
Head and Neck Cancers Kazumi Chino, M.D. Radiation Oncology.

HEAD AND NECK CANCERS Updated May 2016 by Dr. Daniel Yokom (PGY5 Medical Oncology Resident, University of Toronto) Reviewed by Dr. Raymond Jang (Staff Medical Oncologist, University of Toronto) and Dr. Desiree Hao (Staff Medical Oncologist, University of Calgary) DISCLAIMER: The following are study notes compiled by the above PGY5 medical oncology residents and reviewed by a staff medical oncologist. They reflect what we feel is relevant knowledge for graduating medical oncology residents preparing for their final examination. The information has not been surveyed or ratified by the Royal College. NOTE: Head and neck squamous cell carcinoma (HNSCC) and EBVrelated nasopharyngeal carcinoma (NPC) are very different and will be discussed separately Head and Neck Squamous Cell Carcinoma
A) PUBLIC HEALTH
EPIDEMIOLOGY (1) Incidence:
o In 2010 over 4000 Canadians were diagnosed with HNSCC o HPVassociated HNSCC usually diagnosed at a younger age o Increasing incidence of HPVassociated HNSCC (primarily oropharyngeal) while tobacco
related incidence is declining (2) o Male:Female > 3:1 depending on anatomical site
Mortality: o In 2010 over 1500 Canadians died from HNSCC
RISK FACTORS
o Smoking o HPV o EtOH
PREVENTION & SCREENING Prevention:
o Smoking and EtOH cessation o HPV vaccine and methods to reduce HPV exposure
Screening: o No screening recommendations in Canada or United States.
B) PRESENTATION & DIAGNOSIS
SYMPTOMS & SIGNS Common Symptoms:
o Palpable mass or lymph node o Weight loss o Often depends on primary, for example:
Laryngeal: hoarseness or other changes in the voice, cough, difficult or noisy breathing
Oropharyngeal: sore throat lasting longer than a few weeks, feeling that something is stuck in the throat, difficult or painful swallowing, ear pain
Oral cavity: nonhealing ulcer or mass INVESTIGATIONS

Physical exam: o Oral cavity o Head and neck lymph nodes o Cranial nerve exam
Laboratory: o Routine BW, hepatitis screen
Diagnostic Imaging: o CT head and neck o MRI neck for oropharyngeal, may be necessary for other sites o CT chest (stage II or higher) o PET scan for HNSCC primary unknown o CT abdomen and bone scan are not routinely performed
Diagnostic Procedures: o Endoscopy and biopsy o Consider FNA of suspicious lymph nodes for staging
Other: o Ensure women with HPV+ HNSCC have routine surveillance for cervical cancer – pelvic
exam and pap smear.
PATHOLOGY & MOLECULAR BIOLOGY Common Histology:
o Vast majority are squamous cell carcinoma and discussion in this chapter pertains to SCC. o Differential includes adenocarcinoma, melanoma, sarcoma, lymphoma
Common Metastatic Sites: o Local recurrence and lymph nodes o Lung o Bone
Relevant Molecular Biology: o HPV testing using IHC for p16(3)
STAGING Staging for HNSCC is complex as it is different for each anatomical site. General rules to follow: N1 = one LN less than 3 cm N2a = one LN >3 cm and < 6 cm N2b = multiple ipsilateral LN; all < 6 cm N2c = bilateral or contralateral LN; all <6cm N3 = LN > 6cm T13 N1 = Stage III T13 N23 = Stage IV T4 any N = Stage IV Any distant metastatic site = Stage IVC NOTE: New staging recommendations for HPV+ oropharyngeal cancer to be published in 2016 (4)
C) TREATMENT EARLY STAGE
Bottom Line General Approach: o Primary surgery or radical radiation alone o No role for chemotherapy

Prognosis: o 5yr OS 5690% depending on location of the tumor
LOCALLY ADVANCED
Bottom Line General Approach: o Management depends on a number of factors including anatomical site, size, invasion,
comorbidities, patient preference, etc: Consider discussion at a multidisciplinary tumor board Often:
Oral cavity: primary surgery followed by radiation +/ chemotherapy Oropharyngeal, laryngeal, hypopharyngeal: Radiation +/ chemotherapy,
surgery for salvage therapy only
o If goes for primary radiation +/ concurrent chemotherapy Radiation: 70Gy/35# Cisplatin 100mg/m2 d1, 22, 43 (5)
50% of patients do not get third dose Consider RT + weekly cisplatin 40mg/m2 for less well patients If cisplatin contraindicated consider RT + cetuximab 400mg/m2 load (one
week prior to RT) then 250mg/m2 weekly during radiation (6) No clear benefit for patients over 71 years of age – area of ongoing
research. Ongoing trials investigating whether less intense chemotherapy is effective for
patients with HPV+ HNSCC (7)
o If goes for primary surgery then postoperative management: No adjuvant treatment if lowrisk (no intermediate or highrisk features) Intermediate risk: adjuvant RT alone 66Gy/33#
>T2 Close margins PNI LVI N2 or greater Level IV or V nodes
Highrisk (8): adjuvant CRT with highdose cisplatin 100mg/m2 d1, 22, 43 Positive margins Extracapsular spread
Note: Begin within 11 weeks of surgery
Prognosis: o Better with HPV+ nonsmokers(9) o Highrisk for secondary malignancy (usually due to lifestyle i.e. smoking)
Followup:
o Imaging ~2 months after treatment Important Phase III Clinical Trials:

RTOG 9111 Concurrent chemotherapy and radiotherapy for organ preservation in advanced laryngeal
cancer. Forastiere et al. NEJM. 2003. UPDATED: LongTerm Results of RTOG 9111: A Comparison of Three Nonsurgical
Treatment Strategies to Preserve the Larynx in Patients With Locally Advanced Larynx Cancer. Forastiere et al. JCO. 2013.
Regimen 1. Induction cisplatin 100mg/m2 d1 plus 5FU 1000mg/m2/d d15 q3w x
3 cycles followed by RT 70Gy/35# 2. Concurrent cisplatin 100mg/m2 d1, 22, 43 and RT 3. RT alone
Primary Endpoint Laryngectomyfree survival Inclusion/Exclusion Criteria
Previously untreated stage III/IV HNSCC of the larynx T1 and T4 excluded Karnofsky PPS >= 60
Size (N) 518 Results LaryngectomyFree Survival: Concurrent CRT significantly
improved LFS HR 0.58 (95% CI 0.370.89, p=0.005) Overall Survival: No difference although trend towards worse with
concurrent CRT HR 1.25 (95% CI 0.98 – 1.61, p=0.08) compared to induction chemotherapy
Toxicity Concurrent CRT more toxic: stomatitis (43% vs 20%), esophagitis (35% vs 19%), nausea/vomiting (20% vs 14%)
Conclusion Concurrent CRT improved laryngectomyfree survival with no improvement in OS
Other Comments 70% of patients in concurrent CRT arm received 3 cycles of cisplatin (more than realworld numbers)
Radiotherapy plus cetuximab for squamouscell carcinoma of the head and neck. Bonner
et al. NEJM. 2006.
Regimen 1. RT alone, 7076Gy 2. RT plus Cetuximab (400mg/m2 load 1 week prior to RT then
250mg/m2 weekly during RT) Primary Endpoint Locoregional control Inclusion/Exclusion Criteria
Previously untreated stage III/IV nonmetastatic HNSCC of the oropharynx, hypopharynx or larynx
Karnofsky PPS >= 60 Normal hematopoietic, hepatic and renal function
Size (N) 424 Results Locoregional control: RT+cetux significantly improved locoregional
progression median 24.4mo vs 14.9mo, HR 0.68 (95% CI 0.520.89, p=0.005)
Overall Survival: RT+cetux significantly improved median survival 49.0 vs 29.3 mo (p=0.03), 3y OS 55% vs 45% (p=0.05), HR 0.74 (95% CI 0.570.97)
Toxicity acneiform rash: 87% vs 10% all grades, 17% gr 35 infusion reaction: 15% vs 2% all grades, 3% vs 0% gr 35 other mild side effects of cetuximab: weight loss, headache, nausea
Conclusion RT+cetux improves locoregional control and overall survival compared to RT alone
Other Important Published Data for HNSCC:

Defining risk levels in locally advanced head and neck cancers: A comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (#9501). Bernier et al. Head & Neck. 2005.
Methods: o Analysis of pooled data from EORTC 22931 (10) and RTOG 9501 (11,12). Both studies
compared postsurgery adjuvant radiation to adjuvant chemoradiation with highdose cisplatin (100mg/m2 d1,22,43) in patients with highrisk features.
Results o Patients who benefit from addition of adjuvant highdose cisplatin to radiation include those
with features of positive margins and/or extracapsular extension from lymph nodes Patients without these features had no survival advantage with addition of
chemotherapy Bottomline
o Patients with positive margins and/or extracapsular extension have improved survival with addition of cisplatin to radiation.
Metaanalysis of chemotherapy in head and neck cancer (MACHNC): An update on 93 randomised trials and 17,346 patients. Pignon et al. Radiotherapy and Oncology. 2009.
Methods: o Individual patient data from trials comparing locoregional treatment of radiation with or
without chemotherapy Results
o 87 trials with 16,485 individual patients included o HR for death = 0.88 (p < 0.0001) for addition of any chemotherapy, 5year absolute survival
benefit of 4.5% (p < 0.0001) o Concurrent CRT better than sequential (either induction or adjuvant)
HR for death = 0.81 for concurrent CRT, 5year absolute survival benefit = 6.5% o Decreasing benefit with age, particularly >70yo
Bottomline o Significant benefit of concurrent CRT o Consider RT alone for patients >70yo
Notes o Trials of NPC only were excluded
Metaanalysis of chemotherapy in head and neck cancer (MACHNC): A comprehensive analysis by tumour site. Blanchard et al. Radiotherapy and Oncology. 2011.
Methods: o Individual patient data from trials comparing locoregional treatment of radiation with or
without chemotherapy o Patients divided into 4 tumor locations: oral cavity, oropharynx, hypopharynx and larynx
Other tumor locations were excluded Results
o 87 trials with 16,192 individual patients included o Addition of chemotherapy beneficial for all sites o Concurrent CRT better than sequential statistically for oropharyngeal and laryngeal only.
5year OS benefits of concurrent vs sequential: 8.9% oral cavity (p = 0.15) 8.1% oropharynx (p < 0.0001) 5.4% larynx (p = 0.05) 4% hypopharynx (p = 0.31)
Bottomline
o Significant benefit of chemotherapy for all anatomical sites o Concurrent better for oropharyngeal and laryngeal and likely also for oral cavity and
hypopharynx although not statistically significant SUPPORTIVE MEASURES
Consults: o All patients should be referred to a dietitian and considered for a feeding tube
Assess weight prior to each chemo dose, >10% weight loss is concerning o SLP o Dentistry o Smoking cessation o Consider hearing test
Hydration o Patients on highdose cisplatin require significant hydration at home or some centres
choose to admit patients to hospital METASTATIC
Bottom Line General Approach: o Consider salvage surgery or radiation o Firstline is cisplatin 75mg/m2 d1 and 5FU 1000mg/m2/d d14 q34w
Consider splitting cisplatin 25mg/m2/d d13 o Other firstline regimens: weekly cisplatin, carboplatin + paclitaxel o Cetuximab added to platinum + 5FU in some places based on EXTREME trial(13) but not
funded in Ontario o No evidence for survival for secondline treatments but reasonable option is docetaxel
Evidence for nivolumab in second line will be available in 2016
Prognosis: o Median OS 69 months, better in HPVrelated disease
Important Phase III Clinical Trials:
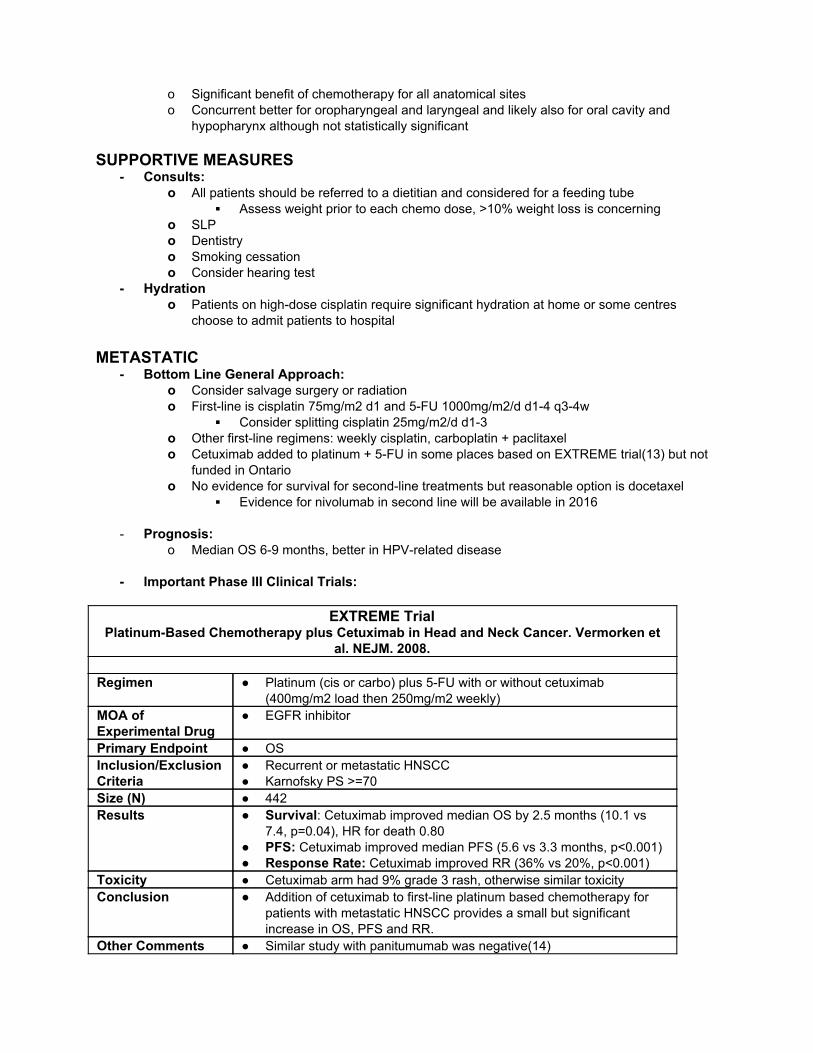
EXTREME Trial
PlatinumBased Chemotherapy plus Cetuximab in Head and Neck Cancer. Vermorken et al. NEJM. 2008.
Regimen Platinum (cis or carbo) plus 5FU with or without cetuximab
(400mg/m2 load then 250mg/m2 weekly) MOA of Experimental Drug
EGFR inhibitor
Primary Endpoint OS Inclusion/Exclusion Criteria
Recurrent or metastatic HNSCC Karnofsky PS >=70
Size (N) 442 Results Survival: Cetuximab improved median OS by 2.5 months (10.1 vs
7.4, p=0.04), HR for death 0.80 PFS: Cetuximab improved median PFS (5.6 vs 3.3 months, p<0.001) Response Rate: Cetuximab improved RR (36% vs 20%, p<0.001)
Toxicity Cetuximab arm had 9% grade 3 rash, otherwise similar toxicity Conclusion Addition of cetuximab to firstline platinum based chemotherapy for
patients with metastatic HNSCC provides a small but significant increase in OS, PFS and RR.
Other Comments Similar study with panitumumab was negative(14)

Nasopharyngeal Carcinoma
A) PUBLIC HEALTH
EPIDEMIOLOGY(1) Incidence:
o Rare: <1:100,000/yr in North America, up to 65:100,000 among patients in Northern Africa, Southern China and Southeast Asia.
o In 2010 250 Canadians were diagnosed with NPC o Male:Female = 2:1
Mortality: o In 2010 100 Canadians died from NPC
RISK FACTORS NPC
o Most common in Southeast Asian and Chinese ancestry o EpsteinBarr virus o Salted fish and meat o Smoking
PREVENTION & SCREENING Prevention:
o Smoking cessation o Reduce intake of salted fish and meat o Reduce occupational exposures
Screening: o No screening recommendations in Canada or United States.
B) PRESENTATION & DIAGNOSIS
SYMPTOMS & SIGNS Common Symptoms:
o Palpable mass or lymphadenopathy o Nasal symptoms: nose bleeds or bloody discharge from the nose, stuffiness or blockage in
the nose o Ear symptoms: pain or blockage in one ear, persistent infections in one ear, ringing in the
ear, or tinnitus, hearing difficulties or hearing loss o Eye symptoms: bulging eye, diplopia o trismus, sore throat, facial pain, headache, cranial nerve deficits o weight loss
INVESTIGATIONS

Physical exam Laboratory:
o Routine BW, hepatitis screen o EBV level
Diagnostic Imaging: o CT head and neck o MRI neck o CT chest o PET scan if no obvious metastases o CT abdomen and bone scan are not routinely performed
Diagnostic Procedures: o Endoscopy o Biopsy/FNA, EBER on tumor
PATHOLOGY & MOLECULAR BIOLOGY Common Histology:
o Keratinizing squamouscell carcinoma (WHO type I) o Differentiated nonkeratinizing carcinoma (WHO type II)
Strongest relationship with EBV o Undifferentiated carcinoma (WHO type III)
Common Metastatic Sites: o Local recurrence o Lung o Bone
Relevant Molecular Biology: STAGING
C) TREATMENT LOCALIZED / ADJUVANT / RESECTABLE
Bottom Line General Approach: o Stage I
Radiation to primary (70Gy/35#) o Stage II
Radiation plus highdose cisplatin (100mg/m2) +/ adjuvant chemotherapy Prognosis:
o 5yr OS 7090%
Important Phase III Clinical Trials for NPC:
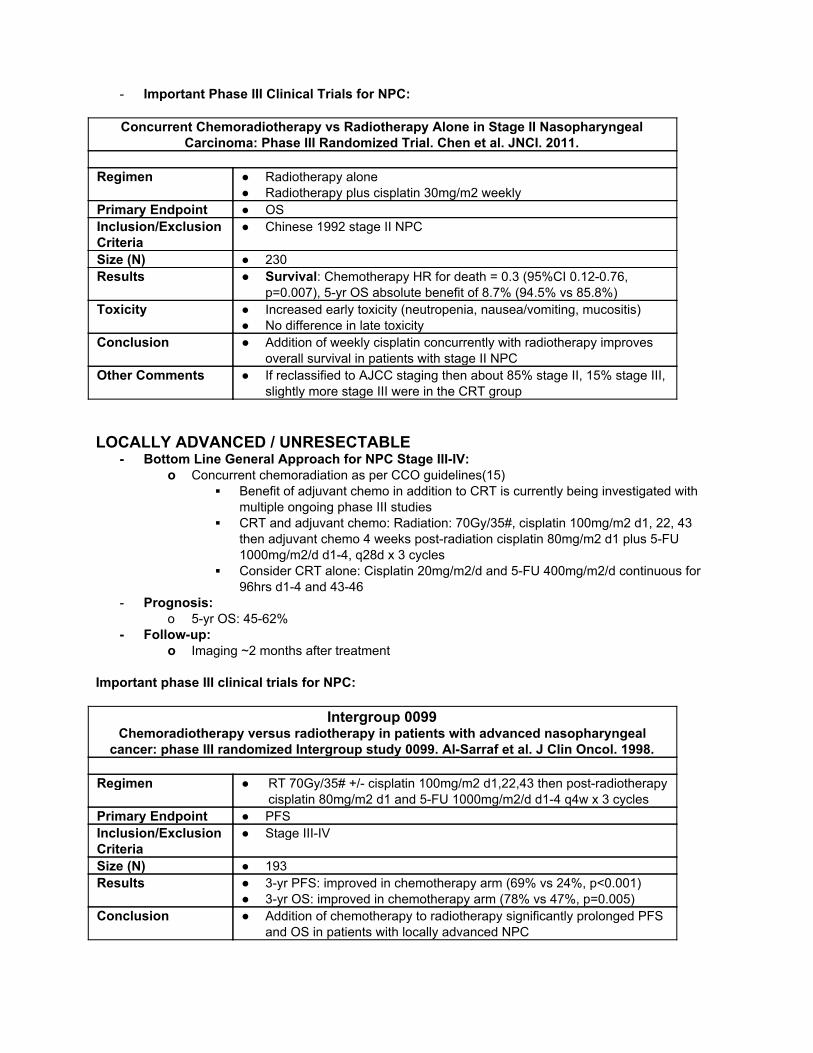
Concurrent Chemoradiotherapy vs Radiotherapy Alone in Stage II Nasopharyngeal Carcinoma: Phase III Randomized Trial. Chen et al. JNCI. 2011.
Regimen Radiotherapy alone
Radiotherapy plus cisplatin 30mg/m2 weekly Primary Endpoint OS Inclusion/Exclusion Criteria
Chinese 1992 stage II NPC
Size (N) 230 Results Survival: Chemotherapy HR for death = 0.3 (95%CI 0.120.76,
p=0.007), 5yr OS absolute benefit of 8.7% (94.5% vs 85.8%) Toxicity Increased early toxicity (neutropenia, nausea/vomiting, mucositis)
No difference in late toxicity Conclusion Addition of weekly cisplatin concurrently with radiotherapy improves
overall survival in patients with stage II NPC Other Comments If reclassified to AJCC staging then about 85% stage II, 15% stage III,
slightly more stage III were in the CRT group LOCALLY ADVANCED / UNRESECTABLE
Bottom Line General Approach for NPC Stage IIIIV: o Concurrent chemoradiation as per CCO guidelines(15)
Benefit of adjuvant chemo in addition to CRT is currently being investigated with multiple ongoing phase III studies
CRT and adjuvant chemo: Radiation: 70Gy/35#, cisplatin 100mg/m2 d1, 22, 43 then adjuvant chemo 4 weeks postradiation cisplatin 80mg/m2 d1 plus 5FU 1000mg/m2/d d14, q28d x 3 cycles
Consider CRT alone: Cisplatin 20mg/m2/d and 5FU 400mg/m2/d continuous for 96hrs d14 and 4346
Prognosis: o 5yr OS: 4562%
Followup: o Imaging ~2 months after treatment
Important phase III clinical trials for NPC:
Intergroup 0099 Chemoradiotherapy versus radiotherapy in patients with advanced nasopharyngeal
cancer: phase III randomized Intergroup study 0099. AlSarraf et al. J Clin Oncol. 1998.
Regimen RT 70Gy/35# +/ cisplatin 100mg/m2 d1,22,43 then postradiotherapy cisplatin 80mg/m2 d1 and 5FU 1000mg/m2/d d14 q4w x 3 cycles
Primary Endpoint PFS Inclusion/Exclusion Criteria
Stage IIIIV
Size (N) 193 Results 3yr PFS: improved in chemotherapy arm (69% vs 24%, p<0.001)
3yr OS: improved in chemotherapy arm (78% vs 47%, p=0.005) Conclusion Addition of chemotherapy to radiotherapy significantly prolonged PFS
and OS in patients with locally advanced NPC

Other Important Published Data for NPC: Concurrent chemoradiotherapy plus adjuvant chemotherapy versus concurrent chemoradiotherapy alone in patients with locoregionally advanced nasopharyngeal carcinoma: a phase 3 multicentre randomised controlled trial. Chen et al. Lancet Oncol. 2012.
Methods: o Phase III RCT of concurrent radiation (66Gy/33#) plus weekly cisplatin (40mg/m2) with or
without adjuvant cisplatin (80mg/m2 d1) and 5FU (800mg/m2/d d14) q4w x 3 cycles o Primary endpoint was failurefree survival
Results o 508 patients enrolled o No difference in 2yr failurefree survival (86% vs 84%, p=0.13) o No difference in toxicity
Bottomline o No benefit of adding adjuvant cisplatin and 5FU to CRT for locally advanced NPC
Note o Early results published, final results are pending
Chemotherapy and radiotherapy in nasopharyngeal carcinoma: an update of the MACNPC metaanalysis. Blanchard et al. Lancet Oncology. 2015.
Methods: o Individual patient data from trials comparing treatment of radiation with or without
chemotherapy for locally advanced NPC, updated from 2006 metaanalysis. o Included interaction testing for different schedules of chemotherapy
Results o 19 trials with 4806 individual patients included o Pooled HR for death 0.79 (95%CI 0.730.86, p<0.0001) o Absolute 5yr OS benefit of chemotherapy is 6.3% o Concurrent chemotherapy with or without adjuvant chemotherapy is better than adjuvant
alone or induction alone (p=0.01) Bottomline
o Concurrent chemoradiation significantly improves OS, PFS and local control in patients with locally advanced NPC.
o Addition of adjuvant chemotherapy to chemoradiation of unclear benefit, nonsignificant trend towards improvement with adjuvant chemotherapy.
o Minimal or no benefit with induction chemotherapy or adjuvant chemotherapy alone SUPPORTIVE MEASURES
o Refer to supportive measures for HNSCC METASTATIC
Bottom Line General Approach: o Consider salvage surgery or radiation o No randomized evidence, consider clinical trial o Cisplatin and gemcitabine typically given as firstline, one possible regimen is:
Cisplatin 70mg/m2 d1 and gemcitabine 1000mg/m2 d1 and 8 q21d o Other firstline regimens: carboplatin and gemcitabine, cisplatin and 5FU, cisplatin and
paclitaxel, weekly cisplatin, capecitabine Prognosis:
o 5yr OS 20%
Other Important Published Data for NPC:

Comparison of five cisplatinbased regimens frequently used as the firstline protocols in metastatic nasopharyngeal carcinoma. Jin et al. J Cancer Res Clin Oncol. 2012.
Methods: o Retrospective review of 822 patients with metastatic or recurrent NPC
Results o Five common treatments: cisplatin plus gemcitabine, cisplatin plus 5FU, cisplatin plus
paclitaxel, cisplatin plus paclitaxel plus 5FU and cisplatin plus 5FU plus bleomycin. o Highest RR with cisgem (71.1%), statistically significant over cis5FU (60.2%), p=0.033. o No difference in PFS or OS. o More toxicity with threedrug regimens.
Bottomline o Cisgem, cis5FU and cispaclitaxel are all active regimens for metastatic NPC o No benefit for three drugs over two.
D) REFERENCES
1. Canadian Cancer Society. Canadian Cancer Statistics 2015: Special topic: Predictions of the future
burden of cancer in Canada. 2015; 2. Forte T, Niu J, Lockwood GA, Bryant HE. Incidence trends in head and neck cancers and human
papillomavirus (HPV)associated oropharyngeal cancer in Canada, 19922009. Cancer Causes Control. 2012 Aug;23(8):1343–8.
3. Gilbert R, Winquist E, Waldron J, Mcquestion M. The Management of Head and Neck Cancer in Ontario : Organizational and Clinical Practice Guideline Recommendations. 2009.
4. O’Sullivan B, Huang SH, Su J, Garden AS, Sturgis EM, Dahlstrom K, et al. Development and validation of a staging system for HPVrelated oropharyngeal cancer by the International Collaboration on Oropharyngeal cancer Network for Staging (ICONS): a multicentre cohort study. Lancet Oncol. 2016 Feb 26;17(4):440–51.
5. Adelstein DJ, Li Y, Adams GL, Wagner H, Kish J a, Ensley JF, et al. An intergroup phase III comparison of standard radiation therapy and two schedules of concurrent chemoradiotherapy in patients with unresectable squamous cell head and neck cancer. J Clin Oncol. 2003;21(1):92–8.
6. Bonner JA, Harari PM, Giralt J, Azarnia N, Shin DM, Cohen RB, et al. Radiotherapy plus Cetuximab for SquamousCell Carcinoma of the Head and Neck. N Engl J Med. 2006 Feb 9;354(6):567–78.
7. O’Sullivan B, Huang SH, Siu LL, Waldron J, Zhao H, PerezOrdonez B, et al. Deintensification candidate subgroups in human papillomavirusrelated oropharyngeal cancer according to minimal risk of distant metastasis. J Clin Oncol. 2013 Feb 10;31(5):543–50.
8. Bernier J, Cooper JS, Pajak TF, van Glabbeke M, Bourhis J, Forastiere A, et al. Defining risk levels in locally advanced head and neck cancers: a comparative analysis of concurrent postoperative radiation plus chemotherapy trials of the EORTC (#22931) and RTOG (# 9501). Head Neck. 2005 Oct;27(10):843–50.
9. Ang KK, Harris J, Wheeler R, Weber R, Rosenthal DI, NguyenTân PF, et al. Human papillomavirus and survival of patients with oropharyngeal cancer. N Engl J Med. 2010 Jul 1;363(1):24–35.
10. Bernier J, Domenge C, Ozsahin M, Matuszewska K, Lefèbvre JL, Greiner RH, et al. Postoperative irradiation with or without concomitant chemotherapy for locally advanced head and neck cancer. N Engl J Med. 2004;350(19):1945–52.
11. Cooper JS, Pajak TF, Forastiere AA, Jacobs J, Campbell BH, Saxman SB, et al. Postoperative concurrent radiotherapy and chemotherapy for highrisk squamouscell carcinoma of the head and neck. N Engl J Med. 2004 May 6;350(19):1937–44.
12. Cooper JS, Zhang Q, Pajak TF, Forastiere AA, Jacobs J, Saxman SB, et al. Longterm followup of the RTOG 9501/intergroup phase III trial: postoperative concurrent radiation therapy and chemotherapy in highrisk squamous cell carcinoma of the head and neck. Int J Radiat Oncol Biol Phys. 2012 Dec 1;84(5):1198–205.
13. Vermorken JB, Mesia R, Rivera F, Remenar E, Kawecki A, Rottey S, et al. Platinumbased

chemotherapy plus cetuximab in head and neck cancer. N Engl J Med. 2008 Sep 11;359(11):1116–27.
14. Vermorken JB, StöhlmacherWilliams J, Davidenko I, Licitra L, Winquist E, Villanueva C, et al. Cisplatin and fluorouracil with or without panitumumab in patients with recurrent or metastatic squamouscell carcinoma of the head and neck (SPECTRUM): an openlabel phase 3 randomised trial. Lancet Oncol. 2013 Jul;14(8):697–710.
15. Thephamongkhol K, Browman G, Hodson I, Oliver T, Zuraw L. A Quality Initiative of the Program in Evidencebased Care (PEBC), Cancer Care Ontario (CCO) Nasopharyngeal Cancer. 2013.


















