HAZARD COMMUNICATION Marzo 2003 Codigo 12/2003. Hazard Communication HAZARD COMMUNICATION.

Hazard and absolute risk for the heart(researchers)
Thomas Alexander Gerds
23 Maj 2014
1 / 42

Prolog: A side
Citat fra en email:
Dernæst har jeg brug for at forstå hvorfor vi ikke kan plotte HR,
men i stedet survival%?
Herovre er vi glade for HR, da mange anvender det.
2 / 42

Prolog: B side
When I was diagnosed with lymphoma 11 years ago, I was eager to learn
my prognosis. 1
For example, I had heard I had a favorable histologic subtype, but I did
not know how much weight it should be given.
I really wanted a predicted probability of survival and didn't speci�cally
care what the prognostic factors were, what my relative risk might be, or
in what risk group I belonged.
1M Kattan. Statistical prediction models, arti�cial neural networks, and thesophism 'I am a patient, not a statistic`. Journal of Clinical Oncology,20:885-887, 2002.
3 / 42

AimTo bring (back) the full story to those who got so used to the terms
hazard rate and hazard ratio.
Outline
I hazard rate ↔ absolute risk
I absolute risk ratio ↔ hazard rate ratio
I competing risk ↔ loss to follow-up (censored)
I estimation ↔ prediction ↔ landmarking
Analogy
living ↔ cycling
4 / 42

hazard rate ↔ absolute risk
5 / 42

Speed and hazard
Speed can be thought of as the rate at which an object coversdistance.
I A fast-moving object has a high speed and covers a relativelylarge distance in a given amount of time
I A slow-moving object covers a relatively small amount ofdistance in the same amount of time.
Hazard rate can be thought of as the speed at which a person getsa disease or dies.
I An exposed person has a high hazard rate and will get diseasedwith a relatively large probability within a given time period.
I A non-exposed person has a low hazard rate and will getdiseased with a relatively small probability within the sametime period.
6 / 42

Speed and duration
If we know the (average) speed of a cyclist on the road from placeA to place B we can calculate the (expected) duration that thecyclist would need to cycle from A to B.
The speed changes along the road according to gradient and otherthings, the duration is relative to the length of the road.
7 / 42

Hazard and absolute risk
If we know the (average) hazard rate of a person in a time intervalbetween date A and date B we can calculate the (expected)probability that the person would have a stroke between the datesA and B.
The hazard rate changes over time according to exposure and otherthings, the absolute risk of stroke is relative to the length of thetime interval.
8 / 42

Computing duration
Suppose the speed of a cyclist is piece-wise constant on the roadbetween A and B:
Section Distance (km) Speed (km/h) Duration (min)
A �> a 10 15 40.0a �> b 20 20 60.0b �> B 20 22 54.5
I Total distance: 50 km
I Total duration: 154.5 minutes
Conclusion: The cyclist needs 154.5 minutes to cycle from A to B.
9 / 42

Computing absolute risk
Suppose the stroke hazard rate of a patient is piece-wise constantin the time period between A and B:
Interval Duration (mth) Hazard rate (%/mth) Abs. risk (%)
A �> a 10 1.5 13.9a �> b 20 2.0 33.0b �> B 20 2.2 35.6
I Total duration: 50 months
I Total absolute risk: 62.8%
calculation: 1- (1-0.139)(1-0.33)(1-0.356) = 0.628
Conclusion: The patient will experience a stroke with a probabilityof 62.8% in the period between date A and date B.
10 / 42

Relative risks & risk di�erences
11 / 42
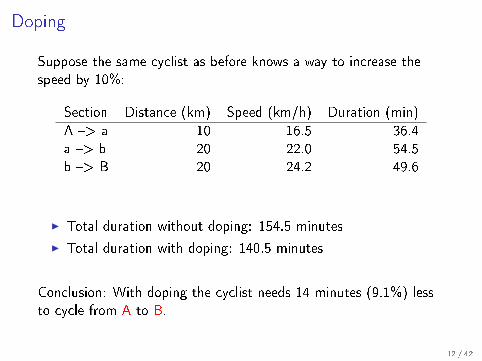
Doping
Suppose the same cyclist as before knows a way to increase thespeed by 10%:
Section Distance (km) Speed (km/h) Duration (min)
A �> a 10 16.5 36.4a �> b 20 22.0 54.5b �> B 20 24.2 49.6
I Total duration without doping: 154.5 minutes
I Total duration with doping: 140.5 minutes
Conclusion: With doping the cyclist needs 14 minutes (9.1%) lessto cycle from A to B.
12 / 42

Relative Risks for Stroke by Age, Sex, and Population Basedon Follow-Up of 18 European Populations in the
MORGAM ProjectKjell Asplund, MD, PhD; Juha Karvanen, DSc(Tech); Simona Giampaoli, MD;
Pekka Jousilahti, MD, PhD; Matti Niemela, MD; Grazyna Broda, MD; Giancarlo Cesana, MD;Jean Dallongeville, MD; Pierre Ducimetriere, MD; Alun Evans, MD; Jean Ferrieres, MD;
Bernadette Haas, MD; Torben Jorgensen, MD; Abdonas Tamosiunas, MD; Diego Vanuzzo, MD;Per-Gunnar Wiklund, MD, PhD; John Yarnell, MD; Kari Kuulasmaa, PhD; Sangita Kulathinal, PhD;
for the MORGAM Project
Background and Purpose—Within the framework of the MOnica Risk, Genetics, Archiving and Monograph (MORGAM)Project, the variations in impact of classical risk factors of stroke by population, sex, and age were analyzed.
Methods—Follow-up data were collected in 43 cohorts in 18 populations in 8 European countries surveyed forcardiovascular risk factors. In 93 695 persons aged 19 to 77 years and free of major cardiovascular disease at baseline,total observation years were 1 234 252 and the number of stroke events analyzed was 3142. Hazard ratios werecalculated by Cox regression analyses.
Results—Each year of age increased the risk of stroke (fatal and nonfatal together) by 9% (95% CI, 9% to 10%) in menand by 10% (9% to 10%) in women. A 10-mm Hg increase in systolic blood pressure involved a similar increase in riskin men (28%; 24% to 32%) and women (25%; 20% to 29%). Smoking conferred a similar excess risk in women (104%;78% to 133%) and in men (82%; 66% to 100%). The effect of increasing body mass index was very modest. Higherhigh-density lipoprotein cholesterol levels decreased the risk of stroke more in women (hazard ratio per mmol/L0.58; 0.49 to 0.68) than in men (0.80; 0.69 to 0.92). The impact of the individual risk factors differed somewhatbetween countries/regions with high blood pressure being particularly important in central Europe (Poland andLithuania).
Conclusions—Age, sex, and region-specific estimates of relative risks for stroke conferred by classical risk factors invarious regions of Europe are provided. From a public health perspective, an important lesson is that smoking confersa high risk for stroke across Europe. (Stroke. 2009;40:2319-2326.)
Key Words: blood pressure � cholesterol � cohort studies � smoking � stroke risk factors
The appraisal of stroke risk in populations or individuals isbased on the recognition that all cardiovascular disorders
are multifactorial in nature. The most widely used risk scorefor stroke was developed within the framework of TheFramingham Heart Study, the original version being pub-lished in 1971 with later refinements based on longer follow-up, addition of more predictors, and using more sophisticated
statistical techniques.1 The Framingham stroke risk score hasbeen used extensively when international and national guide-lines for cardiovascular prevention have been developed.Other stroke prediction scores have been developed later, forinstance based on data from a large population-based US cohortof elderly men and women (the Cardiovascular Health Study),2
a large number of cohorts within the Systematic COronary Risk
Received January 15, 2009; final revision received February 23, 2009; accepted March 12, 2009.From the Department of Public Health and Clinical Medicine (K.A.), Medical Unit, Umeå University Hospital, Umeå, Sweden; the National Institute
for Health and Welfare (J.K., P.J., M.N., K.K.), Helsinki, Finland; the National Centre for Epidemiology, Surveillance and Health Promotion (S.G.),Istituto Superiore di Sanita, Rome, Italy; the Department of Cardiovascular Epidemiology and Prevention (G.B.), National Institute of Cardiology,Warsaw, Poland; Dipartimento de Medicina (G.C.), Prevenzione e Biotecnologie Sanitarie, Universita degli Studi Milano-Bicocca, Monza, Italy; theDepartment of Epidemiology and Public Health (J.D.), Pasteur Institute of Lille, Lille, France; the National Institute of Health and Medical Research(U258; P.D.), Paris, France; the Department of Epidemiology and Public Health (A.E., J.Y.), The Queen’s University of Belfast, Belfast, UK; theDepartment of Epidemiology (J.F.), Faculty of Medicine, Toulouse–Purpan, Toulouse, France; the Department of Epidemiology and Public Health (B.H.),Louis Pasteur University, Faculty of Medicine, Strasbourg, France; the Research Centre for Prevention and Health (T.J.), Capital Region, Denmark;Kaunas University of Medicine (A.T.), Institute of Cardiology, Kaunas, Lithuania; Centro di Prevenzione Cardiovasculare (D.V.), Agenmzia Regionaledella Sanita Friuli Venezia Giulia, Udine, Italy; the Department of Medicine (P.-G.W.), Umeå University Hospital, Umeå, Sweden; and the Indic Societyfor Education and Development (INSEED; S.K.), Nashik, India.
Correspondence to Kjell Asplund, MD, PhD, Riks-Stroke, Medicine, Department of Public Health and Clinical Medicine, University Hospital,SE-70185 Umeå, Sweden. E-mail [email protected]
© 2009 American Heart Association, Inc.
Stroke is available at http://stroke.ahajournals.org DOI: 10.1161/STROKEAHA.109.547869
2319 by guest on May 15, 2014http://stroke.ahajournals.org/Downloaded from
13 / 42

Computing di�erence in absolute risk
Suppose the same patient as before is one year older and thisincreases the hazard rate of stroke by 10% (hazard ratio=1.1):
Interval Duration (mth) Hazard rate (%/mth) Abs. risk (%)
A �> a 10 1.65 15.2a �> b 20 2.20 35.6b �> B 20 2.42 38.4
I Total absolute risk previous age: 62.8%
I Total absolute risk one year older: 66.4%
calculation: 1- (1-0.152)(1-0.356)(1-0.384) = 0.664
Conclusion: Each year of age increases the risk of stroke in theperiod between date A and date B by 3.6 %.
14 / 42

Relative absolute risk and absolute risk di�erence
To compute the relative risk of stroke in a given time period basedon a Cox regression analysis we need to combine the baseline
hazard rate, the hazard ratio and the length of the time interval.
I A statement about the (relative) risk of stroke without areference to a time interval is meaningless.
I The model assumes that the hazard ratio does not depend ontime
I The model assumes that the hazard ratio does not depend onthe other risk factors
The hazard ratio alone does not characterize the relative risk . . .
15 / 42

Hazard scale vs survival scale:Hazard ratio=2
Years
Sur
viva
l pro
babi
lity
0 2 4 6 8
0 %
25 %
50 %
75 %
100
%
5−year survival probability
not exposed 99.2 %
exposed 92.8 %
Hazard ratio=2
YearsS
urvi
val p
roba
bilit
y
0 2 4 6 8
0 %
25 %
50 %
75 %
100
%
5−year survival probability
not exposed 59.1 %
exposed 2.5 %
Hazard ratio=2
Years
Sur
viva
l pro
babi
lity
0 2 4 6 8
0 %
25 %
50 %
75 %
100
%
5−year survival probability
not exposed 77.2 %
exposed 16.2 %
Hazard ratio=2
Years
Sur
viva
l pro
babi
lity
0 2 4 6 8
0 %
25 %
50 %
75 %
100
%
5−year survival probability
not exposed 90.8 %
exposed 47.9 %
16 / 42

Competing risks ↔ loss to follow-up
17 / 42

Competing risk
Speed = 0
Censored
Speed = ?
18 / 42

Competing risks
What happens:
I A cyclist can have an accident or get injured.
Consequences:
I after the accident the speed is zero.
Decision making:
I To estimate the chances of a cyclists to win a race, one has tocombine the expected speed with the expected probability ofan accident/injury.
19 / 42

Competing risks
What happens:
I A patient can die � free from stroke.
Consequences:
I after death the hazard rate of stroke is zero.
Decision making:
I To estimate the risk of stroke, one has to combine theexpected hazard rate of stroke with the expected hazard rateof death due to other causes.
20 / 42

Example case study
Suppose a 40 year old and a 80 year old person need to decide foror against prophylactic coagulation therapy.
Suppose further the predicted risk of dying from cardiovasculardisease within the next 10 years for both persons is 12%. Howcould this happen?
One plausible explanation is that the 40 year old person has otherrisk factors that the 80 year old person does not have.
Another plausible explanation is that the 80 year old person has amuch higher risk to die due to non-cardiovascular causes within thenext 10 years than the 40 year old person.
21 / 42

Loss to followup (right-censored)What happens:
I the cyclist disappears into a tunnel and the cameraman cannotfollow for some reason, the cycle computer stops working, anindividual time-trail is analysed before all riders have arrived.
Consequences:
I We loose track of the cyclists' speed
For estimation:
I We can assume that the speed inside the tunnel is comparableto the speed outside the tunnel.
I There can be an accident inside the tunnel!
22 / 42

Loss to followup (right-censored)
What happens:
I It's time to analyse the data and the patient is still alive andevent-free, the patient has moved to a di�erent country, thepatient did not show up to followup examinations
Consequences:
I After loss to followup, events have unknown onset times (nocompeting risks)
I After loss to followup, events have unknown onset times and itis uncertain if they happen (competing risks)
For estimation:
I We can assume that the hazard rates after the end of theindividual study period are comparable to the hazard rates ofthe other patients who are not lost to followup.
23 / 42

Estimation
24 / 42

Estimation of speed
At any speci�c place 't' on the road between A and B we cancompute the average speed � among the cyclists for whom we havemeasured the speed:
I those that do not have an accident/injury before 't'
I those that are still tracked by a motorcycle
It is assumed that those who are not tracked are represented by
those who are tracked (independent censoring).
Survival of the �ttest
I The interpretation of the average speed at place 't' is limitedto the subgroup of cyclists who were able to cycle this far.
I This subgroup is changing along the road due to accidents andinjuries.
25 / 42

Estimation of hazard
For any speci�c time point 't' between dates A and B we canestimate the average hazard rate of stroke by dividing the numberof strokes that occur exactly at time 't' by the number of patientswho were observed at time 't':
I those who survived event-free
I those who are not lost to followup.
It is assumed that those who are lost to followup are represented by
those who are still in the study (independent censoring).
Depletion of the susceptible
I The interpretation of the average hazard at 't' is limited to thesubgroup of the population who survived event-free until 't'.
I This subgroup is changing over time due to events and deathdue to other causes
26 / 42

Estimation of absolute risk (formula I)
F1(t|X ) = Cumulative incidence of event 1
∫B
A
exp
(−∫
s
0
{λ1(u|X ) + λ2(u|X )}du)
︸ ︷︷ ︸No event of any cause until s
λ1(s|X )︸ ︷︷ ︸Event type 1 at s
ds.
I Cox regression for stroke hazard:
λ1(u|X ) = λ01(u) exp(βX )
I Cox regression for hazard of death other causes:
λ2(u|X ) = λ02(u) exp(γX )
27 / 42

Combination of cause-speci�c Cox regression
Remarks:
I A covariate that reduces the cause-speci�c hazard of acompeting risk indirectly increases the cumulative incidence ofevent j .
I covariates found to change the absolute risk of strokeI either change the cause-speci�c hazard of strokeI or change the cause-speci�c hazard of death other causesI or change both
Disadvantages:
I we need to model all competing risks
I the change of the absolute risk depends on a change of asingle covariate in a complicated way
28 / 42

Estimation of absolute risk (formula II)
It would be desirable to have a model in which the regressioncoe�cients β have the following interpretation:
The absolute risk of a stroke during the next 't' years changes with
a factor exp(β) for a one unit change of age, given �xed values for
the other predictor variables.
Absolute risk regression:2, 3
F1(t|X ) = F01(t) exp(βX ) (Log-binomial model)
Disadvantages:
I estimation of β requires a (regression) model for theprobability of not being lost to followup
I model has numerical problems with e�ects of continuouscovariates
2Absolute risk regression (Stat. med., 2012, 31, 3921�30)3Fine-Gray model: log(-log(-F1(t|X))) = η X; "sub-hazard ratio" η has no
clear interpretation.29 / 42

Prediction & landmarking
30 / 42

Prediction
Kattan: I wanted a tailored predicted probability of survival . . .
Absolute risk given covariates = individual prediction
Requirements:
I time origin: A must be the same for all subjects
I time horizon: B must be the same for all subjects
I a proper account for competing risks
I absolute risk should be calibrated
I no time-dependent covariates: the prediction may not dependon things that are unknown at time A
31 / 42

Landmark analyses (Benn et al. 2014)
Patients were included when at their birthdays when they turned50, 60, 70 and 80 years, respectively.
Individuals were followed until stroke occurred, death or the end ofthe study period, whichever came �rst.
For presentation of risks we choose a prediction horizon of 5-yearsafter inclusion.
The aim is to assess how the risk of stroke changes in presence ofatrial �brillation (AF) compared to absence of AF.
32 / 42

Competing risks and loss to followup
Competing risks
Age
Cum
ulat
ive
inci
denc
e
60 61 62 63 64 65 66 67 68 69 70
0 %
25 %
50 %
75 %
493387 290287 108806
Stroke before deathDeath
% loss to followup
Age
Cum
ulat
ive
inci
denc
e
60 61 62 63 64 65 66 67 68 69 70
0 %
25 %
50 %
75 %
493387 290287 108806
Shown: data for men
33 / 42

Hazard ratio (AF versus no-AF)
Cause-speci�c Cox regression, event: stroke
univariate Cox univariate Cox adjusted* Cox adjusted* Cox
sex male female male femaleAge 60 2.0 2.8 1.6 1.9Age 70 1.7 2.5 1.4 1.8Age 80 1.7 2.4 1.4 1.9
Cause-speci�c Cox regression, event: death without stroke
univariate Cox univariate Cox adjusted* Cox adjusted* Cox
sex male female male femaleAge 60 1.8 2.2 1.3 1.6Age 70 1.8 2.0 1.3 1.4Age 80 1.6 1.9 1.3 1.4
*Adjusted for hypertension, diabetes, vascular disease, previous stroke, heart failure
E.g., the hazard rate is increased by 70% (adjusted 40%) for a menage 70 with AF compared to without AF.
34 / 42

Absolute risks (60 years)
Age
Cum
ulat
ive
inci
denc
e
60 61 62 63 64 65 66 67 68 69 70
0 %
25 %
50 %
75 %
486418 286827 1077926969 3460 1014
Men
No AF at age 60AF at age 60
Women
No AF at age 60AF at age 60
Risk of stroke
AgeC
umul
ativ
e in
cide
nce
60 61 62 63 64 65 66 67 68 69 70
0 %
25 %
50 %
75 %486418 286827 107792
6969 3460 1014
Men
No AF at age 60AF at age 60
Women
No AF at age 60AF at age 60
Risk of death without stroke
35 / 42

Absolute risks (70 years)
Age
Cum
ulat
ive
inci
denc
e
70 71 72 73 74 75 76 77 78 79 80
0 %
25 %
50 %
75 %
289211 144955 504878502 3405 936
Men
No AF at age 70AF at age 70
Women
No AF at age 70AF at age 70
Risk of stroke
AgeC
umul
ativ
e in
cide
nce
70 71 72 73 74 75 76 77 78 79 80
0 %
25 %
50 %
75 %289211 144955 50487
8502 3405 936
Men
No AF at age 70AF at age 70
Women
No AF at age 70AF at age 70
Risk of death without stroke
36 / 42

Absolute risks (80 years)
Age
Cum
ulat
ive
inci
denc
e
80 81 82 83 84 85 86 87 88 89 90
0 %
25 %
50 %
75 %
148515 56296 118289454 2414 351
Men
No AF at age 80AF at age 80
Women
No AF at age 80AF at age 80
Risk of stroke
AgeC
umul
ativ
e in
cide
nce
80 81 82 83 84 85 86 87 88 89 90
0 %
25 %
50 %
75 %148515 56296 11828
9454 2414 351
Men
No AF at age 80AF at age 80
Women
No AF at age 80AF at age 80
Risk of death without stroke
37 / 42

Frequent pro�les (male, age 60)
Risk pro�le no-AF (n) AF (n) 5-yr stroke no-AF 5-yr stroke AF 5-yr death no-AF 5-yr death AF
None 383893 3528 2.4 4.4 4.9 6.7hypertension 43376 1149 3.2 5.3 5.6 8.3diabetes 13110 157 4.6 7.6 9.2 15.0vascular disease 11228 273 5.0 10.2 8.7 7.5diabetes/hypertension 8246 183 4.6 5.4 9.0 17.9previous stroke 7996 158 14.3 20.6 9.0 11.3vascular disease/hypertension 5245 234 4.5 5.9 9.3 6.7previous stroke/hypertension 3240 87 13.7 15.5 7.0 5.1diabetes/vascular disease/hypertension 1286 61 5.9 12.4 15.4 20.1hypertension 1019 326 4.5 6.1 17.8 20.0
05
1015
20 Stroke risk (AF) − Stroke risk (no−AF)
38 / 42

Frequent pro�les (female, age 80)
Risk pro�le no-AF (n) AF (n) 5-yr stroke no-AF 5-yr stroke AF 5-yr death no-AF 5-yr death AF
None 139526 3027 7.5 13.7 20.5 31.3hypertension 43869 1868 8.3 15.0 18.0 25.3previous stroke 9380 721 22.3 36.4 29.4 33.7diabetes 5478 222 12.1 16.1 29.0 42.6vascular disease 5218 350 10.8 17.2 33.0 35.3diabetes/hypertension 4771 268 11.3 16.5 23.1 39.3previous stroke/hypertension 4515 438 20.7 30.3 22.2 30.5vascular disease/hypertension 3892 344 9.4 21.1 30.2 30.3heart failure 2407 745 8.2 17.5 47.1 45.4hypertension 1343 542 9.4 13.3 39.6 41.7
05
1015
20 Stroke risk (AF) − Stroke risk (no−AF)
39 / 42

Summary
A hazard ratio su�ciently answers questions of the form:
Is there an association between AF and the risk is of stroke?
It is however not enough to answer questions of the form:
What the absolute risk of stroke within the next 5 years?
40 / 42

Summary (continued)
To validate a Cox proportional hazard model one needs to consider:
I if the hazard ratio depends on time
I if the hazard ratio depends on risk due to other factors
I selection of the population over time a�ects the interpretation
To predict the absolute risk from a Cox proportional hazard modelone needs:
I a well de�ned time origin (i.e., �rst diagnosis of AF)
I a well de�ned time horizon (i.e., 5 years later)
I a well-de�ned population with su�cient follow-up
I Cox models for competing risks or model for loss to follow-up
41 / 42

Eselsbrücke
Cycling Life
speed hazard rateduration [A,B] absolute risk [A,B]
accident/injury competing risks -> speed zerotunnel loss to follow-up -> assume same speed
doping treatment (baseline)energy bar treatment (time-dependent)muscle status bloodpressure, time-dependent internal covariate
uphill November in Denmark, external covariate
42 / 42