Headache - Home Page | Department of Medicine Conference1... · - Tension-type headache -...
75
Anna Morenkova, MD, PhD Assistant Professor Department of Neurology UC Irvine Headache
Transcript of Headache - Home Page | Department of Medicine Conference1... · - Tension-type headache -...
Anna Morenkova MD PhD Assistant Professor
Department of Neurology UC Irvine
Headache
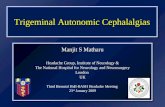
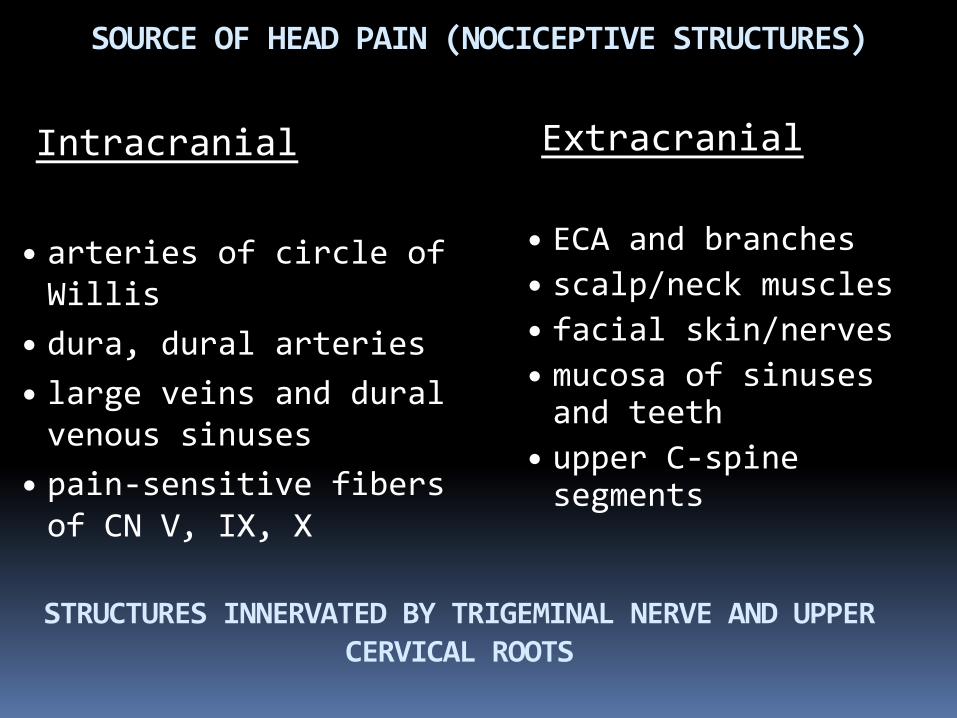
SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
Intracranial
bull arteries of circle of Willis
bull dura dural arteries bull large veins and dural venous sinuses
bull pain-sensitive fibers of CN V IX X
Extracranial
bull ECA and branches bull scalpneck muscles bull facial skinnerves bull mucosa of sinuses and teeth
bull upper C-spine segments
STRUCTURES INNERVATED BY TRIGEMINAL NERVE AND UPPER CERVICAL ROOTS
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - Other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorders - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache Disorders Classification
A 39-year old man presents to your office with the abrupt onset severe diffuse headache nausea and blurred vision Headache began about 6 hours ago He tried high dose ibuprofen combined with acetaminophen twice since headache onset with no relief He has a history of migraine with 2-3 headaches per month that would respond to ibuprofen within 2 hours of use His blood pressure is 14570 His examination is normal
Headache High prevalence
Presentation to medical attention is either due to headache severity failure to respond to analgesics or due to concern of underlying pathology
Headache is a frequent presenting symptom in the emergency room
Physical examination is often normal
gt90 of patients have PRIMARY HEADACHE DISORDER
History is most important
First objective Distinguish primary from secondary headaches
Second objective Establish correct diagnosis of primary
headache disorder
Third objective Initiate appropriate abortive and
preventive treatment
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flags Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
YES
Headache features HistoryReview of systems
Diagnostic Criteria Red Flags
Headache features
Location Quality Severity Time to peak Duration Constant or episodic Frequency Periodicity Onset
Associated neurologic symptoms
Preceding transient neurologic symptoms (aura)
Aggravating and alleviating factors
Pertinent Questions History of prior illness
Constitutional symptoms
Transient neurologic symptoms preceding associated or following the headache
Medicationssupplements (new medications or changes in medication regimen)
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
SNOOP4 secondary causes (Red Flags) Systemic symptomssigns fever chills night sweats myalgia weight loss (GCA meningoencephalitisabscess malignancy systemic infection)
Neurologic symptomssigns (focal or global including changes in behavior or personality diplopia transient visual obscurations pulsatile tinnitus numbness or weakness in facelimbs vertigo loss of balance)
Onset after age 50 Onset recent
Pattern change (if previous history of headache) 1 Progressive headache with loss of headache-free periods 2 Precipitated by Valsalva Chiari malformation structural lesions that obstruct CSF flow dural CSF leak Most headaches are worsened by Valsalva Certain primary headaches may be precipitated by Valsalva (primary cough headache) All headaches that are provoked by Valsalva require imaging to rule out secondary cause
3 Postural aggravation (worse standing or lying) intracranial hypotension (CSF leak) Chiari intracranial hypertension (CSF flow obstruction) worse with certain neck movementsposition (cervicogenic)
4 Papilledema Indicates intracranial hypertension Ask about transient visual obscurations diplopia and visual field defects
A 39-year old man presents to your office with the abrupt onset extremely severe diffuse headache nausea and blurred vision Headache began about 6 hours ago When asked he admits that this is the worst headache he has ever had He also reports some neck pain and says it feels stiff He has a history of migraine What would be the next course of action 1 Ketorolac im injection and antiemetic 2 Sumatriptan sc injection 3 Arrange for an urgent lumbar puncture 4 Obtain an urgent CT of the head without contrast 5 Start IV hydration with NS CT of the head is normal Next step LP does not show xanthochromia Next step CTA hn is normal Next step
Thunderclap Headache
Severe headache of abrupt onset (peaks within seconds)
No warning as a clap of thunder MUST BE EVALUATED in the Emergency Room
Causes of Thunderclap Headache SAH due to cerebral aneurysm or AVM rupture
Cervico-cerebral arterial dissection
Cerebral venous sinus thrombosis
Acute hypertensive crisis
Illicit drug use with secondary intracranial hemorrhage or infarction
Cerebral reversible vasoconstriction syndrome posterior reversible encephalopathy syndrome (PRES)
Pituitary apoplexy
Third ventricle colloid cyst
Spontaneous intracranial hypotension (CSF leak)
Ischemic or hemorrhagic stroke
Primary thunderclap headache (no underlying intracranial pathology after extensive workup)
Presenter
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
Intracranial
bull arteries of circle of Willis
bull dura dural arteries bull large veins and dural venous sinuses
bull pain-sensitive fibers of CN V IX X
Extracranial
bull ECA and branches bull scalpneck muscles bull facial skinnerves bull mucosa of sinuses and teeth
bull upper C-spine segments
STRUCTURES INNERVATED BY TRIGEMINAL NERVE AND UPPER CERVICAL ROOTS
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - Other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorders - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache Disorders Classification
A 39-year old man presents to your office with the abrupt onset severe diffuse headache nausea and blurred vision Headache began about 6 hours ago He tried high dose ibuprofen combined with acetaminophen twice since headache onset with no relief He has a history of migraine with 2-3 headaches per month that would respond to ibuprofen within 2 hours of use His blood pressure is 14570 His examination is normal
Headache High prevalence
Presentation to medical attention is either due to headache severity failure to respond to analgesics or due to concern of underlying pathology
Headache is a frequent presenting symptom in the emergency room
Physical examination is often normal
gt90 of patients have PRIMARY HEADACHE DISORDER
History is most important
First objective Distinguish primary from secondary headaches
Second objective Establish correct diagnosis of primary
headache disorder
Third objective Initiate appropriate abortive and
preventive treatment
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flags Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
YES
Headache features HistoryReview of systems
Diagnostic Criteria Red Flags
Headache features
Location Quality Severity Time to peak Duration Constant or episodic Frequency Periodicity Onset
Associated neurologic symptoms
Preceding transient neurologic symptoms (aura)
Aggravating and alleviating factors
Pertinent Questions History of prior illness
Constitutional symptoms
Transient neurologic symptoms preceding associated or following the headache
Medicationssupplements (new medications or changes in medication regimen)
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
SNOOP4 secondary causes (Red Flags) Systemic symptomssigns fever chills night sweats myalgia weight loss (GCA meningoencephalitisabscess malignancy systemic infection)
Neurologic symptomssigns (focal or global including changes in behavior or personality diplopia transient visual obscurations pulsatile tinnitus numbness or weakness in facelimbs vertigo loss of balance)
Onset after age 50 Onset recent
Pattern change (if previous history of headache) 1 Progressive headache with loss of headache-free periods 2 Precipitated by Valsalva Chiari malformation structural lesions that obstruct CSF flow dural CSF leak Most headaches are worsened by Valsalva Certain primary headaches may be precipitated by Valsalva (primary cough headache) All headaches that are provoked by Valsalva require imaging to rule out secondary cause
3 Postural aggravation (worse standing or lying) intracranial hypotension (CSF leak) Chiari intracranial hypertension (CSF flow obstruction) worse with certain neck movementsposition (cervicogenic)
4 Papilledema Indicates intracranial hypertension Ask about transient visual obscurations diplopia and visual field defects
A 39-year old man presents to your office with the abrupt onset extremely severe diffuse headache nausea and blurred vision Headache began about 6 hours ago When asked he admits that this is the worst headache he has ever had He also reports some neck pain and says it feels stiff He has a history of migraine What would be the next course of action 1 Ketorolac im injection and antiemetic 2 Sumatriptan sc injection 3 Arrange for an urgent lumbar puncture 4 Obtain an urgent CT of the head without contrast 5 Start IV hydration with NS CT of the head is normal Next step LP does not show xanthochromia Next step CTA hn is normal Next step
Thunderclap Headache
Severe headache of abrupt onset (peaks within seconds)
No warning as a clap of thunder MUST BE EVALUATED in the Emergency Room
Causes of Thunderclap Headache SAH due to cerebral aneurysm or AVM rupture
Cervico-cerebral arterial dissection
Cerebral venous sinus thrombosis
Acute hypertensive crisis
Illicit drug use with secondary intracranial hemorrhage or infarction
Cerebral reversible vasoconstriction syndrome posterior reversible encephalopathy syndrome (PRES)
Pituitary apoplexy
Third ventricle colloid cyst
Spontaneous intracranial hypotension (CSF leak)
Ischemic or hemorrhagic stroke
Primary thunderclap headache (no underlying intracranial pathology after extensive workup)
Presenter
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - Other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorders - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache Disorders Classification
A 39-year old man presents to your office with the abrupt onset severe diffuse headache nausea and blurred vision Headache began about 6 hours ago He tried high dose ibuprofen combined with acetaminophen twice since headache onset with no relief He has a history of migraine with 2-3 headaches per month that would respond to ibuprofen within 2 hours of use His blood pressure is 14570 His examination is normal
Headache High prevalence
Presentation to medical attention is either due to headache severity failure to respond to analgesics or due to concern of underlying pathology
Headache is a frequent presenting symptom in the emergency room
Physical examination is often normal
gt90 of patients have PRIMARY HEADACHE DISORDER
History is most important
First objective Distinguish primary from secondary headaches
Second objective Establish correct diagnosis of primary
headache disorder
Third objective Initiate appropriate abortive and
preventive treatment
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flags Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
YES
Headache features HistoryReview of systems
Diagnostic Criteria Red Flags
Headache features
Location Quality Severity Time to peak Duration Constant or episodic Frequency Periodicity Onset
Associated neurologic symptoms
Preceding transient neurologic symptoms (aura)
Aggravating and alleviating factors
Pertinent Questions History of prior illness
Constitutional symptoms
Transient neurologic symptoms preceding associated or following the headache
Medicationssupplements (new medications or changes in medication regimen)
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
SNOOP4 secondary causes (Red Flags) Systemic symptomssigns fever chills night sweats myalgia weight loss (GCA meningoencephalitisabscess malignancy systemic infection)
Neurologic symptomssigns (focal or global including changes in behavior or personality diplopia transient visual obscurations pulsatile tinnitus numbness or weakness in facelimbs vertigo loss of balance)
Onset after age 50 Onset recent
Pattern change (if previous history of headache) 1 Progressive headache with loss of headache-free periods 2 Precipitated by Valsalva Chiari malformation structural lesions that obstruct CSF flow dural CSF leak Most headaches are worsened by Valsalva Certain primary headaches may be precipitated by Valsalva (primary cough headache) All headaches that are provoked by Valsalva require imaging to rule out secondary cause
3 Postural aggravation (worse standing or lying) intracranial hypotension (CSF leak) Chiari intracranial hypertension (CSF flow obstruction) worse with certain neck movementsposition (cervicogenic)
4 Papilledema Indicates intracranial hypertension Ask about transient visual obscurations diplopia and visual field defects
A 39-year old man presents to your office with the abrupt onset extremely severe diffuse headache nausea and blurred vision Headache began about 6 hours ago When asked he admits that this is the worst headache he has ever had He also reports some neck pain and says it feels stiff He has a history of migraine What would be the next course of action 1 Ketorolac im injection and antiemetic 2 Sumatriptan sc injection 3 Arrange for an urgent lumbar puncture 4 Obtain an urgent CT of the head without contrast 5 Start IV hydration with NS CT of the head is normal Next step LP does not show xanthochromia Next step CTA hn is normal Next step
Thunderclap Headache
Severe headache of abrupt onset (peaks within seconds)
No warning as a clap of thunder MUST BE EVALUATED in the Emergency Room
Causes of Thunderclap Headache SAH due to cerebral aneurysm or AVM rupture
Cervico-cerebral arterial dissection
Cerebral venous sinus thrombosis
Acute hypertensive crisis
Illicit drug use with secondary intracranial hemorrhage or infarction
Cerebral reversible vasoconstriction syndrome posterior reversible encephalopathy syndrome (PRES)
Pituitary apoplexy
Third ventricle colloid cyst
Spontaneous intracranial hypotension (CSF leak)
Ischemic or hemorrhagic stroke
Primary thunderclap headache (no underlying intracranial pathology after extensive workup)
Presenter
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
A 39-year old man presents to your office with the abrupt onset severe diffuse headache nausea and blurred vision Headache began about 6 hours ago He tried high dose ibuprofen combined with acetaminophen twice since headache onset with no relief He has a history of migraine with 2-3 headaches per month that would respond to ibuprofen within 2 hours of use His blood pressure is 14570 His examination is normal
Headache High prevalence
Presentation to medical attention is either due to headache severity failure to respond to analgesics or due to concern of underlying pathology
Headache is a frequent presenting symptom in the emergency room
Physical examination is often normal
gt90 of patients have PRIMARY HEADACHE DISORDER
History is most important
First objective Distinguish primary from secondary headaches
Second objective Establish correct diagnosis of primary
headache disorder
Third objective Initiate appropriate abortive and
preventive treatment
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flags Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
YES
Headache features HistoryReview of systems
Diagnostic Criteria Red Flags
Headache features
Location Quality Severity Time to peak Duration Constant or episodic Frequency Periodicity Onset
Associated neurologic symptoms
Preceding transient neurologic symptoms (aura)
Aggravating and alleviating factors
Pertinent Questions History of prior illness
Constitutional symptoms
Transient neurologic symptoms preceding associated or following the headache
Medicationssupplements (new medications or changes in medication regimen)
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
SNOOP4 secondary causes (Red Flags) Systemic symptomssigns fever chills night sweats myalgia weight loss (GCA meningoencephalitisabscess malignancy systemic infection)
Neurologic symptomssigns (focal or global including changes in behavior or personality diplopia transient visual obscurations pulsatile tinnitus numbness or weakness in facelimbs vertigo loss of balance)
Onset after age 50 Onset recent
Pattern change (if previous history of headache) 1 Progressive headache with loss of headache-free periods 2 Precipitated by Valsalva Chiari malformation structural lesions that obstruct CSF flow dural CSF leak Most headaches are worsened by Valsalva Certain primary headaches may be precipitated by Valsalva (primary cough headache) All headaches that are provoked by Valsalva require imaging to rule out secondary cause
3 Postural aggravation (worse standing or lying) intracranial hypotension (CSF leak) Chiari intracranial hypertension (CSF flow obstruction) worse with certain neck movementsposition (cervicogenic)
4 Papilledema Indicates intracranial hypertension Ask about transient visual obscurations diplopia and visual field defects
A 39-year old man presents to your office with the abrupt onset extremely severe diffuse headache nausea and blurred vision Headache began about 6 hours ago When asked he admits that this is the worst headache he has ever had He also reports some neck pain and says it feels stiff He has a history of migraine What would be the next course of action 1 Ketorolac im injection and antiemetic 2 Sumatriptan sc injection 3 Arrange for an urgent lumbar puncture 4 Obtain an urgent CT of the head without contrast 5 Start IV hydration with NS CT of the head is normal Next step LP does not show xanthochromia Next step CTA hn is normal Next step
Thunderclap Headache
Severe headache of abrupt onset (peaks within seconds)
No warning as a clap of thunder MUST BE EVALUATED in the Emergency Room
Causes of Thunderclap Headache SAH due to cerebral aneurysm or AVM rupture
Cervico-cerebral arterial dissection
Cerebral venous sinus thrombosis
Acute hypertensive crisis
Illicit drug use with secondary intracranial hemorrhage or infarction
Cerebral reversible vasoconstriction syndrome posterior reversible encephalopathy syndrome (PRES)
Pituitary apoplexy
Third ventricle colloid cyst
Spontaneous intracranial hypotension (CSF leak)
Ischemic or hemorrhagic stroke
Primary thunderclap headache (no underlying intracranial pathology after extensive workup)
Presenter
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Headache High prevalence
Presentation to medical attention is either due to headache severity failure to respond to analgesics or due to concern of underlying pathology
Headache is a frequent presenting symptom in the emergency room
Physical examination is often normal
gt90 of patients have PRIMARY HEADACHE DISORDER
History is most important
First objective Distinguish primary from secondary headaches
Second objective Establish correct diagnosis of primary
headache disorder
Third objective Initiate appropriate abortive and
preventive treatment
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flags Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
YES
Headache features HistoryReview of systems
Diagnostic Criteria Red Flags
Headache features
Location Quality Severity Time to peak Duration Constant or episodic Frequency Periodicity Onset
Associated neurologic symptoms
Preceding transient neurologic symptoms (aura)
Aggravating and alleviating factors
Pertinent Questions History of prior illness
Constitutional symptoms
Transient neurologic symptoms preceding associated or following the headache
Medicationssupplements (new medications or changes in medication regimen)
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
SNOOP4 secondary causes (Red Flags) Systemic symptomssigns fever chills night sweats myalgia weight loss (GCA meningoencephalitisabscess malignancy systemic infection)
Neurologic symptomssigns (focal or global including changes in behavior or personality diplopia transient visual obscurations pulsatile tinnitus numbness or weakness in facelimbs vertigo loss of balance)
Onset after age 50 Onset recent
Pattern change (if previous history of headache) 1 Progressive headache with loss of headache-free periods 2 Precipitated by Valsalva Chiari malformation structural lesions that obstruct CSF flow dural CSF leak Most headaches are worsened by Valsalva Certain primary headaches may be precipitated by Valsalva (primary cough headache) All headaches that are provoked by Valsalva require imaging to rule out secondary cause
3 Postural aggravation (worse standing or lying) intracranial hypotension (CSF leak) Chiari intracranial hypertension (CSF flow obstruction) worse with certain neck movementsposition (cervicogenic)
4 Papilledema Indicates intracranial hypertension Ask about transient visual obscurations diplopia and visual field defects
A 39-year old man presents to your office with the abrupt onset extremely severe diffuse headache nausea and blurred vision Headache began about 6 hours ago When asked he admits that this is the worst headache he has ever had He also reports some neck pain and says it feels stiff He has a history of migraine What would be the next course of action 1 Ketorolac im injection and antiemetic 2 Sumatriptan sc injection 3 Arrange for an urgent lumbar puncture 4 Obtain an urgent CT of the head without contrast 5 Start IV hydration with NS CT of the head is normal Next step LP does not show xanthochromia Next step CTA hn is normal Next step
Thunderclap Headache
Severe headache of abrupt onset (peaks within seconds)
No warning as a clap of thunder MUST BE EVALUATED in the Emergency Room
Causes of Thunderclap Headache SAH due to cerebral aneurysm or AVM rupture
Cervico-cerebral arterial dissection
Cerebral venous sinus thrombosis
Acute hypertensive crisis
Illicit drug use with secondary intracranial hemorrhage or infarction
Cerebral reversible vasoconstriction syndrome posterior reversible encephalopathy syndrome (PRES)
Pituitary apoplexy
Third ventricle colloid cyst
Spontaneous intracranial hypotension (CSF leak)
Ischemic or hemorrhagic stroke
Primary thunderclap headache (no underlying intracranial pathology after extensive workup)
Presenter
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
First objective Distinguish primary from secondary headaches
Second objective Establish correct diagnosis of primary
headache disorder
Third objective Initiate appropriate abortive and
preventive treatment
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flags Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
YES
Headache features HistoryReview of systems
Diagnostic Criteria Red Flags
Headache features
Location Quality Severity Time to peak Duration Constant or episodic Frequency Periodicity Onset
Associated neurologic symptoms
Preceding transient neurologic symptoms (aura)
Aggravating and alleviating factors
Pertinent Questions History of prior illness
Constitutional symptoms
Transient neurologic symptoms preceding associated or following the headache
Medicationssupplements (new medications or changes in medication regimen)
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
SNOOP4 secondary causes (Red Flags) Systemic symptomssigns fever chills night sweats myalgia weight loss (GCA meningoencephalitisabscess malignancy systemic infection)
Neurologic symptomssigns (focal or global including changes in behavior or personality diplopia transient visual obscurations pulsatile tinnitus numbness or weakness in facelimbs vertigo loss of balance)
Onset after age 50 Onset recent
Pattern change (if previous history of headache) 1 Progressive headache with loss of headache-free periods 2 Precipitated by Valsalva Chiari malformation structural lesions that obstruct CSF flow dural CSF leak Most headaches are worsened by Valsalva Certain primary headaches may be precipitated by Valsalva (primary cough headache) All headaches that are provoked by Valsalva require imaging to rule out secondary cause
3 Postural aggravation (worse standing or lying) intracranial hypotension (CSF leak) Chiari intracranial hypertension (CSF flow obstruction) worse with certain neck movementsposition (cervicogenic)
4 Papilledema Indicates intracranial hypertension Ask about transient visual obscurations diplopia and visual field defects
A 39-year old man presents to your office with the abrupt onset extremely severe diffuse headache nausea and blurred vision Headache began about 6 hours ago When asked he admits that this is the worst headache he has ever had He also reports some neck pain and says it feels stiff He has a history of migraine What would be the next course of action 1 Ketorolac im injection and antiemetic 2 Sumatriptan sc injection 3 Arrange for an urgent lumbar puncture 4 Obtain an urgent CT of the head without contrast 5 Start IV hydration with NS CT of the head is normal Next step LP does not show xanthochromia Next step CTA hn is normal Next step
Thunderclap Headache
Severe headache of abrupt onset (peaks within seconds)
No warning as a clap of thunder MUST BE EVALUATED in the Emergency Room
Causes of Thunderclap Headache SAH due to cerebral aneurysm or AVM rupture
Cervico-cerebral arterial dissection
Cerebral venous sinus thrombosis
Acute hypertensive crisis
Illicit drug use with secondary intracranial hemorrhage or infarction
Cerebral reversible vasoconstriction syndrome posterior reversible encephalopathy syndrome (PRES)
Pituitary apoplexy
Third ventricle colloid cyst
Spontaneous intracranial hypotension (CSF leak)
Ischemic or hemorrhagic stroke
Primary thunderclap headache (no underlying intracranial pathology after extensive workup)
Presenter
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
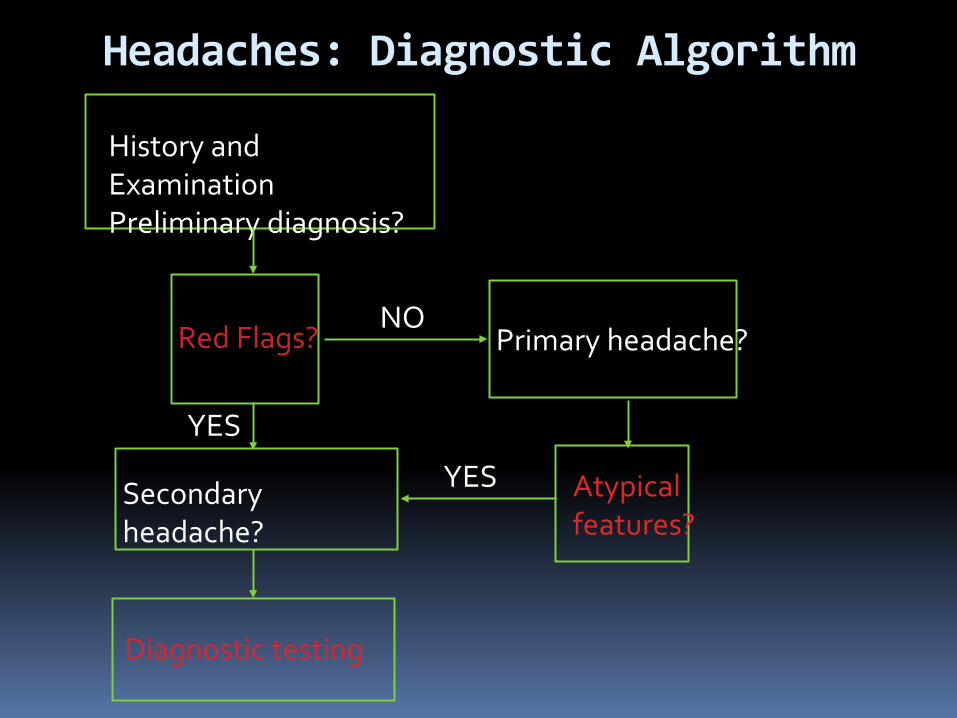
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flags Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
YES
Headache features HistoryReview of systems
Diagnostic Criteria Red Flags
Headache features
Location Quality Severity Time to peak Duration Constant or episodic Frequency Periodicity Onset
Associated neurologic symptoms
Preceding transient neurologic symptoms (aura)
Aggravating and alleviating factors
Pertinent Questions History of prior illness
Constitutional symptoms
Transient neurologic symptoms preceding associated or following the headache
Medicationssupplements (new medications or changes in medication regimen)
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
SNOOP4 secondary causes (Red Flags) Systemic symptomssigns fever chills night sweats myalgia weight loss (GCA meningoencephalitisabscess malignancy systemic infection)
Neurologic symptomssigns (focal or global including changes in behavior or personality diplopia transient visual obscurations pulsatile tinnitus numbness or weakness in facelimbs vertigo loss of balance)
Onset after age 50 Onset recent
Pattern change (if previous history of headache) 1 Progressive headache with loss of headache-free periods 2 Precipitated by Valsalva Chiari malformation structural lesions that obstruct CSF flow dural CSF leak Most headaches are worsened by Valsalva Certain primary headaches may be precipitated by Valsalva (primary cough headache) All headaches that are provoked by Valsalva require imaging to rule out secondary cause
3 Postural aggravation (worse standing or lying) intracranial hypotension (CSF leak) Chiari intracranial hypertension (CSF flow obstruction) worse with certain neck movementsposition (cervicogenic)
4 Papilledema Indicates intracranial hypertension Ask about transient visual obscurations diplopia and visual field defects
A 39-year old man presents to your office with the abrupt onset extremely severe diffuse headache nausea and blurred vision Headache began about 6 hours ago When asked he admits that this is the worst headache he has ever had He also reports some neck pain and says it feels stiff He has a history of migraine What would be the next course of action 1 Ketorolac im injection and antiemetic 2 Sumatriptan sc injection 3 Arrange for an urgent lumbar puncture 4 Obtain an urgent CT of the head without contrast 5 Start IV hydration with NS CT of the head is normal Next step LP does not show xanthochromia Next step CTA hn is normal Next step
Thunderclap Headache
Severe headache of abrupt onset (peaks within seconds)
No warning as a clap of thunder MUST BE EVALUATED in the Emergency Room
Causes of Thunderclap Headache SAH due to cerebral aneurysm or AVM rupture
Cervico-cerebral arterial dissection
Cerebral venous sinus thrombosis
Acute hypertensive crisis
Illicit drug use with secondary intracranial hemorrhage or infarction
Cerebral reversible vasoconstriction syndrome posterior reversible encephalopathy syndrome (PRES)
Pituitary apoplexy
Third ventricle colloid cyst
Spontaneous intracranial hypotension (CSF leak)
Ischemic or hemorrhagic stroke
Primary thunderclap headache (no underlying intracranial pathology after extensive workup)
Presenter
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Headache features HistoryReview of systems
Diagnostic Criteria Red Flags
Headache features
Location Quality Severity Time to peak Duration Constant or episodic Frequency Periodicity Onset
Associated neurologic symptoms
Preceding transient neurologic symptoms (aura)
Aggravating and alleviating factors
Pertinent Questions History of prior illness
Constitutional symptoms
Transient neurologic symptoms preceding associated or following the headache
Medicationssupplements (new medications or changes in medication regimen)
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
SNOOP4 secondary causes (Red Flags) Systemic symptomssigns fever chills night sweats myalgia weight loss (GCA meningoencephalitisabscess malignancy systemic infection)
Neurologic symptomssigns (focal or global including changes in behavior or personality diplopia transient visual obscurations pulsatile tinnitus numbness or weakness in facelimbs vertigo loss of balance)
Onset after age 50 Onset recent
Pattern change (if previous history of headache) 1 Progressive headache with loss of headache-free periods 2 Precipitated by Valsalva Chiari malformation structural lesions that obstruct CSF flow dural CSF leak Most headaches are worsened by Valsalva Certain primary headaches may be precipitated by Valsalva (primary cough headache) All headaches that are provoked by Valsalva require imaging to rule out secondary cause
3 Postural aggravation (worse standing or lying) intracranial hypotension (CSF leak) Chiari intracranial hypertension (CSF flow obstruction) worse with certain neck movementsposition (cervicogenic)
4 Papilledema Indicates intracranial hypertension Ask about transient visual obscurations diplopia and visual field defects
A 39-year old man presents to your office with the abrupt onset extremely severe diffuse headache nausea and blurred vision Headache began about 6 hours ago When asked he admits that this is the worst headache he has ever had He also reports some neck pain and says it feels stiff He has a history of migraine What would be the next course of action 1 Ketorolac im injection and antiemetic 2 Sumatriptan sc injection 3 Arrange for an urgent lumbar puncture 4 Obtain an urgent CT of the head without contrast 5 Start IV hydration with NS CT of the head is normal Next step LP does not show xanthochromia Next step CTA hn is normal Next step
Thunderclap Headache
Severe headache of abrupt onset (peaks within seconds)
No warning as a clap of thunder MUST BE EVALUATED in the Emergency Room
Causes of Thunderclap Headache SAH due to cerebral aneurysm or AVM rupture
Cervico-cerebral arterial dissection
Cerebral venous sinus thrombosis
Acute hypertensive crisis
Illicit drug use with secondary intracranial hemorrhage or infarction
Cerebral reversible vasoconstriction syndrome posterior reversible encephalopathy syndrome (PRES)
Pituitary apoplexy
Third ventricle colloid cyst
Spontaneous intracranial hypotension (CSF leak)
Ischemic or hemorrhagic stroke
Primary thunderclap headache (no underlying intracranial pathology after extensive workup)
Presenter
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Headache features
Location Quality Severity Time to peak Duration Constant or episodic Frequency Periodicity Onset
Associated neurologic symptoms
Preceding transient neurologic symptoms (aura)
Aggravating and alleviating factors
Pertinent Questions History of prior illness
Constitutional symptoms
Transient neurologic symptoms preceding associated or following the headache
Medicationssupplements (new medications or changes in medication regimen)
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
SNOOP4 secondary causes (Red Flags) Systemic symptomssigns fever chills night sweats myalgia weight loss (GCA meningoencephalitisabscess malignancy systemic infection)
Neurologic symptomssigns (focal or global including changes in behavior or personality diplopia transient visual obscurations pulsatile tinnitus numbness or weakness in facelimbs vertigo loss of balance)
Onset after age 50 Onset recent
Pattern change (if previous history of headache) 1 Progressive headache with loss of headache-free periods 2 Precipitated by Valsalva Chiari malformation structural lesions that obstruct CSF flow dural CSF leak Most headaches are worsened by Valsalva Certain primary headaches may be precipitated by Valsalva (primary cough headache) All headaches that are provoked by Valsalva require imaging to rule out secondary cause
3 Postural aggravation (worse standing or lying) intracranial hypotension (CSF leak) Chiari intracranial hypertension (CSF flow obstruction) worse with certain neck movementsposition (cervicogenic)
4 Papilledema Indicates intracranial hypertension Ask about transient visual obscurations diplopia and visual field defects
A 39-year old man presents to your office with the abrupt onset extremely severe diffuse headache nausea and blurred vision Headache began about 6 hours ago When asked he admits that this is the worst headache he has ever had He also reports some neck pain and says it feels stiff He has a history of migraine What would be the next course of action 1 Ketorolac im injection and antiemetic 2 Sumatriptan sc injection 3 Arrange for an urgent lumbar puncture 4 Obtain an urgent CT of the head without contrast 5 Start IV hydration with NS CT of the head is normal Next step LP does not show xanthochromia Next step CTA hn is normal Next step
Thunderclap Headache
Severe headache of abrupt onset (peaks within seconds)
No warning as a clap of thunder MUST BE EVALUATED in the Emergency Room
Causes of Thunderclap Headache SAH due to cerebral aneurysm or AVM rupture
Cervico-cerebral arterial dissection
Cerebral venous sinus thrombosis
Acute hypertensive crisis
Illicit drug use with secondary intracranial hemorrhage or infarction
Cerebral reversible vasoconstriction syndrome posterior reversible encephalopathy syndrome (PRES)
Pituitary apoplexy
Third ventricle colloid cyst
Spontaneous intracranial hypotension (CSF leak)
Ischemic or hemorrhagic stroke
Primary thunderclap headache (no underlying intracranial pathology after extensive workup)
Presenter
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Pertinent Questions History of prior illness
Constitutional symptoms
Transient neurologic symptoms preceding associated or following the headache
Medicationssupplements (new medications or changes in medication regimen)
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
SNOOP4 secondary causes (Red Flags) Systemic symptomssigns fever chills night sweats myalgia weight loss (GCA meningoencephalitisabscess malignancy systemic infection)
Neurologic symptomssigns (focal or global including changes in behavior or personality diplopia transient visual obscurations pulsatile tinnitus numbness or weakness in facelimbs vertigo loss of balance)
Onset after age 50 Onset recent
Pattern change (if previous history of headache) 1 Progressive headache with loss of headache-free periods 2 Precipitated by Valsalva Chiari malformation structural lesions that obstruct CSF flow dural CSF leak Most headaches are worsened by Valsalva Certain primary headaches may be precipitated by Valsalva (primary cough headache) All headaches that are provoked by Valsalva require imaging to rule out secondary cause
3 Postural aggravation (worse standing or lying) intracranial hypotension (CSF leak) Chiari intracranial hypertension (CSF flow obstruction) worse with certain neck movementsposition (cervicogenic)
4 Papilledema Indicates intracranial hypertension Ask about transient visual obscurations diplopia and visual field defects
A 39-year old man presents to your office with the abrupt onset extremely severe diffuse headache nausea and blurred vision Headache began about 6 hours ago When asked he admits that this is the worst headache he has ever had He also reports some neck pain and says it feels stiff He has a history of migraine What would be the next course of action 1 Ketorolac im injection and antiemetic 2 Sumatriptan sc injection 3 Arrange for an urgent lumbar puncture 4 Obtain an urgent CT of the head without contrast 5 Start IV hydration with NS CT of the head is normal Next step LP does not show xanthochromia Next step CTA hn is normal Next step
Thunderclap Headache
Severe headache of abrupt onset (peaks within seconds)
No warning as a clap of thunder MUST BE EVALUATED in the Emergency Room
Causes of Thunderclap Headache SAH due to cerebral aneurysm or AVM rupture
Cervico-cerebral arterial dissection
Cerebral venous sinus thrombosis
Acute hypertensive crisis
Illicit drug use with secondary intracranial hemorrhage or infarction
Cerebral reversible vasoconstriction syndrome posterior reversible encephalopathy syndrome (PRES)
Pituitary apoplexy
Third ventricle colloid cyst
Spontaneous intracranial hypotension (CSF leak)
Ischemic or hemorrhagic stroke
Primary thunderclap headache (no underlying intracranial pathology after extensive workup)
Presenter
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
SNOOP4 secondary causes (Red Flags) Systemic symptomssigns fever chills night sweats myalgia weight loss (GCA meningoencephalitisabscess malignancy systemic infection)
Neurologic symptomssigns (focal or global including changes in behavior or personality diplopia transient visual obscurations pulsatile tinnitus numbness or weakness in facelimbs vertigo loss of balance)
Onset after age 50 Onset recent
Pattern change (if previous history of headache) 1 Progressive headache with loss of headache-free periods 2 Precipitated by Valsalva Chiari malformation structural lesions that obstruct CSF flow dural CSF leak Most headaches are worsened by Valsalva Certain primary headaches may be precipitated by Valsalva (primary cough headache) All headaches that are provoked by Valsalva require imaging to rule out secondary cause
3 Postural aggravation (worse standing or lying) intracranial hypotension (CSF leak) Chiari intracranial hypertension (CSF flow obstruction) worse with certain neck movementsposition (cervicogenic)
4 Papilledema Indicates intracranial hypertension Ask about transient visual obscurations diplopia and visual field defects
A 39-year old man presents to your office with the abrupt onset extremely severe diffuse headache nausea and blurred vision Headache began about 6 hours ago When asked he admits that this is the worst headache he has ever had He also reports some neck pain and says it feels stiff He has a history of migraine What would be the next course of action 1 Ketorolac im injection and antiemetic 2 Sumatriptan sc injection 3 Arrange for an urgent lumbar puncture 4 Obtain an urgent CT of the head without contrast 5 Start IV hydration with NS CT of the head is normal Next step LP does not show xanthochromia Next step CTA hn is normal Next step
Thunderclap Headache
Severe headache of abrupt onset (peaks within seconds)
No warning as a clap of thunder MUST BE EVALUATED in the Emergency Room
Causes of Thunderclap Headache SAH due to cerebral aneurysm or AVM rupture
Cervico-cerebral arterial dissection
Cerebral venous sinus thrombosis
Acute hypertensive crisis
Illicit drug use with secondary intracranial hemorrhage or infarction
Cerebral reversible vasoconstriction syndrome posterior reversible encephalopathy syndrome (PRES)
Pituitary apoplexy
Third ventricle colloid cyst
Spontaneous intracranial hypotension (CSF leak)
Ischemic or hemorrhagic stroke
Primary thunderclap headache (no underlying intracranial pathology after extensive workup)
Presenter
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
A 39-year old man presents to your office with the abrupt onset extremely severe diffuse headache nausea and blurred vision Headache began about 6 hours ago When asked he admits that this is the worst headache he has ever had He also reports some neck pain and says it feels stiff He has a history of migraine What would be the next course of action 1 Ketorolac im injection and antiemetic 2 Sumatriptan sc injection 3 Arrange for an urgent lumbar puncture 4 Obtain an urgent CT of the head without contrast 5 Start IV hydration with NS CT of the head is normal Next step LP does not show xanthochromia Next step CTA hn is normal Next step
Thunderclap Headache
Severe headache of abrupt onset (peaks within seconds)
No warning as a clap of thunder MUST BE EVALUATED in the Emergency Room
Causes of Thunderclap Headache SAH due to cerebral aneurysm or AVM rupture
Cervico-cerebral arterial dissection
Cerebral venous sinus thrombosis
Acute hypertensive crisis
Illicit drug use with secondary intracranial hemorrhage or infarction
Cerebral reversible vasoconstriction syndrome posterior reversible encephalopathy syndrome (PRES)
Pituitary apoplexy
Third ventricle colloid cyst
Spontaneous intracranial hypotension (CSF leak)
Ischemic or hemorrhagic stroke
Primary thunderclap headache (no underlying intracranial pathology after extensive workup)
Presenter
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Thunderclap Headache
Severe headache of abrupt onset (peaks within seconds)
No warning as a clap of thunder MUST BE EVALUATED in the Emergency Room
Causes of Thunderclap Headache SAH due to cerebral aneurysm or AVM rupture
Cervico-cerebral arterial dissection
Cerebral venous sinus thrombosis
Acute hypertensive crisis
Illicit drug use with secondary intracranial hemorrhage or infarction
Cerebral reversible vasoconstriction syndrome posterior reversible encephalopathy syndrome (PRES)
Pituitary apoplexy
Third ventricle colloid cyst
Spontaneous intracranial hypotension (CSF leak)
Ischemic or hemorrhagic stroke
Primary thunderclap headache (no underlying intracranial pathology after extensive workup)
Presenter
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Causes of Thunderclap Headache SAH due to cerebral aneurysm or AVM rupture
Cervico-cerebral arterial dissection
Cerebral venous sinus thrombosis
Acute hypertensive crisis
Illicit drug use with secondary intracranial hemorrhage or infarction
Cerebral reversible vasoconstriction syndrome posterior reversible encephalopathy syndrome (PRES)
Pituitary apoplexy
Third ventricle colloid cyst
Spontaneous intracranial hypotension (CSF leak)
Ischemic or hemorrhagic stroke
Primary thunderclap headache (no underlying intracranial pathology after extensive workup)
Presenter
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
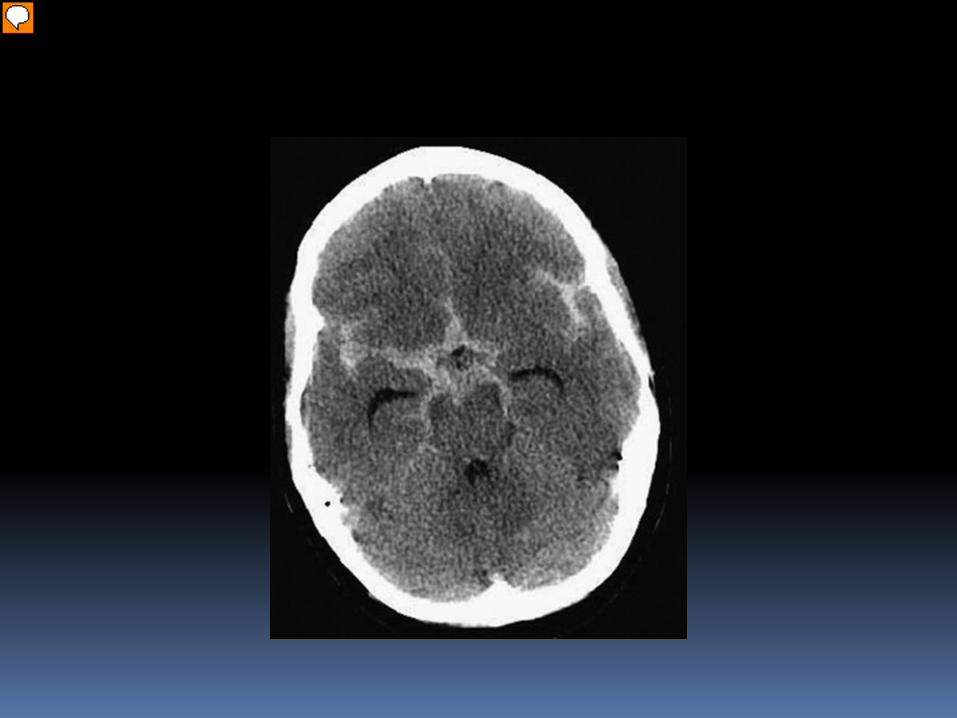
Presentation Notes
SAH
Presenter
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
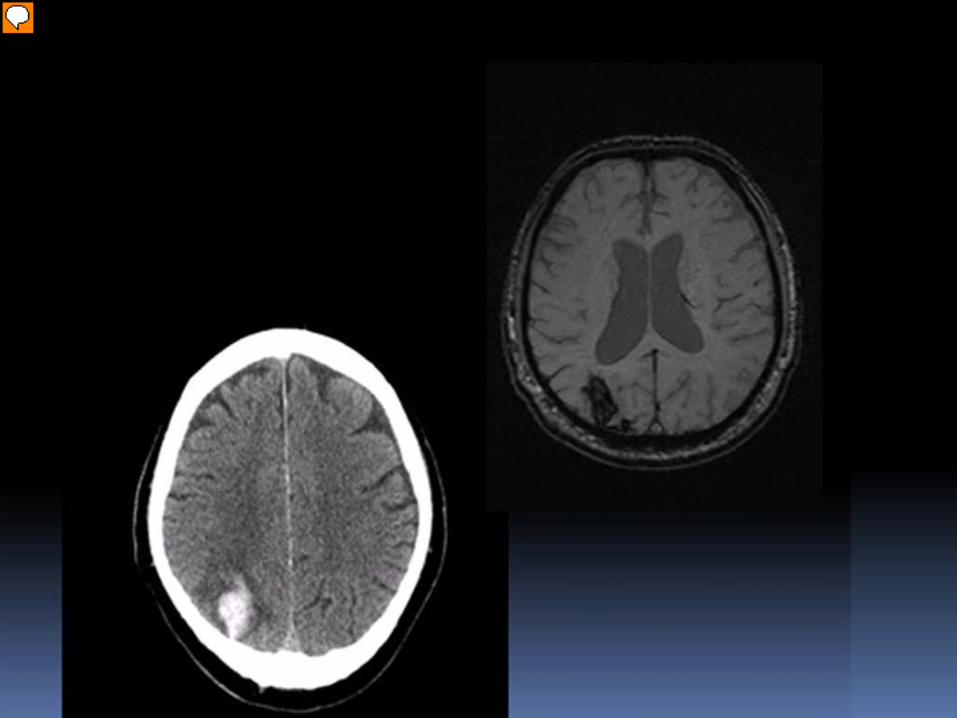
Presentation Notes
Lobar ICH---Cerebral amyloid angiopathy
Presenter
Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-

Presentation Notes
Cerebral venous thrombosis
Presenter
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
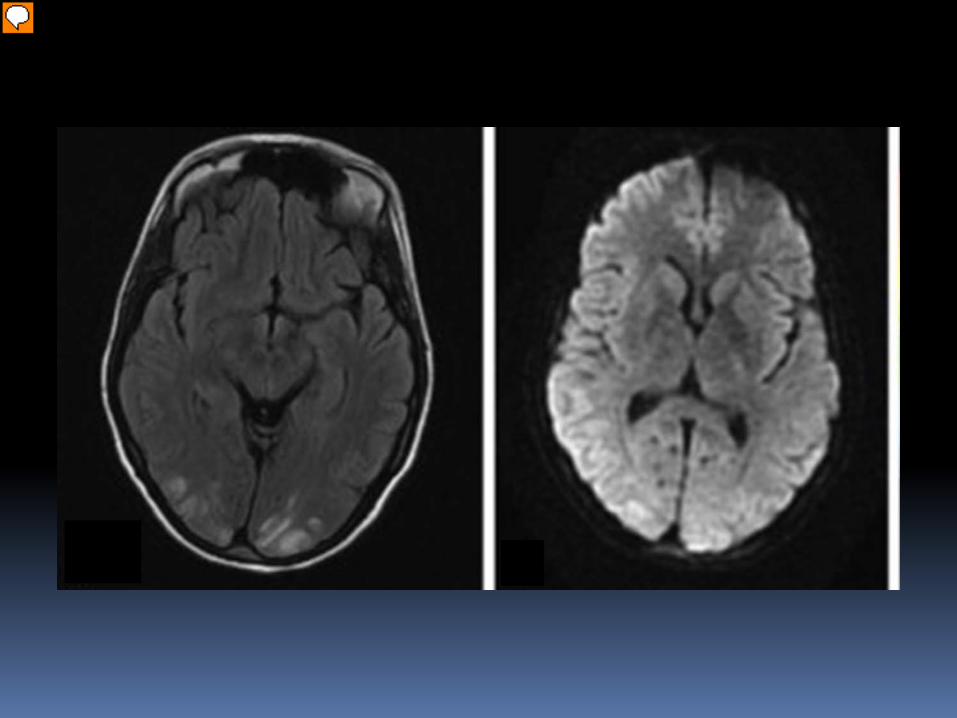
Presentation Notes
Hypertensive encephalopathyPRES
Presenter
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
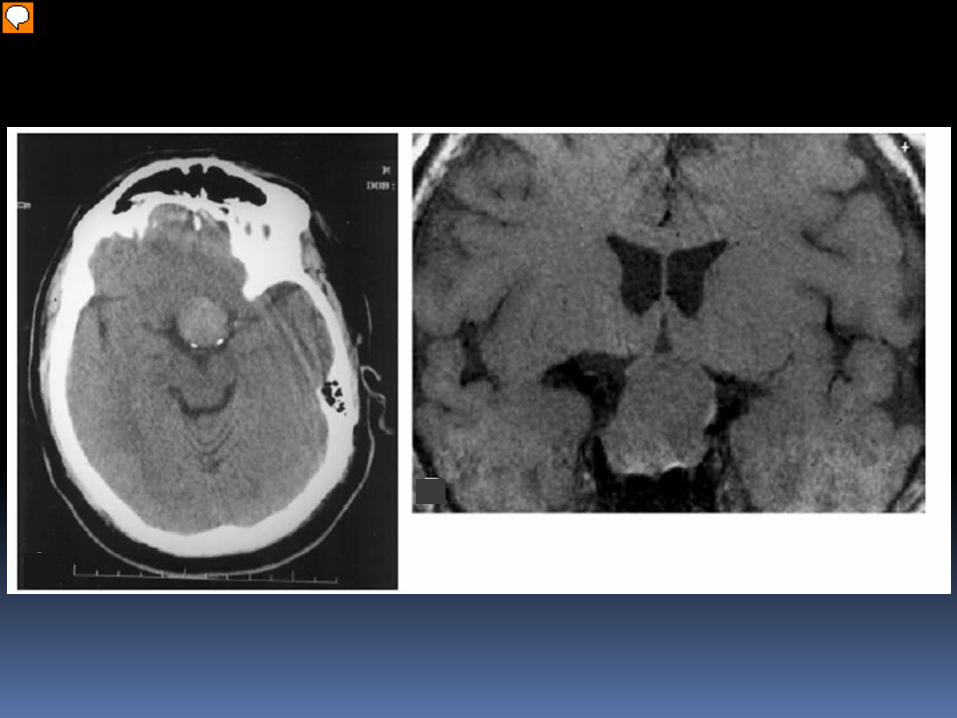
Presentation Notes
Pituitary apoplexy
Presenter
Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-

Presentation Notes
Chiari I
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Primary Headaches
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Primary Headaches 1 Migraine 2 Tension-type headache 3 Trigeminal autonomic cephalalgia (TAC) - Cluster headache - Paroxysmal hemicrania - SUNCTSUNA 4 Other primary headaches - New Daily Persistent Headache - Hemicrania continua - Primary cough headache - Primary exertional headache - Headache associated with sexual activity - Primary stabbing headache - Hypnic headache
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
An overweight 36-year-old woman presents with 3-4 severe debilitating headaches per month for the last 2 years The headaches last 1 to 2 days They are sometimes localized bifrontally but more often localized to the right temple right frontal region and behind the right eye There is often bilateral rhinorrhea and congestion associated with her headaches and sense of pressure over the bridge the nose and sides of the nose The pain is usually throbbing but may be pressure-like when not very severe She has to wear sunglasses and go to a quiet place and lay down because ldquoshe canrsquot functionrdquo She denies any prodrome or auras What is the most likely diagnosis 1 Cluster headache 2 Sinus headache 3 Tension-type headache 4 Episodic migraine 5 Idiopathic intracranial hypertension (pseudotumor cerebri)
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Migraine
95 of patients presenting in clinical practice with headache have migraine
Clinical diagnosis
Young age of onset by age of 40 yo 90 of patients with migraine have had their first attack
Positive family history (70 have first degree relative with migraine)
Prevalence 12 in general population
WomenMen 31
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
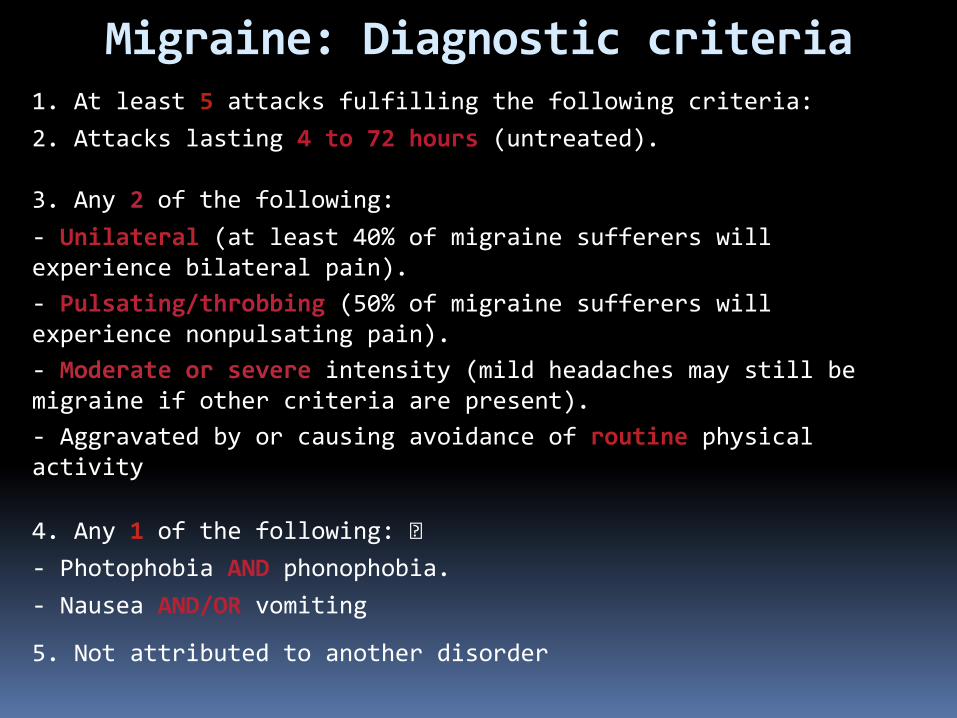
Migraine Diagnostic criteria 1 At least 5 attacks fulfilling the following criteria 2 Attacks lasting 4 to 72 hours (untreated) 3 Any 2 of the following - Unilateral (at least 40 of migraine sufferers will experience bilateral pain) - Pulsatingthrobbing (50 of migraine sufferers will experience nonpulsating pain) - Moderate or severe intensity (mild headaches may still be migraine if other criteria are present) - Aggravated by or causing avoidance of routine physical activity 4 Any 1 of the following 11130881113088 - Photophobia AND phonophobia - Nausea ANDOR vomiting 5 Not attributed to another disorder
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
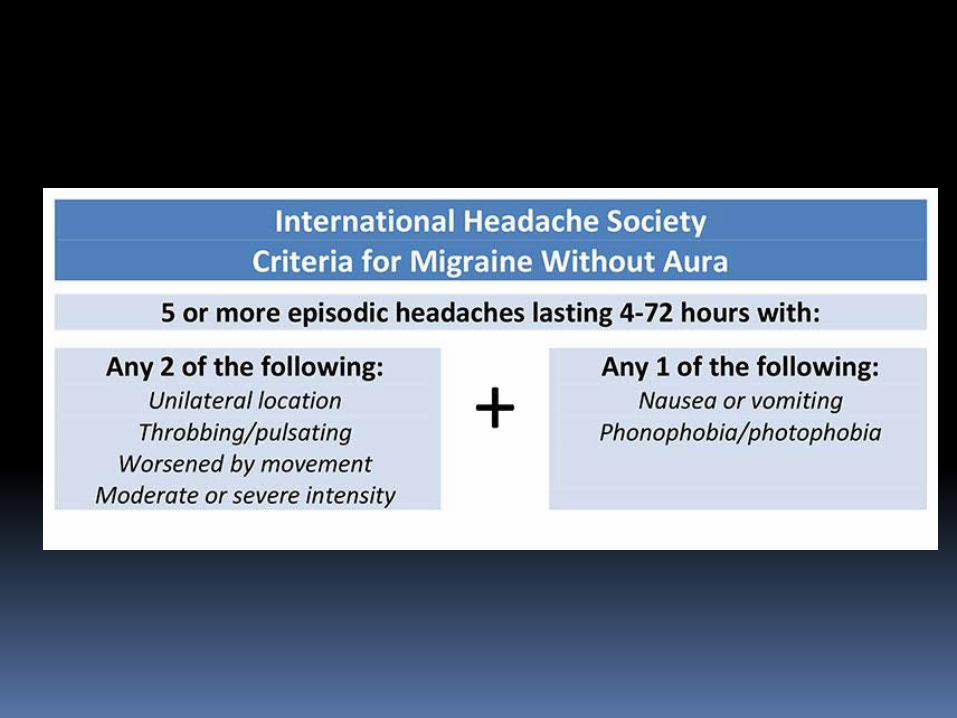
probable migraine (ldquomigrainous headacherdquo)
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Migraine headache May switch sides and may become bilateraldiffuse
Prodrome (up to 3 days prior to attack) mood changes decreased energy yawning thirst food craving
Pain builds up over 30 min to 2 hrs to peak
Cutaneous allodynia develops in most patients during migraine attack
Presenter
Presentation Notes
May throb on valsalva or movement or head low position
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Migraine with Aura Aura transient visual sensory or language disturbance or other focal brainstem or cerebral symptoms that precede or accompany the headache
Aura occurs in 25 of migraine patients
Does not occur with each attack
Duration of aura 5 to 30 minutes
Migraine equivalent = acephalgic migraine = migraine aura without headache
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for about 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She denies any other symptoms such as general weaknessfatigue fevers chills weight loss joint pain rash Diagnosis 1 Migraine with visual aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Aura of migraine diagnostic criteria
At least 2 attacks Aura consisting of at least one of the following but no motor weakness
1 Fully reversible VISUAL symptoms (including positive andor negative features) 2 Fully reversible SENSORY symptoms (including positive andor negative symptoms) 3 Fully reversible DYSPHASIC speech disturbance
Migraine with MOTOR deficit is classified as hemiplegic migraine Migraine with BRAINSTEM SYMPTOMS is classified as basilar-type migraine Duration of typical aura 5 to 30 minutes (lt60 min)
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
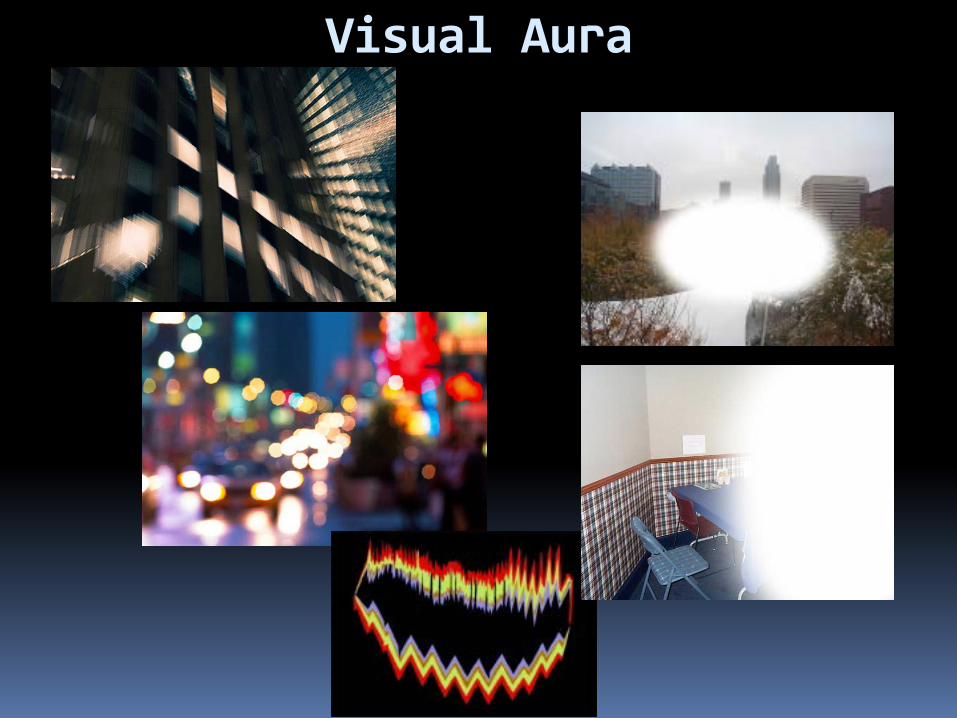
Visual Aura
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Sensory Aura
Sensory auras may spread in 10-20 min from where they started to maximal distribution
Slower than sensory seizure spread
Much slower than TIA sensory symptoms spread
Latent period of few minutes between aura and headache development
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
A 65-year-old woman went on a roller coaster ride One day later she began having left-sided retro-orbital daily intermittent throbbing headache lasting from several minutes to several hours There was no associated sensitivity to light or sound and no nausea or vomiting The headache has continued for 3 weeks on-and-off and today she had what sounds like amaurosis fugax in the left eye (ldquocurtain going downrdquo for 10 seconds) She had rare migraine headaches in her 30rsquos-40rsquos She feels weak ldquoall overrdquo and states that her shoulders have been hurting for at least 6 months On directed questioning she endorses to getting tired of chewing and her jaw hurts On examination left temporal scalp area is exquisitely sensitive to touch Initial brain imaging and vascular imaging has been unremarkable Diagnosis 1 Migraine with aura status migrainosus 2 Temporal arteritis 3 Internal carotid artery dissection 4 Glaucoma
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Migraine Management Education and counseling reduces anxiety and improves adherence to pharmacologic treatment
Migraine diary Trigger avoidance (food odors) and dietary changes (elimination diets should be avoided)
Good hydration Sleep hygiene (weekend headaches) Regular meals and avoidance of fasting Reducing caffeine alcohol smoking cessation Medication review and changes Regular exercise Stress reduction and coping techniques biofeedback relaxation training hypnosis cognitive and behavioral training
bull nitrates bull hydralazine bull cialisviagra bull beta-agonists bull stimulants bull dopamine agonists bull estrogen
Presenter
Presentation Notes
Some medications can cause headaches (reserpine nifidipine and other vasodilators theophylline derivative oral contraceptives PPIs
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Potential Food Triggers Some association of certain food items with migraine
Nitrites (hotdogs preserved cold cuts) Monosodium glutamate (canned food Chinese food)
Aspartam (artificial sweetener) Aged cheeses fermented food red wine Chicken liver pork Chocolate Sweets nuts dairy citrus fruits
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Pharmacologic treatment
Abortive
Prophylactic
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
A 34-year-old overweight woman present with a severe migraine headache that began 2 days ago but is now nearly gone She has not identified any triggers since these headaches began 2 years ago She has tried to avoid stress and kept a headache diary prior to a visit with you today She averages about 5 migraines per month each lasting up to 1-2 days What is the best choice of treatment at this time assuming there are no contraindications 1 Prescribe sumatriptan and a NSAID to take immediately today to stop her resolving headache 2 Prescribe preventive agent 3 Give IV dihydroergotamine (DHE) infusion today in the office 4 Follow her over the next couple of months before prescribing anything 5 Prescribe sumatriptan to use as needed as well as preventive agent
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Abortive migraine treatment as early as possibleat onset of aura
Simple analgesics bullAspirin bullNSAIDs bullAcetaminophen bullAnalgesic combination with caffeine (avoid using gt 2week)
Triptans bullAgonists at specific 5-HT receptors bull5HT1B agonists promote vasoconstriction bull5HT1D agonists block release of neuropeptides from perivascular trigeminal afferents
Dihydroergotamine (DHE) for prolonged migraine attackstatus migrainosus
Triptans DHE contraindicated in CAD cerebrovascular disease peripheral vascular disease caution in hypertension
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
The patient depicted in previous case returns 1 week later She is now in prolonged severe headache phase that began 4 days ago She has missed 2 days of work Her last triptan dose was 1 day ago As you examine her head you find that her right temporal and right frontal regions are exquisitely sensitive to touch What is the best choice of treatment at this point assuming there are no contraindications 1 Increase her preventive medication dose and have her take another triptan 2 Change her preventive agent because it does not appear to be working 3 Give IV dihydroergotamine (DHE) infusion 4 Change her triptan and have her take one now 5 Proceed with CT of the head without contrast to investigate the dysesthesia found on examination
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
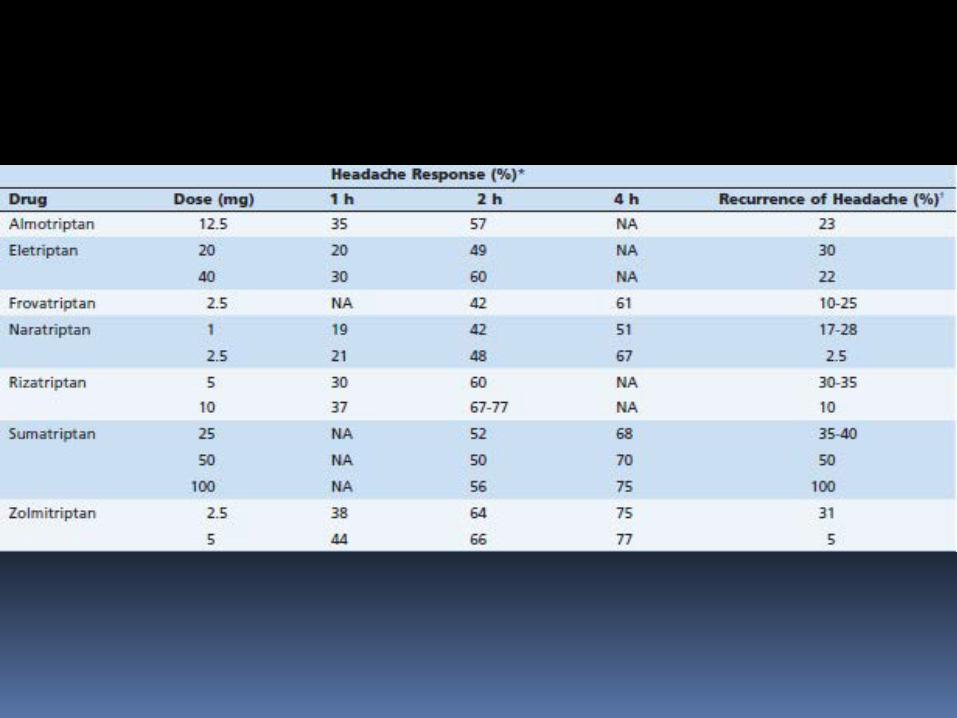
During the office visit a 46-year-old man with a longstanding history of recurrent headaches is diagnosed for the first time with migraine He has a history of anxiety hypertension hyperlipidemia smoking and is noncompliant with medications Family history is significant for his mother having migraine and his father dying from a ldquoheart attackrdquo in his mid fifties If this patient presented to the emergency department at the very onset of a migraine what would be the least optimal choice of treatment 1 Sumatriptan 2 Ketorolac 3 Valproic acid 4 Prochrolperazine 5 IV magnesium
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Preventiveprophylactic treatment
Consider prophylactic treatment if
bull frequency of headaches gt 2 per month
bull frequency and duration of migraines interfere with life style
bull headache duration gt 24 hours
bull severe prolonged headaches not responsive to abortive medications intolerance of abortive medications contraindications to abortive medications
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Preventive Treatment Medication selection based on patientrsquos characteristics
comorbidities and side effect profile of the medications
Medications do not exert their effect for at least 2 weeks most of the time - not sooner than 2 months
Doses known to be therapeutic should be reached before failure is considered
Ongoing frequent use of analgesics impedes onset of benefit from preventive medication
Multiple agents may be necessary
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Preventive Treatment Beta-blockers propranolol 80-240 mgday
Tricyclic antidepressants amitriptyline (75 mg qhs) nortriptyline desipramine imipramine
Selective serotonin reuptake inhibitors bull Not consistently proven beneficial bull May cause headaches
Anticonvulsants topiramate valproate
CCB verapamil 80-160 mg tid or ER qd Useful in migraine with aura
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Comorbid Condition Medication
Hypertension Beta blockers CCB ACE inhibitor ARB (candesartan)
Angina Beta blockers
Stress anxiety Beta blockers
Depression Tricyclic antidepressants SSRIs
Overweight Topiramate
Underweight Tricyclic antidepressants
Epilepsy Valproic acid topiramate
Bipolar disorderMania Valproic acid
Prophylactic medication selection
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
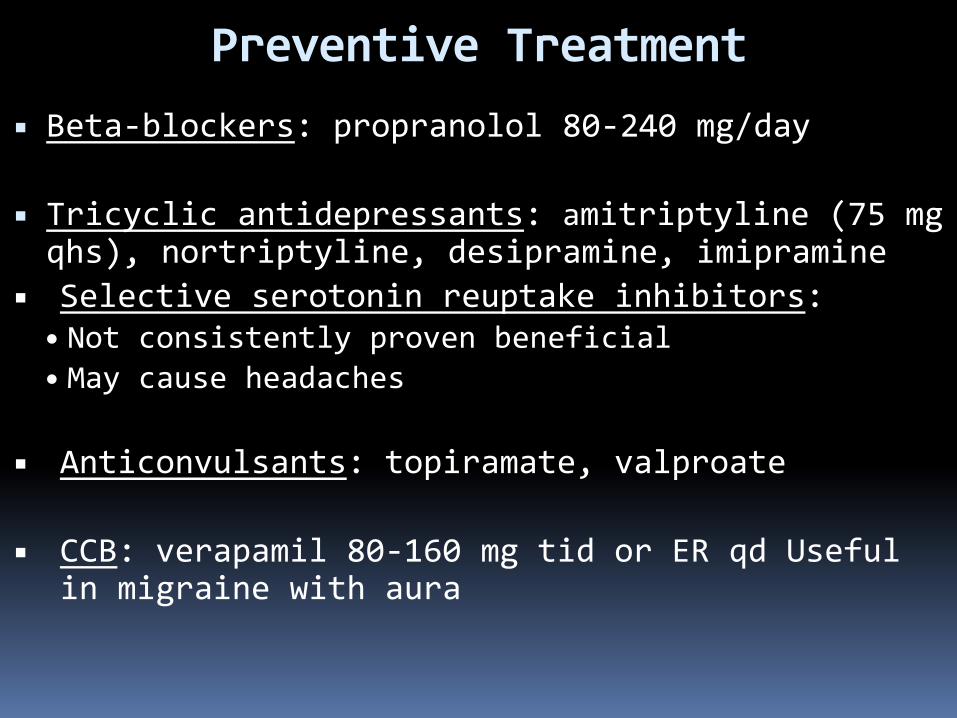
A 22-year-old mildly overweight woman presents to the emergency department with increasing frequency of previously diagnosed migraine Other medical history is unremarkable with exception of mild asthma and recurrent constipation The attacks are occurring 4 days per week and are lasting the entire day What would be the best preventive medication to start in this patient 1 Amitriptyline 2 Propranolol 3 Sumatriptan 4 Topiramate 5 Verapamil
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
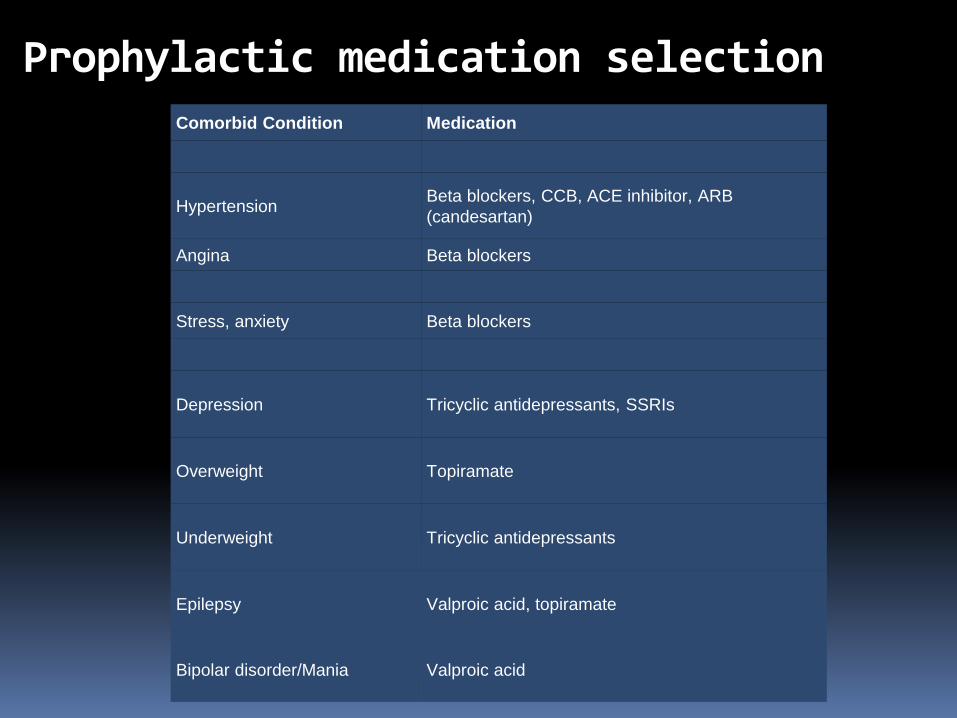
Botulinum toxin type A Proven efficacy in chronic migraine
Reduces proinflammatory and vasodilating neuropeptides from nociceptive terminals
Reduces or inhibits development of peripheral and central trigeminal sensitization
5 Units in forehead temporalis splenius capitis trapezius muscles into 31 injection sites
Effect starts after 7-10 days and lasts 3 months
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
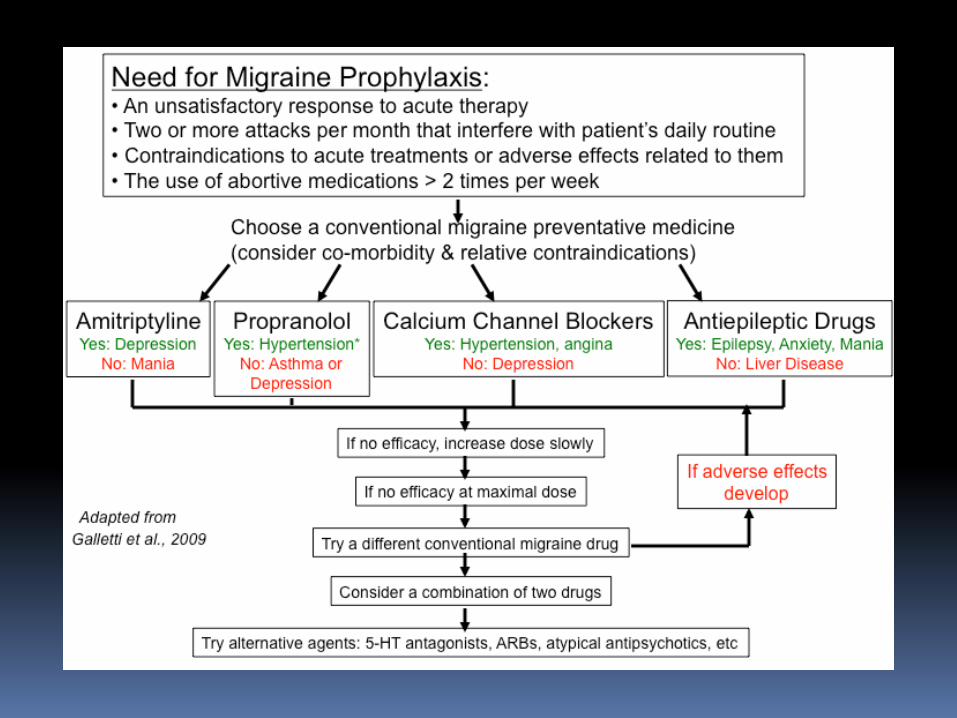
Butterbur extract (Petadolex)
DO NOT use parts of plant use only commercially available preparation (Petadolex)
mdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdashmdash Monitoring liver enzymes is recommended
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
A 38-year-old woman complains of frequent headaches for the past 2-3 years The pain is located in bilateral fronto-temporal areas described as pressure-like band-like tightness There is no associated sensitivity to light or sound No associated nausea or vomiting Headache is not positional The pain is not aggravated by routine physical activity and she is able to continue with her daily routine with these headaches Headaches last from several hours to several days and respond fairly well to over-the-counter analgesics She has had up to 10 headache-days per month for the past several months She denies any other symptoms such as vision changes double vision tinnitus vertigo Her general and neurologic examination is normal except tenderness of pericranial muscles to palpation Diagnosis Treatment 1 Migraine 2 Sinus headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Psychogenic headache
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
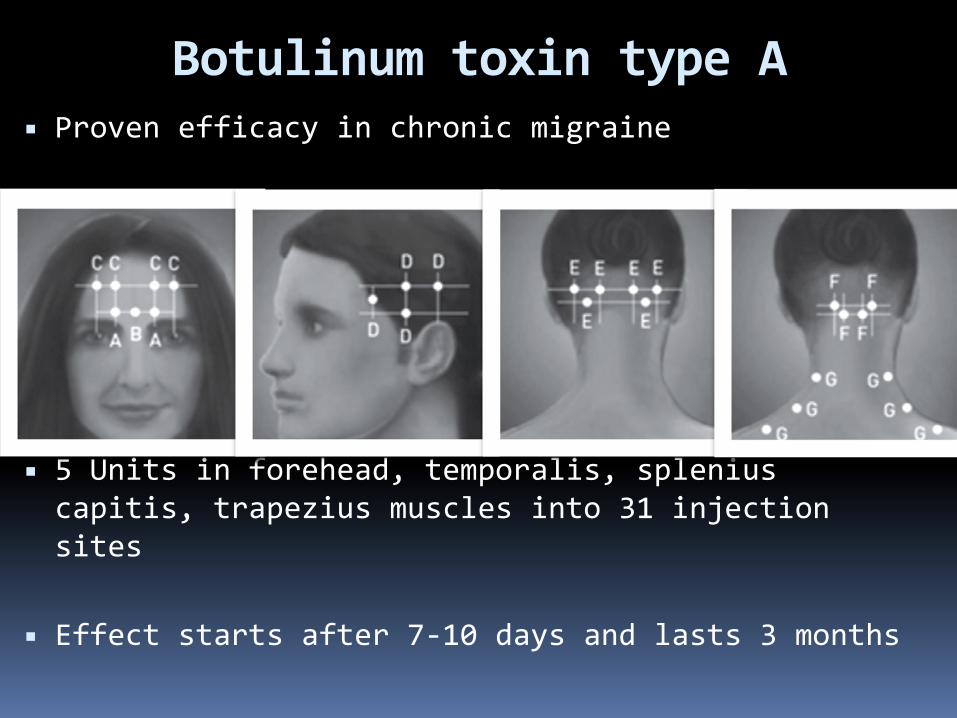
Tension Type Headache Prevalence 30-78
Can begin at any age
Bilateral generalized or band-like pressure around the head
Frequency episodic or chronic (gt 15 days a month for more than 3 months)
With and without pericranial muscle involvement
Persistent contraction of the scalp neck jaw muscles related to central mechanism
Cranio-cervical muscle tenderness
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Tension type headache Diagnostic criteria
ldquoNOT A MIGRAINErdquo bull Not unilateral bull Not throbbing or pulsating bull Not severe but mild to moderate bull Not aggravatedprovoked by routine
physical activity bull No photo- AND phonophobia bull No nausea or vomiting
+ bull No other explanation
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Tension type headache Treatment
Techniques of relaxation (biofeedback) neck massage
Medications 1 Abortive bull acetaminophen+isometheptene+dichloralphenazone bull avoid codeine propoxyphene butalbital with caffeine (high potential to cause medication overuse headache)
2 Preventive bull amitriptyline is the best choice bull other TCAs gabapentin mirtazapine topiramate
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
A 46-year-old man presents with episodic headaches His headaches are described as severe attacks of unilateral pain lasting 15-40 minutes and associated with ipsilateral droopy eyelid tearing redness of the eye and nasal congestion He has 1-3 attacks daily or every other day Some attacks occur during the night waking him up from sleep typically at 2 am He is agitated and restless during the headache and cannot stay still The attacks occur in bouts lasting for several weeks up to 4 months then remit for several months then return He has had these headaches for 2 years Neurologic examination is normal He was told that during the attacks his pupil on the side of the headache is smaller compared to the other pupil Diagnosis 1 Migraine 2 Hemicrania continua 3 Pseudutumor cerebri 4 Cluster headache 5 Glaucoma
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
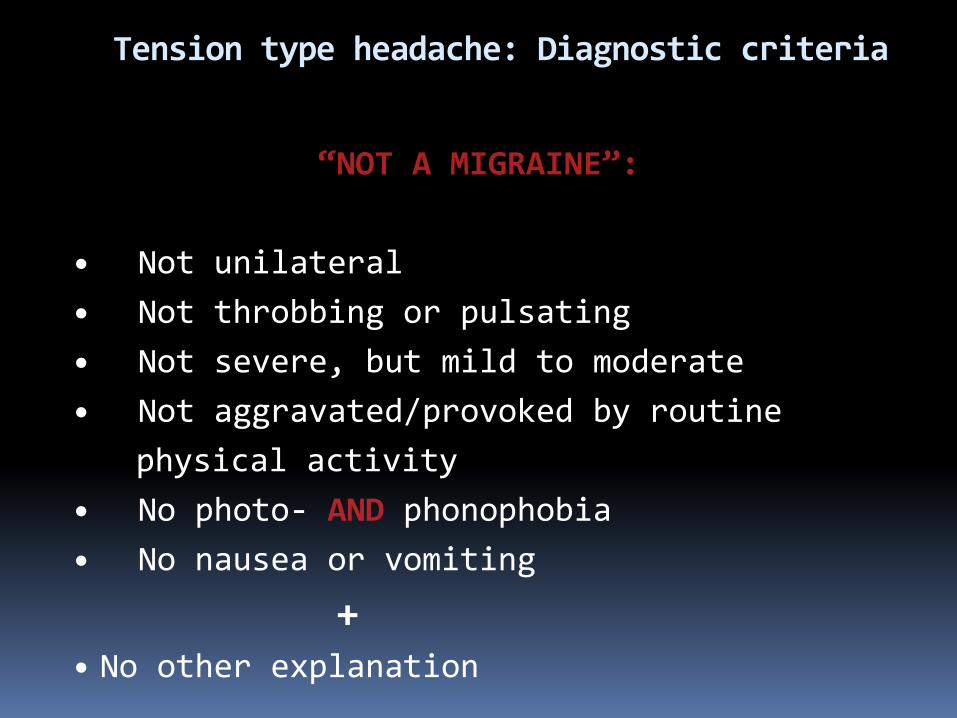
Trigeminal Autonomic Cephalalgias (TACs) 1Cluster headache
2Paroxysmal hemicrania 3SUNCTSUNA
Common features
bull pain location in the distribution of trigeminal nerve V1 bull strictly unilateral bull unilateral ipsilateral cranial autonomic associated symptoms bull periodicity bull need to rule out secondary causes pituitary hypothalamic cavernous sinus trigeminal nerve pathologic process Distinguishing features
bull attack duration (longest in cluster headache shortest in SUNCT) and number of attacks a day (highest in SUNCTSUNA)
bull unique response to medications (abortive and preventive)
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
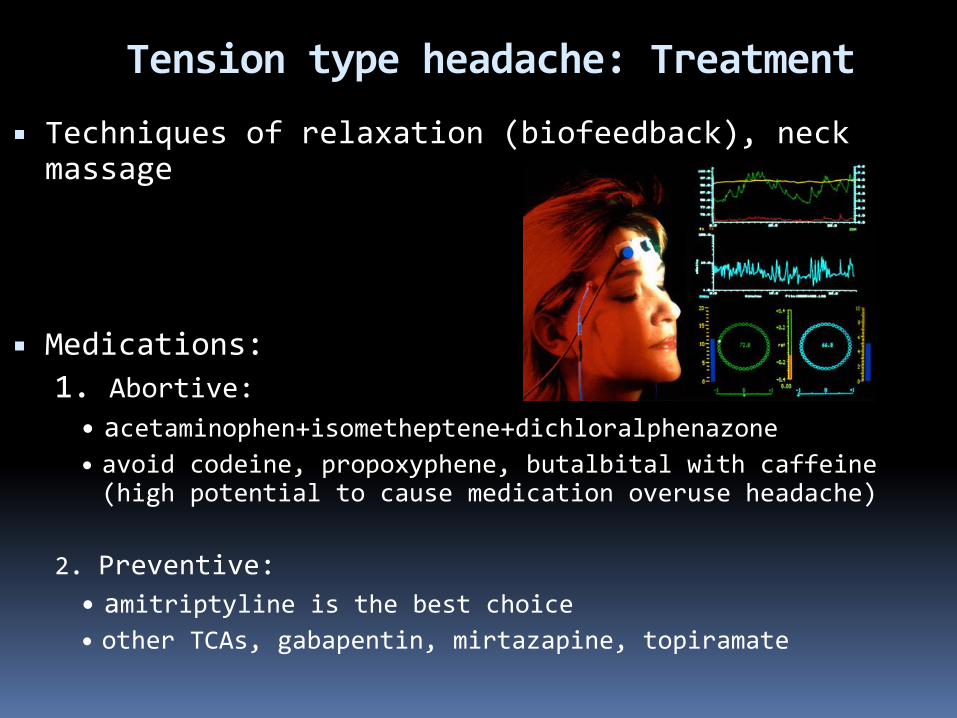
Cluster Headache
Prevalence 12000 Men gtgt women (431) Onset in 3rd decade of life Most painful recurrent headache (ldquosuicide headache) Unilateral orbitaltemporalsupraorbital Throbbing ldquohot poker in the eyerdquo ldquoeye being pushed outrdquo Rapid buildup of pain over 5-10 min Attack duration 15 min-3 hrs Restless patient and prefers to pace 1-8 attacks a day onset during night or few hours after falling asleep (ldquoalarmrdquo headache)
Daily or eod attacks in clusters lasting 6-12 weeks followed by remissions for months or years
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Cluster Headache Diagnostic criteria
A At least 5 attacks fulfilling B - D
B Severe unilateral orbital supraorbital andor temporal pain lasting 15 - 180 min untreated
C Headache is associated with at least 1 of the following signs that have to be present on the pain side 1Conjunctival injection 2Lacrimation 3Nasal congestion 4Rhinorrhea 5Forehead and facial sweating 6Miosis 7Ptosis 8Eyelid edema
D Frequency of attacks from 1 every other day to 8 a day
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Cluster headache Management bullAbortive bullHigh flow O2 (12 Lmin 100 O2 via NRM seated) bullSumatriptan sc superior to intranasal sc and intranasal are superior to oral bullDHE intranasal (2 mg) is superior to oral im and sc bullZolmitriptan intranasal oral bullLidocaine spray or nasal drops (only moderate reduction of pain in less than 30 of patients)
bullTransitional (ldquobridgerdquo) bullCourse of steroids 60 mg oral prednisone with rapid taper by 10 mg every 2-3 days over 18-24 days bullErgotamine tartrate orallyrectally to prevent nocturnal attacks bullDHE few doses every 6-8 hrs bullOccipital nerve block
bullMaintenance prophylaxis bullCalcium channel blockers (verapamil) 480-720 mg a day as tid or ER bullLithium carbonate 300 mg tid or 450 ER qd bullValproic acid 600-2000 mg
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Paroxysmal Hemicrania(PH) Onset in third decade of life Women gtgt Men (51) Severe unilateral orbitalretroorbitaltemporal pain Attack duration 2-30 minutes Attack frequency gt 5 a day Ipsilateral cranial autonomic symptoms
Episodic PH attacks for 4-24 weeks followed by remission periods
Chronic PH daily with multiple discrete attacks without remissions
Indomethacin in TID dose (total up to 225 mgday) diagnosis-defining treatment
May be difficult to distinguish from cluster HA mdashgt trial
of indomethacin (diagnosis-defining treatment)
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
SUNCTSUNA Onset in fourth decade of life
MenWomen is 32
Short-lasting Unilateral Neuralgiform headache with
Conjunctival injection and TearingAutonomic symptoms
Orbitalretroorbitaltemporal pain with ipsilateral autonomic symptoms
attack duration less than 2 min attack frequency 100-200 a day
Daily or almost daily for weeksmonths wwo remissions
Lamotrigine has best evidence of benefit
Rule out pituitary cavernous sinus pathology neurovascular
conflict (trigeminal neuralgia)
Surgical procedures for refractory cases
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Other Primary Headaches
F
Primary cough headache Primary stabbing headache Primary exertional headache Primary headache associated with sexual activity
Primary thunderclap headache Hypnic headache Hemicrania continua New daily persistent headache
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Secondary Headaches
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
A 26-year-old obese woman with borderline hypertension presents with worsening headache which she describes as a bifrontal and bioccipital band-like pressure and pain variable in intensity - from mild to severe fluctuating throughout the day Occasionally she experiences brief visual loss or graying especially with straining which lasts only seconds On directed questioning she endorses to occasional mild double vision Occasionally she is sensitive to light and sound She sometimes gets nauseated and vomits when the pain is severe and she feels her vision is becoming increasingly blurred What do you suspect may be a diagnosis Diagnostic tests Treatment 1 Migraine 2 Psychogenic headache 3 Pseudotumor cerebri 4 Tension-type headache 5 Posterior fossa tumor CTH mdashgt Lumbar puncture + fundoscopic examination mdashgt acetazlamidetopiramate mdashgt furosemide mdashgt CSF diversion procedures (VP shunt LP shunt VA shunt) optic nerve sheath fenestration
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Medication Overuse Headache (MOH)
Old term rebound headache Headache related to overuse of abortive medication for patients with frequent headaches
Diagnostic criteria
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Medication Overuse Headache
Opioids butalbital-based medications aspirinacetaminophencaffeine highest risk
Triptans moderate risk NSAIDs lowest risk
Treatment
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
bull Vascular disorders
bull Intracranial nonvascular disorders
bull Head andor neck trauma
bull Infection
bull Disorders of homeostasis (metabolic derangements)
bull Substance or its withdrawal
bull Pathology of cranium ENT teeth and mouth other
facial structures
bull Psychiatric disorder
Secondary headaches
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
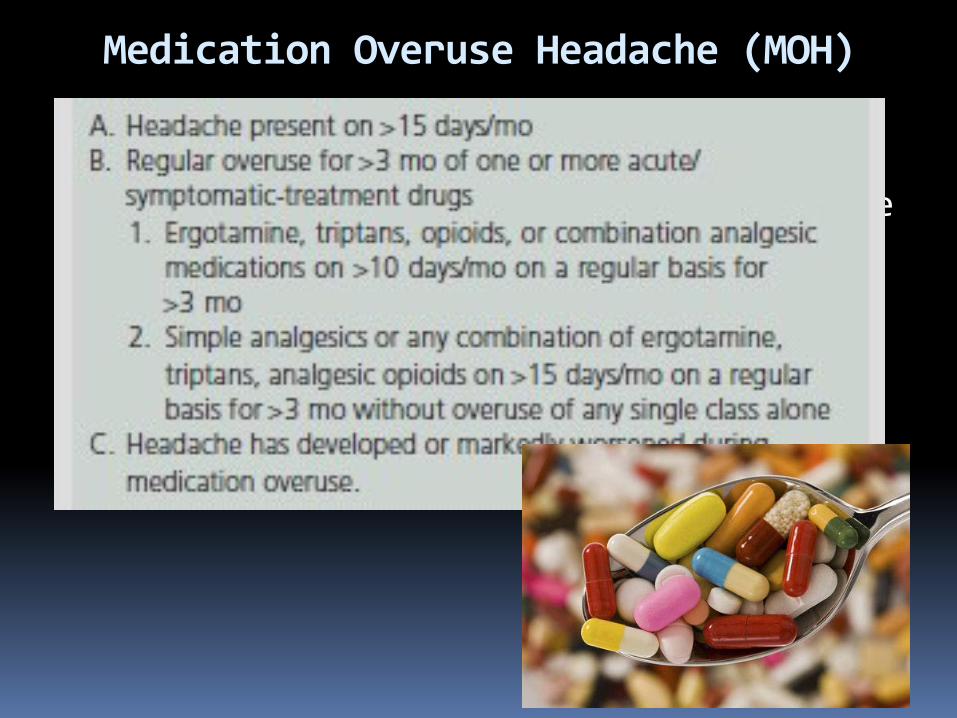
I Primary headaches - Migraine - Tension-type headache - Trigeminal autonomic cephalalgias (TAC) cluster headache paroxysmal hemicrania SUNCTSUNA - other primary headaches
II Secondary headaches - Vascular disorders - Intracranial nonvascular disorder - Head andor neck trauma - Infection - Disorders of homeostasis (metabolic derangements) - Substance or its withdrawal - Cranium ENT teeth and mouth other facial structures - Psychiatric disorder III Cranial neuralgias central or primary facial pain and other headaches
Headache classification
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
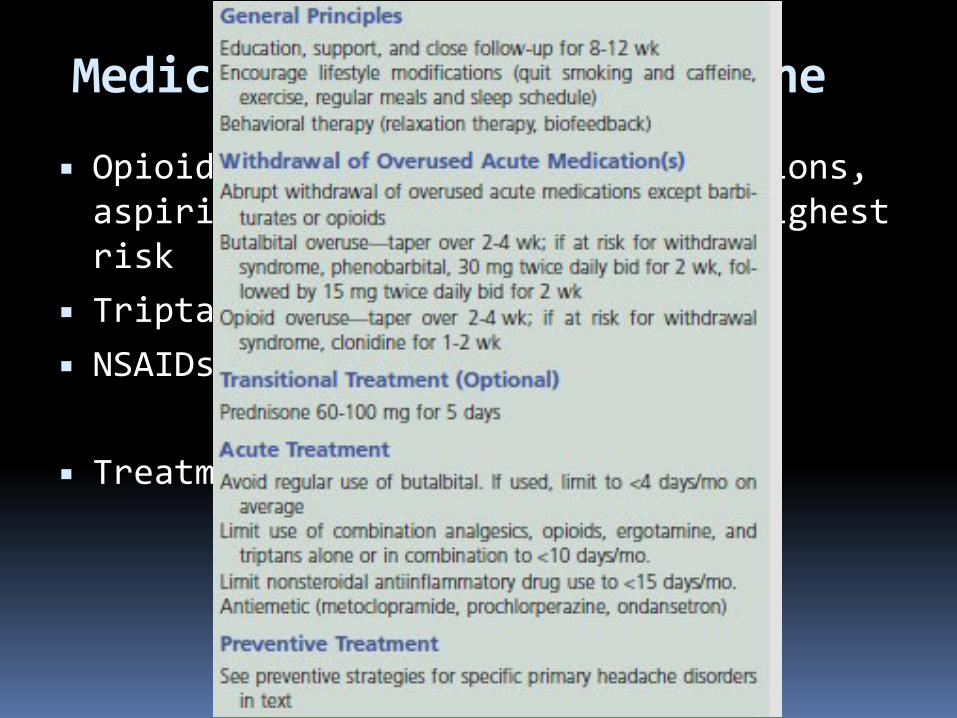
Headaches Diagnostic Algorithm
History and Examination Preliminary diagnosis
Red Flag Primary headache
Secondary headache
NO
YES
Atypical features
Diagnostic testing
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Take home points Most headaches are primary Red Flags (SNOOP4) History and semiology are the most important Diagnostic criteria should be met otherwise diagnosis is ldquoprobable migrainerdquo ldquoprobable cluster headacherdquo etc
Aura positive and negative symptoms for 5-30 minutes Preventive treatment is critical part of treatment Preventive medication choice is based on comorbidities and side effect profile of the medication
Elimination diets are counterproductive Analgesic overuse leads to development of secondary headache - Medication Overuse Headache
Brain +- vascular imaging should be pursued if underlying pathology is suspected
ldquoSinus headachesrdquo are almost nonexistent Cervicogenic headache can be diagnosed only if pathology is at or above C2-C3 level
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
DO NOT IGNORE Thunderclap headache
New onset headache in an adult
Change in headache pattern (intensity frequency new features decreased response to analgesics)
Nocturnal occurrence or early morning awakening
Worseningprecipitation by changes in posture or Valsalva
Presence of focal neurologic signs
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
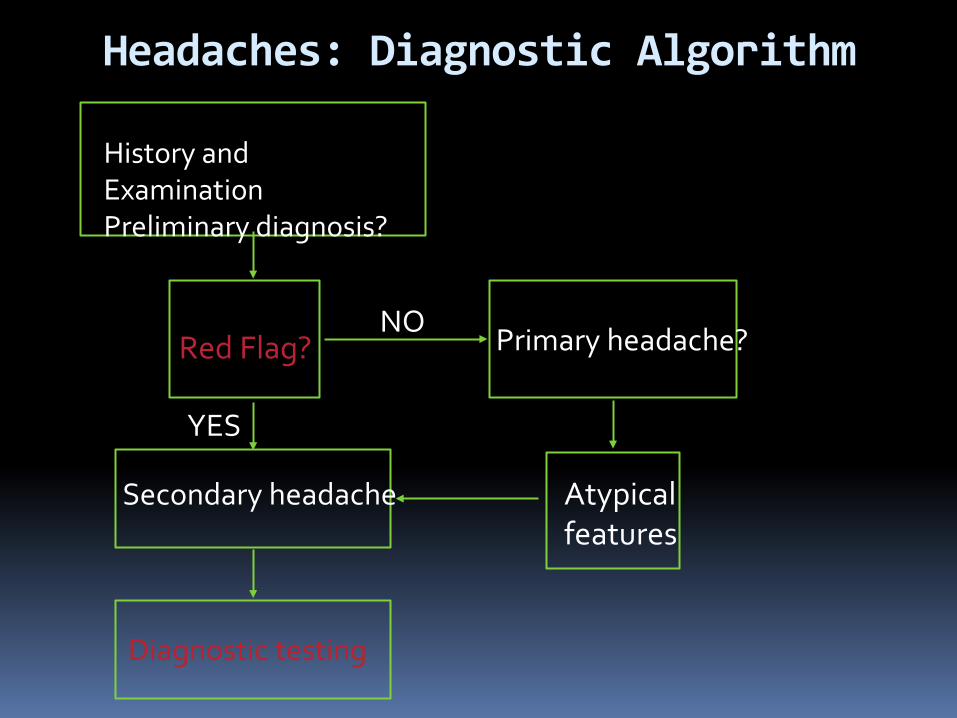
HEADACHE MYTHS
Most headaches are secondary
Headache is a common initial symptom of stroke
Hypertension causes headache
Sinus headaches are common
Occipital neuralgia is common
Cervicogenic headache is due to C4-C7 disc disease
ldquoAtypicalrdquo migraine
Secondary headache in a patient with underlying primary headache disorder always presents with headache of new pattern
Positive Valsalva means secondary headache
Medication side effect is a rare cause of headache
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Questions
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Thank you
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-
Complications of Migraine
1 Status migrainosus
2 Chronic migraine
3 Persistent aura without infarction
4 Migrainous infarction
5 Migralepsy
- Anna Morenkova MD PhD13Assistant Professor13Department of Neurology13UC Irvine
- SOURCE OF HEAD PAIN (NOCICEPTIVE STRUCTURES)
- Headache Disorders Classification
- Slide Number 4
- Headache
- Slide Number 6
- Headaches Diagnostic Algorithm
- Headache features
- Headache features
- Pertinent Questions
- SNOOP4 secondary causes (Red Flags)
- Slide Number 12
- Thunderclap Headache
- Causes of Thunderclap Headache
- Slide Number 15
- Slide Number 16
- Slide Number 17
- Slide Number 18
- Slide Number 19
- Slide Number 20
- Slide Number 21
- Slide Number 22
- Slide Number 23
- Migraine
- Migraine Diagnostic criteria
- probable migraine (ldquomigrainous headacherdquo)
- Migraine headache
- Migraine with Aura
- Slide Number 29
- Aura of migraine diagnostic criteria
- Visual Aura
- Sensory Aura
- Slide Number 33
- Slide Number 34
- Migraine Management
- Potential Food Triggers
- Pharmacologic treatment
- Slide Number 38
- Abortive migraine treatment 13as early as possibleat onset of aura
- Slide Number 40
- Slide Number 41
- Slide Number 42
- Preventiveprophylactic treatment
- Preventive Treatment
- Preventive Treatment
- Prophylactic medication selection
- Slide Number 47
- Slide Number 48
- Botulinum toxin type A
- Butterbur extract (Petadolex)
- Slide Number 51
- Tension Type Headache
- Tension type headache Diagnostic criteria
- Tension type headache Treatment
- Slide Number 55
- Trigeminal Autonomic Cephalalgias (TACs)
- Cluster Headache
- Cluster Headache
- Cluster headache Management
- Paroxysmal Hemicrania(PH)
- SUNCTSUNA
- Other Primary Headaches
- Slide Number 63
- Slide Number 64
- Medication Overuse Headache (MOH)
- Medication Overuse Headache
- Secondary headaches
- Headache classification
- Headaches Diagnostic Algorithm
- Take home points
- DO NOT IGNORE
- HEADACHE MYTHS
- Slide Number 73
- Slide Number 74
- Complications of Migraine
-