Health behavior paper on sleep deprivation
21
Sleep Behavior Among College Students Mackenzie Morgan HLTH 2400 Section 1
-
Upload
mtmorga -
Category
Health & Medicine
-
view
87 -
download
6
Transcript of Health behavior paper on sleep deprivation

Sleep Behavior Among College Students
Mackenzie Morgan
HLTH 2400
Section 1

HEALTH BEHAVIOR
The word “healthy” means different things to different people. According to WHO, and
for the sake of this paper, “health” is defined as “a state of complete physical, mental and social
well-being and not merely the absence of disease or infirmity” (World Health Organization,
2003). This definition takes a very holistic approach, noting not just the physical wellbeing of a
person, as many people would define health, but also social and mental aspects. In fact, social
interactions and good mental health lend themselves to a good physical health. One health
behavior in particular plays a key role in the maintenance of physical health, and that is sleep.
The recommended hours of sleep for children between fourteen and eighteen years are between
nine to eleven hours. For adults, the recommended hours of sleep lessens to seven to eight hours,
however, insufficient sleep is now considered a public health epidemic (CDC, 2014). Sufficient
sleep is notable for aiding in learning and memory, weight loss, cardiovascular health, and
warding off disease (Harvard, 2006). People that get a healthy amount of sleep every night are, in
turn, likely to participate in other healthy behaviors. People who report a lack of sleep on a
nightly basis often also self-report unintentional sleeping habits, such as falling asleep at the
wheel or during school.
STATISTICS
Figure 1 reports statistics on what percentage of each age group reported falling asleep
while driving in the past month. According to Figure 1, the adults age 25-35 reported the highest
percentage of falling asleep at the wheel, which those age 35-45 coming in second and those age
18-25 coming in third. In addition, other non-Hispanic races had the highest percentage of falling
asleep at the wheel, and males reported falling asleep at the wheel more than females.
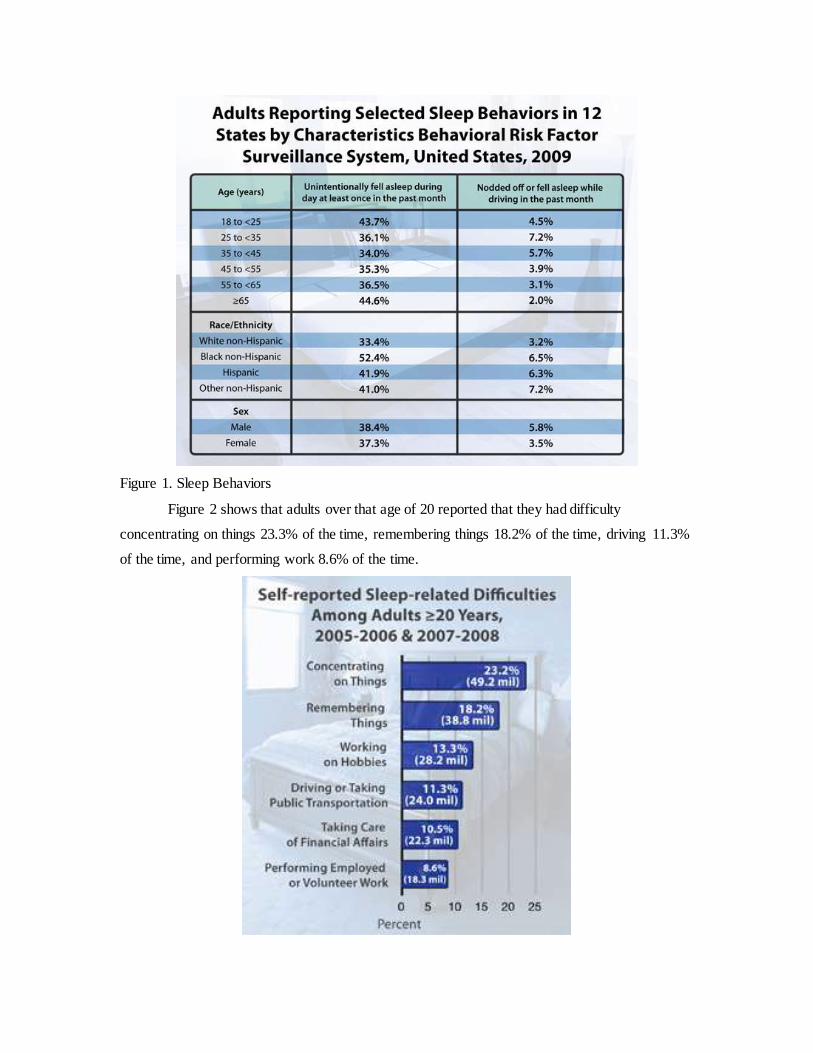
Figure 1. Sleep Behaviors
Figure 2 shows that adults over that age of 20 reported that they had difficulty
concentrating on things 23.3% of the time, remembering things 18.2% of the time, driving 11.3%
of the time, and performing work 8.6% of the time.

Figure 2. Sleep-related Difficulties
Even though only 26% of the population reported nodding off while driving in 2009,
54% of people reported driving while drowsy in 2009 (National Sleep Foundation, 2009). That
means that almost half of those that are drowsy actually fall asleep at the wheel. In 2009, 1.9
million reported having a car accident or a close call due to falling asleep at the wheel (National
Sleep Foundation, 2009). That is almost 2 million accidents that could have been prevented by
having enough sleep the night before. Long-term side effects of sleep deprivation include high
blood pressure, heart failure, obesity, Attention Deficit Disorder, and depression (Breus, 2006).
HEALTHY PEOPLE 2020
With 25% of adults in the U.S. reporting insufficient sleep at least half of every month,
Healthy People 2020, a program that sets national objectives for health improvement of
Americans, set three objectives: 1) “Increase the proportion of students in grades 9-12 who get
sufficient sleep” 2) “Increase the proportion of adults who get sufficient sleep” and 3) “Reduce
the rate of vehicular crashes per 100 million miles traveled that are due to drowsy driving”
(Healthy People, 2013).
The aim of this paper is to look at the sleeping habits of high school and college students,
determine reasons in which students lack good sleeping habits, and look at the risks associated
with poor sleeping habits.
BELIEFS, VALUES, ATTITUDES, KNOWLEDGE
People often don’t get enough sleep because they simply underestimate the importance of
sleep. According to a study published in the Journal of School Health in 2009, students know
what should be done and how to do it in regards to obtaining the right amount of sleep; however,
they still practice risky behaviors. In the study, 82% of participants believed that exercising
regularly throughout the week would aid sleep, but only 68.4% reported actually exercising
regularly (Dake, Noland, Price, & Telljohann, 2009). Similarly, 70% of participants stated that
taking naps throughout the day would help them catch up on sleep, but only 38.6% reported
taking naps (Dake et al., 2009). This data tells us that the issue with sleep deprivation is not that
students don’t know how to combat it, but that students don’t want to combat it. In other terms,
students don’t care enough about the problem to correct the problem. This indicates that, in order
to decrease the percentage of sleep deprivation among students, students’ attitudes and beliefs
about sleep must change.
According to the National Center on Sleep Disorders Research, there are many
misconceptions about sleep that could lead a person to not receive enough sleep. One common
misconceptions is that receiving one less hour of sleep every night wont have an affect on
daytime performance (National Institutes of Health, 2003). This is an incorrect way of thinking,
because a “sleep debt” will form. Over time, even losing one hour of sleep per night can cause a
steady decrease in task performance. Another popular misconception is that a person’s body will
adjust to their sleep schedule (National Institutes of Health, 2003). One way the body prepares to
sleep is by releasing melatonin. Melatonin is a hormone secreted from the pineal gland when
there are low light levels. That is why melatonin is naturally secreted at night. When a person
tries to perform activities during the brain’s time of rest, cognition and motor skills will be
affected (National Institutes of Health, 2003).
DEMOGRAPHICS AND SOCIOECONOMIC STANDARDS
There is statistical evidence that sleeping habits vary between races and ethnicities, as
well as different social classes. In a lecture by Michael Grandner, a professor at the University of
Pennsylvania and member of the Center for Sleep and Circadian Neurobiology, makes a case that
race and income level effect sleep outcome. As seen in Figure 3, compared to whites, blacks,
Mexican-Americans, and other Hispanics all had higher probabilities of poor sleep. Black were
more likely to partake in longer sleeps rather than shorter sleeps, as well as Mexican-Americans.
Other Hispanic and other non-Hispanic races were more likely to partake in short sleep rather
than long sleep (Grandner).

Figure 3. Sleep Duration in relation to race/ethnicity
Source: Grandner
As seen in Figure 4, whites living in poverty had the highest probability of poor sleep
compared to any other race living in poverty, while whites not living in poverty had the lowest
probability of poor sleep compared to any other races not living in poverty (Grandner).

Figure 4. Poverty among different race/ethnicities and sleep
Source: Grandner
Grandner also pointed out that at almost every income level, women had a higher
probability of sleep disturbance compared to men at the same level. Figure 5 shows that, in
regards to education, females had higher probabilities of sleep disturbance then males at every
education level. The education levels include less than high school, high school graduate, and
some college (Grandner). Location of residence also proved to be an indicator sleep, with inner-
cities being associated with a 24% increased risk for poor sleep (Grandner).
Figure 5. Education and Probability of Sleep Disturbances
Source: Grandner
PSYCHOLOGICAL OR PERSONALITY CHARACTERISTICS
At any given moment, approximately 25% of adolescents are experiencing some sort of
psychological distress (Glozier, Martiniuk, Patton, Ivers, Qiang, Hickie, Senserrick, Woodward,
Norton, Stevenson, 2010). This increase in psychological distress has been a rising trend over the
past couple of decades (Glozier et al., 2010). Adolescents typically at risk for having
psychological distress are usually the ones who report sleep disturbance or insufficient sleep
(Glozier et al. 2010). According to the Sleep Journal, the students most likely to sleep
deprivation are extroverts (Balkin, Killgore, Rupp, 2010). According to the study, those exposed
to 12 or more hours of social interaction were more likely to show signs of sleep deprivation than

those who had not been exposed to social interaction for the same amount of time (Balkin et al,
2010). The explanation behind this is that those found in social situations are fatiguing their brain
of sleep by using up the attention and alertness areas of the brain (Balkin et al, 2010).
SOCIAL SUPPORT
Studies show that the ties a young adult has to his or her family, friends, and coworkers
have an effect on his or her health behaviors (Umberson, Crosnoe, and Reczek, 2010). According
to scientists, the human brain evolved where protection against predators was aided by strong
social ties, which allowed for a sense of security that allowed for sleep (Trockel, Barnes, and
Egget, 2000). Research suggests that arguments with others can lead insufficient and disruptive
sleep, while strong social ties with others tend to allow for better quality sleep (Dahl, 2002).
Even though we aren’t predators today, our brain still functions in similar manor. Today, strong
and health ties with the community, our families, and our friends lend to better, less disruptive
sleeping habits.
SOCIAL INTERACTIONS
The social support a person receives comes from the social interactions they have, and
they do this through a number of ways. Social interactions can include relationships with family
members, friends, and the community. One, positive social interactions can make a person feel
cared and loved for. This positive interaction can even have and affect on a person’s physical
health, like lowering stress levels and heart rates. Studies show that high stress and heart rate can
cause disruptive sleep, so having positive social interactions is one way to lower that chance.
Conversely, if a social interaction is negative and causes stress to a person, that person may be
more inclined to have disruptive sleep due to that feeling of conflict and stress. (Umberson and
Montez, 2010). The most important social interaction is the one between a child and his or her
parent. While most college students have fewer interactions with their parents while they are at
college compared to when they are home, the effect is still the same. Children of divorced
parents are more likely to take on the family’s stress as their own, and as previously mentioned,
stress can lead to disruptive sleep (Maume, 2013). Kids of divorced parents can also become
stressed when a parent remarries. Also, if there is a financial burden in the family and a student
has to work or take our student loans to pay for schooling, then the student is more likely to
experience stress and disruptive sleep (Maume, 2013). Up until recently, sleep was not
considered a health behavior; therefore, more research must be done to fully evaluate how social
interactions affect sleep (Maume, 2013)

ORGANIZATIONS, SOCIAL INSTITUTIONS
There are two main organizations on the national level that deal with sleep. One is the
National Sleep Foundation, and another is the American Sleep Association. The National Sleep
Foundation was founded in 1990 in Washington D.C. The mission of the National Sleep
Foundation is to “improve health and well-being through sleep education and advocacy”
(Missions, n.d.). The National Sleep Foundation has set the goals to ensure that: 1) sleep is used
as a vital sign by the health care system, 2) the sleep/wake cycle becomes common knowledge, 3)
schools and workplaces are sleep-friendly, and 4) the science of sleep is used in product making
(Missions, n.d.). To carry out these goals, the National Sleep Foundation has a variety of
programs. For example, the Foundation puts on the National Sleep Awareness Week. This week
is hosted in March, and is designed to educate the public on the importance of sleep. The
Foundation has Sleep Care Center members that put on events in their local communities. The
National Sleep Foundation also supports sleep research and practices reaching out to health care
providers to help with the understanding of sleep-related health problems. In an effort to
collaborate well with professional, governmental, voluntary, and other organizations, the National
Sleep Foundation started the National Sleep Awareness Roundtable (About NSART, n.d.). The
National Sleep Awareness Roundtable coordinates communication between federal agencies,
professional organizations, and the public. The second major organization regarding sleep health
is the American Sleep Association, which was founded in 2002 (National Sleep Foundation,
Phys.Org, n.d.). The American Sleep Association, like the National Sleep Foundation, aims to
bring physicians, health care workers, scientists, and the public to educate all on the importance
of sleep and sleep disorders (About ASA, n.d.)
RELATIONSHIPS BETWEEN ORGANIZATIONS AND COMMUNITIES
Both the National Sleep Foundation and the American Sleep Association work with the
public to help combat unhealthy sleep behaviors. As mentioned before, the National Sleep
Foundation created the National Sleep Awareness Roundtable. One main goal of the National
Sleep Awareness Roundtable is to increase and improve “collaboration among local, state, and
federal agencies; professional organizations; and the public” (About NSF, n.d.). The American
Sleep Association also have links to handouts, message boards, chat rooms, video lectures, and
many more features on their website, making it easy for the public to get involved.
Social Media has also made it easier than ever to connect with the public. The National
Sleep Foundation’s Facebook page regularly shares news articles and information bits on sleep
health. Currently, the National Sleep Foundation is uploading photos to Facebook and Twitter
based on the 2014 Sleep in America Poll® as a part of National Sleep Awareness Week. One
example can be seen in Figure 6.
Figure 6. National Sleep Foundation’s Sleep Awareness Week Campaign Photo
Source: National Sleep Foundation Facebook
Social media has been very important in connecting these large-scale organizations with
the everyday person by brining the issue right to the public in their own homes and work places.
PHYSICAL ENVIRONMENT
Many factors go into the quality and amount of sleep received each night. For example,
room temperature, noise, and light can all affect the quality of sleep. Having cell phone,
computer, or television light later at night have been proven to cause people to go to sleep later
and have more disruptive sleep (Environmental, n.d.). Having loud noise, whether from traffic or
home, can also cause more disruptive sleep and even the release of stress hormones
(Environmental, n.d.). One study found that intermittent sounds, like something falling or a
honking car, could be more harmful to sleep quality than a continuous noise (Environmental,
n.d.). This led to the conclusion that people living in urban areas have a higher probability of
sleep deprivation (Environmental, n.d.).
There are some simple tips that people can follow to aid in healthy sleeping, such as
making a bedroom comfortable and inviting, turning out lights, turning off electronics, and
adjusting the thermostat (Environmental, n.d.)
PUBLIC POLICY, LAW, REGULATION

There are not public policies or laws regarding sleep, because of the nature of this health
behavior.
PREDISPOSING, ENABLING, REINFORCING FACTORS
Predisposing, enabling, and reinforcing factors all influence a person’s behavior, and
therefore, his or her health. Predisposing factors are considered the components that come before
a behavior is done, such as attitudes, knowledge, beliefs, values, and confidence (Williams,
2013). Predisposing factors for sleep behavior of college students would be knowledge about
adverse side effects of sleep deprivation, beliefs about how important healthy sleeping habits are,
and attitudes about getting enough sleep daily. Enabling factors are components that come before
the behavior, but they actually facilitate the behavior, such as teaching skills and physical
limitations (Williams, 2013). An example of an enabling factor is community resources that
educate students on the importance of sleep. Reinforcing factors provide feedback for a behavior
from interactions with family and friends or health professionals (Williams, 2013). Reinforcing
factors are outside of the person but have a social support feel to them, while enabling factors are
outside of the person, but are based more on physical limitations (Williams, 2013). Examples of
reinforcing factors would be how supportive friends and family are towards having enough sleep
daily, how accepting friends and roommates would be of getting enough sleep on weekends
instead of staying out late.
DETERMINANTS INTERACTING TO INFLUENCE BEHAVIOR
Predisposing, reinforcing, and enabling factors are all interwoven to allow for a behavior
to occur. Predisposing factors in regards to sleeping habits among college students include a
college student’s knowledge about the problems associated with sleep deprivation, his or her
attitudes and beliefs towards healthy sleeping habits, as well as his or her motivation to have
healthy sleeping habits. Enabling factors are factors that facilitate a behavior, so in the case of
college students’ sleeping habits, some enabling factors include whether or not services are
provided for increasing awareness of the consequences of sleep deprivation and other unhealthy
sleeping habits. Enabling factors really deal with ways to overcome physical barriers and
limitations, so other examples would be the resources available to learn how to have healthy
sleeping habits. Reinforcing factors are considered intrapersonal and interpersonal, so
interactions with friends, family, and health care professionals that provide feedback are
examples. These interactions provide feedback in the form of rewards or punishments.

Applications of this would be how encouraging a college student’s friends and family were of
trying to have healthy sleeping behaviors.
SOCIAL ECOLOGICAL MODEL DIAGRAM
THEORY OF PLANNED BEHAVIOR
In a study published by the Psychology and Health Journal in 2011, the theory of planned
behavior was applied to the sleeping habit behaviors of college students. A sample of 273 first
year undergraduate psychology students from Australia was given an initial questionnaire online.
One week after the initial questionnaire, the same students were given a follow up questionnaire.
The follow up questionnaire measured the frequency of healthy sleep behaviors. The sample
consisted mostly of students living at home and female students.

Figure 7. Theory of Reasoned Action and Planned Behavior Constructs
The 4 main constructs in the Theory of Reasoned Action and Planned Behavior are
attitude towards the behavior, subjective norms, perceived behavioral control, and behavioral
intention. In this particular study, attitude, subjective norm, perceived behavioral control, and
intention were all measured. Attitudes were measured using a 7-point semantic differential scale.
Subjective norms were measured using a scale of 7-point Likert scale, “1” for very unlikely and
“7” for very likely. Perceived behavioral control was measured for self-efficacy, controllability,
and confidence to partake in healthy sleep behaviors on a 7-point scale, from strongly disagree to
strongly agree. Intention was also measured on a 7-point scale from strongly disagree to strongly
agree. Another variable that was measured was response inhibition, which can be defined as the
ability to inhibit a desired action in favor of less prominent action. Response inhibition was
measured using a Go/No Go computer test. During this test, if a participant hit “go”, when he or
she was supposed to hit “no go” or vice versa, it was counted as an error. It is similar to self-
control. Behavior was measured after one week, and past behavior was assessed at the beginning
using a single item for each behavior (Kor and Mullan, 2011).
Of the 273 that started the survey, only 257 completed the entire survey. The results of
the study indicated that subjective norms and perceived behavioral control were significant
predictors of intention, while attitude was not; it was negatively weighted with intentions.
Intention itself predicted a small amount of variance in behavior. Once intention was controlled
for, perceived behavioral control added more variance to behavior (Kor and Mullan, 2011).
Subjective norms was said to be the strongest predictor of intentions, and response inhibition was
the strongest predictor of behavior (Kor and Mullan, 2011). This means that the sleep behaviors
of a college student are very likely to depend on the demands and reinforcement of friends and

family. With these results in mind, the ability to self control and self regulate should be the target
of interventions (Kor and Mullan, 2011).
INTEGRATIVE MODEL OF BEHAVIOR
The Integrative Model of Behavior follows the Theory of Reasoned Action and Planned
Behavior in the fact that both have attitudes, subjective norms, perceived behavioral control, and
behavioral intentions as major constructs. The Integrative Model of Behavior adds two more
constructs: behavioral skills and environmental constraints. These two new constructs are
considered moderators, meaning that they have an effect on behavior but doesn’t lie in the
pathway of other variables. This can been seen in Figure 8.
Figure 8. Integrative Model of Behavior Diagram (Robbins and Niederdeppe, 2014)
In a study published by Health Communication Journal, a small group of college
undergraduates were given a questionnaire about their attitudes, subjective norms, and perceived
behavioral control regarding sleep. These answers were used to generate a survey that was then
given to a larger group of college undergraduate students. For this particular study, attitudes,
perceived norms, perceived behavioral control, and behavioral intention were all measured, while
descriptive norm beliefs, injunctive norm beliefs, and beliefs about enablers and barriers to
behavioral control were all assessed.
Attitudes are defined as the beliefs about an expected outcome of participating in a
behavior (Robbins and Niederdeppe, 2014). This expectation can be positive or negative, and
that can influence intention to perform a behavior. Perceived norms are the social influences that

affect intention, such as how society approves or disapproves of a certain behavior (Robbins and
Niederdeppe, 2014). Perceived behavioral control is how in control a person feels over
performing a behavior, which in turn influences intention (Robbins and Niederdeppe, 2014).
Intention can be said to be a mediating variable, because it relates the constructs to the behavior.
In this study, attitudes were measured using 7-point semantic differential pairs.
Perceived norms were measured using a 7-point Likert scale from strongly disagree to strongly
agree, and Perceived behavioral control was measured using a 7-point semantic differential from
easy to hard on one question and a 7-point scale from strongly disagree to strongly agree for two
questions (Robbins and Niederdeppe, 2014). Between this study and the study previously
mentioned that applied the Theory of Planned Behavior to the sleeping habits of college students,
the way that attitude, perceived behavioral control, and perceived norms were measured was
almost identical. The difference between experiential attitude and instrumental attitude was not
measured, and
Self-efficacy was not differentiated from perceived control under perceived behavioral control.
Skill knowledge and environmental constraints were not measured, for unknown reasons.
The results of this study conclude that attitudes and perceived behavioral control were the
strongest predictors of intentions (Robbins and Niederdeppe, 2014). Indirect measures, such as
descriptive norm beliefs, injunctive norm beliefs, and beliefs about enablers and barriers to
behavioral control, were stronger predictors of intention than direct measures, such as attitude,
perceived norms, and perceived behavioral control (Robbins and Niederdeppe, 2014).
RECOMMENDATIONS FOR INTERVENTION
After looking at these two studies that apply different health behavior models to sleep
behavior of college students, it would seem as if knowledge about the benefits of healthy sleeping
behaviors. In both cases, the strongest predictor of intention was subjective and perceived norms.
This means that students are basing their behavior off of what society accepts, rather than what is
best of their health. Therefore, awareness of the benefits of having healthy sleeping habits in
regards to school and health in general, needs to be increased. A recommendation given by
Robbins and Niederdeppe (2014) was to have a “message-based intervention.” This means that
the importance of sleep and our misconceptions about how sleep affects our ability to perform
tasks can be address by simply informing students about the benefits of sleep (Robbins and
Niederdeppe, 2014). The same “message-based intervention” can be said for beliefs that time
management and less stress allow for healthy sleeping habits. While these two beliefs are
correlated with intention, not many students hold fast to them. This leaves rom for intervention.

In all, the promotion of healthy sleeping behaviors can be achieved through “strategic
communication” (Robbins and Niederdeppe, 2014). With very effective strategic
communication, messages that encourage healthy sleeping habits in college will hopefully
discourage behaviors and beliefs that discourage healthy sleeping habits. Robbins and
Niederdeppe (2014) also recommended that further research be conducted to study how
descriptive norms are formed and how the sleeping habits of others have so much affect on the
sleeping habits of one person.
INTERVENTION
In order to change the sleeping behavior of college students, the intrapersonal and
interpersonal levels of the social ecological model must be targeted. There are several ways in
which the intrapersonal level of communication from the social ecological model can be
addressed, and they include:
1) Increased knowledge about how to get better sleep
2) Increased knowledge about the negative consequences associated with poor sleeping
habits.
3) Increased skills in how to achieve healthy sleeping habits
Ways to address the interpersonal level of communication include:
1) Increased support from friends and family about healthy sleeping habits
2) Increased support from a job and/or school
In addressing the intrapersonal and interpersonal levels of the social ecological model, several
constructs of the theory of planned behavior and reasoned action are also addressed, such as
attitude towards healthy sleeping habits, perceived behavioral control to have healthy sleeping
habits, and how others view healthy sleeping habits. Increasing knowledge about how to get
better sleeping habits and increasing the support from friends, family, and community affect
behavioral intention, and intention ultimately affects whether or not a behavior is formed.
Another way to look at the sleep behavior of college students would be to look at
predisposing, enabling, and reinforcing factors associated with said behavior. Predisposing
factors, in this case, are very similar to the intrapersonal level of the social ecological model,
mainly being comprised of knowledge, attitudes, beliefs, and values of towards healthy sleeping
behaviors. Enabling factors are antecedents that facilitate a behavior, such as skills, and
resources, and policies; enabling factors are a mixture of the community and organizational levels
of the social ecological model. Reinforcing factors elicit feedback for behavior from interactions

with friends and family and would lead more toward the interpersonal level of the social
ecological model.
One organizational level intervention for a university could be having discussions put on
by student government or some authoritative campus organization, such as a psychology
department, that would be open to college students to allow them to understand why and how to
get better sleep. By having student government try to educate on the issue, more students will be
more likely to listen because student government is comprised of peers of the same age dealing
with the same issues. By having a certain department, such as psychology, put on a discussion,
students will be more likely to listen because a psychology department has authority over the
subject because they will have the most knowledge about the consequences on your body from
insufficient sleep. This intervention would target both interpersonal and intrapersonal levels of
the social ecological model by increasing knowledge, awareness, and skills for better sleeping
habits, as well as targeting the other students and friends to have healthy sleeping habits. This
intervention also addresses the predisposing factors and reinforcing factor, while the intervention
itself would be an enabling factor.
Other nonpharmaceutical interventions can include relaxation therapies, stimulus control
therapy, and sleep restriction therapy (Austin, 2007). Relaxation therapy is a way to calm the
mind before sleep (National Sleep Foundation). This can be accomplished through breathing
exercises, helpful visualizations, mediation, and muscle relaxation exercises (National Sleep
Foundation). Stimulus control therapy is aimed to rewire the brain so that lying in bed is
associated with sleep instead of being awake (National Sleep Foundation). By not napping
throughout the day and getting up at the same time each day, a person can reset his or her bedtime
cues (National Sleep Foundation). Finally, sleep restriction therapy is when a person is restricted
to being in bed for the amount of time he or she actually spends asleep, not how much he or she
wants to sleep (National Sleep Foundation). The goal of this is increase sleep efficiency. Then, a
small amount of time is added to the time in bed, to eventually reach the desired amount of sleep.
There are also pharmaceutical interventions, such as taking drugs that help you sleep
easier and deeper at night. These drugs, however, should only be taken for insomnia that has
been diagnosed by a doctor and has a genetic or biological etiology (National Sleep Foundation).
Even then, drugs that help treat insomnia should only be taken for short periods of time (National
Sleep Foundation).
Some limitations must also be addressed in regards to intervention success. The only
way that relaxation therapy, stimulus control therapy, and sleep restriction therapy will work is if
a student suffers from insomnia. If a student is fully capable of getting better sleep, but chooses

not to, then only the first intervention mentioned will work. However, if a student does not have
healthy sleeping habits because of insomnia or another sleep related disease, then educating him
or her on the importance of healthy sleeping behaviors will be no good, since he or she cannot
partake, even if he or she wishes to. Therefore, there are two categories that a student can be
placed into: 1) choosing not to have healthy sleeping habits and 2) not being able to have healthy
sleeping habits because of a sleep related disease. To get to the root of those who choose not to
have healthy sleeping habits, the attitude and knowledge about the importance of acting on a
certain behavior must be examined. This type of intervention was the first one mentioned about
having a campus discussion. To get to the root of those who cannot sleep well because of
insomnia, specific medical interventions, such as therapy or pharmaceutical drugs, must be used
to treat the disease.
CONCLUSION
Sleep deprivation among college students is a real health behavior epidemic that needs to
be addressed. Sleep is very important in maintaining physical health, aiding in learning and
memorization, increasing cardiovascular health, and warding off diseases (Harvard, 2006). For
college students, lack of sleep often leads to decreased quality of work. In order to combat this
epidemic, the attitudes and beliefs about the importance of sleep must be changed. This can be
done with several interventions that target changing social norms, such as discussions put on by
student government and fliers put up in dorms and residence halls. In the case that a student
doesn’t choose to not get enough sleep, but just can’t get enough sleep, meditation and relaxation
therapies have proven to help (National Sleep Foundation, Insomnia). Pharmaceutical
interventions have also proven effective when a student suffers from insomnia; however,
pharmaceuticals should not be taken for extended periods of time, for the risk of addition to them.
In all, the most change in the sleeping habits of college students will occur if social norms and
perceived behavioral control are changed (Kor and Mullan, 2011).

RESOURCES
About ASA. American Sleep Association. Retrieved 3 March 2014, from
http://www.sleepassociation.org/index.php?p=about
About NSART. NSART. Retrieved 3 March 2014, from http://www.nsart.org/aboutus
About NSF. National Sleep Foundation. Retrieved 3 March 2014, from
http://www.sleepfoundation.org/about-us
Austin, Bess. (2007). Sleep Deprivation in the College Student A Problem Worth
Addressing.
Balkin, T.J., Killgore, W.D., Rupp T.L., (2010). Socializing by Day May Affect
Performance by Night: Vulnerability to Sleep Deprivation is Differentially
Mediated by Social Exposure in Extraverts vs Introverts. Sleep Journal. 33(11):
1475-85.
Breus, M. J. (2006). Sleep Habits: More Important Than You Think. Retrieved January
26, 2014, from
http://www.webmd.com/sleep-disorders/features/important-sleep-habits?page=2
CDC (2014). Insufficient Sleep Is a Public Health Epidemic. Retrieved January 26, 2014,
from http://www.cdc.gov/features/dssleep/
Dahl R,E. (2002). The Regulation of Sleep-Arousal, Affect, and Attention in
Adolescence: Some Questions and Speculations. In Adolescent Sleep Patterns:
Biological, Social, and Psychological Influences, (Pp. 269-84) edited by Carskadon M.
A. New York: Cambridge University Press.
Dake, J., Noland, H., Price, J.H., & Telljohann, S.K. (2009). Adolescents’ Sleep
Behaviors and Perceptions of Sleep. Journal of School Health, 79(5), 224-230. doi:
10.1111/j.1746-1561.2009.00402.x
Environmental Sleep Factors. World Sleep Day. Retrieved 3 March 2014, from
http://worldsleepday.org/environmental-sleep-factors/
Glozier, N., Martiniuk, A., Patton, G., Ivers, R., Qiang, L., Hickie, I., Senserrick, T.,
Woodward, M., Norton, R., Stevenson, M. (2010). Short Sleep Duration in Prevalent and
Persistent Psychological Distress in Yound Adults: The DRIVE Study. Sleep Journal,
33(9), 1139-1145.
Grandner, M.A. Racial/Ethnic and Socioeconomic Sleep Disparities: A key factor in
health disparities? [PDF document]. Retrieved from University of California, San
Francisco Center for Health and Community Online Web site:
http://chc.ucsf.edu/coast/pdfs/2012%20Symposium/Grandner_presentations.pdf
Harvard (2006). Importance of Sleep: Six reasons not to scrimp on sleep. Retrieved
January 27, 2014, from
http://www.health.harvard.edu/press_releases/importance_of_sleep_and_health
Healthy People (2013). Sleep Health Objectives. Retrieved January 27, 2014, from
http://www.healthypeople.gov/2020/topicsobjectives2020/objectiveslist.aspx?topicId=38
Kor, K., Mullan, B.A. (13 Jun 2011). Sleep hygiene behaviours: An application of the
theory of planned behaviour and the investigation of perceived autonomy support, past
behavior and response inhibition. Psychology & Health Journal, 26(9), 1208-1224. doi:
10.1080/08870446.2010.551210
Maume, D.J. (2013). Social Ties and Adolescent Sleep Disruption. Journal of Health and
Social Behavior, 54, 497-515. doi:10.1177/0022146513498512
McKenna, J., Mack J. (1992). “Origins and Paleoecology of Hominid Sleep: An
Evolutionary Perspective.” Sleep Research 2(1):1
Missions and Goals. National Sleep Foundation. Retrieved 3 March 2014, from
http://www.sleepfoundation.org/mission-and-goals
National Institutes of Health (2003). Teacher’s Guide: Information about Sleep.
Retrieved from http://science.education.nih.gov/supplements/nih3/sleep/guide/info-
sleep.htm
National Sleep Foundation (2009). 1.9 Million Drivers Have Fatigue-Related Car
Crashes or Near Misses Each Year. Retrieved January 27, 2014, from
http://www.sleepfoundation.org/article/press-release/19-million-drivers-have-
fatigue-related-car-crashes-or-near-misses-each-year
National Sleep Foundation. (n.d.). In Facebook (Organization). Retrieved March 3,
2014, from https://www.facebook.com/nationalsleepfoundation
National Sleep Foundation .Insomnia and Sleep. Retrieved from
http://sleepfoundation.org/sleep-disorders-problems/insomnia-and-sleep
National Sleep Foundation. Phys. Retrieved 3 March 2014, from
http://phys.org/partners/national-sleep-foundation/
Robbins, R., Niederdeppe, J. (21 Jan 2014). Using the Integrative Model of Behavioral
Prediction to Identify Promising Message Strategies to Promote Healthy Sleep Behavior
Among College Students. Health Communication Journal. doi:
10.1080/10410236.2013.835215
Trockel, M. T., Barnes, M. D., Egget, D. L. (2000). Health-related variables and
academic performance among first-year college students: Implications for sleep and other
behaviors. Journal of American College Health, 49, 125-31. doi:
10.1080/07448480009596294
Umberson, D., Crosnoe R., Reczek C. (2010). Social Relationships and Health Behavior
across the Life Course. Annual Review of Sociology, 36, 139–57. doi: 10.1146/annurev-
soc-070308-120011
Umberson D., Montez, J.K. (2010). Social Relationships and Health: A Flashpoint for
Health Policy. Journal of Health and Social Behavior , 51, 54–66. doi:
10.1177/0022146510383501
Williams, J. (2013) Predisposing, Enabling & Reinforcing Factors [PowerPoint
Slides]. Retrieved from: https://bb.clemson.edu/
World Health Organization (2003). Who Definition of Health. Retrieved January 26,
2014, from http://www.who.int/about/definition/en/print.html