
Health Care and Education Access of Transnational Children ...
49
Southern Methodist University Southern Methodist University SMU Scholar SMU Scholar Mission Foods Texas-Mexico Center Research Mission Foods Texas-Mexico Center Winter 12-7-2020 Health Care and Education Access of Transnational Children in Health Care and Education Access of Transnational Children in Mexico Mexico Catalina Amuedo-Dorantes Laura Juarez Follow this and additional works at: https://scholar.smu.edu/texasmexico-research Part of the Education Policy Commons, Health Policy Commons, International Relations Commons, Latin American Studies Commons, and the Public Policy Commons This document is brought to you for free and open access by the Mission Foods Texas-Mexico Center at SMU Scholar. It has been accepted for inclusion in Mission Foods Texas-Mexico Center Research by an authorized administrator of SMU Scholar. For more information, please visit http://digitalrepository.smu.edu.
Transcript of Health Care and Education Access of Transnational Children ...

Southern Methodist University Southern Methodist University
SMU Scholar SMU Scholar
Mission Foods Texas-Mexico Center Research Mission Foods Texas-Mexico Center
Winter 12-7-2020
Health Care and Education Access of Transnational Children in Health Care and Education Access of Transnational Children in
Mexico Mexico
Catalina Amuedo-Dorantes
Laura Juarez
Follow this and additional works at: https://scholar.smu.edu/texasmexico-research
Part of the Education Policy Commons, Health Policy Commons, International Relations Commons,
Latin American Studies Commons, and the Public Policy Commons
This document is brought to you for free and open access by the Mission Foods Texas-Mexico Center at SMU Scholar. It has been accepted for inclusion in Mission Foods Texas-Mexico Center Research by an authorized administrator of SMU Scholar. For more information, please visit http://digitalrepository.smu.edu.

Health Care and Education Access of Transnational Children in Mexico
Catalina Amuedo-Dorantes and Laura Juarez*
December 7, 2020
Abstract
Between 2001 and 2018, more than 5.5 million Mexican migrants were removed from the United States or returned to Mexico with their families as immigration enforcement escalated. Learning how this transition affected the access to health and education services of their children –also referred to as “the invisibles”– is a policy-relevant topic for both the United States and Mexico. Using representative data on 7.6 million Mexican and U.S.-born children from the 2015 Mexican Intercensal Survey, we provide evidence on the education and health care access gaps between these two groups and on the factors potentially responsible for the barriers encountered by the latter. Relative to children born in Mexico, U.S.-born children are at a considerable disadvantage in terms of health care access, but less so in terms of education access. Lack of a Mexican issued birth certificate is among the factors responsible for gaps in services that can prove persistent. Policies aimed at changing the approach to immigration enforcement in the United States, lessening paperwork requirements in Mexico and easing access to documentation in both countries could be helpful in improving transnational children’s access to basic services, thus promoting their present and long-term well-being.
JEL Codes: I13, I14, I24, F22. Keywords: health care, education, “invisible children”, U.S.-born children in Mexico.
(*) We are grateful to SMU Mission Foods Texas-Mexico Center for their financial support. Authors’ contact information: Catalina Amuedo-Dorantes, Economics and Business Management, University of California Merced, 5200 North Lake Rd., Merced, CA 95343. Email: [email protected] Laura Juarez, Centro de Estudios Económicos, El Colegio de Mexico, Carretera Picacho-Ajusco, Carretera Picacho Ajusco 20, 14110, Mexico City. E-mail: [email protected]

1
1. Introduction
Between 2001 and 2018, more than 5.5 million Mexican migrants were removed from the
United States or returned to Mexico with their families as immigration enforcement escalated
(Nowrasteh, 2019). Learning how this transition affected their children’s (most of them U.S.
citizens) access to health and education services is a policy-relevant topic for both the United States
and Mexico, as well as for the border region. In this paper, we address this important policy issue,
providing evidence on the access to health and education services of U.S.-born children who were
living in Mexico in 2015, and on factors potentially responsible for encountered barriers.
Approximately 400,000 Mexican migrants were removed from the United States on a
yearly basis during the 2008-2012 period alone because of intensified interior immigration
enforcement (Gonzalez-Barrera, 2015). Many deportees were long-term migrants who had been
in the United States for more than ten years. They had permanently settled in the country, formed
families, and had children who were U.S. citizens and only knew one country –the United States.
Suddenly, these families found themselves in Mexico. Many parents lacked the documentation
needed to access education and health services (Shaw, 2016). Their children were attending a
school system they did not know (Román González and Zúñiga, 2014; Zúñiga and Hamann, 2015).
Several studies and policy reports have documented the challenges encountered by these children
–a group referred to as “Los Invisibles” or the “Invisible Ones”. This term has been emblematic
of children who are U.S. citizens, have lived most of their lives in the United States, but now reside
in Mexico (Cave, 2012; Sanchez, 2016; Hwang, 2017). Despite constituting a non-negligible
population estimated at 430,000-600,000 back in 2018 according to Mexico’s Ministry of the
Interior (Cruz, 2018; Shaw, 2016), their experience has been largely overlooked in the literature

2
on migration between the United States and Mexico, in part due to the limited data on these
transnational children.
In this study, we provide evidence on the assimilation of these children back in Mexico by
assessing their access to healthcare and education services, which are essential for their present
and future well-being. To start with, we render a deeper understanding of how such access depends
on selected child and family traits, including their age and gender, their household head’s
educational attainment, their place of residence five years ago, their approximate return date to
Mexico and whether they have proper documentation. To that end, we rely on data from the 2015
Intercensal Survey (Encuesta Intercensal 2015, EIC), a Mexican representative dataset at the
national, state, and municipal levels. We initially work with a sample of both Mexican and U.S.-
born children (about 7.6 million observations) to examine any gaps in their access to health and
education services. As a second step, we focus on U.S.-born children to explore the mechanisms
that could potentially explain such gaps on their access to basic services, i.e. the effects of lack of
proper documentation, the length of time they have been in Mexico, and the interaction of both
factors.
We find that, on average, U.S.-born children are 28% less likely than their Mexican
counterparts to be affiliated with any health care provider. U.S.-born children whose household
head has less than high school education are less likely to be affiliated than those whose household
head is more educated. Among children who are affiliated, U.S. born children are also less likely
to be affiliated with, and receive health care from, a public health care provider and more likely to
have a private or other kind of health care provider. We examine the factors driving these
differences in health care access and find that lack of proper documentation plays a vital role.
U.S.-born children with a foreign or no birth certificate are 62% and 67% less likely to be affiliated

3
to a health care provider than similar children with a Mexican birth certificate, respectively.
Although this documentation barrier seems to be slightly worse for children whose household head
arrived more recently to Mexico (between 2010 and 2015), we find that its negative impact persists
even among children whose household head arrived before 2010, which is particularly worrisome.
In terms of education, we find that U.S.-born children are not at a significant disadvantage,
compared to their Mexican counterparts. For instance, elementary-school children (ages 6 to 12)
display similar access and outcomes, regardless of their country of birth. Furthermore, among
older children, ages 13 to 17, those born in the United States are more likely to attend school, to
be at an age-appropriate school level and, in turn, exhibit smaller educational lags than those born
in Mexico. The advantage of U.S.-born teens is observed for both males and females, but it is
significantly smaller for the latter. Nevertheless, among U.S.-born children, lack of proper
documentation still seems to be keeping some of these “invisible children” out of school and
pushing them into other activities, like working for pay (mostly for males), or at home (for
females).
In sum, we find that U.S.-born children are at a considerable disadvantage in terms of health
care access, but less so in terms of education access, compared to their Mexican-born counterparts.
The differential access to education and health services could be related to a couple of factors.
First, the Mexican educational system is highly centralized in comparison to the health care
system, a trait that favors a quick response to policy challenges posed by the influx of transnational
children. Second, the educational barriers faced by these “invisible children” received much more
attention in the academic literature, creating greater awareness among policymakers. In contrast,
the empirical evidence on their health care access has been sparser.

4
We contribute to the academic and policy discussion about the assimilation of transnational
children by providing comprehensive evidence of the access to education and health care services
of transnational children when their parents return to their origin countries. Unlike most of the
previous studies on transnational children’s access to education, we use nationally representative
data, moving beyond a descriptive analysis by providing estimates of the impact of selected
parental and child characteristics on such access in Mexico, conditioning on a host of relevant
traits. Moreover, we add to the scarce evidence on healthcare affiliation and access when sick of
transnational children, exploring the barriers encountered when accessing both health care and
education services. Specifically, we provide empirical evidence of the role played by lack of
proper documentation and its interaction with residence time in Mexico as access barriers that can
inform future policy. Considering the uncovered barriers to basic services, various policy
approaches could be suggested. In the United States, a more targeted or prioritized immigration
enforcement approach, versus an indiscriminate communitywide approach (e.g. raids), could prove
critical in providing many transnational children the opportunity to grow up in the only country
they know. Once in Mexico, given the lack of significant gaps in their school access, the Mexican
government could explore the possibility of focusing its efforts on easing documentation barriers
to improve health care access among transnational children through its schools.
The literature has documented the long-term impacts of both proper health care and
educational investments during childhood on a wide array of lifetime outcomes ranging from better
employment opportunities, higher earnings, and lower program participation to a lower incidence
of medical conditions and diseases, as well as better health behaviors and improved health status
(e.g. Becker and Chiswick, 1966; Clark and Royer, 2013; Hoynes, Schanzenbach, and
Almond, 2016). Given that binational children are citizens of both Mexico and the United States,

5
both countries should be concerned about their long-term well-being, which can be badly damaged
by the indiscriminate removal of family members from the United States or by their limited access
to basic services once they are in Mexico.
2. Historical and Institutional Background
A) Returns to Mexico amid Intensified Immigration Enforcement
The past three decades have witnessed an unprecedented increase in interior immigration
enforcement in the United States responsible for large numbers of removals. A series of laws in
1996, including the Antiterrorism and Effective Death Penalty Act and the Illegal Immigration
Reform and Immigrant Responsibility Act, laid the ground for deporting more immigrants. The
first policy did so by expanding the list of offenses that would be considered criminal acts that
could be penalized with deportation (Stephens, 2012). The second policy further extended the
regulation of grounds for deportation, establishing penalties for illegal entry and re-entry and,
perhaps most importantly, laying the framework for posterior cooperative agreements between
local and state law enforcement agencies with federal immigration officials (Chishti, Pierce and
Bolter, 2017; Rohald and Lopez, 2014).
Most of this machinery deployed in the aftermath of 9/11. For instance, beginning in 2002,
the federal government started to use the so-called 287(g) agreements enabling local and state law
enforcement agencies to cooperate with federal officials in the enforcement of immigration law.
One year later, in 2003, Congress created the Department of Homeland Security (DHS), which
had three main bodies: U.S. Customs and Border Protection (CBP), Immigration Customs
Enforcement (ICE), and Citizenship and Immigration Services (CIS). CBP and ICE are
responsible for most removals. CBP focuses on border apprehensions, whereas ICE focuses on
interior immigration enforcement. The latter quickly expanded after the mid-2000s through the
6
decentralized adoption of interior immigration enforcement initiatives by states and counties,
including 287(g) agreements and the Secure Communities program –a program that allowed for
the fingerprints of those arrested by law enforcement to be matched against federal immigration
and criminal databases from DHS and the Federal Bureau of Investigation (FBI). These two
initiatives alone were responsible for a record high 360,000 formal removals in Fiscal Year 2008,
with about 234,000 of them occurring in the interior of the United States (Chishti, Pierce and
Bolter, 2017). With increased funding, removals only kept rising during the much of President
Barack Obama’s Administration, whereas returns and U.S.-Mexico border apprehensions kept
decreasing with regards to those in the Clinton and Bush’s Presidencies.
The dynamics detailed above had important consequences. One of them, byproduct of the
overall buildup of immigration enforcement, was the decision by many immigrants to permanently
settle in the United States as opposed to come and go as they had done decades earlier (Hagan,
Eschbach, and Rodriguez, 2008). A second one, resulting from the increased volume of
deportations, especially removals from the interior of the United States, was the breakup and
separation of families. From 1995 through 2017, the share of the undocumented population with
10+ years in the United States rose from 33% to 66% (Passel and Cohn, 2019). Among those of
Mexican origin, that share averaged 83% (Gonzalez-Barrera and Krogstad, 2019) –possibly
unsurprising given the long history of Mexican migration to the United States since the Bracero
Program in the 1960s. Because of the duration of their migration spell, these migrants were more
likely to have communal and familial ties in the country, as well as children who were U.S.
citizens.1
1 In 2018, an estimated 5.1 million U.S. citizen children had at least one undocumented parent (Passel, Cohn and Gramlich, 2019).

7
While many parents were removed and separated from their children, other families opted
to return to Mexico with their families (Medina and Menjívar, 2015). According to Mexico’s 2010
Population Census, more than 360,000 of Mexico’s international migrants returned home between
2005 and 2010 (INEGI, 2010). This pattern is also supported by other surveys, like the Encuesta
sobre Migración en la Frontera Norte de México (Survey on Migration in the Northern Border of
Mexico). Based on its 2005–2010 border estimates, the number of returnees increased from
817,000 to 887,000 (Emif Norte, 2015). Furthermore, many of the returnees were U.S.-born
children. Between 2000 and 2010, the foreign population in Mexico rose from 500,000 to 960,000
(INEGI, 2010). Approximately 22% of them were children between 5 and 14 years of age, most
of whom were born in the United States (INEGI, 2010).
B) Access to Health Care and Education in Mexico
To better understand and contextualize the difficulties faced by families with U.S.-born
children relocating to Mexico, we review the institutional features of the Mexican health care and
education systems, as well as some government programs targeting migrants and their families.
The Mexican health care system is composed of public and private institutions. In turn,
public health care institutions can be broadly classified into a contributory segment tied to formal
employment in the private or public sectors, and a non-contributory segment aimed at providing
care to the uninsured population. Therefore, access requirements and quality of care differ among
public health care providers.
Two institutions dominate the contributory public health care segment: the Mexican
Institute of Social Security (IMSS) for private-sector salaried employees, and the Health and Social
Security Institute for Government Employees (ISSSTE) for employees of the federal government.
Smaller public institutions cover salaried employees in the military, Pemex (the public oil

8
company) and state governments. By law, employers must register their eligible employees with
the corresponding social security institution. Then, workers, employers, and the federal
government pay contributions and, in return, registered workers gain access to various fringe
benefits, including health care services for themselves and their families. However, due to non-
compliance, access to this type of health care coverage is limited. In addition, affiliated individuals
must register in the closest health clinic to get health care. As a result, access to these services is
costly in terms of time and paperwork.
The non-contributory segment is mostly run by the Ministry of Health (Secretaría de Salud,
SSA) at the federal level. State governments are also in charge of some clinics and hospitals for
the uninsured. Between 2002 and 2015, Seguro Popular (Popular Insurance, SP) was the main
government program providing health care access to the uninsured. Given that our data is from
2015, we describe how SP operated up to that year.2 The SP program expanded both the number
of health interventions, including prescription drugs, that would be provided free of charge to
affiliated families, and increased the resources devoted to health care for the uninsured.3
According to Frenk et al. (2009), SP covered about 90% of the services demanded at public clinics
and hospitals. Under this scheme, state governments provided health care in their health facilities
and the federal government provided funds, according to the number of beneficiaries. By 2010,
SP operated in all states. Individuals had to pay premiums to insure their families through SP, but
the first three income deciles were exempt from payment.
2 The current administration, which took office at the end of 2018, is implementing significant changes in the health care system and, as such, the SP program no longer operates as it did before. 3 Before Seguro Popular, some health services were provided to the uninsured population by both federal and state public hospitals, but they were restricted to emergency care and other basic medical procedures. The patients would pay for medications and for any additional care.

9
In principle, anyone not covered by a contributory system could affiliate to SP. To do so,
one must present originals and copies of several official documents, like a unique population
registry number (Clave Única de Registro de Población, CURP) or birth certificate, an official ID,
and a document validating her address at the closest affiliation booth.4 To affiliate children,
parents must present their CURP or birth certificate.5 These requirements could be a challenge for
families with U.S.-born children, especially if they relocated to Mexico in a rushed manner.
Private health insurance is very limited in Mexico. Given the cost and quality issues
surrounding the IMSS health care, a small share of high-income salaried workers in the private
sector get employer-provided private health insurance, usually on top of IMSS benefits. This
insurance usually covers major health events and expenses. For most day-to-day health care and
minor health issues, those who can afford it go to private doctors and pay out-of-pocket. In
addition to doctors in private hospitals and clinics, pharmacy-adjacent doctor offices expanded in
Mexico, particularly after 2010, and are quite common (Rubli, 2020). In these doctor offices,
patients pay either small or no consultation fees because they usually buy their prescriptions there
too.
Between 2000 and 2015, the federal government had several programs to provide health
care access to Mexican migrants and their families.6 The program Vete Sano y Regresa Sano
(Leave Healthy and Come Back Healthy) provided health information and primary care to
migrants and their families. Seguridad Social para Mexicanos en el Extranjero (Social Security
4 Although foreign official IDs are not explicitly excluded, the list of accepted IDs include mostly those issued by Mexican authorities: voter ID, passport, driver’s license, professional license, military service card, consular registration card (matrícula consular), or ID from the National Institute for Older Adults (Instituto Nacional de las Personas Adultas Mayores, INAPAM). 5 Please refer to: https://www.gob.mx/salud/seguropopular/documentos/sabes-cuales-son-los-requisitos-para-afiliarte-al-seguro-popular-resuelve-tus-dudas-respecto-a-afiliacion-renovacion-cobertura-y-mas 6 Giorguli et al. (2014) provide an overview of the different programs and actions that the Mexican government has implemented for migrants and their families, both at the federal and the state level. Please refer to Cuadro 3 of their work.
10
for Mexicans Abroad) provided IMSS health care coverage to Mexican workers abroad, and once
they return to Mexico, as well as to family left behind in Mexico. Seguro Popular para Migrantes
(Popular Insurance for Migrants) also provided health care coverage, through the SP program, for
the migrant’s family living in Mexico.
The education system in Mexico is more centralized than the health care system,
particularly at lower education levels,7 which include preschool (ages 3 to 5), primary school (ages
6 to 12), and middle school (ages 12-15). Overall, the Ministry of Education (Secretaría de
Educación Pública, SEP) regulates public and private schools at the federal and state levels. SEP
controls key aspects of education at lower levels, like the curricula, and teachers’ compensation
and promotion. By law, education is compulsory from preschool to high school (ages 15-18), but
enrollment is universal only at the primary level.8 Due to SEP’s prominent role, the system is
more integrated at lower educational levels than at the high school level, where three different
subsystems provide some diversity in the type of curricula.9 However, a lack of coordination
between these subsystems makes it hard for students to transfer from one type of high school to
another. In addition, whereas progression between primary and middle school depends mostly on
having the primary education certificate, the transition to high school depends primarily on passing
an admission exam on top of presenting the middle school certificate.
For migrant children, since the 1980s, the Mexican government started the Binational
Program of Migrant Education Mexico-USA (Programa Binacional de Educación Migrante
México-EUA, PROBEM) aimed at easing the school transitions of students who move between
7 The description on the structure of the Mexican education system in this paragraph is based on SEP (2000). 8 In Mexico, primary education has been compulsory since the end of the 19th century. Middle school became compulsory in 1993, preschool in 2009, and high school in 2012. 9 These subsystems are general high school (bachillerato general), technical high school (bachillerato tecnológico), and technical-professional education (educación profesional técnica).

11
the two countries during the academic year. Since 1995, both countries agreed on the Transfer
Document for Binational Migrant Student USA-MEXICO (Documento de Transferencia del
Estudiante Migrante Binacional México-EUA, DT), which is a binational official transcript that is
accepted in both countries. To obtain a DT, a person must present a report card or official transcript
from the last grade completed and, in some cases, from previous grades. For some of these
documents, an official translation to Spanish and an apostille used to be required.10 Thus, for some
students, the DT by itself might not have eased the barriers to access education in Mexico. Because
of this, SEP eased the requirements to incorporate binational students to Mexican schools. For
instance, it allowed schools to accept a student from a foreign school even without proper
identification documents or academic proof of their last grade completed. However, in practice,
such top-down regulations at the federal level seem not to have permeated at the school level.
Enrollment is still denied based on a lack of proper documents or a lack of spots, particularly in
urban areas, where schools are already at full capacity (Vargas Valle, 2019). Although parents
could, in principle, complain and look for support at one of SEP area offices, they usually do not
due to lack of information or time.
The Mexican government has continued to tackle the barriers faced by binational children
in accessing essential services by easing requirements and promoting proper documentation in
Mexico. In 2015, it eliminated the apostille requirements and the official translation of school and
identity documents for enrolling children in Mexican schools and recognizing their completed
grades at the basic and high school levels.11 And, in 2017, a presidential initiative removed these
10 For primary, the DT requires presenting the report card or official transcript of the last grade completed; for middle school (grades 7th-9th), the report or official transcript of both 6th grade and the last grade completed; for high school, the report or official transcript of 6th-9th grades, and the official transcript for the grades 10th-12th completed. In the latter case, the official transcripts for grades 10th-12th had to be translated and apostilled. 11 Acuerdo Secretarial 286 de la SEP sobre las normas para la acreditación, certificación y revalidación de los estudios cursados en el extranjero en el nivel básico y media superior

12
requirements at the college level and increased the flexibility of other admission requirements.
Since 2016, other efforts have focused on promoting the registration of U.S.-born children who
have at least one Mexican parent and, thus, qualify for binational status in Mexico.12 However,
most of these changes took place after 2015 –the year corresponding to our data. As a result, we
find that the lack of proper documentation is a significant hurdle for these children when accessing
health and education services in Mexico. Besides, despite these government efforts to foster the
assimilation of U.S.-born children in Mexico, results have been limited by lack of information,
resources, or consistency (Giorguli et al. 2014; Vargas Valle, 2019). For instance, Giorguli et al.
(2014), after reviewing the array of government programs for migrants and their families, conclude
that no clear and comprehensive policy aimed at incorporating them fully to the work, education
and social realms exists either at the federal or at the state level in Mexico.
3. Literature on the Healthcare Access and Schooling of U.S.-born Minors in Mexico
A recent, yet rapidly growing, literature has addressed the role of interior immigration
enforcement on accessing health care in the U.S. and on the educational attainment of U.S. born
children with likely undocumented migrant parents from Mexico and Central America (e.g.
Watson, 2014; Amuedo-Dorantes and Antman, 2017; Amuedo-Dorantes and Lopez, 2017;
Amuedo-Dorantes and Sparber, 2014; Koohi, 2017). However, evidence on the adaptation to life
in Mexico of the so-called ‘invisible’ children –namely, those who left the United States after their
parents were deported or returned voluntarily to Mexico, has been relatively scarce (Cruz, 2018).
For instance, existing work has described the experiences and challenges faced by these
children at Mexican schools, relying on student surveys, in-depth interviews of students and
12 The program “Soy Mexico. Registro de Nacimiento de la Población Mexicano-Americana” (I am Mexico. Birth registration of the Mexican American Population) allows the online validation of U.S. birth certificates, to make it easier for Mexican-American individuals to obtain a Mexican birth certificate and CURP.

13
teachers, visits and on-site observation in schools in selected Mexican states (Sanchez García and
Zúñiga, 2010, for Nuevo León and Zacatecas; Zúñiga and Hamman, 2013, for Puebla and Jalisco;
or Panait and Zúñiga, 2016, for Zacatecas; or Medina and Menjívar, 2015). Despite their focus on
selected populations, i.e., children enrolled in Mexican schools in a sample of states at the time of
the study, these studies provide a vivid picture of the hardships and mixed feelings experimented
by children after transitioning from the United States to the Mexican education system. They
document the specific barriers faced by many of these transnational students, who in name and
appearance are like other Mexican students with no international experience, such as linguistic
adaptation and lack of documentation to register at school. By using the 2015 EIC data, we
quantify the gaps in education outcomes, caused by these barriers, between Mexican and U.S. born
children nationwide, thus providing a more comprehensive and representative picture of some of
the educational challenges endured by transnational children in Mexico.
Regarding access to health care, the literature has shown that Mexican migrants returning
from the United States have a higher probability of lacking such access compared to pre-departure
(Donate et al. 2017). This lack of access is, in part, related to returnees’ failure to get jobs
providing health insurance, compared to non-migrant Mexicans (e.g. Masferrer et al., 2017; Aguila
et al. 2015) –a circumstance that could negatively impact the health care access of their
dependents, e.g. their children. Yet, Donato and Duncan (2011) find no statistically significant
differences in a subjective measure of health between children who lived in the United States and
returned to Mexico, compared to children who always lived in Mexico. Nevertheless, their data
covers the period 1995-1997 –a period during which return migration flows differed from those in
recent years. In addition, it focuses on a subjective measure of health, as opposed to health care
access and use.

14
In a recent study, Wassink (2020) documents the lower health insurance coverage of U.S.-
born minors living in Mexico, as well as their greater reliance on private insurance, especially
among those who arrived during the past year, using data from Mexico’s 2018 National Survey of
Demographic Dynamics (ENADID, N=78,370). Besides other differences in the data used and
the estimation methods, we add considerably to the evidence provided by this previous study in
several ways. By using data from the 2015 EIC, we benefit from a much larger sample to unveil a
more representative picture of children’s health insurance, and also on their actual health care use
when they are sick. In addition, we explore whether these health care gaps between Mexican and
U.S. born children vary with the age and gender of the child and the education of her household
head. Finally, we examine whether the lack of proper documentation, and its interaction with the
residence time in Mexico, play a role in explaining access barriers.
Summarizing, the contribution of this study is threefold. First, we quantify the gaps in the
school outcomes of transnational migrant children in Mexico, compared to non-migrant Mexican
children, using nationally representative data. Thus, we provide a broader and thorough picture of
access barriers and their implications in terms of school attendance and educational delays.
Second, we move beyond a descriptive analysis and provide estimates of the impact of selected
parental and child characteristics on transnational children’s access to education services in
Mexico, conditioning on a host of relevant traits. Finally, besides education access, we add
considerably to the scarce evidence on healthcare affiliation and access when sick of the so-called
‘invisible’ children in Mexico. Importantly, for all outcomes we explore the role played by the
lack of proper documentation, and its interaction with residence time in Mexico, as mechanisms
that can hint on policies to address access barriers.
15
4. Data
We use data from the 2015 Intercensal Survey (Encuesta Intercensal 2015, EIC), collected
by the Mexican Institute of Statistics and Geography (Instituto Nacional de Estadística y
Geografía, INEGI) as an intermediate survey between the 2010 and 2020 full Mexican population
Censuses. The EIC survey has a sample of about 6 million Mexican dwellings, and it is
representative at the national, state, and municipal level. Also, it is representative at the locality
level for those with 50,000 or more inhabitants. The data was collected during March 2015.13
For our study, the EIC data present several advantages. First, it has information on our
outcomes of interest, namely, health care and education outcomes. Second, we can identify U.S.-
born children because, for each household member, the survey asks about the state of birth, if the
person was born in Mexico, or the country of birth if she was born abroad. Third, the survey has
information on whether each person holds a birth certificate and whether it was issued in Mexico
or the United States. This allow us to gauge the extent to which the lack of proper documents is a
barrier to access health and education services in Mexico among U.S.-born children. Fourth, we
can observe where each household member lived in 2010 –that is, five years prior. This enables
us to identify if U.S.-born children and the head of their households arrived recently (between
2010 and 2015) or not (before 2010) and, in turn, explore their progression of access to education
and health care services. Furthermore, by looking at the interaction of residence time in Mexico,
proxied by this information on the period of arrival, and the lack of proper documentation we
gauge if families are able to overcome the latter over time, or if it remains an integration barrier
for quite some time.
13 For more information on the EIC survey, please refer to: https://www.inegi.org.mx/programas/intercensal/2015/

16
More specifically, the EIC survey asks whether each person is affiliated with any health
care provider and the type, whether she received health care when sick and where. Thus, we use
dummies for whether the child is affiliated with any health care provider. According to the
discussion in section 2B, for children who are affiliated, we look at the type of health care provider
by creating dummies for each type: public contributory (like IMSS or ISSSTE), public non-
contributory (SP), private, or any other kind. We also examine the probability of getting health
care when sick and, for those who got care, we follow the same classification to look at which type
of health care they got.
For household members age 3 and older, the survey also has information on whether they
attend school and the last grade achieved. We use the last grade achieved, together with the child’s
age, to construct a dummy variable for whether the child is at an age-appropriate grade, and another
variable measuring the number of years that she is lagging. For these variables, we assume that a
child is 6-7 years old in first grade, 7-8 years old in second grade, and so on. As a result, the age-
appropriate grade dummy is equal to 1 if we observe that the last grade achieved corresponds to
this age-grade schedule. For the variable measuring the years of educational lag, we construct the
minimum educational attainment that a child should have, based on her age, and then take the
difference between her actual last grade completed and this minimum.
Our sample consists of children ages 0 to 17 when examining their access to health care,
and of children 6 to 17 years old for schooling outcomes. The EIC collects information on work
outcomes for all individuals who are at least 12 years old. Thus, as complementary evidence, we
look at the probability of working for pay or at home for children age 12 to 17.
As detailed in the next section, in the first part of our analysis, we use a sample of both
Mexican and U.S.-born children (about 7.6 million observations) to compare their access to health

17
and education services. In this part of the analysis, we exclude households that have children who
were born in any other country (6,765 child observations, 0.08% of the sample). Subsequently, in
a second part of the study, we focus on U.S.-born children to explore the effects of lack of proper
documentation, the accumulated time of residence in Mexico, and the interaction of both factors,
on their access to basic services. Our interest is on children who were living in either the United
States or Mexico in 2010, five years before the EIC survey; therefore, we exclude U.S.-born
children who were living in any other country in that year (17,957 observations, 16.7% of the U.S.-
born sample). We also exclude household heads living in any other country in 2010 (478
observations, 0.44% of the sample)
Finally, the EIC data allow us to account for a rich set of individual and household traits in
our analysis. As detailed in the next section, we control for personal characteristics of the child,
for the presence of her parents at home, and for relevant household sociodemographic
characteristics, including the size and number of children in different age groups in the household.
In our estimations, we also control for the characteristics of the household head, instead of those
of her parents, to avoid dropping observations since the survey only collects parental
characteristics for parents who live in the same household as the child.14
5. Methodology
Broadly speaking, our analysis consists of two parts. For the first part, we use a sample of
Mexican and U.S.-born children to gauge if children born in the U.S. have lower access to health
and schooling services. To that end, we estimate different versions of the following model:
(1) 𝑌𝑌𝑖𝑖ℎ𝑚𝑚 = 𝛼𝛼 + λ𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑖𝑖 + 𝑋𝑋𝑖𝑖′𝛽𝛽 + 𝑍𝑍ℎ′ 𝛾𝛾 + 𝛿𝛿𝑚𝑚 + 𝜀𝜀𝑖𝑖ℎ𝑚𝑚
14 About 64 percent of fathers and 13 percent of mothers of Mexican-born children are household heads, whereas for U.S.-born children, the corresponding figures are 57 percent and 18 percent, respectively. So, despite these differences, for the majority of children, we are capturing parental characteristics when using those of their household head.

18
where 𝑌𝑌𝑖𝑖ℎ𝑚𝑚 stands for the outcome of interest for the child i in household h in municipality m.
When examining children’s health care access, these outcomes are dummy variables indicative of:
(1) whether the child is affiliated to a health care provider, (2) the type of health care provider, if
affiliated, (3) whether the child received care when sick, (4) and the type of institution that
provided care. Our schooling outcomes are dummies for whether the child: (1) attends school and
(2) is at an age-appropriate school level. We also look at (3) the number of years s/he is lagging
in school.
Our key regressor is 𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑖𝑖 –a dummy variable equal to 1 if the child was born in the
United States and 0 if born in Mexico. The coefficient on this variable measures the gap in
outcomes between these two groups of children. As mentioned before, the EIC data allows us to
include a rich set of individual and household controls. The vector 𝑋𝑋𝑖𝑖′ includes child traits, i.e.
age, gender, indigenous descent, as well as whether the child has both parents at home, only the
mother, only the father, or none of them (the reference category). The vector 𝑍𝑍ℎ includes
information on the household size, the number of children in different age groups; dummies
indicative of whether all children were born in Mexico (the reference category), in the United
States, or in both countries; a dummy for whether the household belongs to the first wealth quintile,
and a dummy for whether the household resides in a rural locality. As discussed in the previous
section, we also control for the characteristics of the child’s household head, including age, years
of education, gender, indigenous descent, information on whether s/he was born in Mexico or
abroad, and whether s/he lived in Mexico in 2010. Finally, the model in equation (1) includes
municipal fixed effects (𝛿𝛿𝑚𝑚) to capture any idiosyncratic and unobserved differences across
municipalities affecting children’s health care and education access.

19
To explore the existence of differential effects by age, we also estimate equation (1)
separately for the following age groups: children 0-5 years old, 6-12 years old, and 13 to 17 years
old when examining health care outcomes; and for the last two groups when assessing educational
outcomes. Within each age group, we also examine if the impact of being born in the United States
varies by the child’s gender and the education of the child’s household head by estimating the
following variation of equation (1):
(2) 𝑌𝑌𝑖𝑖ℎ𝑚𝑚 = 𝛼𝛼 + λ1𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑖𝑖 + λ2𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑏𝑖𝑖 × 𝑐𝑐ℎ𝑏𝑏𝑏𝑏𝑏𝑏𝑐𝑐𝑎𝑎𝑖𝑖 + 𝑋𝑋𝑖𝑖′𝛽𝛽 + 𝑍𝑍ℎ′ 𝛾𝛾 + 𝛿𝛿𝑚𝑚 + 𝜀𝜀𝑖𝑖ℎ𝑚𝑚
where 𝑐𝑐ℎ𝑏𝑏𝑏𝑏𝑏𝑏𝑐𝑐𝑎𝑎𝑖𝑖 stands for either the child’s gender or for whether the household head has less
than 12 years of education, i.e., less than completed high school –both traits are included in 𝑋𝑋𝑖𝑖′.
All other terms in equation (2) remain the same as in equation (1).
For the second part of the analysis, we focus on the sample of U.S.-born children to
examine their assimilation pace in Mexico and potential barriers to their access of essential
services. To evaluate their assimilation, we explore differences in their outcomes based on whether
they and their head of household resided in the United States 5 years earlier, in 2010. Regarding
the potential barriers they face, we pay close attention to the role of having a foreign birth
certificate and no birth certificate at all on the child’s access to health care and education services,
based on previous reports underscoring documentation barriers. In addition, we explore the joint
role played by these two aspects (time in Mexico and documentation) to identify access barriers
among recent vs. earlier arrivals. In this part, our model is given by:
(3) 𝑌𝑌𝑖𝑖ℎ𝑚𝑚 = 𝛼𝛼 + λ1𝑓𝑓𝑏𝑏𝑏𝑏𝑓𝑓𝑓𝑓𝑓𝑓𝑏𝑏𝑏𝑏𝑐𝑐𝑖𝑖 + λ2𝑏𝑏𝑏𝑏𝑏𝑏𝑐𝑐𝑖𝑖 + λ3𝑓𝑓𝑏𝑏𝑏𝑏𝑓𝑓𝑓𝑓𝑓𝑓𝑏𝑏𝑏𝑏𝑐𝑐𝑖𝑖 × 𝑏𝑏𝑓𝑓𝑐𝑐𝑓𝑓𝑏𝑏𝑎𝑎𝑏𝑏𝑏𝑏𝑏𝑏𝑓𝑓𝑟𝑟𝑏𝑏𝑟𝑟ℎ
+λ4𝑏𝑏𝑏𝑏𝑏𝑏𝑐𝑐𝑖𝑖 × 𝑏𝑏𝑓𝑓𝑐𝑐𝑓𝑓𝑏𝑏𝑎𝑎𝑏𝑏𝑏𝑏𝑏𝑏𝑓𝑓𝑟𝑟𝑏𝑏𝑟𝑟ℎ + 𝑋𝑋𝑖𝑖′𝛽𝛽 + 𝑍𝑍ℎ′ 𝛾𝛾 + 𝛿𝛿𝑚𝑚 + 𝜀𝜀𝑖𝑖ℎ𝑚𝑚
where 𝑓𝑓𝑏𝑏𝑏𝑏𝑓𝑓𝑓𝑓𝑓𝑓𝑏𝑏𝑏𝑏𝑐𝑐𝑖𝑖 and 𝑏𝑏𝑏𝑏𝑏𝑏𝑐𝑐𝑖𝑖 are indicators for whether the child has a foreign birth certificate or
none at all, respectively. The reference category is U.S. born children who have a Mexican birth

20
certificate.15 In this specification, we also include the interaction of these variables with
𝑏𝑏𝑓𝑓𝑐𝑐𝑓𝑓𝑏𝑏𝑎𝑎𝑏𝑏𝑏𝑏𝑏𝑏𝑓𝑓𝑟𝑟𝑏𝑏𝑟𝑟ℎ - a dummy indicative of whether the child’s household head was living in the
United States in 2010 and arrived to Mexico between 2010 and 2015. In that case, the reference
category are household heads who were already living in Mexico in 2010. This dummy for recent
arrival is included by itself in 𝑍𝑍ℎ′ . All other terms in equation (3), including the dependent
variables, are the same ones described earlier, except for the vector 𝑋𝑋𝑖𝑖′ which also includes a
dummy for whether the child was living in the United States in 2010.
As in the first part of our analysis, we also look at heterogeneous impacts by age, estimating
equation (3) separately for each of the same age groups defined earlier, and including interactions
of gender and education of the household head with our key regressors (the birth certificate, recent
arrival variables, and their interactions).
Finally, to shed some light on the collateral damage of restricted access to education on
these invisible children settling down in Mexico with their returning parents, we also look at the
incidence of child labor outside and inside the home. To that end, we estimate equation (3) using
a sample of U.S.-born children ages 12 to 17, for which the EIC reports work variables, and allow
the impacts to differ by the child’s gender and the education of the household head, as before. The
dependent variables are, alternatively, a dummy for whether the child works for pay and another
one for whether she works on household chores.
All estimations are performed by ordinary least squares (OLS), clustering standard errors
at the municipality level. For the sake of brevity, in the next section, we report only the
specifications for which we found significant differences by gender and education of the household
head and comment briefly on the omitted ones.
15 Recall that U.S. born children who have at least one Mexican parent qualify for binational status, so they can be registered in Mexico and obtain a Mexican birth certificate.

21
6. Access to Health Care and Education of the “Invisible Ones”
A) Some Descriptive Evidence
Tables A, B and C in the appendix present descriptive statistics for our dependent and
independent variables. Table A shows basic descriptive statistics for the complete sample of
children, as well as by their place of birth (Mexico or the United States) and shows that about 85%
of children born in Mexico are affiliated with a health care provider, compared to only 56% of
U.S. born children. In addition, children born in Mexico are more likely to be affiliated with a
public health care provider (83%) than children born in the United States (43%), who are instead
more likely to be affiliated with a private provider (7% versus 2% for Mexican children). However,
about 97-99% of all children receive health care when they get sick, with differences in the type
of health care provider by place of birth resembling those for affiliation. In contrast, U.S.-born
children have better mean schooling outcomes than their Mexican-born counterparts. About 81%
of the former attend school, compared to 71% of the latter. Compared to Mexican-born children,
U.S.-born children are also more likely to be at an age-appropriate grade and have fewer years of
lag in school. They also are less likely to work for pay or at home than children born in Mexico.
Table A shows that 99% of Mexican-born children have a Mexican birth certificate,
compared with only 47% of U.S.-born children. About 45% of the latter have a foreign birth
certificate, and 7% report having none. About 73% of children born in Mexico lived in Mexico in
2010, compared to 66% of U.S. born children, and 14% of the latter group were still living in the
U.S. in 2010. Finally, a larger proportion of U.S.-born children lives in a household in the highest
two wealth quartiles (49%), compared to their counterparts born in Mexico (38%). The percentage
of both groups who lives in a rural locality, with fewer than 2,500 inhabitants, is very similar (23-
26%).

22
Table B in the in the appendix focuses only on the sample of U.S.-born children and
presents descriptive statistics by whether the head of their household arrived more recently to
Mexico (between 2010 and 2015) or earlier than 2010. Both groups seem to have similar mean
outcomes for health care and education access, except for the likelihood of being affiliated with a
health care provider, which is lower for recent arrivals (52%), compared to earlier ones (59%).
More recent arrivals also have a lower likelihood of being affiliated and receiving health care at a
public contributory institution (12%) than earlier arrivals (21%), which suggests that employment
opportunities improve with the household head’s residence time in Mexico. Children in both
groups are distributed similarly across wealth quartiles. Finally, more recent arrivals are slightly
more likely to live in a rural locality (31%) compared to children whose household head has been
living longer in Mexico (24%).
Table C focuses again on U.S. born children only and presents descriptive statistics for
three subgroups among them: (i) those who have a Mexican birth certificate, (ii) those who have a
foreign birth certificate, and (iii) those who report not having any kind birth certificate. In general,
the differences in the health care and education access between the first group and the other two
are drastic, whereas the differences between having a foreign birth certificate and having none are
small. For instance, 77% of U.S.-born children who hold a Mexican birth certificate are affiliated
to a health care provider, compared to 38% and 34% of children who hold a foreign birth certificate
or none at all, respectively. Children who hold a Mexican birth certificate are also more likely to
be affiliated with a public health care institution (72%) than those in the latter two groups (26-
27%). Once again, the patterns for health care use follow those for affiliation.
In Table C, the mean differences in the schooling outcomes between these three groups are
much smaller, but they also indicate that having a Mexican birth certificate is an advantage for

23
U.S.-born children. Children who have one are a bit more likely to attend school, to be at an age-
appropriate grade, and lag less in school, compared to children who have a foreign birth certificate,
or none. Moving down on Table B, we see that these three groups of children are remarkably
similar in all sociodemographic characteristics, including the probability that they or their
household heads were living in the U.S. or Mexico in 2010, their distribution across wealth
quartiles, and all other individual and household characteristics. Yet, due to the lack of Mexican
documents, they differ starkly in their access to basic services. In the next subsection, we explore
the patterns in Tables A, B and C more thoroughly using regression-based analysis.
B) Health Care and Educational Access by Place of Birth
Are U.S. born children returning to Mexico at a disadvantage accessing health care?
Table 1 shows that U.S.-born children are 28% less likely to be affiliated to a health care provider
than their Mexican counterparts. This gap is larger (38%) among the youngest children, those who
are 0 to 5 years old. Health care coverage is furthered reduced among U.S.-born children in
households headed by individuals with less than a high school education, who are 10% less likely
to be affiliated to a health care provider than their U.S.-born counterparts with a more educated
household head.
Table 1 also shows that, despite lacking health insurance coverage, most children get care
when sick. For instance, even though U.S.-born children are 28% less likely than their Mexican
counterparts to have health insurance, they are only 1% less likely to get the care they need when
sick –a differential propensity that is inversely related to children’s ages, i.e. older children are
more likely to lack appropriate care when sick than younger children, and concentrated among
U.S.-born children with less educated household heads. We do not find significant differences in
the impact of being born in the U.S. by gender; therefore, we omit these results for brevity.

24
Tables 2 and 3 further break down the estimates in Table 1 by type of health care provider,
reflecting inequities in children’s access to care based on their place of birth and the educational
attainment of their household head. We do not present separate estimations based on the child’s
age, because the pattern is similar for all age groups, and we also find no significant heterogeneity
by gender. For instance, based on the results in Table 2, U.S.-born children are 9% and 5% less
likely than their Mexican counterparts to be affiliated to a contributory and non-contributory public
health care provider, respectively. Instead, these U.S.-born children are 1.2 to 2 times more likely
than Mexican-born children to be affiliated to a private or other kind of health care provider. There
are also considerable differences in the type of health insurance coverage enjoyed by children
based on their household head’s education. For example, U.S.-born children with less educated
household heads are 5% less likely to be affiliated to a contributory public health care provider
than Mexican-born children, whereas the corresponding gap for those with more educated
household heads is 20%. In contrast, U.S. born children are 43% more likely to have private health
insurance than Mexican-born children if their household head has less than high school, compared
to more than 3 times if their household head is more educated. In sum, U.S.-born children are
more likely be affiliated to a private health care provider than Mexican-born children, and this
affiliation pattern is even more prevalent if their household’s heads are more educated.
Not surprisingly, following their patterns for affiliation, U.S.-born children are between 21
and 25% less likely to receive care by a public health care provider when sick than Mexican-born
children. This likelihood is lower for U.S.-born children with more educated parents when the
care is provided by public health institutions part of the contributory system. Where do U.S.-born
children receive the care they need when sick? U.S.-born children are 75% to close to 1.7 times

25
more likely than Mexican-born children to receive care in a private health care provider or another
type of institution, respectively.
Are the inequities in health care access by place of birth also manifested in the access to
schooling? The answer is not necessarily. Table 4 displays differences in school attendance, age-
appropriate schooling, and educational lags among younger and older children based on their place
of birth, gender, and household head’s educational attainment. Perhaps the most notable finding
is the lack of differences by place of birth for young children between the ages of 6 and 12. It is
among older children, ages 13 to 17, that we find some differences between those born in the
United States and those born in Mexico by gender. Indeed, U.S.-born males are 5% more likely
than their Mexican-born counterparts to attend school or be at an age-appropriate school level.
Their educational lag is, in turn, 17% lower. U.S.-born females also have an educational advantage
relative to females born in Mexico at these older ages, but it is smaller than that of men. They are
2 to 2.4% more likely to attend school and to be in age-appropriate schooling than their Mexican-
born counterparts, respectively, and their education lag is 6% lower.
Finally, educational gaps between U.S. and Mexico born older youth are highly conditional
on the educational attainment of the household head. Interestingly, due to their comparison group,
it is youth with less educated household heads that do comparatively better. Specifically, U.S.-
born children with less educated household heads are 5% more likely than their Mexican
counterparts to attend school or be at an age-appropriate school level, with a 19% smaller
educational lag, whereas this lag is only 10% smaller when the parents are more skilled.
C) Understanding Barriers to Health Care and Education Access of U.S.-Born Children
The estimates in Table 1 underscore the restricted access to proper health care coverage
endured by U.S.-born children, when compared to their counterparts born in Mexico. In Table 5,

26
we dig a big deeper into the factors driving their lower coverage. Is it their recent arrival to the
country? Or does it have to do with documentation barriers? Based on the results in column (1),
the major impediment seems to be the latter. U.S.-born children with a foreign or no birth
certificate are 62% and 67% less likely to be affiliated to a health care provider than similar
children with a Mexican birth certificate, respectively. In contrast, if the child arrived recently –
within the past 5 years, their propensity to have health care coverage is about 12% lower. Thus,
being a recent arrival to Mexico, by itself, has a lower impact on the child’s health care coverage
than lack of proper documentation. In fact, U.S. born children with household heads who recently
arrived in the country are 10% more likely to be affiliated to a health care provider than their
counterparts whose household heads arrived earlier on. The interactions between our proxy for
residence time in Mexico and the birth certificate dummies show that the negative effect of not
having a Mexican birth certificate is about 10-12 percentage points larger for children whose
household head arrived more recently to Mexico, compared to those who arrived before 2010.
However, the larger negative effect of the birth certificate dummies alone suggests that
documentation barriers for children whose household head arrived before 2010 are persistent. This
might also explain why, when assessing if the child received proper care when sick, it is the lack
of a Mexican birth certificate that seems to play a role, even if small, in lowering their propensity
to get that care by 1.3% when they have a foreign birth certificate and by 3% if they lack one.
Note that for the results in Table 5, and also for those in Tables 6 and 7, we focus on the whole
sample of U.S.-born children since there are no significant differences by age.
An examination of the estimates in Tables 6 and 7 sheds further light on these results. Table
6 shows that the lack of a Mexican birth certificate, which plays a crucial role in lowering the
child’s propensity to be affiliated at all, mostly reduces affiliation to a public health care provider.

27
In contrast, U.S.-born children with a foreign birth certificate are 66% and 1.6 times more likely
than those with a Mexican birth certificate to have a private or other type of health care provider,
respectively. In a similar vein, U.S.-born children lacking any birth certificate are 26% less likely
to be affiliated to a public, non-contributory health care provider than their U.S.-born counterparts
with a Mexican birth certificate, but 76% and 1.2 times more likely to have a private or other type
of health care provider, correspondingly. Finally, the recent arrival of the household head plays a
key role. U.S.-born children with household heads who arrived within the last 5 years are between
12.5% and 25.3% less likely to be affiliated to a public-contributory, private or other type of health
care provider, but 14.5% more prone to have public, non-contributory health coverage, than U.S.-
born children with households who arrived further in the past. This probably reflects an increased
effort of the Mexican government to provide support and information about basic services to more
recent arrivals, compared to previous ones. For instance, starting in 2012, the government
established several health care booths at the main points of entry to Mexico, precisely to provide
basic care to returning and deported migrants and to affiliate them to SP.16 Overall, U.S.-born
children with a foreign birth certificate and whose household heads arrived within the past 5 years
are about 1.12 times more likely to have health care coverage through a private provider than other
U.S.-born children –a propensity equaling 24.5% among those lacking a birth certificate.
We next conduct a similar analysis to better understand the barriers to receiving proper care
encountered by U.S.-born children at various health care providers. Based on the estimates in
16 These booths, called “Health Care Booths for Repatriated Migrants” (Módulos de Atención a la Salud del Migrante Repatriado, in Spanish) are located in Tijuana, Matamoros, Nuevo Laredo, Reynosa and Nogales. For the most recent information about them, please refer to: https://saludfronterizamx.org/modulo-salud-migrante/index.php. From January 2013 to June 2017, these booths provided care and support to about 23,000 migrants (please refer to “Quinto Informe de Gobierno, 2016-2017”, Presidencia de la República).

28
Table 7, the impacts of not having a Mexican birth certificate and the residence time in Mexico on
the type of health used when sick follow a similar pattern than those for affiliation just discussed.
In sum, the estimates in Tables 5 through 7 suggest that the lack of documentation, along
with institutional factors –such as accessibility to health care based on the type of employment and
program availability, are significant hurdles to the health care coverage and care receipt of U.S.-
born children returning to Mexico with their families. Do they play a similar role in the
educational context?
The estimates in Table 8 address this question. The fact that educational gaps by place of
birth were not prominent among young children suggests that the barriers noted above are not as
relevant in the educational context. Indeed, among U.S.-born children ages 6 to 12, it is apparent
that having a foreign birth certificate is not a considerable barrier to school attendance, even though
it is associated to a 40% greater educational lag. These results could reflect the gradual easing of
enrollment requirements over time for these children, who might have not been able to enroll
immediately due to their lack of a Mexican birth certificate, but could do so later on and so they
lagged behind. Also, the recent arrival of the child and that of the household head, combined with
the lack of birth certificate appear be more relevant in explaining the educational attainment of
these young kids. For instance, U.S.-born children lacking any birth certificate and whose
household heads arrived in the country within the last 5 years are 5% less likely than similar
children to have an age-appropriate schooling level. In addition, their educational lag in years is
about 4% greater. Overall, the combined impact of these variables suggests that other elements,
like information or knowledge about the school system, language or other assimilation barriers
might be at play.

29
In the case of older youth, having a foreign birth certificate or lacking one altogether make
them considerably less likely to attend school or be at an age-appropriate school level. For
example, U.S.-born youth lacking a birth certificate are 12% less likely to attend school compared
to their counterparts who have a Mexican birth certificate. In addition to the lack of proper
documentation, recently arrived youth are 7.5% less likely to attend school, when compared to
earlier arrivals. Yet, U.S.-born youth whose household heads arrived within the past 5 years are
4.4% more likely to be attending school than those whose household heads arrived earlier than
2010.
Finally, we might reasonably ask what these older youth do if they become less likely to
attend school. Are they pushed into the labor market or home labor? The estimates in column (1)
in Table 9 show that U.S.-born males and females with a foreign birth certificate are 65% and 25%
more likely to work for pay than their counterparts with a Mexican birth certificate, respectively.
In a similar vein, U.S.-born youth lacking a birth certificate are 57% more likely to work for pay
than their counterparts with a Mexican birth certificate, regardless of gender.
Column (2) in Table 9 shows that having a foreign birth certificate or none at all increases
the likelihood of working a home only for female youth between 69% and 1.9 times, compared to
other U.S. born youth. Similarly, working at home is twice as prevalent among U.S.-born youth
who were living in the United States 5 years earlier, but 53% less likely among those whose
household heads recently came back to Mexico.
In sum, the results in Tables 8 and 9 confirm that the lack of proper documentation keeps
these “invisible children” out of school and pushes them into other activities, like working for pay
or at home.

30
7. Summary and Policy Implications
Over the past two decades, the United States has experienced an unprecedented increase in
immigration enforcement, resulting in large numbers of deportees (Nowrasteh, 2019). Many of
them were long-term Mexican migrants who had settled in the United States and formed families.
Suddenly, they found themselves back in Mexico with their children, who had been born and raised
in the United States. In this paper, we examine the health care and education barriers encountered
by these children –a group also referred to as “Los Invisibles” or the “Invisible Ones” in the
literature, and whose number is estimated to be close to half a million in 2018 (Cruz, 2018; Shaw,
2016).
Using data from the 2015 Mexican EIC, we document that these children are 28% less
likely than their Mexican counterparts to be affiliated with any health care provider. Among
children who are affiliated, U.S. born children are also less likely to be affiliated with, and receive
health care from, a public health care provider and more likely to have a private or other kind of
health care provider. We also find that lack of proper documentation is a significant and persistent
barrier that could explain these gaps in health care access. Notably, we find that in 2015 it was
still a significant barrier among U.S.-born children whose household head arrived before 2010 to
Mexico. Regarding education, on average we find no significant gaps in the outcomes of primary-
school children (ages 6 and 12) by place of birth and positive gaps for U.S.-born teenagers (ages
13 to 17), compared to their Mexican-born counterparts. However, when we focus on U.S. born
children only, our results show that the lack of proper documentation is causing some of them to
be left behind.
In sum, we find that U.S.-born children are at a considerable disadvantage in terms of health
care access, but less so in terms of education access, compared to their Mexican-born counterparts.

31
A couple of factors could explain these mixed findings. First, as discussed in the background
section, the education system in Mexico is much more centralized, particularly at the basic
educational levels, compared to the health care system. Such centralization favors prompter and
more uniform responses to the policy challenges posed by the recent influx of transnational
children. Second, the education barriers face by these invisible children have received much more
attention in the academic literature, probably contributing to a higher awareness among
policymakers, whereas the empirical evidence on their health care access has been scarce. Thus,
we contribute to the academic and policy discussion about the assimilation of these transnational
children by providing comprehensive evidence of the substantial gaps that remain in health care
coverage. Such gaps, as well as their found persistence, are worrisome. They can not only expose
transnational children and their families to considerable health risks with long-term consequences,
but also to catastrophic expenses. In addition, by documenting the role played by lack of proper
documentation in accessing these services, we are able to underscore the relevance of easing
documentation requirements as a key policy in facilitating these children’s access to health care.
Given the lack of significant gaps in school access at lower school levels, the Mexican government
could rely on school authorities to reach out to transnational children and their families, providing
them with direct support to get their Mexican identification documents (birth certificate and
CURP) and with assistance to sign up for publicly provided health care coverage. In fact, some
health care coverage, free of charge, already exists for students at the high school, college, and
graduate levels in Mexico.
Regarding education, our results suggest that the active easing of barriers implemented by
the Mexican government through SEP have favored the education access of transnational children.
However, such efforts should continue to be promoted and enforced, as some transnational youth

32
are still being left out of school due to lack of proper documents. In addition, the literature
highlights the challenges and hardships that “invisible children” face once they can attend a
Mexican school, such as language barriers, among others. Hence, the focus should be on
improving the quality of their educational experience, to ensure that these children progress
adequately, and to prevent them from getting discouraged and dropping out, particularly as they
transition to high school and college.
On the United States side, changing immigration enforcement from a communitywide to a
more targeted approach that gives priority to children and provides a path for their families to stay
together in the country could also benefit these children considerably, sparing them the trauma of
leaving their country and try to find their way in an almost completely new environment.
Transnational children are citizens of both Mexico and the United States. Given the well-
documented long-term impacts of adequate health care and educational investments early in life
on later life outcomes (e.g. Becker and Chiswick, 1966; Clark and Royer, 2013; Hoynes,
Schanzenbach, and Almond, 2016), both countries should be invested in facilitating their access
to such services. After all, as adults, these children might choose to go back to the United States
or to stay in Mexico. Limited access to basic services could seriously hamper their development
and growth, breaking the cycle of intergenerational progress that probably motivated their parents
to migrate in the first place.

33
References
Águila E., Fonseca R., Vega A. 2015. Self-Employment, Health Insurance, and Return Migration of Middle-Aged and Elderly Mexican Males. In: Vega W., Markides K., Angel J., Torres-Gil F. (eds) Challenges of Latino Aging in the Americas. Springer, Cham Amuedo-Dorantes, Catalina, and Francisca Antman. 2017. “Schooling and Labor Market Effects of Temporary Authorization: Evidence from DACA,” Journal of Population Economics, 30 (1): 339-373.
Amuedo-Dorantes, Catalina, and Mary Lopez. 2017. “The Hidden Educational Costs of Intensified Immigration Enforcement,” Southern Economic Journal, 84 (1): 120-154.
Amuedo-Dorantes, Catalina and Chad Sparber. 2014. “In-State Tuition for Undocumented Immigrants and its Impact on College Enrollment, Tuition Costs, Student Financial Aid, and Indebtedness,” Regional Science and Urban Economics, 49: 11-24.
Becker, Gary S. and Barry R. Chiswick. 1966. “Education and the Distribution of Earnings” American Economic Review 56: 358-369.
Cave, Damien. 2012. “American Children, Now Struggling to Adjust to Life in Mexico,” The New York Times, June 18. Available at: http:// www.nytimes.com/2012/06/19/world/ americas/american-born-childrenstruggle-to-adjust-in-mexico.html.
Chishti, Muzaffar, Sarah Pierce, and Jessica Bolter. 2017. “The Obama Record on Deportations: Deporter in Chief or Not?” Migration Policy Institute: Washington DC. Available at www.migrationpolicy.org.
Clark, Damon and Heather Royer. 2013. “The Effect of Education on Adult Mortality and Health: Evidence from Britain” American Economic Review, 103: 2087-2120.
Cruz, Pamela. 2018. “A Vulnerable Population: U.S. Citizen Minors Living in Mexico,” Policy Brief, Baker Institute for Public Policy, Rice University. Available online at: https://www.bakerinstitute.org/media/files/research-document/3869bc0a/bi-brief-031918-mex-citizenminors.pdf
Donato, Katherine M. and Duncan, E. M. 2011. “Migration, Social Networks, and Child Health in Mexican Families.” Journal of Marriage and Family, 73: 713-728. DOI:10.1111/j.1741-3737.2011.00841.x
Emif Norte. 2015. “Encuestas Sobre Migración En Las Fronteras Norte Y Sur de México.” [A Study of Migration Along the North and South Borders of Mexico.] COLEF. Available at: http://www.colef.mx/emif/index.php.
Gonzalez-Barrera, A., and Mnauel Krogstad J. 2019. “The Number of U.S. Born Babies with Unauthorized Immigrant Parents Has Fallen Since 2017.” Pew Research Center: Washington DC. Available at: www.pewresearch.org.

34
Gonzalez-Barrera, Ana. 2015. “More Mexicans Leaving Than Coming to the U.S.,” Pew Research Center, November. At: http://www.pewhispanic.org/2015/11/19/more-mexicans-leaving-than-coming-tothe-u-s/.
Hagan, J, Eschbach K, Rodriguez N. 2008. “U.S. Deportation Policy, Family Separation, and Circular Migration” International Migration Review, 42: 64-88.
Hoynes, Hilary, Diane Whitmore Schanzenbach, and Douglas Almond. 2016. “Long-Run Impacts of Childhood Access to the Safety Net.” American Economic Review, 106 (4): 903-34.
Hwang, Kristen. 2017. “As American kids pour across the border, Mexican schools struggle to keep up,” USA Today, September 5. At: https://www.usatoday.com/story/news/nation-ow/2017/09/05/americankids-pour-across-border-mexicanschools-struggle-keep-up/629458001/.
Instituto Nacional de Estadística Geografía e Informática (INEGI). 2010. “Poblacion, Nacional de Estadistica Y Geografia. [National Institute of Statistics and Geography]” Available at: http://www.inegi.org.mx/Sistemas/temasV2/Default.aspx?s=est&c=17484.
Koohi, Shiva. 2017. “College Prospects and Risky Behavior among Mexican Immigrant Youth: The Effects of In-State Tuition Policies on Schooling and Childbearing,” Economics of Education Review, June (58): 162-74.
Lakhani, Nina. 2015. “U.S.-born students in Mexico risk becoming ‘lost generation’”, Los Angeles Times, March 9. Available online at: https://www.latimes.com/world/mexico-americas/la-fg-mexico-schools-americans-20150309-story.html
Martinez-Donate, Ana P., Ifna Ejebe, Xiao Zhang, Sylvia Guendelman, Félice Lê-Scherban, Gudelia Rangel, Eduardo Gonzalez-Fagoaga, Melbourne F. Hovell, and Catalina Amuedo-Dorantes. 2017. “Access to Health Care Among Mexican Migrants and Immigrants: A Comparison Across Migration Phases”, Journal of Health Care for the Poor and Underserved 28(4): 1314–1326.
Masferrer, C. Sánchez, L. y Rodríguez. R. 2017. “Condiciones laborales de los migrantes de retorno de Estados Unidos”, Apuntes para la Equidad, No. 2, May. El Colegio de México.
Medina, Dulce and Cecilia Menjívar. 2015. “The context of return migration: challenges of mixed-status families in Mexico’s schools,” Ethnic and Racial Studies, 38:12, 2123-2139.
Nowrasteh, Alex. 2019. “Deportation rates in historical perspective” Cato at Liberty. Available at: https://www.cato.org/blog/deportation-rates-historical-perspective [Accessed on 11/21/2020]
Panait Catalina and Victor Zúñiga. 2016. “Children circulating between the U.S. and Mexico: fractured schooling and linguistic ruptures” Mexican Studies, 32: 226–51.
Passel Jeffrey S., and D’Vera Cohn. 2018. “U.S. Unauthorized Immigrant Population, 2017”. Pew Research Center: Washington DC. Available online at www.pewresearch.org
35
Rohal, Molly and Mark Hugo Lopez. 2014. “The Rise of Federal Immigration Crimes: Unlawful Reentry Drives Growth,” Pew Research Center: Washington DC. Available at www.pewresearch.org
Román González, Betsabé and Víctor Zúñiga. 2014. “Children Returning from the U.S. to Mexico: School Sweet School?” Migraciones Internacionales, 7(4): 277–86, http://www. scielo.org.mx/scielo.php?script=sci_art text&pid=S1665-89062014000200010
Sanchez, Claudio. 2016. “‘Invisible’ Children: Raised in The U.S., Now Struggling In Mexico,” NPR, November 13 at http://www.npr.org/sections/ ed/2016/11/13/498271392/invisiblechildren-raised-in-the-u-s-nowstruggling-in-mexico.
Sánchez García, Juan and Víctor Zúñiga. 2010. “Trayectorias de los alumnos transnacionales en México. Propuesta intercultural de atención educativa.” Trayectorias, 12(30), 5-23. Available online at: http://www.redalyc.org/articulo.oa?id=60713488002
Shaw, Amelia. 2016. “An Invisible Tide: Undocumented U.S. Kids in Mexico,” The Foreign Service Journal, 93(8): 48–52, http://www.afsa.org/ invisible-tide-undocumented-us-kidsmexico; Secretaría de Gobernación, “Miguel Ángel Osorio Chong.”
Stephens, Robert W. 2012. “Antiterrorism and Effective Death Penalty Act of 1996 (U.S.)” in Loue, Sana; Sajatovic, Martha (eds.), Encyclopedia of Immigrant Health, Springer, pp. 207-208.
Wassink, Joshua T. 2020. “Out of Sight and Uninsured: Access to Healthcare Among US-Born Minors in Mexico.” Journal of Immigrant Minority Health 22: 448–455.
Watson, Tara. 2014. “Inside the Refrigerator: Immigration Enforcement and Chilling Effects in Medicaid Participation“, American Economic Journal: Economic Policy, 6 (3): 313-38.
Zúñiga, Víctor, and Edmund T. Hamann. 2015. “Going to a home you have never been to: the return migration of Mexican and American-Mexican children,” Children’s Geographies 13(6): 644.
Zúñiga, Víctor and Edmund T. Hamann. 2013. “Understanding American Mexican Children.” Faculty Publications: Department of Teaching, Learning and Teacher Education, University of Nebraska. 359. Available online at: https://digitalcommons.unl.edu/teachlearnfacpub/359

36
Table 1: Health Care Access
Outcome: Child is Affiliated to a Health Care Provider Child Got Care When Last Sick Sample: All 0-5 6-12 13-17 All All 0-5 6-12 13-17 All Column: (1) (2) (3) (4) (5) (6) (7) (8) (9) (10)
Child born in USA -0.237*** -0.318*** -0.224*** -0.196*** -0.172*** -0.009*** -0.005* -0.008*** -0.011*** 0.000 (0.008) (0.011) (0.009) (0.012) (0.008) (0.001) (0.003) (0.001) (0.003) (0.003) Child born in USA* Head has less than H.S.
-0.086*** -0.013*** (0.009) (0.003)
Observations 7,656,973 2,475,719 3,048,668 2,132,586 7,656,973 7,692,263 2,505,471 3,051,881 2,134,911 7,692,263 R-squared 0.029 0.027 0.033 0.032 0.029 0.013 0.042 0.004 0.005 0.013 DV Mean 0.847 0.838 0.858 0.841 0.847 0.988 0.981 0.993 0.989 0.988
Notes: All models include a constant term, as well as controls for: (1) children’s gender, age, indigenous origin, living arrangements (whether they live with their mother, father, both or none), birth certificate ownership (Mexican, foreign or no birth certificate), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior), and (2) household and household head traits, including: household size and composition (number of children of 0-5, 6-12, 13-17 in the household, as well as dummy variables for whether all children were born in Mexico, the United States or in both countries), household wealth (dummies indicative of the household’s position in a particular wealth quintile) and location (rural or urban), as well as information on the household head’s gender, age, indigenous origin, educational attainment, place of birth (Mexico, U.S. or elsewhere), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior). All models also include municipality fixed effects, and standard errors are clustered at the municipality level. *p<0.1, **p<0.05, ***p<0.01.

37
Table 2: Health Care Access by Type of Affiliation
Outcome: At Public Health Care Provider - contributory
At Public Health Care Provider – non-contributory
At Private Health Care Provider
At Other Kind of Health Care Provider
Column: (1) (2) (3) (4) (5) (6) (7) (8)
Child born in USA -0.035*** -0.078*** -0.028*** -0.035*** 0.032*** 0.083*** 0.026*** 0.031*** (0.007) (0.013) (0.007) (0.008) (0.005) (0.007) (0.007) (0.010) Child born in USA* Head has less than H.S.
0.058*** 0.011 -0.072*** -0.007 (0.013) (0.010) (0.007) (0.007)
Observations 6,599,982 6,599,982 6,599,982 6,599,982 6,599,982 6,599,982 6,599,982 6,599,982 R-squared 0.256 0.260 0.306 0.311 0.041 0.042 0.008 0.008 DV Mean 0.401 0.401 0.582 0.582 0.0257 0.0257 0.0137 0.0137
Notes: All models include a constant term, as well as controls for: (1) children’s gender, age, indigenous origin, living arrangements (whether they live with their mother, father, both or none), birth certificate ownership (Mexican, foreign or no birth certificate), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior), and (2) household and household head traits, including: household size and composition (number of children of 0-5, 6-12, 13-17 in the household, as well as dummy variables for whether all children were born in Mexico, the United States or in both countries), household wealth (dummies indicative of the household’s position in a particular wealth quintile) and location (rural or urban), as well as information on the household head’s gender, age, indigenous origin, educational attainment, place of birth (Mexico, U.S. or elsewhere), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior). All models also include municipality fixed effects, and standard errors are clustered at the municipality level. *p<0.1, **p<0.05, ***p<0.01.

38
Table 3: Health Care Access When Last Sick
Outcome: At Public Health Care Provider - contributory
At Public Health Care Provider – non-contributory
At Private Health Care Provider
At Other Kind of Health Care Provider
Column: (1) (2) (3) (4) (5) (6) (7) (8)
Child born in USA -0.080*** -0.147*** -0.098*** -0.039*** 0.156*** 0.162*** 0.023*** 0.024*** (0.008) (0.011) (0.005) (0.006) (0.008) (0.010) (0.005) (0.006) Child born in USA* Head has less than HS
0.088*** -0.079*** -0.008 -0.001 (0.009) (0.008) (0.010) (0.005)
Observations 7,593,453 7,593,453 7,593,453 7,593,453 7,593,453 7,593,453 7,593,453 7,593,453 R-squared 0.128 0.130 0.214 0.217 0.046 0.047 0.017 0.017 DV Mean 0.321 0.321 0.459 0.459 0.207 0.207 0.0134 0.0134
Notes: All models include a constant term, as well as controls for: (1) children’s gender, age, indigenous origin, living arrangements (whether they live with their mother, father, both or none), birth certificate ownership (Mexican, foreign or no birth certificate), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior), and (2) household and household head traits, including: household size and composition (number of children of 0-5, 6-12, 13-17 in the household, as well as dummy variables for whether all children were born in Mexico, the United States or in both countries), household wealth (dummies indicative of the household’s position in a particular wealth quintile) and location (rural or urban), as well as information on the household head’s gender, age, indigenous origin, educational attainment, place of birth (Mexico, U.S. or elsewhere), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior). All models also include municipality fixed effects, and standard errors are clustered at the municipality level. *p<0.1, **p<0.05, ***p<0.01.

39
Table 4: Access to Education
Age Group: Ages 6-12 Ages 13-17
Outcome: Attends School Age-Appropriate
Schooling Educational Lag in
Years Attends School Age-Appropriate
Schooling Educational Lag in
Years Column (1) (2) (3) (4) (5) (6) (7) (8) (9) (10) (11) (12)
Child born in USA 0.002 -0.001 -0.006* -0.005 0.006 0.012 0.040*** 0.000 0.037*** -0.005 -0.078*** 0.047** (0.003) (0.003) (0.004) (0.004) (0.007) (0.008) (0.007) (0.009) (0.011) (0.012) (0.023) (0.022) Child born in USA * Child is Female
-0.001 -0.000 0.002 -0.021*** -0.025*** 0.048** (0.002) (0.002) (0.004) (0.005) (0.008) (0.020)
Child born in USA * Head has less than HS
0.003 -0.002 -0.006 0.038*** 0.039*** -0.132*** (0.003) (0.002) (0.005) (0.006) (0.011) (0.022)
Observations 3,049,087 3,049,087 3,035,895 3,035,895 3,035,895 3,035,895 2,133,481 2,133,481 2,129,039 2,129,039 2,129,039 2,129,039 R-squared 0.012 0.013 0.023 0.024 0.015 0.016 0.119 0.119 0.109 0.109 0.090 0.092 DV Mean 0.978 0.978 0.962 0.962 0.0637 0.0637 0.812 0.812 0.793 0.793 0.451 0.451
Notes: All models include a constant term, as well as controls for: (1) children’s gender, age, indigenous origin, living arrangements (whether they live with their mother, father, both or none), birth certificate ownership (Mexican, foreign or no birth certificate), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior), and (2) household and household head traits, including: household size and composition (number of children of 0-5, 6-12, 13-17 in the household, as well as dummy variables for whether all children were born in Mexico, the United States or in both countries), household wealth (dummies indicative of the household’s position in a particular wealth quintile) and location (rural or urban), as well as information on the household head’s gender, age, indigenous origin, educational attainment, place of birth (Mexico, U.S. or elsewhere), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior). All models also include municipality fixed effects, and standard errors are clustered at the municipality level. *p<0.1, **p<0.05, ***p<0.01.

40
Table 5: Health Care Access of U.S. Born Children
Column: (1) (2) Outcome: Child is Affiliated to a Health Care Provider Child Got Care When Last Sick Child has a foreign birth certificate -0.359*** -0.013*** (0.014) (0.003) Child has no birth certificate -0.388*** -0.028*** (0.020) (0.008) Child was living in USA in 2010 -0.069*** -0.007* (0.012) (0.004) Recently arrived HH head 0.057*** 0.005 (0.014) (0.003)
Child has foreign birth certificate x Recently arrived H.H. head -0.099*** -0.023*** (0.018) (0.007) Child has no birth certificate x Recently arrived H.H. head -0.115*** -0.018 (0.032) (0.012) Observations 84,777 85,090 R-squared 0.188 0.027 DV Mean 0.578 0.978
Notes: All models include a constant term, as well as controls for: (1) children’s gender, age, indigenous origin, living arrangements (whether they live with their mother, father, both or none), birth certificate ownership (Mexican, foreign or no birth certificate), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior), and (2) household and household head traits, including: household size and composition (number of children of 0-5, 6-12, 13-17 in the household, as well as dummy variables for whether all children were born in Mexico, the United States or in both countries), household wealth (dummies indicative of the household’s position in a particular wealth quintile) and location (rural or urban), as well as information on the household head’s gender, age, indigenous origin, educational attainment, place of birth (Mexico, U.S. or elsewhere), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior). All models also include municipality fixed effects, and standard errors are clustered at the municipality level. *p<0.1, **p<0.05, ***p<0.01.

41
Table 6: Health Care Access of U.S. Born Children by Type of Affiliation
Column: (1) (2) (3) (4)
Outcome: At Public Health Care Provider - contributory
At Public Health Care Provider – non-contributory
At Private Health Care Provider
At Other Kind of Health Care Provider
Child has a foreign birth certificate
-0.047** -0.113*** 0.067*** 0.080*** (0.019) (0.010) (0.009) (0.014)
Child has no birth certificate -0.019 -0.135*** 0.077*** 0.063*** (0.031) (0.019) (0.017) (0.013)
Child was living in USA in 2010 -0.041*** 0.015 0.004 0.017**
(0.015) (0.017) (0.009) (0.009) Recently arrived HH head -0.043** 0.076*** -0.020** -0.013** (0.020) (0.025) (0.009) (0.007) Child has foreign birth certificate x Recently arrived HH head
-0.004 -0.026 0.043** -0.011 (0.025) (0.035) (0.021) (0.025)
Child has no birth certificate x Recently arrived HH head
0.066 0.011 -0.056* -0.022 (0.099) (0.089) (0.032) (0.028)
Observations 50,298 50,298 50,298 50,298 R-squared 0.177 0.351 0.145 0.087 DV Mean 0.345 0.525 0.102 0.0514
Notes: All models include a constant term, as well as controls for: (1) children’s gender, age, indigenous origin, living arrangements (whether they live with their mother, father, both or none), birth certificate ownership (Mexican, foreign or no birth certificate), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior), and (2) household and household head traits, including: household size and composition (number of children of 0-5, 6-12, 13-17 in the household, as well as dummy variables for whether all children were born in Mexico, the United States or in both countries), household wealth (dummies indicative of the household’s position in a particular wealth quintile) and location (rural or urban), as well as information on the household head’s gender, age, indigenous origin, educational attainment, place of birth (Mexico, U.S. or elsewhere), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior). All models also include municipality fixed effects, and standard errors are clustered at the municipality level. *p<0.1, **p<0.05, ***p<0.01.
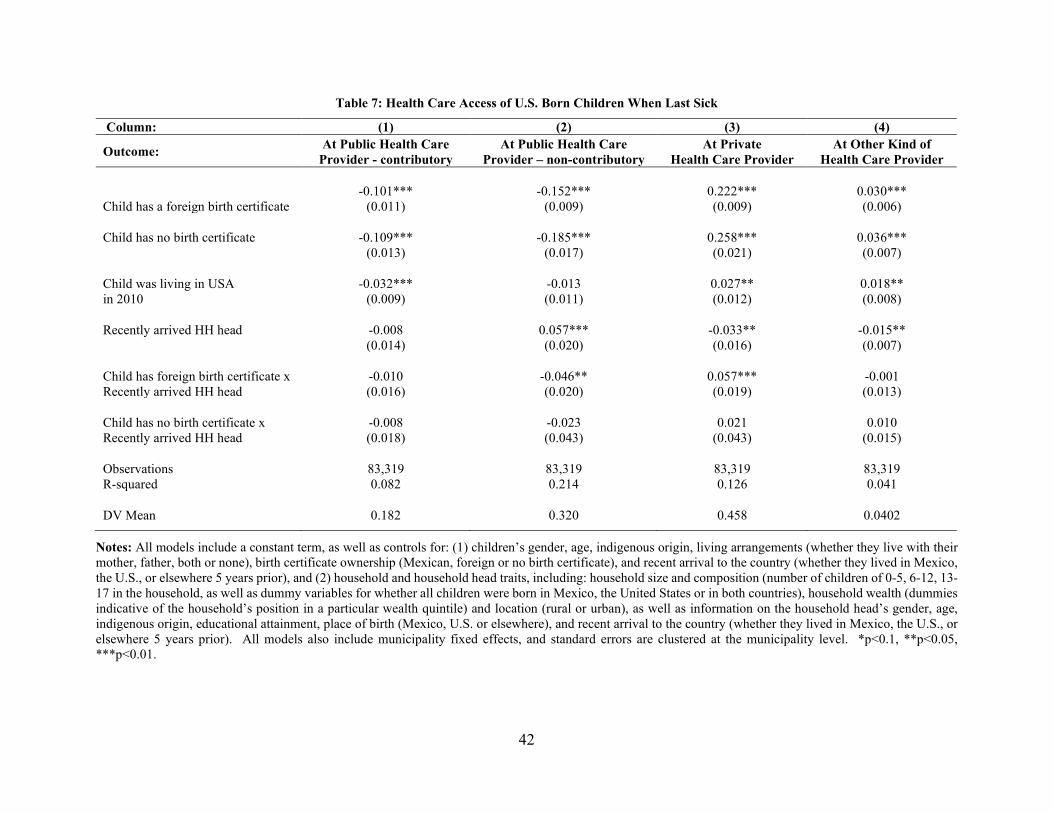
42
Table 7: Health Care Access of U.S. Born Children When Last Sick
Column: (1) (2) (3) (4)
Outcome: At Public Health Care Provider - contributory
At Public Health Care Provider – non-contributory
At Private Health Care Provider
At Other Kind of Health Care Provider
Child has a foreign birth certificate -0.101*** -0.152*** 0.222*** 0.030***
(0.011) (0.009) (0.009) (0.006) Child has no birth certificate -0.109*** -0.185*** 0.258*** 0.036*** (0.013) (0.017) (0.021) (0.007) Child was living in USA in 2010
-0.032*** -0.013 0.027** 0.018** (0.009) (0.011) (0.012) (0.008)
Recently arrived HH head -0.008 0.057*** -0.033** -0.015** (0.014) (0.020) (0.016) (0.007) Child has foreign birth certificate x Recently arrived HH head
-0.010 -0.046** 0.057*** -0.001 (0.016) (0.020) (0.019) (0.013)
Child has no birth certificate x Recently arrived HH head
-0.008 -0.023 0.021 0.010 (0.018) (0.043) (0.043) (0.015)
Observations 83,319 83,319 83,319 83,319 R-squared 0.082 0.214 0.126 0.041 DV Mean 0.182 0.320 0.458 0.0402
Notes: All models include a constant term, as well as controls for: (1) children’s gender, age, indigenous origin, living arrangements (whether they live with their mother, father, both or none), birth certificate ownership (Mexican, foreign or no birth certificate), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior), and (2) household and household head traits, including: household size and composition (number of children of 0-5, 6-12, 13-17 in the household, as well as dummy variables for whether all children were born in Mexico, the United States or in both countries), household wealth (dummies indicative of the household’s position in a particular wealth quintile) and location (rural or urban), as well as information on the household head’s gender, age, indigenous origin, educational attainment, place of birth (Mexico, U.S. or elsewhere), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior). All models also include municipality fixed effects, and standard errors are clustered at the municipality level. *p<0.1, **p<0.05, ***p<0.01.

43
Table 8: Access to Education of U.S. Born Children
Age Group: Ages 6-12 Ages 13-17
Outcome: Attends School
Age-Appropriate Schooling
Educational Lag in Years
Attends School
Age-Appropriate Schooling
Educational Lag in Years
Column: (1) (2) (3) (4) (5) (6)
Child has a foreign birth certificate
-0.008*** -0.013*** 0.019*** -0.079*** -0.056*** 0.115*** (0.003) (0.003) (0.005) (0.008) (0.010) (0.019)
Child has no birth certificate -0.011** -0.005 0.009 -0.102*** -0.100*** 0.205*** (0.005) (0.004) (0.007) (0.021) (0.027) (0.053)
Child was living in USA in 2010
-0.012*** -0.019*** 0.026*** -0.066*** -0.027 0.058 (0.004) (0.005) (0.010) (0.018) (0.017) (0.049)
Recently arrived HH head 0.006 0.009 -0.017* 0.039** -0.001 -0.028 (0.004) (0.006) (0.009) (0.018) (0.020) (0.050) Child has foreign birth certificate x Recently arrived HH head
-0.006 -0.011* 0.008 -0.008 0.003 -0.011 (0.006) (0.006) (0.008) (0.023) (0.022) (0.051)
Child has no birth certificate x Recently arrived HH head
-0.045 -0.044** 0.045* -0.019 0.009 -0.105 (0.033) (0.022) (0.025) (0.058) (0.064) (0.074)
Observations 58,400 58,178 58,178 21,107 21,039 21,039 R-squared 0.023 0.040 0.033 0.191 0.124 0.087 DV Mean 0.981 0.968 0.0479 0.879 0.861 0.248
Notes: All models include a constant term, as well as controls for: (1) children’s gender, age, indigenous origin, living arrangements (whether they live with their mother, father, both or none), birth certificate ownership (Mexican, foreign or no birth certificate), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior), and (2) household and household head traits, including: household size and composition (number of children of 0-5, 6-12, 13-17 in the household, as well as dummy variables for whether all children were born in Mexico, the United States or in both countries), household wealth (dummies indicative of the household’s position in a particular wealth quintile) and location (rural or urban), as well as information on the household head’s gender, age, indigenous origin, educational attainment, place of birth (Mexico, U.S. or elsewhere), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior). All models also include municipality fixed effects, and standard errors are clustered at the municipality level. *p<0.1, **p<0.05, ***p<0.01.

44
Table 9: U.S. Born Children Ages 12-17 Working Outside the Home or at the Home
Column: (1) (2) Outcome: Child Works for Pay Child Works at Home
Child has a foreign birth certificate 0.031*** 0.004 (0.007) (0.003) Child has no birth certificate 0.027** 0.000 (0.013) (0.003) Child was living in USA in 2010 -0.005 0.031*** (0.008) (0.009) Recently arrived HH head 0.012 -0.016** (0.015) (0.008) Recently arrived H.H. head * Child if Female -0.008 -0.003 (0.015) (0.013) Child has foreign birth certificate * Child if Female -0.019** 0.021*** (0.008) (0.007) Child has no birth certificate * Child if Female 0.011 0.057** (0.024) (0.027) Child has foreign birth certificate * Head recent arrival
-0.020 (0.020)
-0.004 (0.006)
Child has foreign birth certificate * Recently arrived H.H. head * Child if Female
0.020 0.003 (0.023) (0.021)
Child has no birth certificate * Recently arrived H.H. head
-0.008 (0.030)
0.013 (0.011)
Child has no birth certificate * Recently arrived H.H. head * Child is Female
0.033 -0.055 (0.058) (0.052)
Observations 28,135 28,135 R-squared 0.078 0.112 DV Mean 0.0474 0.0304
Notes: All models include a constant term, as well as controls for: (1) children’s gender, age, indigenous origin, living arrangements (whether they live with their mother, father, both or none), birth certificate ownership (Mexican, foreign or no birth certificate), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior), and (2) household and household head traits, including: household size and composition (number of children of 0-5, 6-12, 13-17 in the household, as well as dummy variables for whether all children were born in Mexico, the United States or in both countries), household wealth (dummies indicative of the household’s position in a particular wealth quintile) and location (rural or urban), as well as information on the household head’s gender, age, indigenous origin, educational attainment, place of birth (Mexico, U.S. or elsewhere), and recent arrival to the country (whether they lived in Mexico, the U.S., or elsewhere 5 years prior). All models also include municipality fixed effects, and standard errors are clustered at the municipality level. *p<0.1, **p<0.05, ***p<0.01.

45
APPENDIX TABLES - Table A: Descriptive Statistics for All Children
Variable Name All Children Children Born in Mexico Children Born in the U.S. Outcomes: Child affiliated to health provider 0.85 0.361 8022690 0.85 0.357 7914566 0.56 0.497 108124 Public/contributory 0.34 0.474 8022690 0.34 0.474 7914566 0.2 0.4 108124 Public/non-contributory 0.49 0.5 8022690 0.49 0.5 7914566 0.26 0.441 108124 Private 0.02 0.147 8022690 0.02 0.145 7914566 0.07 0.255 108124 Other 0.01 0.107 8022690 0.01 0.106 7914566 0.04 0.184 108124
Child received care when sick 0.99 0.112 8062080 0.99 0.111 7953402 0.97 0.159 108678 By public/contributory system 0.32 0.465 8062080 0.32 0.466 7953402 0.17 0.38 108678 By public/non-contributory 0.45 0.498 8062080 0.45 0.498 7953402 0.28 0.448 108678 By private 0.2 0.404 8062080 0.2 0.401 7953402 0.47 0.499 108678 By other 0.01 0.115 8062080 0.01 0.113 7953402 0.05 0.215 108678
Child attends school 0.72 0.448 8043870 0.72 0.449 7935457 0.81 0.393 108413 Child is at age-appropriate level 0.89 0.312 5404839 0.89 0.313 5320066 0.94 0.243 84773 Years child is lagging in school 0.18 0.78 6736155 0.18 0.784 6637004 0.09 0.486 99151 Child works outside the home 0.03 0.17 8054724 0.03 0.17 7946134 0.01 0.113 108590 Child works at home 0.02 0.133 8054724 0.02 0.134 7946134 0.01 0.091 108590 Regressors: Child is female 0.49 0.5 8062080 0.49 0.5 7953402 0.5 0.5 108678 Child aged 0 to 5 0.32 0.468 8062080 0.32 0.468 7953402 0.25 0.433 108678 Child aged 6 to 12 0.4 0.489 8062080 0.39 0.488 7953402 0.54 0.499 108678 Child aged 13 to 17 0.28 0.45 8062080 0.28 0.45 7953402 0.21 0.408 108678 Child is indigenous 0.24 0.425 8060245 0.24 0.426 7951628 0.11 0.312 108617 Child only has mom in the HH 0.2 0.4 8062080 0.2 0.399 7953402 0.24 0.428 108678 Child only has dad in the HH 0.02 0.147 8062080 0.02 0.147 7953402 0.03 0.16 108678 Child has both parents in the HH 0.72 0.449 7947465 0.72 0.448 7840154 0.67 0.47 107311 Child has no parent in the HH 0.05 0.224 8062080 0.05 0.224 7953402 0.06 0.232 108678 Child born in Mexico 0.99 0.118 8062080 1 0 7953402 0 0 108678 Child born in the U.S. 0.01 0.118 8062080 0 0 7953402 1 0 108678 Child born elsewhere 0 0 8062080 0 0 7953402 0 0 108678 Child w/Mexican birth certificate 0.98 0.144 8006793 0.99 0.118 7898861 0.47 0.499 107932 Child w/foreign birth certificate 0.01 0.081 8006793 0 0.015 7898861 0.45 0.498 107932 Child w/no birth certificate 0.01 0.12 8006793 0.01 0.117 7898861 0.07 0.262 107932 Child dnk about birth certificate 0.01 0.091 8062080 0.01 0.091 7953402 0.01 0.089 108678 Child lived in Mexico in 2010 0.73 0.446 8002587 0.73 0.445 7894881 0.66 0.474 107706 Child lived in U.S. in 2010 0 0.053 8002587 0 0.03 7894881 0.14 0.348 107706 Child lived elsewhere in 2010 0.27 0.444 8002587 0.27 0.445 7894881 0.2 0.401 107706 HH size 5.34 2.112 8062080 5.35 2.117 7953402 4.99 1.746 108678 No of children 0-5 in the HH 0.83 0.906 8062080 0.83 0.907 7953402 0.78 0.866 108678 No of children 6-12 in the HH 1.1 0.991 8062080 1.1 0.991 7953402 1.26 0.976 108678 No of children 13-17 in the HH 0.72 0.837 8062080 0.72 0.838 7953402 0.57 0.763 108678 No of children 0-17 in the HH 2.65 1.397 8062080 2.65 1.399 7953402 2.61 1.257 108678 All kids born in Mexico 0.97 0.161 8062080 0.99 0.112 7953402 0 0 108678 All kids born in U.S. 0.01 0.088 8062080 0 0 7953402 0.55 0.498 108678 Kids born in Mex and the U.S. 0.01 0.118 8062080 0.01 0.088 7953402 0.45 0.497 108678 HH head’s age 42.68 12.669 8057905 42.69 12.676 7949279 41.79 12.181 108626 HH is female 0.25 0.432 8062080 0.25 0.432 7953402 0.28 0.449 108678 HH head’s schooling 8.31 4.569 8032410 8.29 4.569 7924156 9.38 4.485 108254 HH head is indigenous 0.29 0.454 8060869 0.29 0.455 7952222 0.18 0.38 108647 HH head born in Mexico 1 0.055 8048639 1 0.051 7940175 0.96 0.185 108464 H.H. head born in U.S. 0 0.036 8048639 0 0.03 7940175 0.03 0.171 108464 HH head born elsewhere 0 0.041 8048639 0 0.041 7940175 0.01 0.072 108464 HH head lived in Mex in 2010 0.99 0.088 8045452 0.99 0.076 7936983 0.85 0.353 108469 HH head lived in U.S. in 2010 0.01 0.085 8045452 0.01 0.072 7936983 0.14 0.349 108469 HH head lived elsewhere in 2010 0 0.023 8045452 0 0.022 7936983 0 0.065 108469 HH first wealth quartiles 0.25 0.432 7751688 0.25 0.434 7647076 0.08 0.272 104612 HH second wealth quartile 0.22 0.414 7751688 0.22 0.415 7647076 0.16 0.367 104612 HH third wealth quartile 0.2 0.399 7751688 0.2 0.398 7647076 0.22 0.416 104612 HH fourth wealth quartile 0.18 0.383 7751688 0.18 0.382 7647076 0.27 0.444 104612 HH resides in rural area 0.26 0.44 8062080 0.26 0.441 7953402 0.23 0.422 108678

46
Table B: Descriptive Statistics – Children Born in the U.S.
Variable Name All Children Recently Arrived H.H. Head
Head Arrived 6+ Yrs. Ago
Outcomes: Child affiliated to health provider 0.58 0.494 89931 0.52 0.499 15681 0.59 0.493 74250 Public/contributory 0.2 0.4 89931 0.12 0.322 15681 0.21 0.409 74250 Public/non-contributory 0.3 0.458 89931 0.35 0.478 15681 0.29 0.454 74250 Private 0.06 0.238 89931 0.04 0.192 15681 0.06 0.244 74250 Other 0.03 0.172 89931 0.02 0.147 15681 0.03 0.175 74250
Child received care when sick 0.98 0.153 90338 0.97 0.172 15735 0.98 0.15 74603 By public/contributory system 0.18 0.383 90338 0.12 0.325 15735 0.19 0.391 74603 By public/non-contributory 0.31 0.463 90338 0.36 0.48 15735 0.3 0.459 74603 By private 0.45 0.497 90338 0.45 0.498 15735 0.45 0.497 74603 By other 0.04 0.195 90338 0.04 0.192 15735 0.04 0.196 74603
Child attends school 0.95 0.217 90240 0.95 0.221 15722 0.95 0.216 74518 Child is at age-appropriate level 0.94 0.242 83832 0.94 0.241 13971 0.94 0.243 69861 Years child is lagging in school 0.1 0.511 89909 0.08 0.415 15680 0.1 0.526 74229 Child works outside the home 0.02 0.126 90253 0.01 0.105 15723 0.02 0.129 74530 Child works at home 0.01 0.101 90253 0.01 0.085 15723 0.01 0.104 74530
Regressors: Child is female 0.5 0.5 90338 0.5 0.5 15735 0.5 0.5 74603 Child aged 0 to 5 0.07 0.256 90338 0.11 0.312 15735 0.06 0.245 74603 Child aged 6 to 12 0.67 0.471 90338 0.7 0.456 15735 0.66 0.473 74603 Child aged 13 to 17 0.26 0.44 90338 0.19 0.389 15735 0.27 0.446 74603 Child is indigenous 0.12 0.324 90292 0.15 0.357 15732 0.11 0.318 74560 Child only has mom in the HH 0.25 0.432 90338 0.2 0.4 15735 0.26 0.437 74603 Child only has dad in the HH 0.03 0.167 90338 0.03 0.161 15735 0.03 0.169 74603 Child has both parents in the HH 0.66 0.475 89306 0.74 0.438 15600 0.64 0.48 73706 Child has no parent in the HH 0.06 0.242 90338 0.03 0.167 15735 0.07 0.252 74603 Child w/Mexican birth certificate 0.51 0.5 89747 0.5 0.5 15663 0.51 0.5 74084 Child w/foreign birth certificate 0.42 0.494 89747 0.44 0.497 15663 0.42 0.494 74084 Child w/no birth certificate 0.07 0.25 89747 0.06 0.244 15663 0.07 0.251 74084 Child dnk about birth certificate 0.01 0.086 90338 0 0.068 15735 0.01 0.088 74603 Child lived in Mexico in 2010 0.82 0.38 89388 0.18 0.385 15558 0.93 0.253 73830 Child lived in U.S. in 2010 0.18 0.38 89388 0.82 0.385 15558 0.07 0.253 73830 Child lived elsewhere in 2010 0 0 89388 0 0 15558 0 0 73830 HH size 5.02 1.736 90338 4.8 1.376 15735 5.06 1.786 74603 No of children 0-5 in the HH 0.59 0.777 90338 0.66 0.784 15735 0.58 0.776 74603 No of children 6-12 in the HH 1.42 0.939 90338 1.52 0.9 15735 1.41 0.945 74603 No of children 13-17 in the HH 0.66 0.789 90338 0.59 0.792 15735 0.67 0.788 74603 No of children 0-17 in the HH 2.67 1.252 90338 2.77 1.166 15735 2.65 1.265 74603 All kids born in Mexico 0 0 90338 0 0 15735 0 0 74603 All kids born in U.S. 0.51 0.5 90338 0.61 0.488 15735 0.5 0.5 74603 Kids born in Mex and the U.S. 0.48 0.5 90338 0.39 0.487 15735 0.5 0.5 74603 HH head’s age 42.54 11.944 90293 37.6 7.418 15725 43.36 12.345 74568 HH is female 0.29 0.454 90338 0.27 0.444 15735 0.29 0.455 74603 HH head’s schooling 9.07 4.386 90005 8.87 3.574 15667 9.1 4.505 74338 HH head is indigenous 0.19 0.39 90321 0.23 0.418 15732 0.18 0.384 74589 HH head born in Mexico 0.97 0.171 90156 0.94 0.235 15708 0.97 0.157 74448 H.H. head born in U.S. 0.03 0.157 90156 0.05 0.217 15708 0.02 0.145 74448 HH head born elsewhere 0 0.068 90156 0.01 0.095 15708 0 0.063 74448 HH head lived in Mex in 2010 0.86 0.349 90338 0 0 15735 1 0 74603 HH head lived in U.S. in 2010 0.14 0.349 90338 1 0 15735 0 0 74603 HH head lived elsewhere in 2010 0 0 90338 0 0 15735 0 0 74603 HH first wealth quartiles 0.09 0.284 87050 0.1 0.303 15127 0.09 0.281 71923 HH second wealth quartile 0.17 0.376 87050 0.18 0.384 15127 0.17 0.374 71923 HH third wealth quartile 0.23 0.418 87050 0.24 0.43 15127 0.22 0.416 71923 HH fourth wealth quartile 0.26 0.441 87050 0.27 0.446 15127 0.26 0.44 71923 HH resides in rural area 0.25 0.432 90338 0.31 0.464 15735 0.24 0.426 74603

47
Table C: Descriptive Statistics – Children Born in the U.S.
Variable Name Child w/Mex. Birth Cert. Child w/Foreign Birth Cert. Child w/out Birth Cert.
Outcomes: Child affiliated to health provider 0.77 0.422 49457 0.38 0.486 34473 0.34 0.474 5618 Public/contributory 0.27 0.442 49457 0.13 0.336 34473 0.13 0.333 5618 Public/non-contributory 0.45 0.498 49457 0.14 0.35 34473 0.13 0.332 5618 Private 0.05 0.221 49457 0.07 0.256 34473 0.06 0.238 5618 Other 0.02 0.124 49457 0.05 0.212 34473 0.03 0.18 5618
Child received care when sick 0.99 0.106 49570 0.97 0.181 34679 0.95 0.221 5667 By public/contributory system 0.23 0.421 49570 0.13 0.332 34679 0.11 0.316 5667 By public/non-contributory 0.41 0.492 49570 0.21 0.409 34679 0.19 0.389 5667 By private 0.33 0.471 49570 0.57 0.495 34679 0.59 0.492 5667 By other 0.02 0.136 49570 0.06 0.238 34679 0.06 0.242 5667
Child attends school 0.97 0.177 49532 0.93 0.247 34631 0.92 0.273 5661 Child is at age-appropriate level 0.95 0.216 46290 0.92 0.265 31962 0.92 0.275 5195 Years child is lagging in school 0.08 0.46 49361 0.12 0.547 34501 0.14 0.63 5631 Child works outside the home 0.01 0.119 49536 0.02 0.13 34636 0.02 0.143 5661 Child works at home 0.01 0.089 49536 0.01 0.11 34636 0.02 0.124 5661
Regressors: Child is female 0.5 0.5 49570 0.5 0.5 34679 0.49 0.5 5667 Child aged 0 to 5 0.06 0.245 49570 0.08 0.264 34679 0.09 0.286 5667 Child aged 6 to 12 0.66 0.474 49570 0.68 0.467 34679 0.67 0.47 5667 Child aged 13 to 17 0.28 0.447 49570 0.25 0.431 34679 0.24 0.426 5667 Child is indigenous 0.15 0.355 49556 0.09 0.287 34668 0.08 0.268 5665 Child only has mom in the HH 0.25 0.431 49570 0.25 0.433 34679 0.26 0.437 5667 Child only has dad in the HH 0.03 0.166 49570 0.03 0.17 34679 0.03 0.163 5667 Child has both parents in the HH 0.66 0.473 49028 0.65 0.478 34295 0.65 0.476 5582 Child has no parent in the HH 0.06 0.235 49570 0.07 0.253 34679 0.06 0.233 5667 Child w/Mexican birth certificate 1 0 49570 0 0 34679 0 0 5667 Child w/foreign birth certificate 0 0 49570 1 0 34679 0 0 5667 Child w/no birth certificate 0 0 49570 0 0 34679 1 0 5667 Child dnk about birth certificate 0 0 49570 0 0 34679 0 0 5667 Child lived in Mexico in 2010 0.84 0.362 49116 0.8 0.398 34266 0.81 0.389 5592 Child lived in U.S. in 2010 0.16 0.362 49116 0.2 0.398 34266 0.19 0.389 5592 Child lived elsewhere in 2010 0 0 49116 0 0 34266 0 0 5592 HH size 4.91 1.659 49570 5.11 1.748 34679 5.22 2.111 5667 No of children 0-5 in the HH 0.54 0.724 49570 0.64 0.818 34679 0.68 0.867 5667 No of children 6-12 in the HH 1.37 0.893 49570 1.48 0.972 34679 1.47 1.043 5667 No of children 13-17 in the HH 0.66 0.774 49570 0.65 0.799 34679 0.66 0.827 5667 No of children 0-17 in the HH 2.56 1.174 49570 2.77 1.285 34679 2.81 1.518 5667 All kids born in Mexico 0 0 49570 0 0 34679 0 0 5667 All kids born in U.S. 0.5 0.5 49570 0.52 0.499 34679 0.51 0.5 5667 Kids born in Mex and the U.S. 0.49 0.5 49570 0.47 0.499 34679 0.49 0.5 5667 HH head’s age 43.15 12.033 49550 41.92 11.884 34659 41.86 11.552 5663 HH is female 0.28 0.45 49570 0.29 0.456 34679 0.31 0.464 5667 HH head’s schooling 9.27 4.521 49400 8.87 4.217 34524 8.8 4.291 5649 HH head is indigenous 0.22 0.411 49561 0.16 0.364 34672 0.16 0.365 5667 HH head born in Mexico 0.98 0.135 49474 0.96 0.203 34595 0.96 0.187 5663 H.H. head born in U.S. 0.01 0.121 49474 0.04 0.189 34595 0.03 0.177 5663 HH head born elsewhere 0 0.061 49474 0.01 0.077 34595 0 0.062 5663 HH head lived in Mex in 2010 0.86 0.345 49490 0.85 0.355 34600 0.87 0.341 5657 HH head lived in U.S. in 2010 0.14 0.345 49490 0.15 0.355 34600 0.13 0.341 5657 HH head lived elsewhere in 2010 0 0 49490 0 0 34600 0 0 5657 HH first wealth quartiles 0.09 0.286 47797 0.09 0.284 33414 0.08 0.277 5441 HH second wealth quartile 0.16 0.371 47797 0.18 0.382 33414 0.17 0.372 5441 HH third wealth quartile 0.21 0.405 47797 0.24 0.43 33414 0.25 0.435 5441 HH fourth wealth quartile 0.26 0.44 47797 0.26 0.441 33414 0.27 0.446 5441 HH resides in rural area 0.27 0.446 49570 0.22 0.416 34679 0.24 0.424 5667

![TRANSNATIONAL TORT AND ACCESS TO REMEDY ......2018] Transnational Tort and Access to Remedy 3 against a corporate defendant in 17 years,5 and the only claim of its nature be brought](https://static.fdocuments.in/doc/165x107/5ea145d9e67a223afb6fb050/transnational-tort-and-access-to-remedy-2018-transnational-tort-and-access.jpg)
















