating coronary heart disease than whites
Black women are the least likely to have such procedures recommended
Sources: Schulman KA et al, N Engl J Med 1999;340(8); Ayanian JZ et al, JAMA, 1993;269,20; Giles et al, Arch Intern Med 1995;155(3); Johnson PA et al, Ann Intern Med 1993;119(8))

Policy Considerations
Access to medical care Adoption of standards and guidelines for prevention, detection,
treatment and rehabilitation of heart disease for all patients Physician diversity and resident training in cultural and gender
competence Re-investment in tobacco prevention and cessation initiatives Improved access to high quality, heart healthy foods,
especially in rural and urban low-income areas Increased access to safe walking/activity areas and promotion
of innovative strategies to facilitate exercise time
Contact Information
Paula A. Johnson, MD, MPHChief, Division of Women’s Health; Executive Director, Connors Center for Women’s Health and Gender BiologyBrigham and Women’s HospitalPhone: (617) 732-8985, Fax: 264-5191Email: [email protected]
Rachel A. Wilson, MPHDirector of Women’s Health Policy and AdvocacyBrigham and Women’s HospitalPhone: (617) 525-7516, Fax: (617) 525-7746Email: [email protected]