Health care transition (HCT) service models 2014/April webinar/PPT... · Health care transition...
25
Health care transition (HCT) service models Cecily L. Betz, PhD, RN, FAAN Associate Professor Keck School of Medicine Director of Research/Director of Nursing Training USC University Center of Excellence at CHLA Director, Health Care Transition Program, CHLA Spina Bifida Program Editor-in-Chief, Journal of Pediatric Nursing
Transcript of Health care transition (HCT) service models 2014/April webinar/PPT... · Health care transition...

Health care transition (HCT) service models Cecily L. Betz, PhD, RN, FAAN
Associate Professor Keck School of Medicine
Director of Research/Director of Nursing Training USC University Center of Excellence at CHLA
Director, Health Care Transition Program, CHLA Spina Bifida Program Editor-in-Chief, Journal of Pediatric Nursing

Presentation Goal and Objectives
Goal: The audience be acquainted with the current HCT service models and the implications for the provision of services for youth and young adults with ASD
Objectives: The audience will be able to discuss: 1) Comparison and contrast of service features of HCT service models and implications for practice in providing services to YYA with ASD. 2) Identification of the features of best practice HCT service models applicable for YYA with ASD.
2

Types of HCT Service Models

HCT Service Models: Intervention Types
• HCT Coordinator • Facilitate ↑ health literacy, self management, self advocacy
– Develop navigation skills – Implement HCT clinical pathway – Refer to transition and adult services – Facilitate uninterrupted, continuous transfer of care
to adult services
(Betz & Redcay, 2003; Cadario et al., 2009; Holmes-Walker et al., 2007; Parfitt, 2008; Vidal et al., 2004)
4

HCT Service Models: Intervention Types
• AEA-SHCN Instructional Approach – Instruct to ↑ health literacy, self management,
self advocate
(Annunziato et al., 2007; Betz et al., 2010; Cuttell et al., 2005; Gholap et al., 2006; Holmes-Walker et al., 2007; Lane et al., 2007)
5
Health Literacy
Self Advocate
Self Management

HCT Service Models: Intervention Types
• Joint pediatric/adult services – Facilitate uninterrupted, continuous transfer of care
to adult services
– Improve linkages/communication between pediatrics/adult services
– Exposure to adult care in supportive environment
(Cadario et al., 2009; Gholap et al., 2006; Nakhla et al., 2009)
6

HCT Service Models: Intervention Types
• Telephonic/digital approaches Use of text messaging – Provide services and support via
telephone/Internet
(Gholap et al., 2006; Holmes-Walker et al., 2007; Pai & Ostendorf, 2011; Watson et al., 2011)
7

HCT Service Models: Intervention Types
• Transition Clinic – Focus on adolescent issues – Serves as interim step to transferring to
adult care
(Cadario et al., 2009; Gholap et al., 2006; Lane et al., 2007; Pai & Ostendorf, 2011; Watson et al., 2011)
8

Basic Features of HCT Service Models

Two HCT Practice Models (Mennito, & Clark, 2010)
• Youth-adult focused – Focus on developmental needs – Non-Categorical approach – Consideration of biopsychosocial needs
• Disease-specific focused – Interdisciplinary model – One disease type
10

HCT Service Framework/Components

Service Framework (Binks et al., 2007;Watson et al., 2011)
• cus – Family & Youth Centered – Timely/Coordinated – Interdisciplinary Team framework – Time of transfer is established – Long preparation period prior to transfer – Psychosocial/Educational/Vocational – Service Coordination and Referral – Measure and track outcomes of HCT – Facilitate Health Literacy & SM Competencies
12

Research Limitations of HCT Intervention Models

Research Limitations
• Problematic research designs/methods used – Descriptive studies – Cross sectional designs – Limited longitudinal studies – Lack of randomization – Few, if any hypotheses noted – Small sample sizes – Site/provider biases – No power analysis – Tools with weak psychometrics – Missing description of validity and reliability (Betz, & Smith, 2010; Binks et al., 2007; Bloom et al., 2012; Crowley et al., 2010; Pai & Ostendorf, 2012; Wang et al., 2010; Watson et al., 2011)
14

Factors Influencing HCT Outcomes

HCTRC Model
• Individual (AEA-SHCN) Domain • Family/Social Support Domain • Environment Domain
– Community Resources – Educational System
• Health Care System Domain (HCTRC, Betz, Ferris, et al., in press)
16

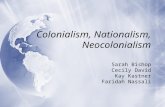
HCTRC Theoretical Model for
Research and Clinical
Practice. (Betz C et. al.
2014)
Environment • Community esources •Service systems
Health Care •PCP (ASD experience) •Specialists (ASD experience) •Number of visits to PCP & specialists per year
•ER and hospitalization use
Family/Social •Extent of family support •Socio-economic Info •Social Support Network
Individual •Comorbidities •Age at diagnosis •Level of severity

Individual Domain (YYA)
• Developmental need for independence – Assume personal responsibility – Becomes the decision-maker – Relies or wants less family involvement – Acquires ADL competencies (money management, cooking,
etc.) – Acquires self management competencies (taking medications) – Age of transfer corresponds to developmental competency
(new providers of adult services) (Betz & Redcay, 2005; Betz et al., 2003; Burra, 2012; Flume et al., 2001; McLaughlin et al., 2008; Reiss et al., 2005)
18

Family/Social Support Domain
• Development of collaborative relationship • Development of shared management • Prominent role as teacher and mentor
– Encourage independence – Provide instruction with learning self management – Role modeling – Serve as case manager, advocate
(Christian et al., 1999; Darrah et al, 2012; Dimitropoulos et al., 2012; Gee et al., 2007; Giarelli et al., 2008; Keickhefer et al., : Luther et al., 2001; Rehm et al., 2012; Reiss et al., 2005)
19

Family/Social Support Domain
• Level of comfort experienced with peers
• Peer support
• Peer role modeling
• Challenges associated with social impairments
(Christian et al., 1999; Giarelli, Bernhardt, Mack et al., 2008; Patterson & Lanier, 1999)
20

Health Care System Domain
• Trusting relationships • Amount of time spent with provider • Communicating directly with YYA • Instilling hope for the future • Initiating and continuing HCT discussion • Providers’ competencies with HCT
(Bloomquist, 2006; Geenen et al., 2003; Hauser & Dorn, 1999; Okumura et al., 2008; Patterson & Lanier, 1999; Reiss et al., 2005; Telfair et al., 2004)
21

Health Care System Domain
• Willingness and commitment to work with one another
• Use of health passports for transfer to adult providers
• Communication amongst transfer providers • Parent-professional partnerships • Interdisciplinary teams
(Flume et al., 2001; Jordan & McDonagh, 2007; LoCasale-Crouch & Johnson, 2005; Patterson & Lanier, 1999; Reiss et al., 2005; Scal & Ireland, 2005)
22

Health Care System Domain
• Care Coordination • Located at comprehensive care centers • Services are comprehensive • Provider HCT training • Release of medical records to adult
providers
(Antonelli et al., 2008; Hauser & Dorn, 1999; Geenen et al., 2003; LoCasale-Crouch & Johnson, 2005; Okumura et al., 2008)
23

Environment Domain
• Access to Health Insurance • Disability legislation, i.e. ADA; Rehabilitation
Act • Federal and State support employment training
and placement systems, i.e. WIA • IEP, 504 Plans, Disabled Student Services
(Betz, & Redcay, 2005; Haverman et al. 2012; Lotstein et al., 2005; Callahan & Cooper, 2006, 2007; Maslow et al., 2011; Shuttuck et al., 2012)
24

HCT Outcomes: Challenges
• Problematic research designs/methods used
–Service vs AEA outcomes –Difficulty operationalizing
outcomes –Limited longitudinal studies (Betz, & Smith, 2010; Binks et al., 2007; Bloom et al., 2012; Crowley et al., 2010; Pai & Ostendorf, 2012; Wang et al., 2010; Watson et al., 2011)
25