
HCH-United-webinar slides
33
Managed Care and Homeless Populations: Linking the HCH Community and MCO Partners April 5, 2016
-
Upload
nguyendung -
Category
Documents
-
view
226 -
download
0
Transcript of HCH-United-webinar slides
Managed Care and Homeless Populations: Linking the HCH Community and MCO PartnersApril 5, 2016
Welcome Learning Objectives:
•Understand the factors influencing Medicaid managed care plans and their approach to serving people experiencing homelessness and how they are seeking opportunities to partner with providers serving the population
•Understand how the HCH Community can maximize common goals with managed care plans
•Describe how two Health Care for the Homeless projects in Washington State (one urban and one rural) are partnering with a managed care plan for medical respite services.
Speakers:
•Catherine Anderson, Vice President, Positioning and Strategy, UnitedHealthcare Community & State
•Barbara DiPietro, Senior Director of Policy, National HCH Council
•Doug Bowes, CEO, UnitedHealthcare Community Plan of Washington
•Edward Dwyer-O'Connor, BS, RN, Senior Manager, Downtown Programs, Harborview Medical Center, Seattle, WA
•Matt Lund, Director of Contracting, UW Medicine at Harborview Medical Center, Seattle, WA
•Rhonda Hauff, COO/Deputy CEO, Yakima Neighborhood Health, Yakima, WA
2
Background on Initiative• Recognized Interest
• 2015 Healthcare for the Homeless Annual Conference
• Began conversations
• Co-wrote the white paper and developed today’s webinar
• Beginning to an on-going conversation
3
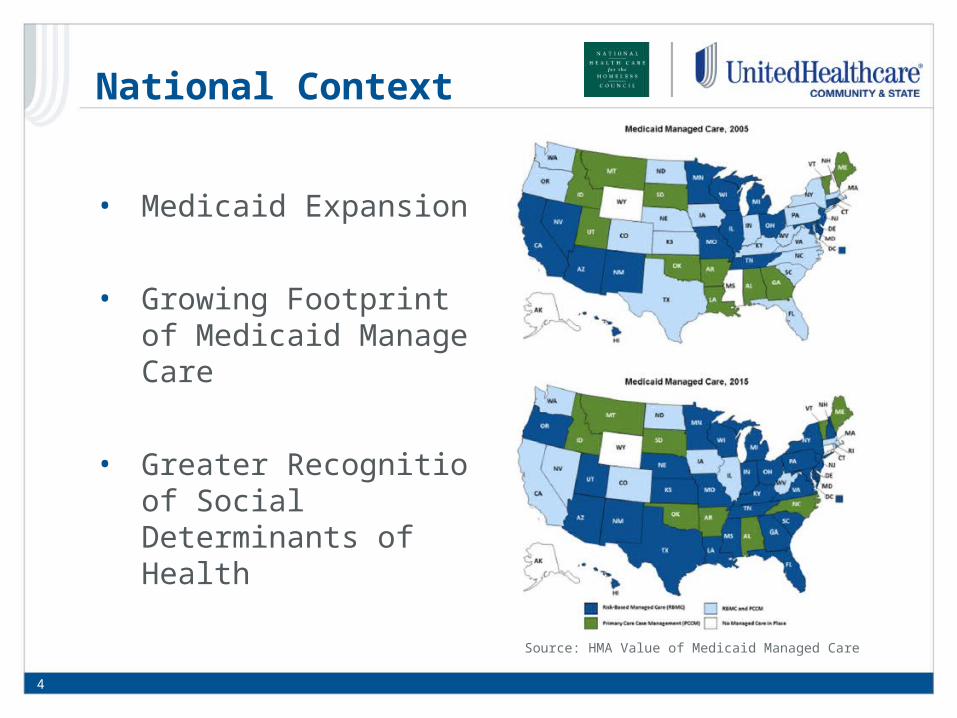
National Context
4
• Medicaid Expansion
• Growing Footprint of Medicaid Managed Care
• Greater Recognition of Social Determinants of Health
Source: HMA Value of Medicaid Managed Care
Medicaid Managed Care
5
Source: Architect of the Capitol
Federal Government •Establishes basic rules and criteria States must follow in the design and operation of a Medicaid program•Covers a significant portion of the costs of Medicaid (varies by state and population) •Approves contracts and rates between states and managed care entities
State Governments •Establish program rules, benefits, eligibility, contract provisions and the rates health plans will be paid to administer the Medicaid program•Compensates the health plans using a per member per month capitated rate
Health Plans•Administer the Medicaid program according to the terms of the contract with the state for their assigned Medicaid beneficiaries•Measured on ability to support their members in receiving preventive treatment, achieving state goals, and meeting other quality metrics established by the state•Established contracts with providers
Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
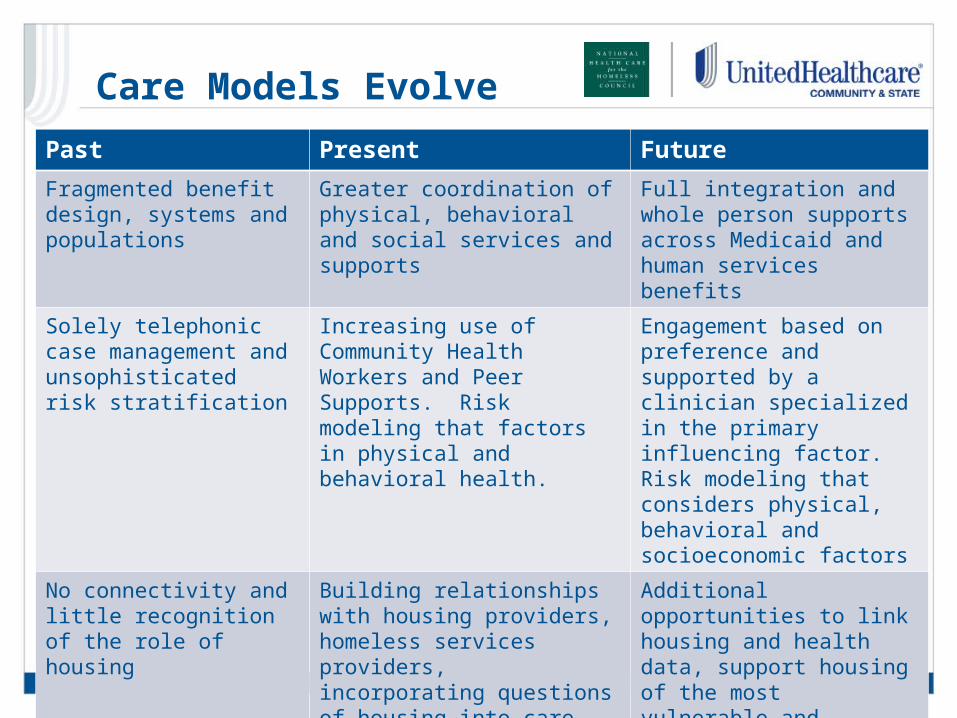
Care Models Evolve
6Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
Past Present FutureFragmented benefit design, systems and populations
Greater coordination of physical, behavioral and social services and supports
Full integration and whole person supports across Medicaid and human services benefits
Solely telephonic case management and unsophisticated risk stratification
Increasing use of Community Health Workers and Peer Supports. Risk modeling that factors in physical and behavioral health.
Engagement based on preference and supported by a clinician specialized in the primary influencing factor. Risk modeling that considers physical, behavioral and socioeconomic factors
No connectivity and little recognition of the role of housing
Building relationships with housing providers, homeless services providers, incorporating questions of housing into care planning
Additional opportunities to link housing and health data, support housing of the most vulnerable and integrate broader array of human services
Policy Considerations
Medicaid benefit and program design matters!•Expansion vs. non-expansion•Populations under managed care contract•Benefits under managed care contract – behavioral health, LTSS/HCBS, housing supports, etc.•Medical Loss Ratio calculations•Care coordination requirements•State program priorities•Delivery and payment reform requirements•Quality definitions, calculations and accountability
7Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.

Needed for Success
• Countless opportunities to collaborate exist, but resources and capacity on both sides are limited
• Evaluating opportunities:• Members impacted• Opportunity to improve quality • Opportunity to improve utilization• Data available to support the decision to invest, track and
demonstrate impact• Presence of trusted partners willing to innovate with
unique skills and expertise
8 Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
Washington Panel on MCO & HCH Collaborations
9

Washington Panel
• Doug Bowes, CEO, UnitedHealthcare Community Plan of Washington
• Edward Dwyer-O'Connor, BS, RN, Senior Manager, Downtown Programs, Harborview Medical Center, Seattle, WA
• Matt Lund, Director of Contracting, UW Medicine at Harborview Medical Center, Seattle, WA
• Rhonda Hauff, COO/Deputy CEO, Yakima Neighborhood Health, Yakima, WA
10Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
Medical Respite• Medical respite care is acute and post-acute medical care for
homeless persons who are too ill or frail to recover from a physical illness or injury on the streets but are not ill enough to be in a hospital.
• Unlike “respite” for caregivers, “medical respite” is short-term residential care that allows homeless individuals the opportunity to rest in a safe environment while accessing medical care and other supportive services.
• Medical respite care is offered in a variety of settings including freestanding facilities, homeless shelters, nursing homes, and transitional housing.
11Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
Washington Context
• UnitedHealthcare Community Plan is the third largest Medicaid
managed care plan in Washington State providing physical health
benefits and services to more than 210,000 members
• We provide face-to-face and telephonic care coordination services
for our most complex members, including many that are homeless
• Washington Medicaid program has continually sought significant
reforms and modernization including:
12Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
Health Plan Journey
• Recognized need
• Built off Established Relationships
• Learned about Jefferson Terrace Program
• Made the case internally
• Worked out the details and executed contract
• Replicated with Yakima Neighborhood Health Services
• Continuing to look for ways to improve coordination, care
transition and evaluation
13Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
Value of Collaboration
• We were interested in seeing to it that our members were able to access the care and recovery environment they needed and to keep them from facing recovery and recuperation on the streets or in a shelter. o Reducing hospital readmissions o Improving the health of the member
• Partnering with medical respite helps to create an essential care linkage opening the door to additional physical and behavioral health care coordination and holistic social support services, all of which uphold our driving goal of the Triple Aim.
14Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
Edward Thomas House
• Respite history in Seattle• Free-standing unit in Jefferson
Terrace/SHA/HUD• Harm Reduction Program/34 beds• Designed for high medical and
behavioral acuity• Braided funding; money from 6
hospitals, Public Health – HUD, HRSA, local MIDD funding and MCOs.
• Hospitals needed IV antibiotic treatment for IVDU
• 475 patients/year. LOS 21 days. 15Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
WHO DOES RESPITE SERVE?• Homeless men and women with complex needs [too sick for the
streets, not sick enough for the hospital]• Acute medical issues; often abscesses and infections R/T IVDU• IV antibiotics often 4-6 weeks• Multiple chronic conditions• Preponderance of chemical dependency plus mental illness• Patients must be independent in mobility [wheelchair OK]• Behavior must be safe for the setting [no threats, violence,
weapons]• Cannot use drugs on the unit• Able to serve much higher acuity [staff includes MD, ARNPs, RNs,
MHPs, MHSs, Mas, custodial and data manager]• Goals for care include; access to entitlements, primary care, case
management services, housing, opiate replacement therapy, chemical dependency treatment
• Client story
APPROACH• Risk sharing and collaboration• Search for innovative ways to provide care for underserved, high
cost patients• Manage the whole person• Look for leverage points in the Triple Aim• Reduce costa• Improve outcomes• Find data to support outcomes and decreased costs [EDH study
of 69 patients showed 70% reduction in hospital days 6 months post respite compared to 6 months pre-respite, a 57% reduction in inpatient admissions also decrease ED visits by 10%]
• MCOs could not pay for respite stay, needed Health Care Authority to allow payment
Path to a Contract• Gained authorization from state Medicaid agency to
bill/reimburse for respite care• Directed to bill and reimburse under G9006 “Coordinated Care
Fee, Home Monitoring”• Determined how and how much to charge• Consulted revenue cycle, contracting, utilization management,
and social work departments to ensure full understanding of work flows
• Assembled helpful data and analysis demonstrating efficacy and cost effectiveness of program
• Hosted tours of facility for managed Medicaid plan reps• Approached managed Medicaid plans with pitch to contract for
respite services
Contract• Coverage and reimbursement established through amendment
to existing agreements• Discussed possible models for reimbursement (per diem, case
rate, etc.)• Discussed: concurrent review/UM needs, program definitions,
scope of services, other expectations• Negotiated key terms, executed amendments, and monitored
events (care delivered, charges issued, reimbursements paid, problems solved, lessons learned)
• Agreement to meet and discuss specs, successes/challenges, and needs on a regular basis
• Recognition of cost savings and improvement of individual and population health

To provide accessible, affordable, quality health care, promote learning opportunities for students of health
professions, end homelessness and improve quality of life in our communities.
YNHS Mission
20

Homeless Respite - Recuperative Housing for those not sick enough
to be in the hospital, and those discharged from the hospital but not well enough to go back to the
streets
Satellites Serve Special Populations
21
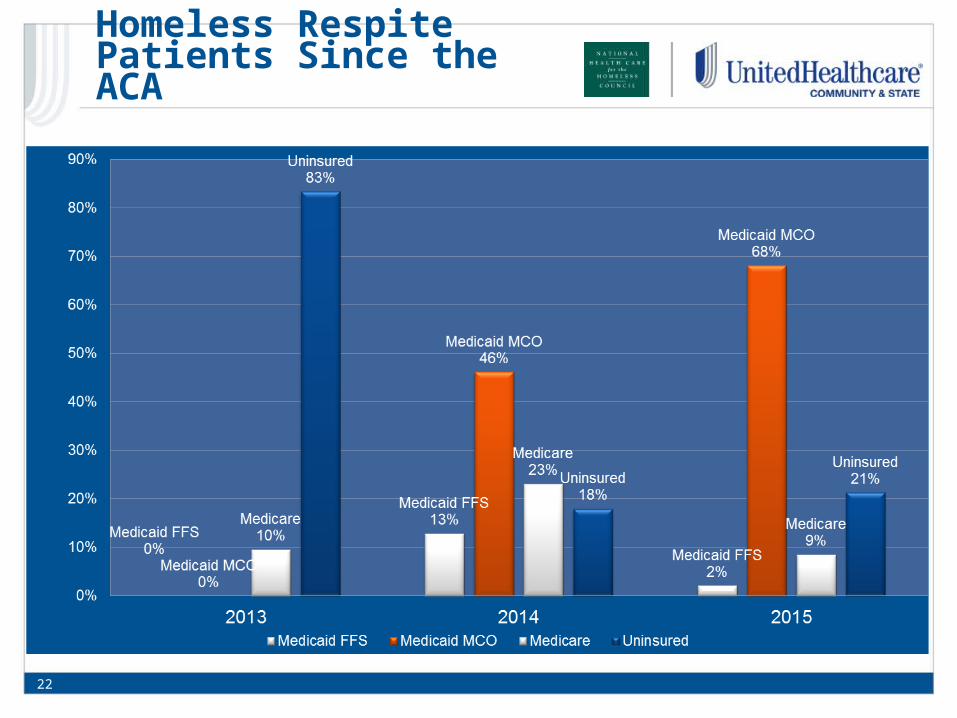
22
Homeless Respite Patients Since the ACA
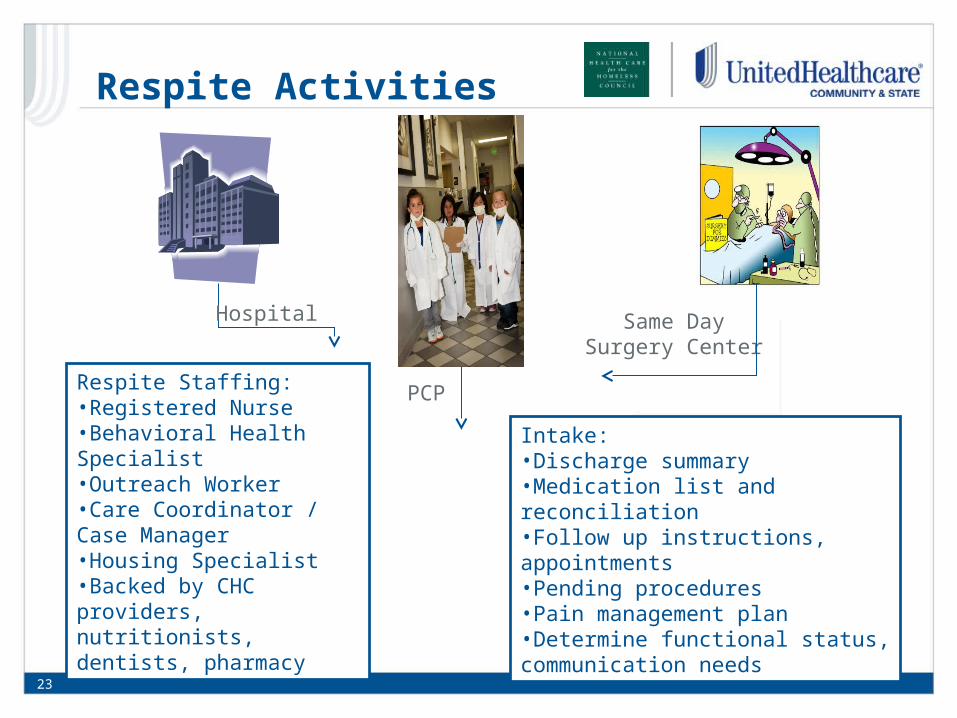
Hospital
PCP
Same Day Surgery Center
Intake:•Discharge summary•Medication list and reconciliation•Follow up instructions, appointments•Pending procedures•Pain management plan•Determine functional status, communication needs
Respite Staffing:•Registered Nurse•Behavioral Health Specialist•Outreach Worker•Care Coordinator / Case Manager•Housing Specialist•Backed by CHC providers, nutritionists, dentists, pharmacy
Respite Activities
23
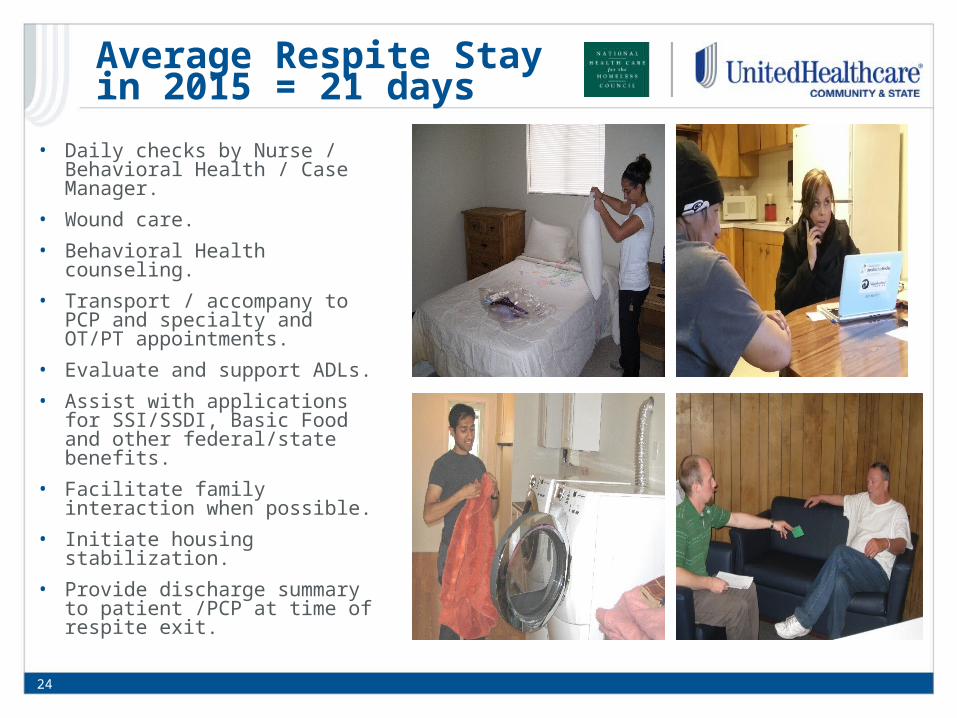
• Daily checks by Nurse / Behavioral Health / Case Manager.
• Wound care.• Behavioral Health counseling.• Transport / accompany to PCP
and specialty and OT/PT appointments.
• Evaluate and support ADLs.• Assist with applications for
SSI/SSDI, Basic Food and other federal/state benefits.
• Facilitate family interaction when possible.
• Initiate housing stabilization.• Provide discharge summary to
patient /PCP at time of respite exit.
24
Average Respite Stay in 2015 = 21 days
ServingIndividuals toEndSeriousTrouble throughAgencies’Support
Who do we SIESTA:
•Chronic medical or social needs
•Cause upheaval in the social service system
•Seen by multiple service providers
•Use a LOT of resources - repeatedly
25
Help is On the Way…SIESTAS
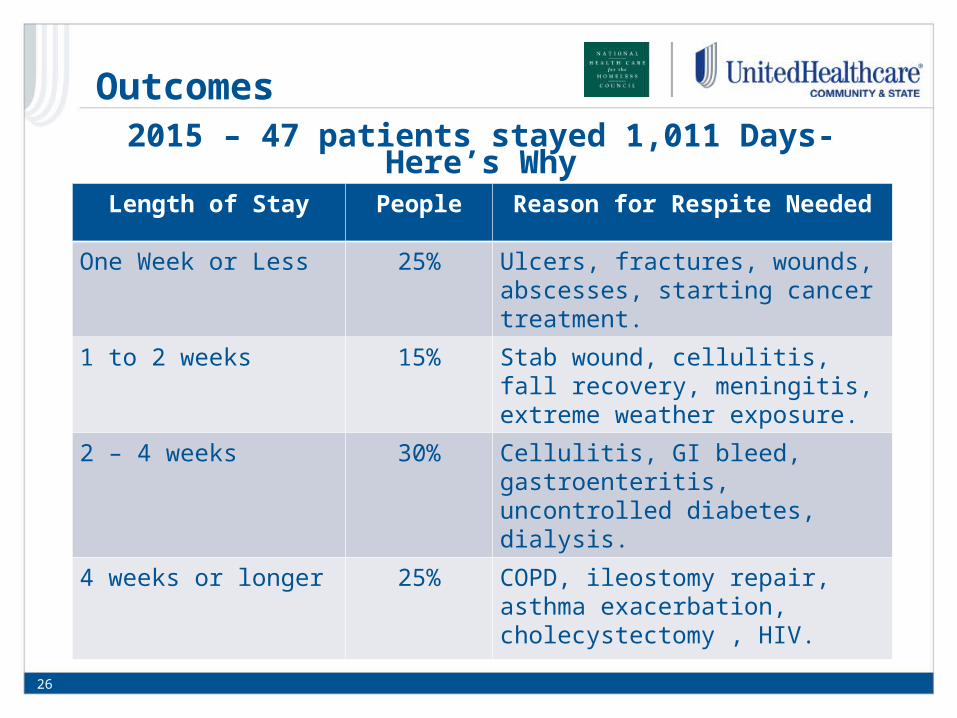
2015 – 47 patients stayed 1,011 Days- Here’s WhyLength of Stay People Reason for Respite Needed
One Week or Less 25% Ulcers, fractures, wounds, abscesses, starting cancer treatment.
1 to 2 weeks 15% Stab wound, cellulitis, fall recovery, meningitis, extreme weather exposure.
2 – 4 weeks 30% Cellulitis, GI bleed, gastroenteritis, uncontrolled diabetes, dialysis.
4 weeks or longer 25% COPD, ileostomy repair, asthma exacerbation, cholecystectomy , HIV.
26
Outcomes
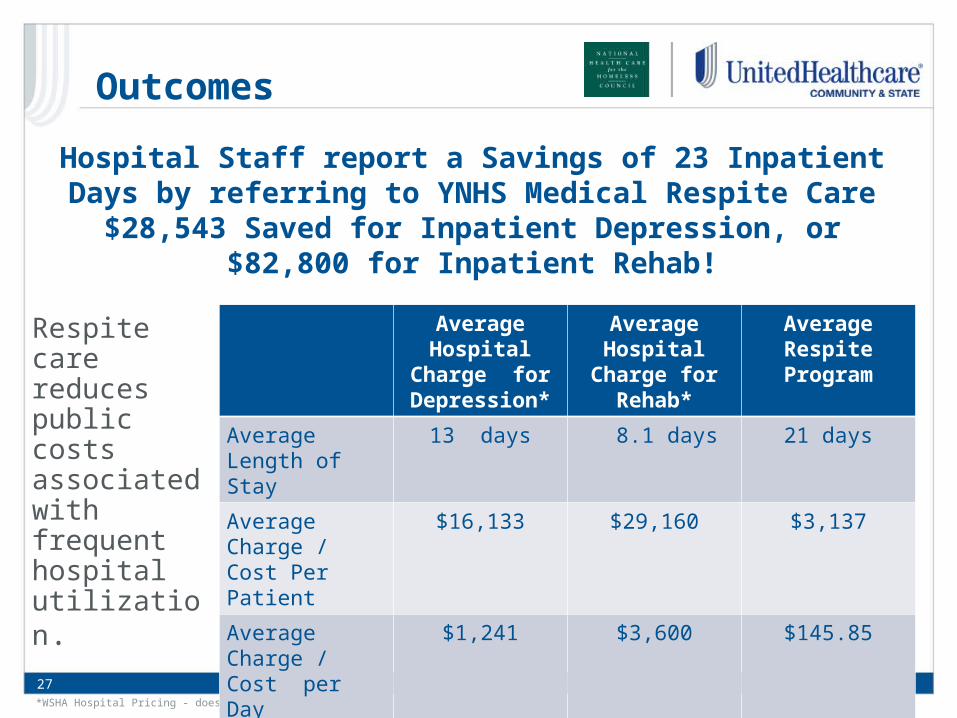
Hospital Staff report a Savings of 23 Inpatient Days by referring to YNHS Medical Respite Care
$28,543 Saved for Inpatient Depression, or $82,800 for Inpatient Rehab!
*WSHA Hospital Pricing - does not include professional fees in charges
Respite care reduces public costs associated with frequent hospital utilization.
AverageHospital
Charge for Depression*
AverageHospital
Charge for Rehab*
AverageRespite Program
Average Length of Stay
13 days 8.1 days 21 days
Average Charge / Cost Per Patient
$16,133 $29,160 $3,137
Average Charge / Cost per Day
$1,241 $3,600 $145.85
27
Outcomes
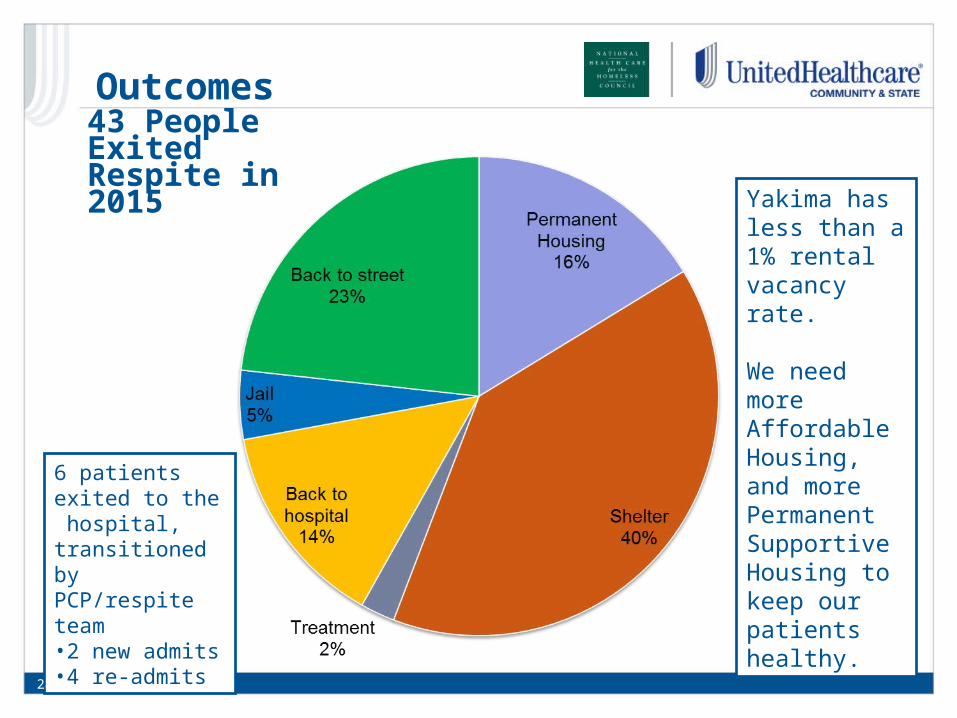
6 patients exited to the hospital, transitioned by PCP/respite team•2 new admits•4 re-admits
Yakima has less than a 1% rental vacancy rate.
We need more Affordable Housing, and more Permanent Supportive Housing to keep our patients healthy.
28
43 People Exited Respite in 2015
Outcomes
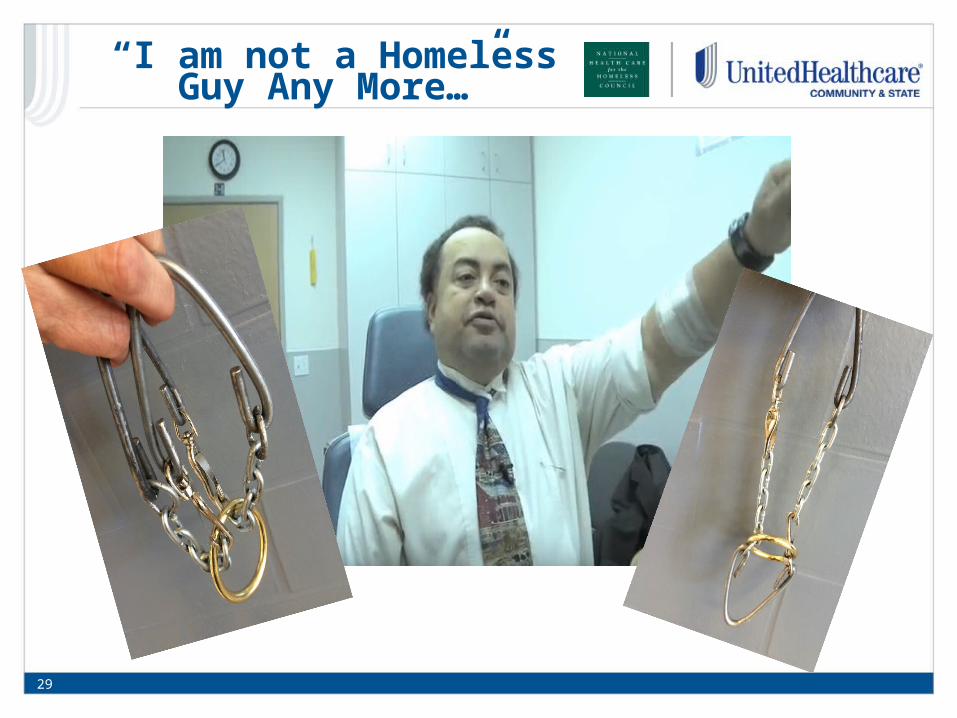
“I am not a Homeless Guy Any More…”
29

YNHS works with 3 MCOs providing Health
Home Services• Targets high cost Medicaid
and Dual Eligible clients.• Provides intense care
coordination and support for high needs patients.
• Sounds like our homeless population!
• HCH staff certified as Health Home Care Coordinators
• Last year YNHS staff provided Health Home Care Coordination to 230 unduplicated patients through our CHC – 55 (23%) were homeless.
30
Health Home Services

Discussion/Q&A Speakers:
•Catherine Anderson, Vice President, Positioning and Strategy, UnitedHealthcare Community & State
•Barbara DiPietro, Senior Director of Policy, National HCH Council
•Doug Bowes, CEO, UnitedHealthcare Community Plan of Washington
•Edward Dwyer-O'Connor, BS, RN, Senior Manager, Downtown Programs, Harborview Medical Center, Seattle, WA
•Matt Lund, Director of Contracting, UW Medicine at Harborview Medical Center, Seattle, WA
•Rhonda Hauff, COO/Deputy CEO, Yakima Neighborhood Health, Yakima, WA
31
Additional Resources
Policy Brief: Managed Care & Homeless Populations: Linking the HCH Community and MCO Partners
Available at:https://www.nhchc.org/wp-content/uploads/2016/03/mco-hch-policy-brief.pdf
Medical Respite Tool Kit:•Intro & overview•Development & finance•Collaborating with hospitals•Operations & clinical care
Available at: https://www.nhchc.org/resources/clinical/medical-respite/tool-kit/
32Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.
Thank you
Thank you for attending this webinar on Managed Care and Homeless Populations: Linking the HCH Community and MCO Partners!
This project is/was supported by the Health Resources and Services Administration (HRSA) of the U.S. Department of Health and Human Services (HHS) under grant number U30CS09746, a National Training and Technical Assistance Cooperative Agreement for $1,625,741, with 0% match from nongovernmental sources. This information or content and conclusions are those of the author and should not be construed as the official position or policy of, nor should any endorsements be inferred by HRSA, HHS or the U.S. Government.
33Proprietary Information of UnitedHealth Group. Do not distribute or reproduce without express permission of UnitedHealth Group.













![Welcome [] Welcome Laying the Groundwork for Meeting QI/QA Program Expectations in an HCH Setting Webinar: Lessons Learned from the San Francisco HCH Program March 6, 2012 We will](https://static.fdocuments.in/doc/165x107/5abda2bd7f8b9ab02d8bdecb/welcome-welcome-laying-the-groundwork-for-meeting-qiqa-program-expectations.jpg)

