HCP Survey _ Results _ Final.
34
1 Healthcare Planners: “What can they bring to the briefing table in Healthcare projects?” Summary of questionnaire results. Abstract. This paper contains a short summary of a questionnaire undertaken as part of the dissertation component of “MSc Planning Buildings for Health” at London South Bank University. The rationale and methodology for the questionnaire are briefly explained. The results are presented in tables and figures, each of which are followed by a brief summary of the findings. The results are followed by conclusions drawn from the primary data and recommendations for further development and research of the Healthcare Planner’s role. Key words: Healthcare Planner, Project briefing, Healthcare Construction. (Author: Delly Dickson, RGN, MSc, July 2015.)
-
Upload
delly-dickson -
Category
Documents
-
view
326 -
download
1
Transcript of HCP Survey _ Results _ Final.

1
Healthcare Planners: “What can they bring to the
briefing table in Healthcare projects?”
Summary of questionnaire results.
Abstract.
This paper contains a short summary of a questionnaire undertaken as part of the
dissertation component of “MSc Planning Buildings for Health” at London South
Bank University. The rationale and methodology for the questionnaire are briefly
explained. The results are presented in tables and figures, each of which are
followed by a brief summary of the findings. The results are followed by conclusions
drawn from the primary data and recommendations for further development and
research of the Healthcare Planner’s role.
Key words: Healthcare Planner, Project briefing, Healthcare Construction.
(Author: Delly Dickson, RGN, MSc, July 2015.)
2
Contents List of Tables ............................................................................................... 3
List of Figures .............................................................................................. 3
Introduction. ................................................................................................. 4
Questionnaire Development. ...................................................................... 4
Questionnaire Content. ............................................................................... 5
Questionnaire Analysis. .............................................................................. 7
Questionnaire Results. ............................................................................... 8
Conclusions............................................................................................... 32
Recommendations. .................................................................................. 33
References. ............................................................................................... 34
3
List of Tables Table 1. Response rate - actual response numbers and percentages by modified grouping.
(Dickson. March 2015) .......................................................................................................... 8
Table 2. HCP declared professional qualifications. (Dickson. March 2015) ......................... 10
Table 3. Comparison table - Perception of the frequency that HCP's are involved in the
briefing process. (Dickson. March 2015) ............................................................................. 14
Table 4. Comparison Table - The top three activities undertaken by HCP's. (Dickson. March
2015) .................................................................................................................................. 20
Table 5. Recognition of HCP skills by Healthcare Construction Industry – perception of
HCP’s. (Dickson. March 2015) ............................................................................................ 21
Table 6. Recognition of HCP skills by Healthcare Construction Industry - perception of
Construction. (Dickson. March 2015) .................................................................................. 22
Table 7. Recognition of HCP skills by Healthcare Construction Industry - perception of
Client. (Dickson. March 2015) ............................................................................................. 23
List of Figures Figure 1. Four groups that are involved in the briefing stages of healthcare projects.
(Dickson. March 2015) .......................................................................................................... 6
Figure 2. HCP declared professions. (Dickson. March 2015) ................................................ 9
Figure 3. Demographics of where all respondents live. (Dickson. March 2015) ................... 11
Figure 4. Demographics of where all respondents have worked. (Dickson. March 2015) .... 12
Figure 5. HCP type of employment. (Dickson. March 2015) ................................................ 13
Figure 6. HCP opinion of the questionnaire statement. Question 11. (Dickson. March 2015)
........................................................................................................................................... 15
Figure 7. Construction Industry and Client opinion of questionnaire statement. Questions 31,
50 and 71. (Dickson. March 2015) ...................................................................................... 16
Figure 8. HCP declared activities from list provided. (Dickson. March 2015) ....................... 17
Figure 9. Construction Industry expectation of HCP activities from list provided. (Dickson.
March 2015) ........................................................................................................................ 18
Figure 10. Client expectation in briefing activities from HCP and substantive staff. (Dickson.
March 2015) ........................................................................................................................ 19
Figure 11. HCP responses - "How do you keep yourself updated?" (Dickson. March 2015) 25
Figure 12. All respondents - "Do you consider that the HCP role requires further
development, with more formal recognition in the healthcare sector?" (Dickson. March 2015)
........................................................................................................................................... 28
Figure 13. All respondents - "How do you think HCP skills or competencies should or could
be measured?" (Dickson. March 2015) ............................................................................... 30
4
Introduction.
During the spring of 2015, an electronic questionnaire was developed for the
dissertation component of the “MSc Planning Buildings for Health” course at the
London South Bank University. Curiosity had been piqued by the role of “Healthcare
Planners” (HCP’s) within the Healthcare Construction Industry in Great Britain. The
purpose of the questionnaire was to explore how Healthcare Planner’s (HCP’s)
contributed to Healthcare Construction Projects. Focus was placed on the briefing
stages of Healthcare Construction Projects. This paper presents a summary of the
questionnaire methodology and the questionnaire results, followed by conclusions
drawn from the data and recommendations for further development and research.
Questionnaire Development.
The preferred method for primary data collection was identified as an electronic
questionnaire, which utilised the strengths of quantitative and qualitative research
methods.
Due to the diversity and complexity of activities undertaken, plus the subjective nature
of the HCP’s role, a combination of descriptive and analytical questions (Neville. 2014,
p.7) facilitated inclusion of the less tangible aspects of the research hypothesis. To
create depth and richness within the research findings (Carr, 1994, p.721) the
responses were initially triangulated across four groups of participants, to enable
comparison of attitudes and values.
A pathway for individual participants to choose was identified at question five. The
decision of which pathway to take was chosen by the participant according to their
own interpretation of their employment status, within the headings offered. Definition
or explanation of the headings was not provided. This intentional omission allowed
participants some flexibility on how to define themselves, along with the opportunity to
probe individual’s perceptions of their role in the subsequent analysis. This meant that
each grouping was self-defined and therefore included a mixture of professions.
5
The questionnaire included both closed and open questions which related to the
findings from a literature review and the hypothesis being investigated. (Robinson.
2014, p.4) All open and most of the closed questions incorporated an opportunity to
include additional comments, either to clarify the response or to add additional
information, which the participant felt was pertinent to the hypothesis.(Oppenheim.
1992, p.112) This facilitated the opportunity to probe beneath the surface and access
data that was rich in personal comment and insight. (Neville. 2014, p.37) However,
acknowledged limitations of this type of research include difficulty in reproducing
results along with subjective findings which are open to differing interpretations,
(Brace. 2013, p.43). This meant that it would be difficult to generalise the results and
to replicate the findings.
To maximise the number of potential participants, invitations were extended via a
mixture of sampling strategies. This resulted in a variable sample size across the
groups as they were approached directly or in-directly for voluntary participation. It is
acknowledged that this sampling strategy provided little control regarding the number
of participants, however, absolute control over participant selection was not a critical
factor for this study. (Neville. 2014, p.31) Limited control was achieved by approaching
participants from within the construction and healthcare industries and the
questionnaire was available on-line for an imposed time limit of four weeks. It is
considered that there are no ethical concerns within this research as all required
permissions have been granted. (Carr. 1994, p.719).
Questionnaire Content.
To enable triangulation of results, a generic questionnaire was developed for
distribution to four main groups who had been identified from the literature as major
contributors to the development of a healthcare project brief. The four main groups
were identified as Health Clients, Principle Supply Chain Partners (PSCP’s), non-
PSCP’s and Healthcare Planners. The groups approached for this research are
identified in figure 1.
6
Figure 1. Four groups that are involved in the briefing stages of healthcare projects. (Dickson. March 2015)
The questionnaire contained a total of eighty six questions, distributed evenly across
the four groups. Following self-identification of their profession at question five, each
participant was funnelled to a specific pathway within the questionnaire. Each pathway
contained the same questions, with generic wording modified to reflect the group’s
perspective in relation to HCP’s. For example, the question “Do you currently work “as
a” Healthcare Planner?” on the HCP pathway, was modified to “Do you currently work
“with” Healthcare Planners?” on the other three pathways. This ensured that questions
were relevant to the participant’s chosen grouping and facilitated subsequent analysis.
A small pilot study distributed to HCP’s, healthcare clients and construction industry
professionals was completed to ensure the format and content was appropriate before
wider distribution. Minor adjustments were made to the questionnaire content following
feedback.
The questionnaire launched on 14th January 2015 for a period of four weeks, to an
initial distribution list of ninety two participants who had expressed an interest. The
questionnaire closed at midnight on 11th February 2015.
Willing participants were added to the distribution list as they expressed interest by
direct contact or via LinkedIn Group forums. This resulted in a total distribution list of
Health Clients
PSCP
Non-PSCP
Healthcare Planners
7
one hundred and forty one (141) people who had expressed an interest in
participating.
Questionnaire Analysis.
Primary data gathered from the questionnaire produced quantitative and qualitative
evidence. To maintain confidentiality, all results have been attributed and presented
according to respondent’s unique identification numbers, generated by the
questionnaire tool. Where responses have been quoted, these numbers have been
further defined by colour with blue denoting Healthcare Planner’s, green denoting
Construction and red denoting Clients.
In explanation of the three groups identified above, the original four groups were not
directly comparable due to low numbers from three of the groups. Therefore the four
responses from the PSCP group and the seven responses from the non-PSCP group
were combined and renamed as Construction giving a total of eleven responses. This
enabled the eleven construction responses to be directly compared with the eleven
client responses. However, it is recognised that the construction and client groups are
not directly comparable to the significantly larger number of HCP responses (fifty). The
questionnaire was subsequently analysed according to the themes emerging from the
questions, due to the large number of variables within the responses.
The data is subject to the respondent’s self-interpretation of the questions, in order to
explore the qualitative aspects of the hypothesis. It was recognised that this was a
weakness in the data, as it would be difficult to replicate the results.
Notably, sixty percent of HCP respondents were resident outside of the UK and were
not familiar with UK National Frameworks or PSCP’s which meant that they were not
always able to make a direct comparison. It is further acknowledged that the data may
be influenced by industry sensitive considerations and is based on subjective personal
experience.
One hundred and forty one email invitations were distributed over a period of five
weeks. Direct invitation by email proved effective, however the snowball method of
distribution had limitations as unique identification and subsequent confidentiality was
8
reliant upon a direct link to individual email addresses. The snowball method did not
allow for this requirement, resulting in an unidentified number of potential participants
being lost.
Questionnaire Results.
A total of eighty six responses were received, equating to a sixty one percent response
rate. However, fourteen entered their demographics only, equating to sixteen percent
who did not complete. In comparison to an expected response rate of thirty percent
(Neville. 2014, p.33) this questionnaire produced a usable sample of seventy two
responses, which equates to a fifty one percent response rate.
It is observed that the above average response rate may be attributable to the
participants having a “…high degree of interest…” in the research subject. (Sheehan.
2001, p.0) These results have been presented below as group numbers and
percentages in table 1.
Group Number of responses
Construction 11 (15%)
Client 11 (15%)
HCP 50 (70%)
Table 1. Response rate - actual response numbers and percentages by modified grouping. (Dickson. March 2015)
Questions one to five.
Questions one to four explored the demographics of all respondents and question five
funnelled the respondent to a particular pathway within the questionnaire. The decision
of which pathway to take was the personal choice of the respondent, according to their
interpretation of the headings offered and definitions were not provided.
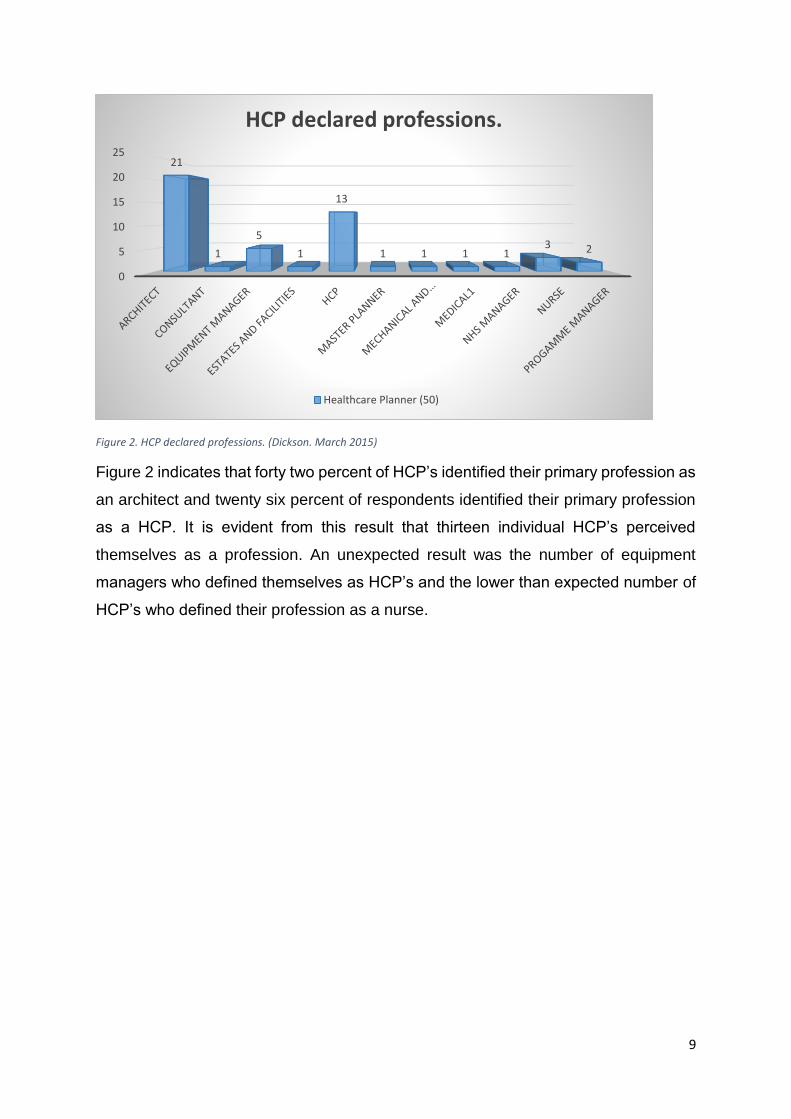
Question one contained multiple sections relating to professional and academic
qualifications. As the focus of this research, the results for HCP’s are presented in
figure 2.
9
Figure 2. HCP declared professions. (Dickson. March 2015)
Figure 2 indicates that forty two percent of HCP’s identified their primary profession as
an architect and twenty six percent of respondents identified their primary profession
as a HCP. It is evident from this result that thirteen individual HCP’s perceived
themselves as a profession. An unexpected result was the number of equipment
managers who defined themselves as HCP’s and the lower than expected number of
HCP’s who defined their profession as a nurse.
0
5
10
15
20
2521
1
5
1
13
1 1 1 13 2
HCP declared professions.
Healthcare Planner (50)
10
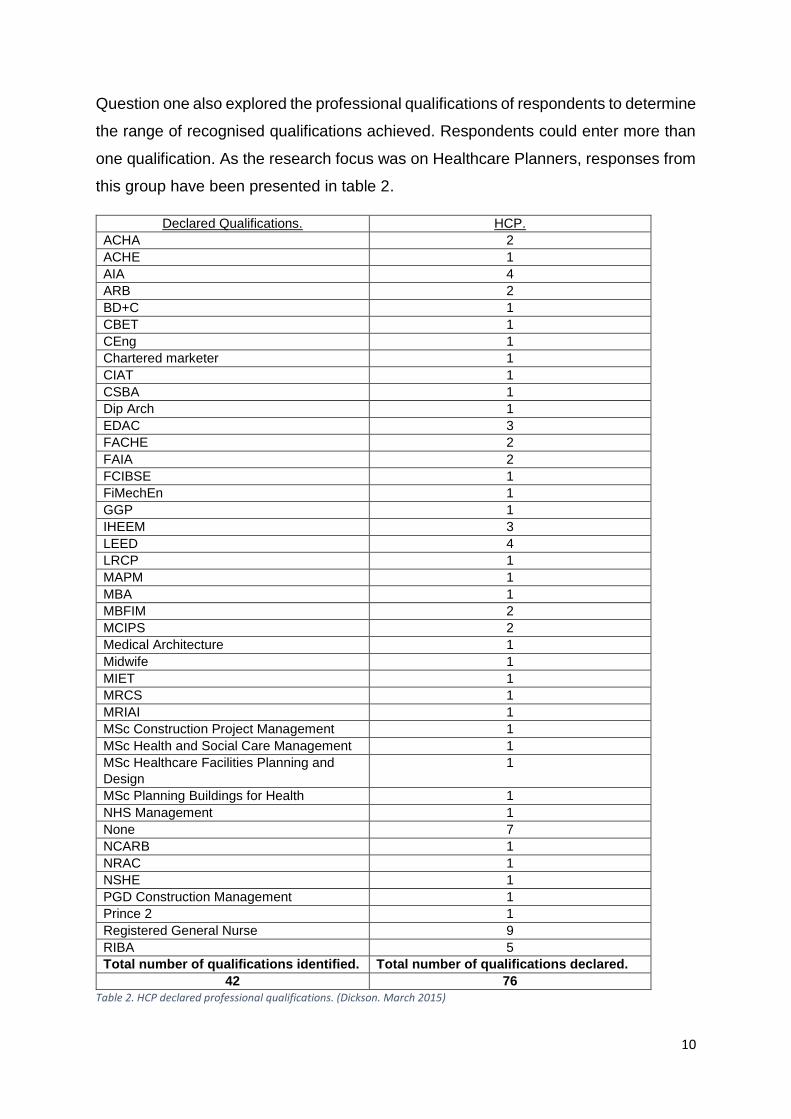
Question one also explored the professional qualifications of respondents to determine
the range of recognised qualifications achieved. Respondents could enter more than
one qualification. As the research focus was on Healthcare Planners, responses from
this group have been presented in table 2.
Declared Qualifications. HCP.
ACHA 2
ACHE 1
AIA 4
ARB 2
BD+C 1
CBET 1
CEng 1
Chartered marketer 1
CIAT 1
CSBA 1
Dip Arch 1
EDAC 3
FACHE 2
FAIA 2
FCIBSE 1
FiMechEn 1
GGP 1
IHEEM 3
LEED 4
LRCP 1
MAPM 1
MBA 1
MBFIM 2
MCIPS 2
Medical Architecture 1
Midwife 1
MIET 1
MRCS 1
MRIAI 1
MSc Construction Project Management 1
MSc Health and Social Care Management 1
MSc Healthcare Facilities Planning and
Design
1
MSc Planning Buildings for Health 1
NHS Management 1
None 7
NCARB 1
NRAC 1
NSHE 1
PGD Construction Management 1
Prince 2 1
Registered General Nurse 9
RIBA 5
Total number of qualifications identified. Total number of qualifications declared.
42 76
Table 2. HCP declared professional qualifications. (Dickson. March 2015)
11
The results in table 2 reveal a wide variety of qualifications, with many HCP’s having
more than one industry recognised qualification. An unexpected result was that
seven respondents identified that they held no professional or academic
qualification.
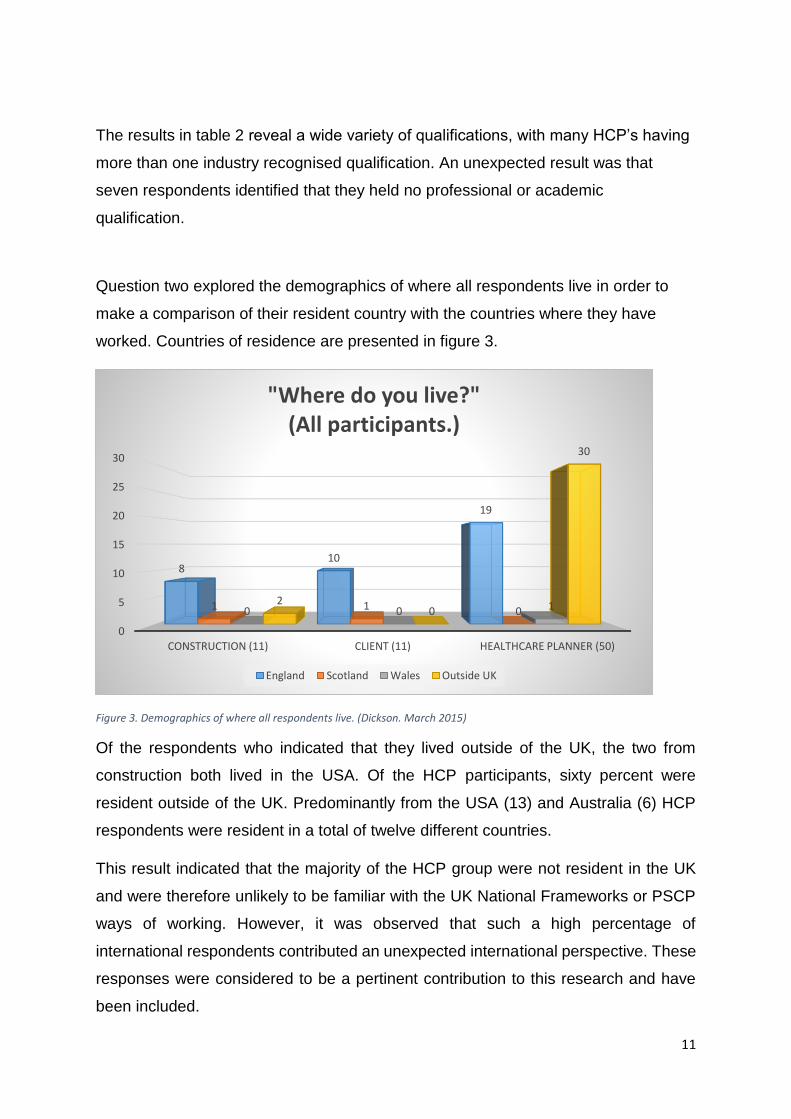
Question two explored the demographics of where all respondents live in order to
make a comparison of their resident country with the countries where they have
worked. Countries of residence are presented in figure 3.
Figure 3. Demographics of where all respondents live. (Dickson. March 2015)
Of the respondents who indicated that they lived outside of the UK, the two from
construction both lived in the USA. Of the HCP participants, sixty percent were
resident outside of the UK. Predominantly from the USA (13) and Australia (6) HCP
respondents were resident in a total of twelve different countries.
This result indicated that the majority of the HCP group were not resident in the UK
and were therefore unlikely to be familiar with the UK National Frameworks or PSCP
ways of working. However, it was observed that such a high percentage of
international respondents contributed an unexpected international perspective. These
responses were considered to be a pertinent contribution to this research and have
been included.
0
5
10
15
20
25
30
CONSTRUCTION (11) CLIENT (11) HEALTHCARE PLANNER (50)
810
19
1 1 00 0 120
30
"Where do you live?"(All participants.)
England Scotland Wales Outside UK
12
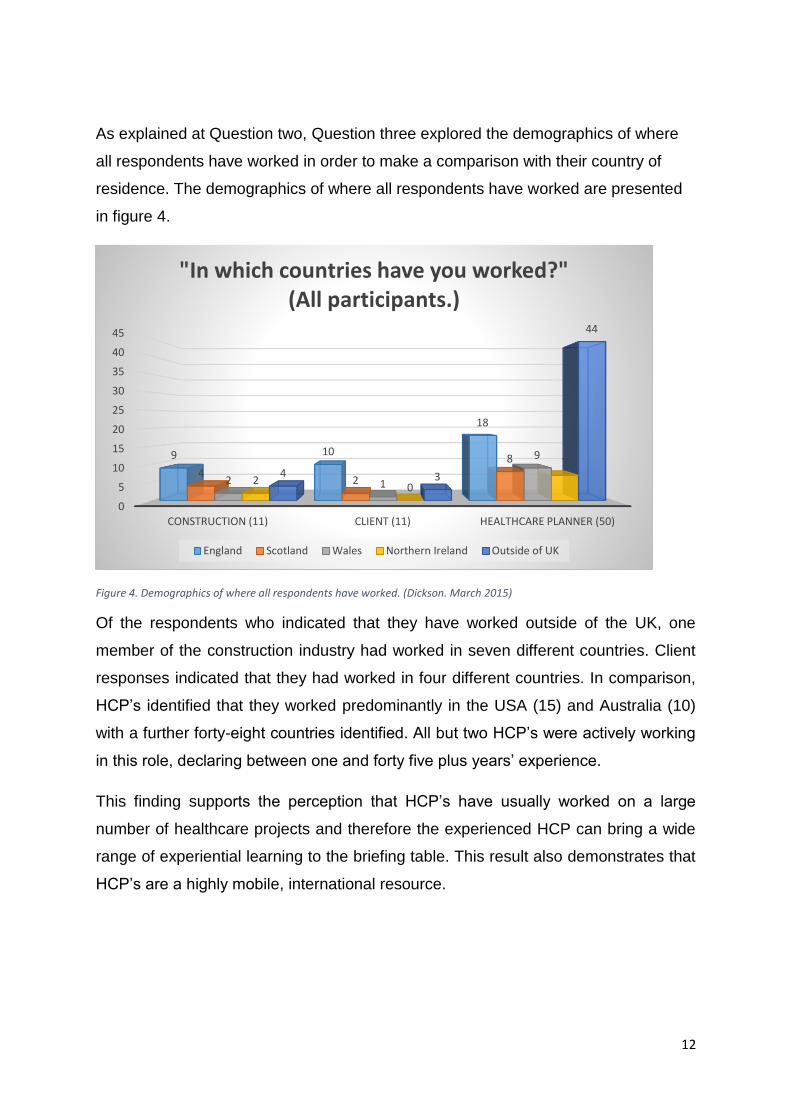
As explained at Question two, Question three explored the demographics of where
all respondents have worked in order to make a comparison with their country of
residence. The demographics of where all respondents have worked are presented
in figure 4.
Figure 4. Demographics of where all respondents have worked. (Dickson. March 2015)
Of the respondents who indicated that they have worked outside of the UK, one
member of the construction industry had worked in seven different countries. Client
responses indicated that they had worked in four different countries. In comparison,
HCP’s identified that they worked predominantly in the USA (15) and Australia (10)
with a further forty-eight countries identified. All but two HCP’s were actively working
in this role, declaring between one and forty five plus years’ experience.
This finding supports the perception that HCP’s have usually worked on a large
number of healthcare projects and therefore the experienced HCP can bring a wide
range of experiential learning to the briefing table. This result also demonstrates that
HCP’s are a highly mobile, international resource.
0
5
10
15
20
25
30
35
40
45
CONSTRUCTION (11) CLIENT (11) HEALTHCARE PLANNER (50)
9 10
18
42
8
2 1
9
20
74 3
44
"In which countries have you worked?"(All participants.)
England Scotland Wales Northern Ireland Outside of UK
13
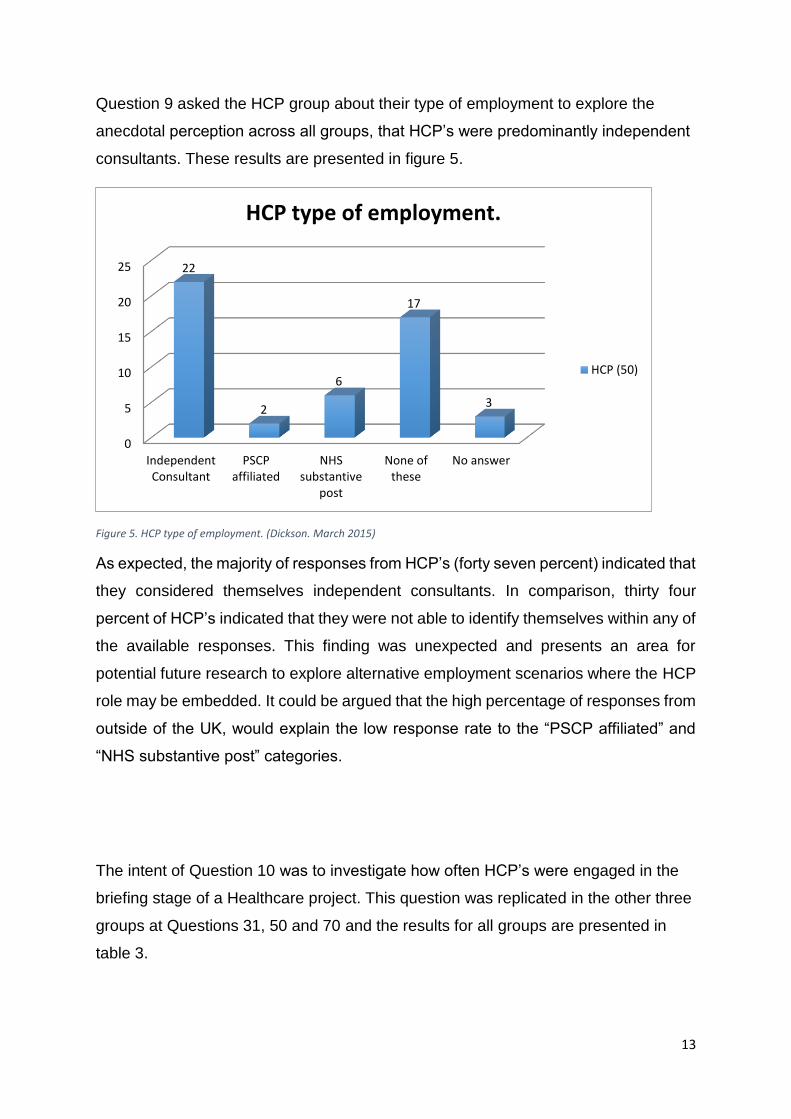
Question 9 asked the HCP group about their type of employment to explore the
anecdotal perception across all groups, that HCP’s were predominantly independent
consultants. These results are presented in figure 5.
Figure 5. HCP type of employment. (Dickson. March 2015)
As expected, the majority of responses from HCP’s (forty seven percent) indicated that
they considered themselves independent consultants. In comparison, thirty four
percent of HCP’s indicated that they were not able to identify themselves within any of
the available responses. This finding was unexpected and presents an area for
potential future research to explore alternative employment scenarios where the HCP
role may be embedded. It could be argued that the high percentage of responses from
outside of the UK, would explain the low response rate to the “PSCP affiliated” and
“NHS substantive post” categories.
The intent of Question 10 was to investigate how often HCP’s were engaged in the
briefing stage of a Healthcare project. This question was replicated in the other three
groups at Questions 31, 50 and 70 and the results for all groups are presented in
table 3.
0
5
10
15
20
25
IndependentConsultant
PSCPaffiliated
NHSsubstantive
post
None ofthese
No answer
22
2
6
17
3
HCP type of employment.
HCP (50)
14
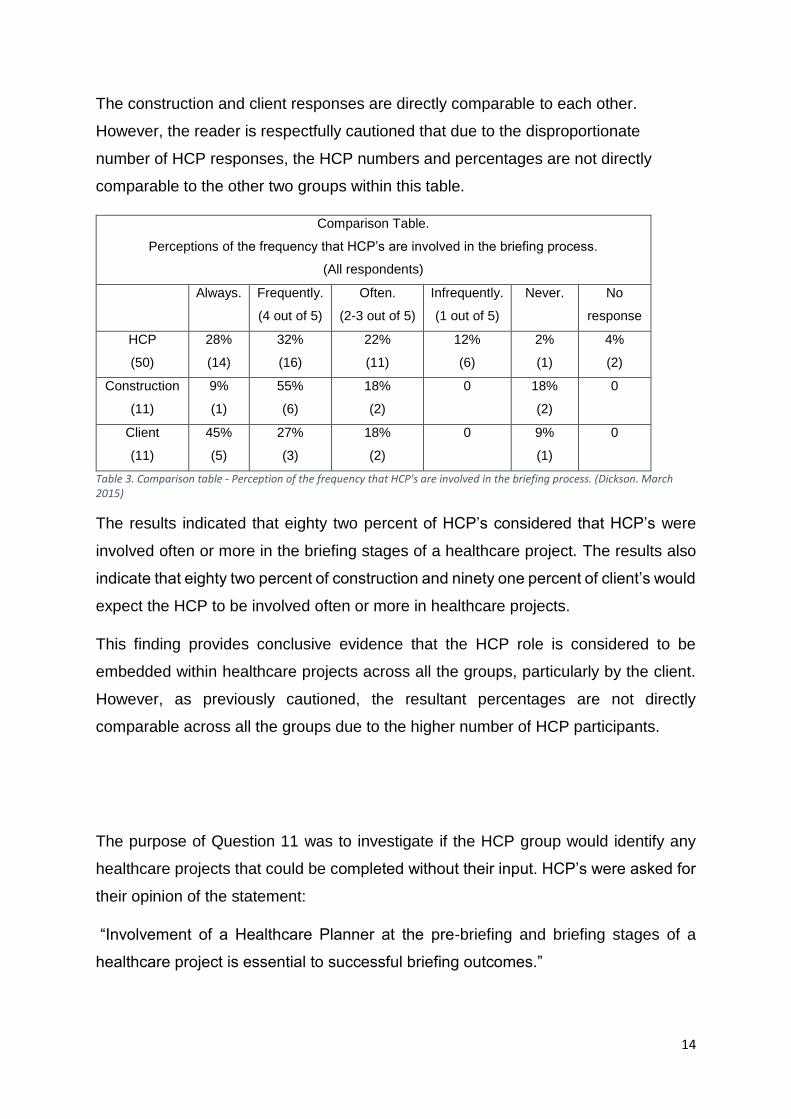
The construction and client responses are directly comparable to each other.
However, the reader is respectfully cautioned that due to the disproportionate
number of HCP responses, the HCP numbers and percentages are not directly
comparable to the other two groups within this table.
Comparison Table.
Perceptions of the frequency that HCP’s are involved in the briefing process.
(All respondents)
Always. Frequently.
(4 out of 5)
Often.
(2-3 out of 5)
Infrequently.
(1 out of 5)
Never. No
response
HCP
(50)
28%
(14)
32%
(16)
22%
(11)
12%
(6)
2%
(1)
4%
(2)
Construction
(11)
9%
(1)
55%
(6)
18%
(2)
0 18%
(2)
0
Client
(11)
45%
(5)
27%
(3)
18%
(2)
0 9%
(1)
0
Table 3. Comparison table - Perception of the frequency that HCP's are involved in the briefing process. (Dickson. March 2015)
The results indicated that eighty two percent of HCP’s considered that HCP’s were
involved often or more in the briefing stages of a healthcare project. The results also
indicate that eighty two percent of construction and ninety one percent of client’s would
expect the HCP to be involved often or more in healthcare projects.
This finding provides conclusive evidence that the HCP role is considered to be
embedded within healthcare projects across all the groups, particularly by the client.
However, as previously cautioned, the resultant percentages are not directly
comparable across all the groups due to the higher number of HCP participants.
The purpose of Question 11 was to investigate if the HCP group would identify any
healthcare projects that could be completed without their input. HCP’s were asked for
their opinion of the statement:
“Involvement of a Healthcare Planner at the pre-briefing and briefing stages of a
healthcare project is essential to successful briefing outcomes.”
15
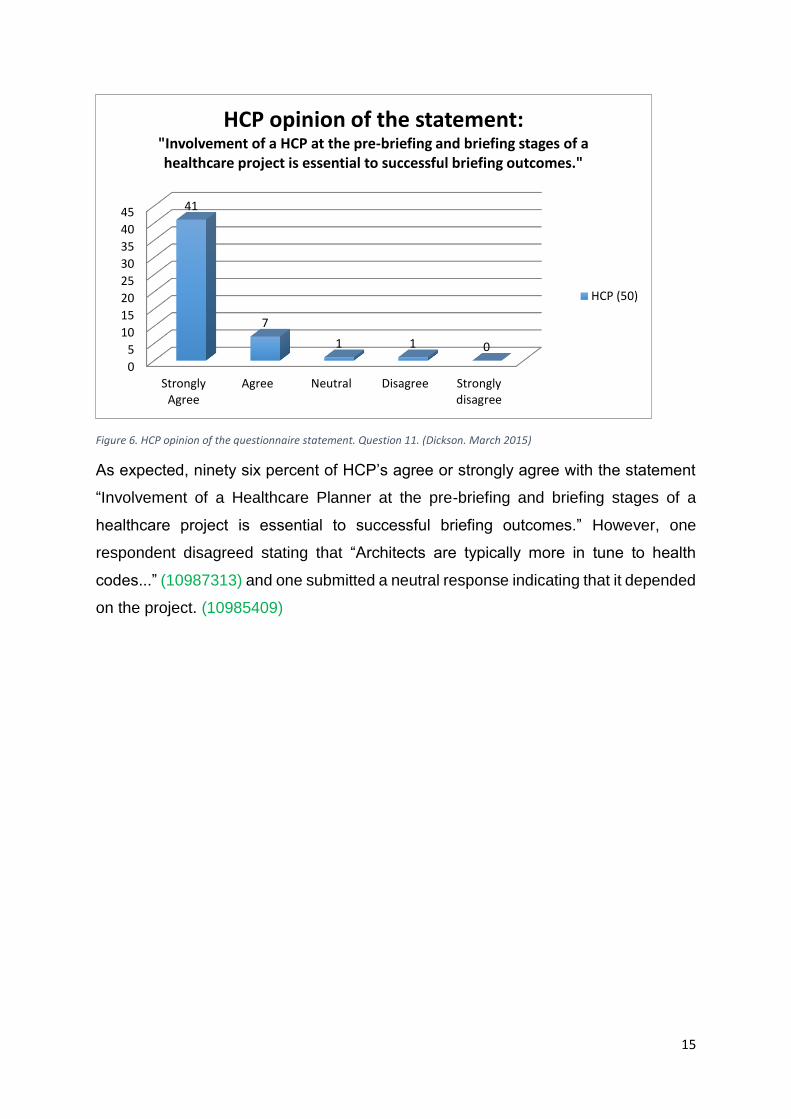
Figure 6. HCP opinion of the questionnaire statement. Question 11. (Dickson. March 2015)
As expected, ninety six percent of HCP’s agree or strongly agree with the statement
“Involvement of a Healthcare Planner at the pre-briefing and briefing stages of a
healthcare project is essential to successful briefing outcomes.” However, one
respondent disagreed stating that “Architects are typically more in tune to health
codes...” (10987313) and one submitted a neutral response indicating that it depended
on the project. (10985409)
0
5
10
15
20
25
30
35
40
45
StronglyAgree
Agree Neutral Disagree Stronglydisagree
41
7
1 1 0
HCP opinion of the statement:"Involvement of a HCP at the pre-briefing and briefing stages of a healthcare project is essential to successful briefing outcomes."
HCP (50)
16
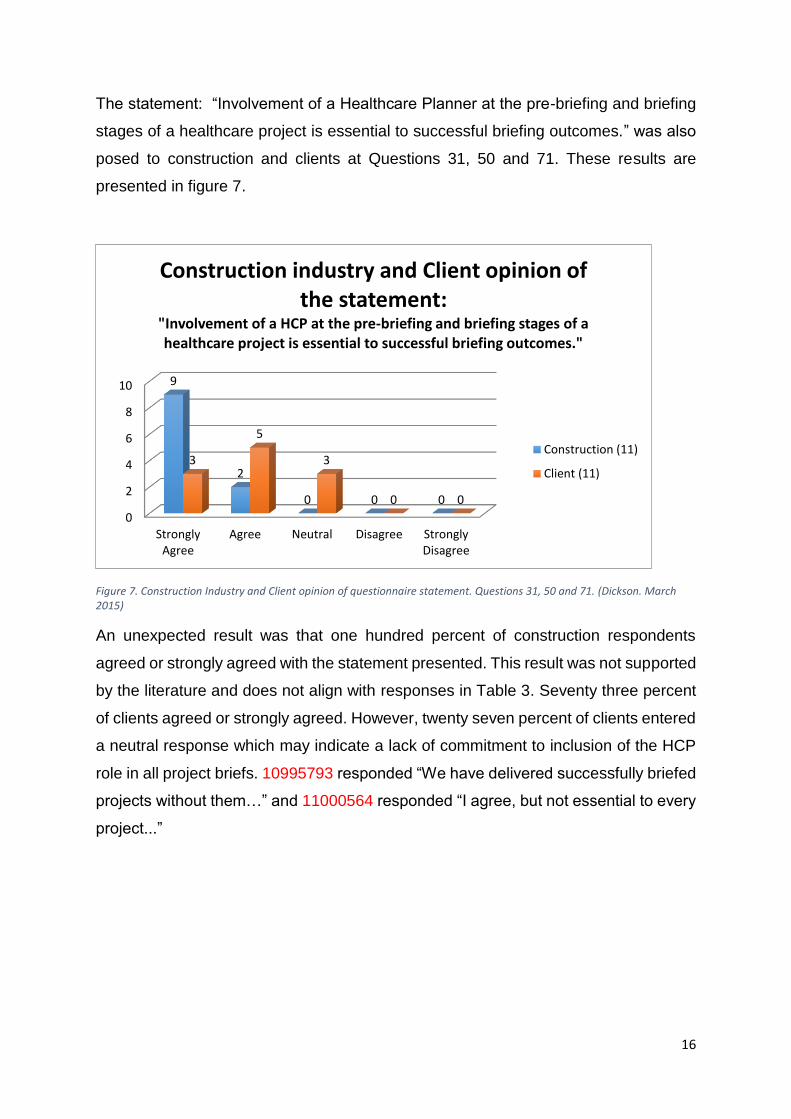
The statement: “Involvement of a Healthcare Planner at the pre-briefing and briefing
stages of a healthcare project is essential to successful briefing outcomes.” was also
posed to construction and clients at Questions 31, 50 and 71. These results are
presented in figure 7.
Figure 7. Construction Industry and Client opinion of questionnaire statement. Questions 31, 50 and 71. (Dickson. March 2015)
An unexpected result was that one hundred percent of construction respondents
agreed or strongly agreed with the statement presented. This result was not supported
by the literature and does not align with responses in Table 3. Seventy three percent
of clients agreed or strongly agreed. However, twenty seven percent of clients entered
a neutral response which may indicate a lack of commitment to inclusion of the HCP
role in all project briefs. 10995793 responded “We have delivered successfully briefed
projects without them…” and 11000564 responded “I agree, but not essential to every
project...”
0
2
4
6
8
10
StronglyAgree
Agree Neutral Disagree StronglyDisagree
9
2
0 0 0
3
5
3
0 0
Construction industry and Client opinion of the statement:
"Involvement of a HCP at the pre-briefing and briefing stages of a healthcare project is essential to successful briefing outcomes."
Construction (11)
Client (11)

17
Within Questions 12, 42, 51 and 72 a list of activities undertaken by HCP’s was
provided. These activities were selected from the most frequently identified activities
of briefing in the literature. The responses from HCP’s, construction and the client have
been presented in figures 8, 9 and 10 below. A short summary of individual group
results follows each figure. The findings from all the groups are presented after figure
10.
At Question 12, the HCP was asked to identify all of the listed activities that they had
engaged in during the briefing stages of a healthcare project and were able to select
multiple activities. The intention of this question was to identify the activities most
frequently undertaken by HCP’s within the briefing process.
Figure 8. HCP declared activities from list provided. (Dickson. March 2015)
Two HCP respondents did not answer this question.
As expected the main briefing activities undertaken by HCP’s were related to
Adjacency Planning, Design Review, Functional Briefing and Presentations to
clients. The results indicate that the activity undertaken the least by HCP’s was the
Estates Strategy, although twenty one respondents (thirty six percent) had been
involved in this activity.
28
41
23
35
2327
31
42
18
37
21
43
3431
25
3642
23
3135
3226
36
05
101520253035404550
Act
ivit
y M
od
ellin
g
Ad
jace
ncy
Pla
nn
ing
Car
e P
ath
way
Mo
del
ling
Clie
nt
Wo
rksh
op
s
Clin
ical
Bri
efin
g
Clin
ical
Str
ateg
y
Dem
and
an
d C
apac
ity…
Des
ign
Re
view
Esta
tes
Stra
tegy
Feas
ibili
ty S
tud
ies
Full
Bu
sin
ess
Cas
e
Fun
ctio
nal
Bri
efin
g
Intr
od
uce
ne
w w
ays
of…
Op
tio
n A
pp
rais
als
Ou
tlin
e B
usi
nes
s C
ase
Pat
ien
t P
ath
way
…
Pre
sen
tati
on
s to
Clie
nts
Ris
k M
anag
eme
nt
Sch
edu
les
of…
Spat
ial A
nal
ysis
Stak
eho
lder
…
Stra
tegi
c B
usi
ne
ss C
ase
Stra
tegi
c P
lan
nin
g
HCP (50) Declared Activities. (From list provided in questionnaire)
18
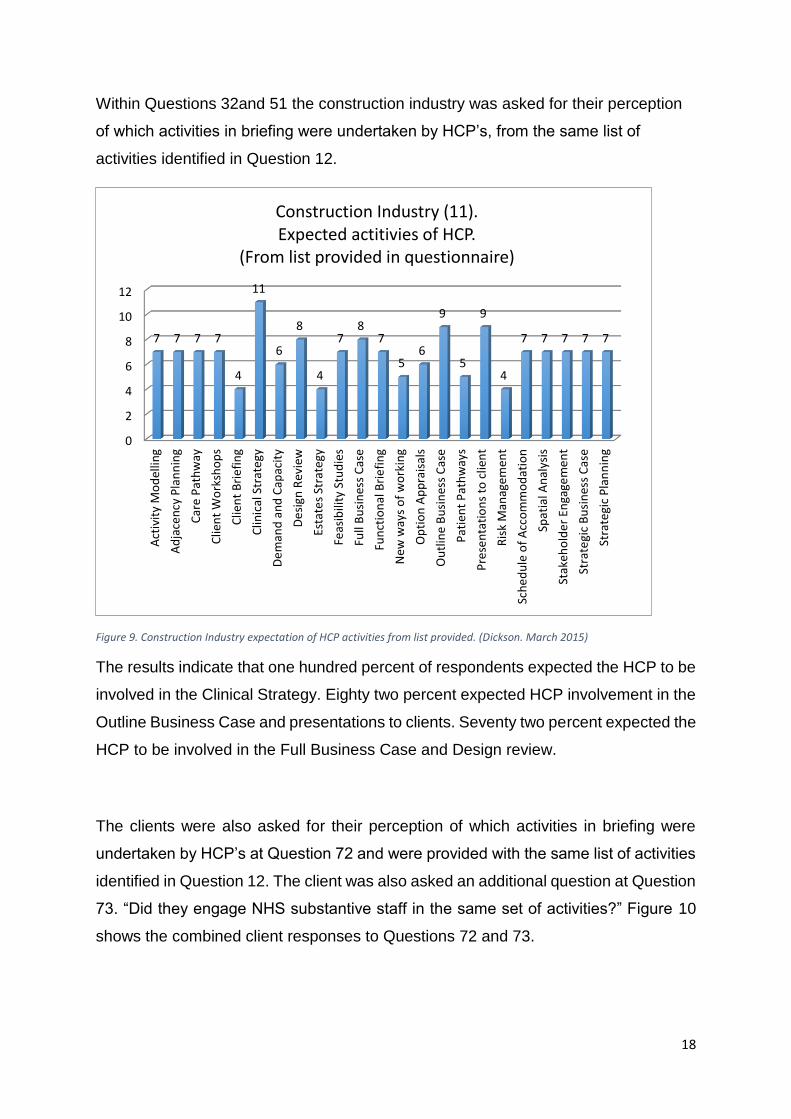
Within Questions 32and 51 the construction industry was asked for their perception
of which activities in briefing were undertaken by HCP’s, from the same list of
activities identified in Question 12.
Figure 9. Construction Industry expectation of HCP activities from list provided. (Dickson. March 2015)
The results indicate that one hundred percent of respondents expected the HCP to be
involved in the Clinical Strategy. Eighty two percent expected HCP involvement in the
Outline Business Case and presentations to clients. Seventy two percent expected the
HCP to be involved in the Full Business Case and Design review.
The clients were also asked for their perception of which activities in briefing were
undertaken by HCP’s at Question 72 and were provided with the same list of activities
identified in Question 12. The client was also asked an additional question at Question
73. “Did they engage NHS substantive staff in the same set of activities?” Figure 10
shows the combined client responses to Questions 72 and 73.
0
2
4
6
8
10
12
Act
ivit
y M
od
ellin
g
Ad
jace
ncy
Pla
nn
ing
Car
e P
ath
way
Clie
nt
Wo
rksh
op
s
Clie
nt
Bri
efi
ng
Clin
ical
Str
ateg
y
De
man
d a
nd
Cap
acit
y
De
sign
Rev
iew
Esta
tes
Stra
tegy
Feas
ibili
ty S
tud
ies
Full
Bu
sin
ess
Cas
e
Fun
ctio
nal
Bri
efi
ng
New
way
s o
f w
ork
ing
Op
tio
n A
pp
rais
als
Ou
tlin
e B
usi
nes
s C
ase
Pat
ien
t P
ath
way
s
Pre
sen
tati
on
s to
clie
nt
Ris
k M
anag
emen
t
Sch
ed
ule
of
Acc
om
mo
dat
ion
Spat
ial A
nal
ysis
Stak
eho
lde
r En
gage
me
nt
Stra
tegi
c B
usi
nes
s C
ase
Stra
tegi
c P
lan
nin
g
7 7 7 7
4
11
6
8
4
78
7
56
9
5
9
4
7 7 7 7 7
Construction Industry (11). Expected actitivies of HCP.
(From list provided in questionnaire)

19
Figure 10. Client expectation in briefing activities from HCP and substantive staff. (Dickson. March 2015)
The results indicate that seventy three percent of clients expected the HCP to be
involved in Activity Modelling and Demand and Capacity Modelling. Sixty four percent
expected the HCP to be involved in Care Pathway Modelling, Client Workshops,
Design Review, Functional Briefing, introducing new ways of working, Outline
Business Case, Patient pathway redesign and Presentations to clients.
In comparison, figure 10 also identified where clients are utilising their substantive staff
to undertake activities in healthcare projects. Ninety six percent of clients identified
that they used substantive staff, to variable degree, across all the activities presented.
The results show that eighty two percent of clients engage their own staff for Outline
Business Cases (OBC), Stakeholder Engagement and Strategic Business Cases
(SBC). Seventy two percent of clients also use their own staff for Adjacency Planning,
Care Pathway Modelling, Client Workshops, Full Business Cases and Presentations
to clients. However, two clients indicated that they do not use substantive staff in any
of the activities presented in the questionnaire.
8
67 7
5 5
87
4
6 67 7
67 7 7
1
65
6 6
3
78 8 8
56
7 76 6
87
6 6
9
78
7
5 5
9 9
7
0123456789
10
Act
ivit
y M
od
ellin
g
Ad
jace
ncy
Pla
nn
ing
Car
e P
ath
way
Mo
del
ling
Clie
nt
Wo
rksh
op
s
Clin
ical
Bri
efin
g
Clin
ical
Str
ateg
y
Dem
and
an
d C
apac
ity…
Des
ign
Re
view
Esta
tes
Stra
tegy
Feas
ibili
ty S
tud
ies
Full
Bu
sin
ess
Cas
e
Fun
ctio
nal
Bri
efin
g
Intr
od
uce
ne
w w
ays
of…
Op
tio
n A
pp
rais
als
Ou
tlin
e B
usi
nes
s C
ase
Pat
ien
t P
ath
way
Re
des
ign
Pre
sen
tati
on
s to
Clie
nts
Ris
k M
anag
eme
nt
Sch
edu
les
of…
Spat
ial A
nal
ysis
Stak
eho
lder
En
gage
men
t
Stra
tegi
c B
usi
ne
ss C
ase
Stra
tegi
c P
lan
nin
g
Client perception (11). Expected Activities undertaken by HCP (blue) and
substantive staff (orange). (From list provided in questionnaire)
20
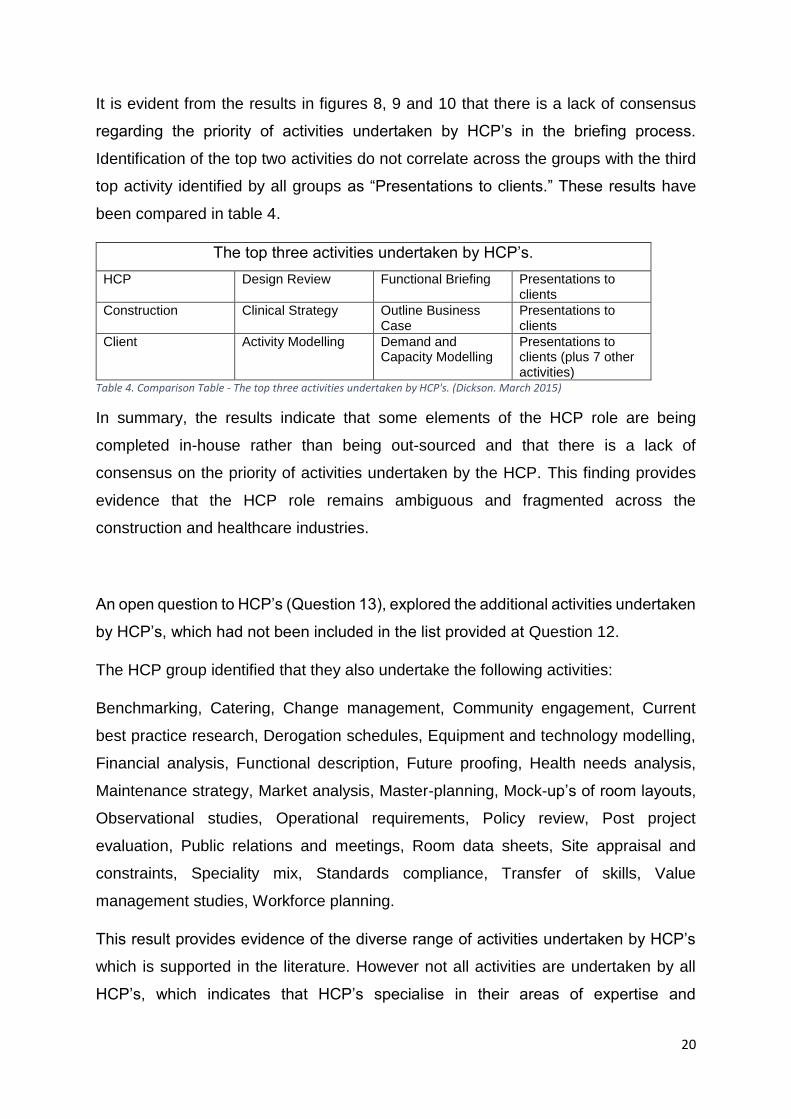
It is evident from the results in figures 8, 9 and 10 that there is a lack of consensus
regarding the priority of activities undertaken by HCP’s in the briefing process.
Identification of the top two activities do not correlate across the groups with the third
top activity identified by all groups as “Presentations to clients.” These results have
been compared in table 4.
The top three activities undertaken by HCP’s.
HCP Design Review Functional Briefing Presentations to clients
Construction Clinical Strategy Outline Business Case
Presentations to clients
Client Activity Modelling Demand and Capacity Modelling
Presentations to clients (plus 7 other activities)
Table 4. Comparison Table - The top three activities undertaken by HCP's. (Dickson. March 2015)
In summary, the results indicate that some elements of the HCP role are being
completed in-house rather than being out-sourced and that there is a lack of
consensus on the priority of activities undertaken by the HCP. This finding provides
evidence that the HCP role remains ambiguous and fragmented across the
construction and healthcare industries.
An open question to HCP’s (Question 13), explored the additional activities undertaken
by HCP’s, which had not been included in the list provided at Question 12.
The HCP group identified that they also undertake the following activities:
Benchmarking, Catering, Change management, Community engagement, Current
best practice research, Derogation schedules, Equipment and technology modelling,
Financial analysis, Functional description, Future proofing, Health needs analysis,
Maintenance strategy, Market analysis, Master-planning, Mock-up’s of room layouts,
Observational studies, Operational requirements, Policy review, Post project
evaluation, Public relations and meetings, Room data sheets, Site appraisal and
constraints, Speciality mix, Standards compliance, Transfer of skills, Value
management studies, Workforce planning.
This result provides evidence of the diverse range of activities undertaken by HCP’s
which is supported in the literature. However not all activities are undertaken by all
HCP’s, which indicates that HCP’s specialise in their areas of expertise and
21
experience. It can be argued that this further fragments the role of the HCP within the
construction and healthcare industries.
The next three tables (tables 5, 6 and 7) investigated the three group’s perceptions of
where the HCP role is recognised within the project team. They have been presented
sequentially by grouping, with a summary of the results following table 7.
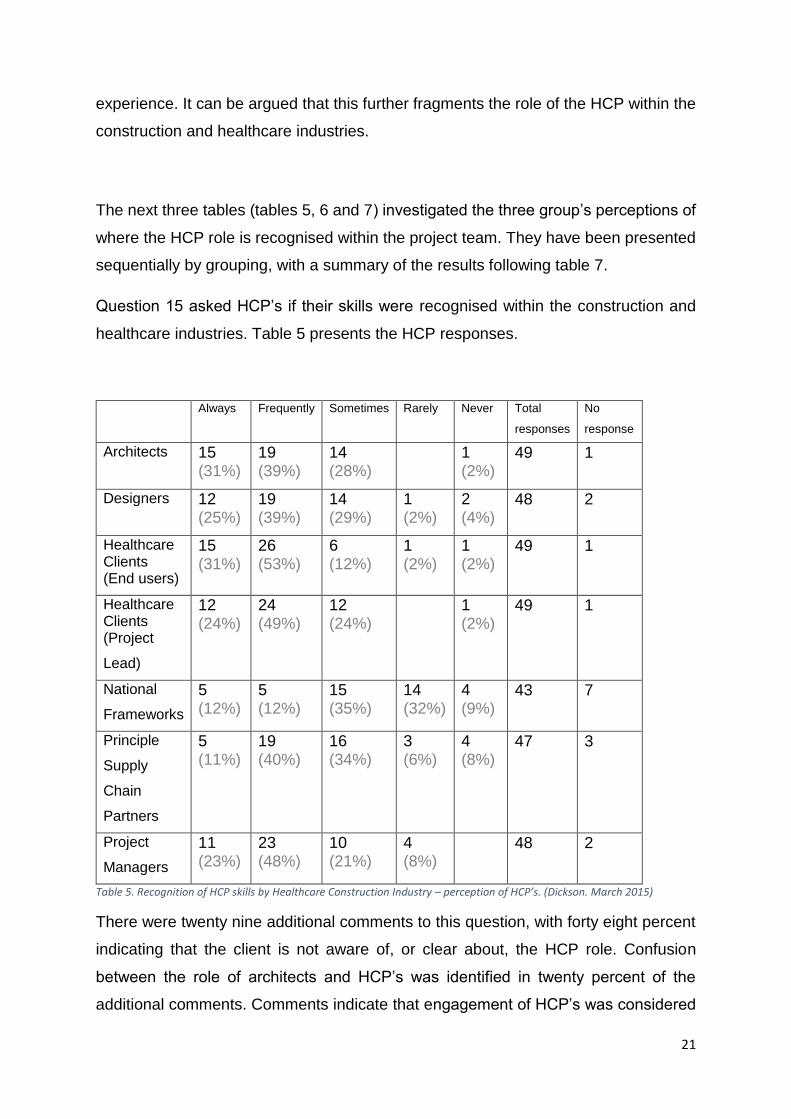
Question 15 asked HCP’s if their skills were recognised within the construction and
healthcare industries. Table 5 presents the HCP responses.
Always Frequently Sometimes Rarely Never Total
responses
No
response
Architects 15 (31%)
19 (39%)
14 (28%)
1 (2%)
49 1
Designers 12 (25%)
19 (39%)
14 (29%)
1 (2%)
2 (4%)
48 2
Healthcare Clients (End users)
15 (31%)
26 (53%)
6 (12%)
1 (2%)
1 (2%)
49 1
Healthcare Clients (Project
Lead)
12 (24%)
24 (49%)
12 (24%)
1 (2%)
49 1
National
Frameworks
5 (12%)
5 (12%)
15 (35%)
14 (32%)
4 (9%)
43 7
Principle
Supply
Chain
Partners
5 (11%)
19 (40%)
16 (34%)
3 (6%)
4 (8%)
47 3
Project
Managers
11 (23%)
23 (48%)
10 (21%)
4 (8%)
48 2
Table 5. Recognition of HCP skills by Healthcare Construction Industry – perception of HCP’s. (Dickson. March 2015)
There were twenty nine additional comments to this question, with forty eight percent
indicating that the client is not aware of, or clear about, the HCP role. Confusion
between the role of architects and HCP’s was identified in twenty percent of the
additional comments. Comments indicate that engagement of HCP’s was considered
22
to be dependent upon the client or project team having previous experience of the
HCP role in seventeen percent of responses.
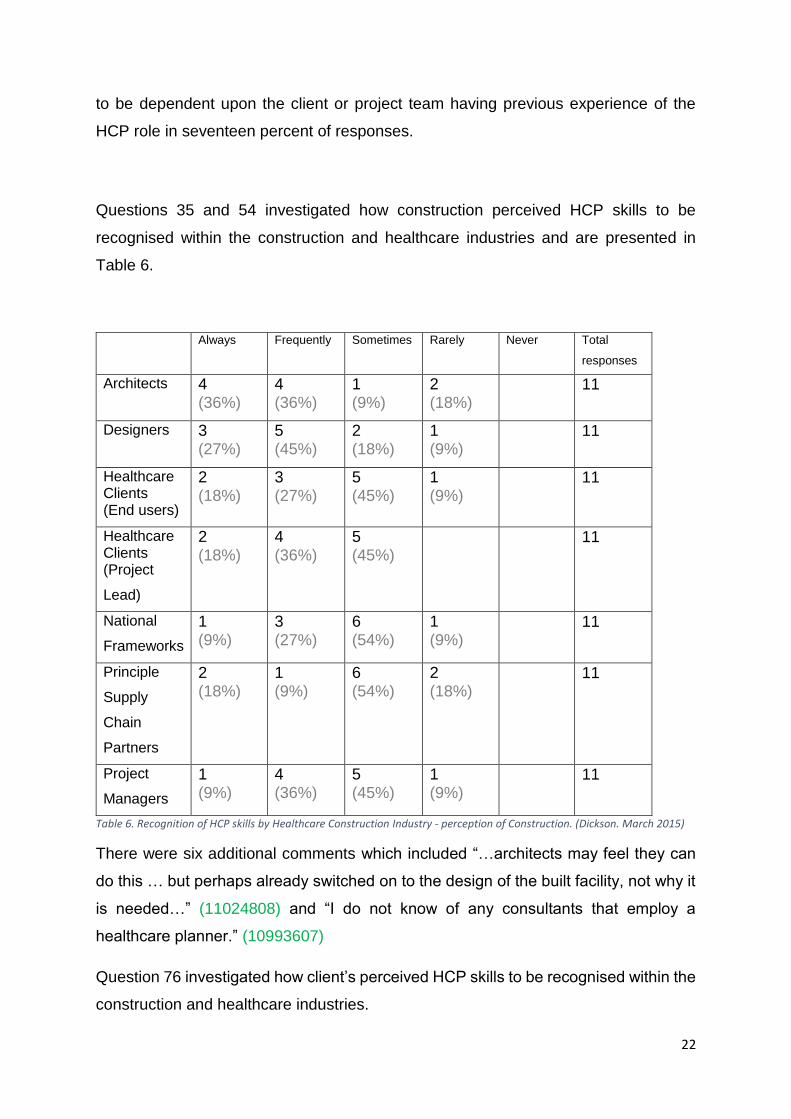
Questions 35 and 54 investigated how construction perceived HCP skills to be
recognised within the construction and healthcare industries and are presented in
Table 6.
Always Frequently Sometimes Rarely Never Total
responses
Architects 4 (36%)
4 (36%)
1 (9%)
2 (18%)
11
Designers 3 (27%)
5 (45%)
2 (18%)
1 (9%)
11
Healthcare Clients (End users)
2 (18%)
3 (27%)
5 (45%)
1 (9%)
11
Healthcare Clients (Project
Lead)
2 (18%)
4 (36%)
5 (45%)
11
National
Frameworks
1 (9%)
3 (27%)
6 (54%)
1 (9%)
11
Principle
Supply
Chain
Partners
2 (18%)
1 (9%)
6 (54%)
2 (18%)
11
Project
Managers
1 (9%)
4 (36%)
5 (45%)
1 (9%)
11
Table 6. Recognition of HCP skills by Healthcare Construction Industry - perception of Construction. (Dickson. March 2015)
There were six additional comments which included “…architects may feel they can
do this … but perhaps already switched on to the design of the built facility, not why it
is needed…” (11024808) and “I do not know of any consultants that employ a
healthcare planner.” (10993607)
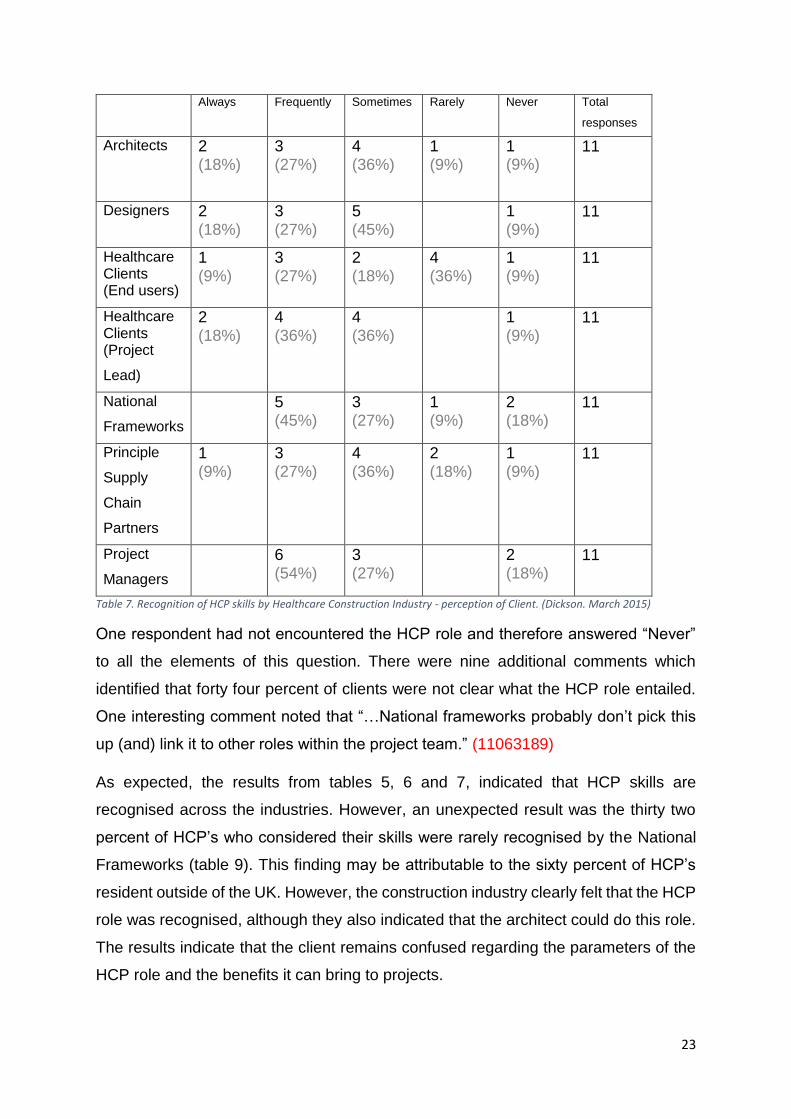
Question 76 investigated how client’s perceived HCP skills to be recognised within the
construction and healthcare industries.
23
Always Frequently Sometimes Rarely Never Total
responses
Architects 2 (18%)
3 (27%)
4 (36%)
1 (9%)
1 (9%)
11
Designers 2 (18%)
3 (27%)
5 (45%)
1 (9%)
11
Healthcare Clients (End users)
1 (9%)
3 (27%)
2 (18%)
4 (36%)
1 (9%)
11
Healthcare Clients (Project
Lead)
2 (18%)
4 (36%)
4 (36%)
1 (9%)
11
National
Frameworks
5 (45%)
3 (27%)
1 (9%)
2 (18%)
11
Principle
Supply
Chain
Partners
1 (9%)
3 (27%)
4 (36%)
2 (18%)
1 (9%)
11
Project
Managers
6 (54%)
3 (27%)
2 (18%)
11
Table 7. Recognition of HCP skills by Healthcare Construction Industry - perception of Client. (Dickson. March 2015)
One respondent had not encountered the HCP role and therefore answered “Never”
to all the elements of this question. There were nine additional comments which
identified that forty four percent of clients were not clear what the HCP role entailed.
One interesting comment noted that “…National frameworks probably don’t pick this
up (and) link it to other roles within the project team.” (11063189)
As expected, the results from tables 5, 6 and 7, indicated that HCP skills are
recognised across the industries. However, an unexpected result was the thirty two
percent of HCP’s who considered their skills were rarely recognised by the National
Frameworks (table 9). This finding may be attributable to the sixty percent of HCP’s
resident outside of the UK. However, the construction industry clearly felt that the HCP
role was recognised, although they also indicated that the architect could do this role.
The results indicate that the client remains confused regarding the parameters of the
HCP role and the benefits it can bring to projects.
24
Question 16, 36, 55, 77 was an open question which asked all three groups “What do
you think could raise the profile of HCP’s to the client on healthcare projects?” It was
possible to enter up to five responses in this question.
There were one hundred and ten HCP comments to this question with the top themes
emerging as publishing and marketing (fifteen percent), evidence and demonstrate
skills (sixteen percent), establishment of a professional body or qualification (eleven
percent) and personal contact (ten percent). Thirty six construction comments were
received indicating that quantitative evidence was required (seventeen percent) and a
professional qualification would assist in raising the HCP profile (eleven percent). The
client group provided thirty additional responses which indicated the top themes for
this group to be a clear definition of the role (twenty three percent) followed by
evidence of benefits achieved (seventeen percent) and increased contact with the
client (seventeen percent).
It is observed from these comments that the client appears to be seeking clarity on the
role along with quantifiable evidence of the benefits to the project. The HCP and client
groups both identify that more direct contact would be beneficial to them. The
construction industry and HCP’s agree with the clients, that more quantitative evidence
is required, going on to say that this should be published and presented in various
forums. The construction and HCP groups indicate that some sort of professional
group or recognised qualification would assist in raising the profile of the HCP.
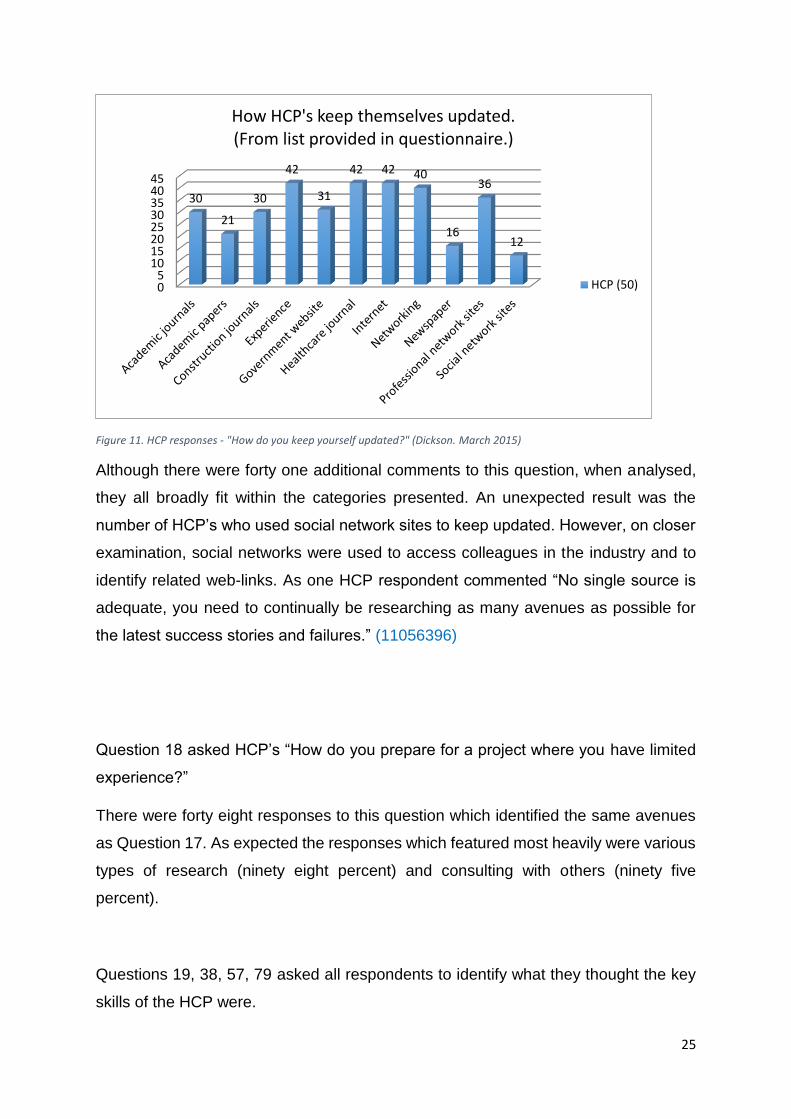
Question 17 asked the HCP “How do you keep yourself updated with
National/Regional/Local developments in healthcare projects?” to explore the
avenues and mediums most commonly used. Responses are presented in figure 11.
25
Figure 11. HCP responses - "How do you keep yourself updated?" (Dickson. March 2015)
Although there were forty one additional comments to this question, when analysed,
they all broadly fit within the categories presented. An unexpected result was the
number of HCP’s who used social network sites to keep updated. However, on closer
examination, social networks were used to access colleagues in the industry and to
identify related web-links. As one HCP respondent commented “No single source is
adequate, you need to continually be researching as many avenues as possible for
the latest success stories and failures.” (11056396)
Question 18 asked HCP’s “How do you prepare for a project where you have limited
experience?”
There were forty eight responses to this question which identified the same avenues
as Question 17. As expected the responses which featured most heavily were various
types of research (ninety eight percent) and consulting with others (ninety five
percent).
Questions 19, 38, 57, 79 asked all respondents to identify what they thought the key
skills of the HCP were.
05
1015202530354045
30
21
30
42
31
42 42 40
16
36
12
How HCP's keep themselves updated.(From list provided in questionnaire.)
HCP (50)
26
Within the HCP group, four percent identified quantitative skills which included: time,
evidence based design, knowledge of building limitations and opportunities,
knowledge of guidance and HBN’s and knowledge of clinical pathways. As expected,
ninety six percent of this group referred to qualitative aspects of their role, such as
understanding of various elements, experience of multiple projects, ability to achieve,
review or challenge, and an objective or independent view.
The construction group generally matched the HCP percentages of quantitative
compared to qualitative responses. This group also identified standardisation of design
as a quantitative skill.
As expected, thirty two percent of the client group were more focused on the
quantitative skills such as project management, legislation, demand and capacity
modelling, building knowledge and expertise in specialist design.
These results suggest that the client is seeking evidence that the HCP role brings
measureable benefits to the project and are perhaps not recognising the qualitative
aspects of the HCP role to the same extent as the other two groups.
Questions 20, 39, 58, 80 asked all groups what personal characteristics were required
by HCP’s.
As expected all groups placed communication and negotiation skills extremely high.
However, recurring characteristics identified by all groups also included patience and
tenacity, confidence and diplomacy, and the ability to listen.
Question 21, 40, 59, 81 asked all groups how they thought HCP’s could demonstrate
that their contribution had enhanced the project outcomes. Respondents were able to
enter up to five activities.
Surprisingly, the HCP group identified a relatively small number of quantifiable
outcomes, which included keeping to schedule, meeting budget and brief parameters,
reduced number of changes within the brief and flexible space. Construction appeared
to find this question easier to quantify, relating their responses to budget measures,
reduction and efficiency of space, compliance with guidance and early clinical sign-
27
off. The client groups related their responses to reductions in variations within the
scheme and reductions in time, which are also quantifiable measures.
Unexpectedly, the clients identified post-project evaluations and a reduction in whole
life costs as quantifiable measures, which had not been mentioned by the HCP’s or
construction. All of the groups mentioned patient or staff satisfaction as measurable
outcomes.
Question 22, 41, 60, 82 asked all groups how they thought HCP’s could demonstrate
that their contribution had enhanced the patient outcomes. Respondents were able to
enter up to five activities.
The HCP group were very focused on the patient and identified several measures to
indicate enhancements to patient outcomes. These included reductions in: falls,
complaints, waiting times, lengths of stay, mortality rates, costs, delays and
readmissions. The HCP group also identified right sized rooms, improved infection
control measures, patient centered care, sustainable development with future
expansion capability, increased use of rooms and evidence based design as other
measures for patient outcomes.
Patient outcome measures identified by the construction group included ease of
treatment, compliance with privacy and dignity, effective use of space, patient and staff
satisfaction surveys, improvement in patient statistics, reduced complaints, a
reduction in cost per admission, adaptable space and improved patient flows.
The client group identified improved attendance, patient and staff satisfaction surveys,
reduced length of stay, reduced falls, less congestion, improved patient safety and
facilitation of best practice as patient outcome measures.
As expected, the responses to this question provided evidence of a high patient focus,
particularly within the HCP group. These measurable patient outcomes were reflected
by all the groups with construction demonstrating a slight bias towards spaces, costs
and statistics.
28
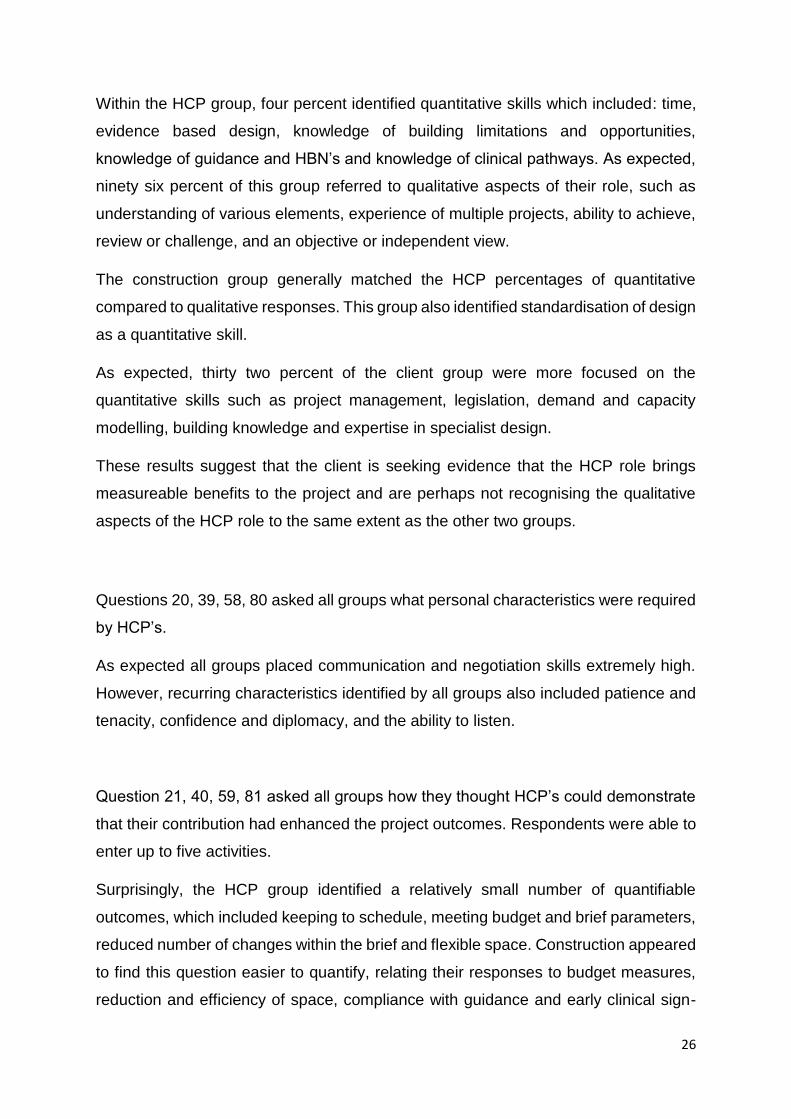
At Questions 23, 42, 61 and 83 all respondent were asked:
“Do you consider that the Healthcare Planner role requires further development, with
more formal recognition in the Healthcare sector?”
The results are presented in figure 12.
Figure 12. All respondents - "Do you consider that the HCP role requires further development, with more formal recognition in the healthcare sector?" (Dickson. March 2015)
Two HCP’s did not answer this question, however, the results clearly demonstrate that
HCP’s agree or strongly agree further development is required. The one HCP who
disagreed resided and worked in Australia and indicated that the role was already well
established. (11050298).The neutral responses from construction included “Perhaps
up to a month’s training.”(10985409) and “…it is more about demonstrating the
value…” (11010574).The client neutral response was concerned about additional cost
to the Trust when there was “…potential for in-house skills to be developed…”
(10991171)
At Questions 24, 43, 62 and 84, all participants were asked:
“What skill set or core-competencies should an individual possess before they could
call themselves a Healthcare Planner?”
As expected, one hundred percent of the HCP group identified knowledge, experience
and understanding as their “skill-set” and “core-competencies.” These comments
0
5
10
15
20
Stronglyagree
Agree Neutral Disagree
20
16
11
13
6
20
5 5
10
All Respondents. "Do you consider that the HCP role requires further development, with more formal recognition in the
healthcare sector"
HCP (50)
Construction (11)
Client (11)
29
primarily related to the client business and inner-workings, but also included
references to the construction industry. Eighty seven percent of the HCP group also
identified analytical skills of some form, which included: various types of benchmarking
data, schedules of accommodation and capacity planning. However, HCP 11010563
commented “You know, I am not sure.” with 10926632 commenting “Tricky, much of
our role could be considered as pastoral!”
Within construction, the same observations were made regarding knowledge,
experience and understanding of the healthcare and construction industries. The
“pastoral” elements identified by 10926632 were also echoed across the construction
group.
“I don’t think it’s possible to define…” (10999232) was one comment from within the
client group, with 10991171 indicating that they were “not clear enough on the role” to
comment.
It can be observed from this result that the “skill-set” and “core-competencies” remain
difficult to define and quantify. However, they do reflect the findings within the
literature. (Haron et al. 2012, p.67)
30
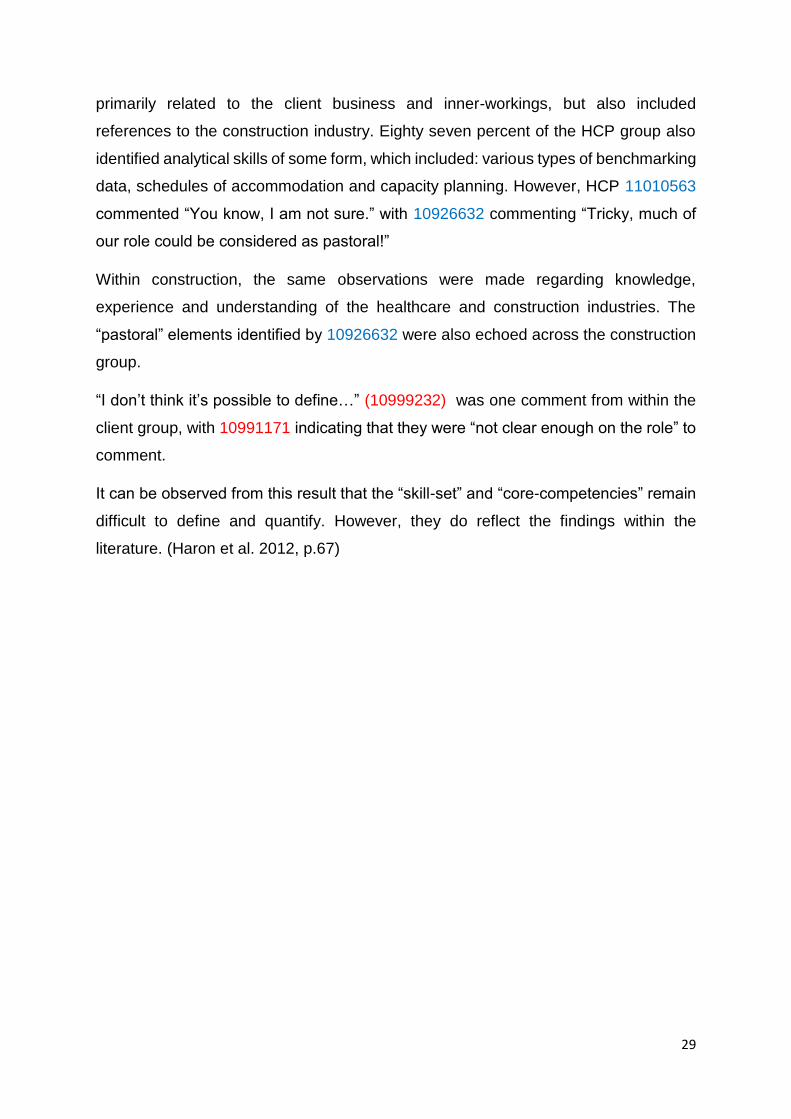
Questions 25, 44, 63 and 85 asked all participants:
“How do you think HCP skills or competencies should or could be measured?”
Participants were able to enter more than one answer and these have been collated
in figure 13.
Figure 13. All respondents - "How do you think HCP skills or competencies should or could be measured?" (Dickson. March 2015)
Eighty two percent of HCP’s identified an experience matrix as their preferred
measuring tool, followed by sixty six percent for a competency matrix. This result was
expected. Fifty four percent of HCP’s advocated an academic qualification, which was
higher than expected, which may indicate that HCP’s are seeking to formalise their
skills. Additional comments recognised that academic qualifications do matter and
may indeed help (10988471, 11061097) but the consensus of opinion was that “…it
has to be a combination of these things, with the main factor being experience.”
(10986136)
Construction comments observed “Balance is required between academic, clinical and
experience.” (10991064) and that “…several measuring tools are applicable and valid,
depending on the detail requirements.” (11075130)
One member of the client group observed that “…a lot of it comes down to common
sense” (10985974) with another indicating “Membership of professional body”
(911043917) as a measurement of HCP skills and competencies.
05
1015202530354045
27
13
33
41
18
35 3 6 6 4 34 49 8 5
1
All Respondents."How do you think HCP skills or competencies should or
could be measured?"
HCP (50)
Construction (11)
Client (11)
31
The final question posed at Questions 26, 45, 64 and 86 asked all participants if they
would like to make any additional observations.
Notable comments from the HCP group included “…often the HCP raises the
questions or issues that are in the “too difficult to do” box…” (11003684) and that
“Quality planning…is paramount.” (11056396)
The construction group commented that “there appears to be no “entry level” for HCP’s
…they would benefit from the creation of a national body…” (10992953) and “…to
often the projections for the future are based on applying the models of the past.”
(11075130)
Two members of the client group (11000564, 10995793) identified that the
competency levels of HCP’s varied widely, adding that HCP’s had demonstrated
“…insufficient research based evidence to back-up their views…” (11000564) in their
interactions with clinicians.
It can be observed from these additional comments that HCP’s are primarily focused
on quality and dealing with the difficult issues. The client responses support findings
from the literature and the questionnaire, in that they are looking for research based
evidence. The construction group indicated that they are also looking for some level
of validation. An unexpected comment from construction suggests that some HCP’s
may not have updated their skills in line with more modern tools or methodologies.
32
Conclusions.
HCP’s are a highly mobile, international resource who can demonstrate a
wide range of experience across multiple healthcare construction projects.
The softer skills of negotiation, objectivity and critical challenge remain difficult
to quantify and continue to raise further questions on how to demonstrate the
value of the HCP’s expertise. The HCP role remains ambiguous and
fragmented across the healthcare and construction industries.
Clients are utilising substantive staff to undertake many of the HCP activities
within projects and are seeking clarity regarding the parameters and
additional benefits of using a HCP.
The HCP’s expertise is not yet substantiated within recognised academic or
industry parameters. HCP’s are not registered or monitored and have no
specific, industry recognised or academic qualification.
There is no central resource relating to Healthcare Planning as a profession,
therefore it is not yet able to call itself a profession. A defined skill set with
measurable competencies would further the HCP’s status by establishing
themselves as a recognised profession within the healthcare construction
industry.
Establishing themselves as an Institute or Association could promote
assurance and confidence in the expertise of the HCP.
33
Recommendations.
1. It is recommended that a robust format is developed that links the HCP’s
activities to the Key Performance Indicators and other measurement criteria
which are already embedded in the healthcare industry. This would begin to
provide irrefutable evidence of the HCP’s involvement, activities and outcomes
within briefing, in a format that the healthcare industry recognises.
2. It is recommended that HCP’s become more adept at promoting their role.
Improved marketing and publication of their quantifiable activities would raise
awareness of the benefits they can bring to healthcare construction projects.
3. It is recommended that the “Healthcare Planner Scope of Service and Duties.”
(Frameworks Scotland 2. 2014, pp.15-19) be adopted across the healthcare
construction industry in the UK, as the definitive base-line criteria for HCP
competencies.
4. It is recommended that established HCP’s work with the UK Government, the
healthcare construction industry and academic institutions, to define the
parameters of a potential qualification for Healthcare Planners.
5. It is recommended that registration as a Healthcare Planner within an Institute
or Association would facilitate monitoring of competencies and accountability
within the healthcare and construction industries.
6. Further research is required into this complex and diverse role within the
healthcare and construction industries.
34
References.
Brace, I. (2013) Questionnaire Design: How to plan, structure and write survey material for effective market research. Third Edition. London: Kogan Page.
Carr, L. T. (1994) The strengths and weaknesses of quantitative and qualitative research: what method for nursing? Journal of Advanced Nursing, 1994, Vol. 20, pp 716 - 721.
Neville, C. (2014) Introduction to Research and Research Methods. [Online]. Available from: http://www.brad.ac.uk/management/media/management/els/20.-Introduction-to-Research-and-Research-Methods---20141021.pdf [Accessed 04 August 2014].
Oppenheim, A. N. (1992) Questionnaire Design, Interviewing and Attitude Measurement. London: Continuum.
Robinson, H. (2014) Approaches to Research (1). [Online]. Available from: ttps://blackboard.lsbu.ac.uk/webapps/portal/frameset.jsp?tab_group=courses&url=%2Fwebapps%2Fblackboard%2Fcontent%2FcontentWrapper.jsp%3Fattachment%3Dtrue%26navItem%3Dcontent%26content_id%3D_1221479_1%26course_id%3D_104325_1%26displayName%3DResearch%2BMeth [Accessed 17 March 2014].
Sheehan, K. B. (2001) E-mail Survey Response Rates: A Review. Journal of Computer-Mediated Communication. Vol. 6. p 0. [Online]. Available from: http://onlinelibrary.wiley.com/doi/10.1111/j.1083-6101.2001.tb00117.x/full [Accessed 04 April 2015].