Hand Injuries DPS L L v2

of 3
-
Upload
arielbarbanente -
Category
Documents
-
view
219 -
download
0
Transcript of Hand Injuries DPS L L v2
-
8/13/2019 Hand Injuries DPS L L v2
1/3
ACOUSTIC MAGAZINE OCTOBER 2011
FEATURE
OCTOBER 2011 ACOUSTIC MAGAZINE 19
EATURE PREVENTING INJURIES IN GUITARISTS
PREVENTING INJURIESIN GUITARISTSFOCAL HAND DYSTONIA
By Katherine Butler www.londonhandtherapy.co.uk
Dystonia is a syndromewhere involuntaryprolonged musclecontractions can
ead to sustained twistingpostures.1,2,3If symptoms startbefore 28 years of age thedystonia is classified as earlyonset, but if they start after28 years of age it is classifiedas late onset. Dystonia can befurther categorised into primarydystonia, where there are noobvious effects on the brain, orsecondary dystonia, where a partof the brain (the basal ganglia)may be affected.
Symptoms can be:
General, where symptomsmanifest in all extremities
Hemi, where symptoms arefocused on one side of the body
Segmental, where a sectionof the body is affected, or
Focal, where a single bodypart is affected.
Any part of the body canbe affected by focal dystonia,including the neck, eyelids, vocal
cords or hand.4,5In this article we will look at
focal hand dystonia (FHD), aate-onset, primary dystonia
that is often task-specific andincludes musicians and writerscramp (Fig 1).
Focal Hand DystoniaIn MusiciansFHD in musicians is a primarydystonia that is painless and isusually task-specific, focal and ofate onset. Symptoms can includeack of coordination, cramps and
tremors.6Tey tend to be sp ecificto each individual and related tothe instrument played.
Patients can respond tosensory tricks, and if they do,this is usually a good indicatorof how successful hand therapywill be. Sensory tricks can beused to fool the brain and give anonsense message to the brain.Tis breaks the fixed messagefor a short time.4,7,8Often thenovelty will not be effective forlong and the brain recalibrates tothe automatic dystonic pattern.Coban, Blu-ack, latex gloves
and splints can all be used assensory tricks (Fig 2).
Its estimated that 210%of professional musicianshave focal hand dystonia,9,10,11which is higher than the 0.1%of writers cramp sufferersin the general population.12FHD is overwhelmingly morecommon in classical than inpop, rock or jazz musicians.e high percentage of FHDin this population reflects thespecific demands of continuousrepetition made upon them.Musicians who suffer from focalhand dystonia may be geneticallypredisposed to developing this
condition, and then excessiveplaying or overtraining may bringit on. Ongoing work to identifyabnormal genes in patients withfocal dystonia continues andresults of further studies areeagerly awaited.
Who Develops FHD?Many factors can triggerthe development of FHD inmusicians, such as a suddenincrease in playing time, changein technique, return to playingafter a long break, trauma,
history of nerve entrapment,psychological aspects or changeof instrument. Repetitivemovements can inducestereotypical feedback messages,which lead to disorganisation inthe area of the brain that controlshand movement (sensory cortex)and a failure in coordinationbetween sensory and motormessages to and from the brain(sensorimotor integration).Tis can lead to uncoordinatedmovement (Fig 3).
reatmentsAt present there is no curefor dystonia, and many ofthe treatments availablehave significant limitations.Current treatments includeoral medication, Botulinumtoxin injections, surgery,rehabilitative therapies andsupportive approaches. Butlerand Rosenkranz13,14publishedtwo papers that clearly outlinemany of the treatments that havebeen researched and trialled withpatients who are aected by FHD.
The rehabilitative
approaches include: Sensory re-education Sensory motor retuning (SMR) Slow- down exercise therapy
(SDET)
Fig 1. Task-specific action-induced focal hand dystonia has different forms, including musicians dystonia, which canaffect the hand and embouchure (a), and writers cramp (b).
a) b)
Fig 2a. A p last ic sp li nt b ei ng u se d a s a s enso ry tr ick . Fig 2b. A l ycr a fing er s le eve a nd p las ti c s pl int bei ng use d as a se ns or y t ri ck .
playing the piano. Te authorsconclude that proprioceptivetraining applied for only 15minutes significantly restoredthe pattern of sensory motororganisation in musicians dystoniaand improved motor performanceon the piano objectively andsubjectively for up to 24 hours.Tis intervention is a highlypromising tool for rehabilitationand it is hoped that furtherinvestigations into this excitingtreatment technique can continue.
Sensory re-education is atreatment technique used atLondon Hand erapy and
many patients respond well to it.Careful explanation and massiveamounts of encouragement arerequired for a patient to continuewith this treatment techniquelong enough for the sensorychanges to occur and for theeffects to be noticed whileplaying their instrument.
Sensory MotorRetuning (SMR)Te compensating finger is fixedin a splint while the dystonicfinger carries out exercises.23Tese exercises are completedunder supervision and involveone or more of the other digits to
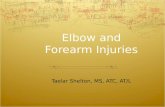
Figures 3a, b and c. Manipulatingembossed items such as dominoes(a), identifying sensory stimulation(b) and discriminating and matchingcommon household items (c).
Figure 3: Byl model of focal hand dystonia in humans showing impairment ofthe sensorimotor feedback loop.
sensorimotor integration fails
induces motorincoordination
disorganisation insensory cortex
induces stereotype & repetitivemovement feedback messaging
repetitive movements
showing impairment of the sensorimotorfeedback loop.
a)
b)
c)
Multi-disciplinary approach Limb immobilisation Supportive approaches
In this paper some of the morecommonly used treatmenttechniques and current researchfindings will be explored.
SensoryRe-educationRepetitive motions can induceplasticity changes in the sensorycortex, which may degradethe hand representation andinterfere with motor control.15,16Using sensory training to treatpatients with FD is raisedthrough this research. Sensoryre-education programmesfacilitate and positively influence
the relearning process andimprove function. Sensorydiscrimination training is taughtas part of the home exerciseprogramme.17,18,19However, thesame number of repetitionsthat lead to the disorder maybe required to restore the handrepresentation, so cooperationis essential when using thistreatment technique.15,16
o facilitate normal sensationand perception, and reinforce handfunction, patients are asked tovisualise healing, imagine normalsensory processing, motor controland task execution. Byl expectspatients to complete 12 hoursa day of sensory discriminationactivities at home.17Teseactivities can include: matchingobjects/shapes or textures,braille reading, or identifying andmanipulating common householdobjects with vision occluded(Figure 3a, b and c).
Zeuner et al20report on their
studies of the efficacy of learningto read Braille as a method ofsensory training for patientswith focal hand dystonia. Teauthors conclude that training inBraille reading improves spatialdiscrimination and decreases thelevel of disability in patients withfocal hand dystonia. Tey alsoshow that sensory training lastinglonger than eight weeks may leadto continued improvement.21
Rosenkranz et al22presentproprioceptive (awareness ofwhere your body is in space)training as a sensory interventionin order to assist in increasingcontrol of movements while
-
8/13/2019 Hand Injuries DPS L L v2
2/320 ACOUSTIC MAGAZINE OCTOBER 2011
FEATURE PREVENTING INJURIES IN GUITARISTS
exercise for up to 2.5 hours perday for eight consecutive days.24,25
It is believed that SMRproduces functionalimprovement associated with
neuronal reorganisation. Candiaet al24present results of 11professional musicians who took
part in a prospective case seriesthat had a follow-up comparisongroup of 325 months for
piano and guitar subjects and04 months for oboe and flutesubjects. SMR was seen as beinga valuable treatment technique
for pianists and guitarists aseach patient displayed improvedperformance without the splint.
reatments that alter movementpatterns may provide assistance
to patients with FHD.
Slow-Down ExerciseTerapy (SDE)An exercise called slow-downmovement therapy (SDET) that
Sakai26presents, works very wellwith guitarists, even though theinitial research was performed
using pianists. Te therapyfollows these five steps: e patient chooses a piece
of music that causes a dystonichand movement.
e performance speed is
reduced until there is nodystonic movement evidentand the metronome marking
is noted.
At this slow tempo the patientrehearses the piece for half anhour per day for two weeks
and is allowed to play otherpieces freely.
After two weeks the speed is
increased by 10%. If symptomsdo not appear with thisincrease in speed the patient
proceeds to practise for anadditional two weeks at thistempo. If the dystonic
movement does reappear thenthe speed is decreased.
After two weeks the speed
is gradually increased again byanother 10%, and theprogramme continues.
SDE therapy teaches a patient to
reduce the speed of movementbelow the level where memoriesand emotions associated withdystonia exist. Movement patternsare then retrained. Tis treatment
technique is utilised in the clinicsetting with great effect. Manypatients find it encouraging being
able to play their instrument freelywhen not doing the slow-downexercises and appreciate mapping
their progress by looking at themetronome markings.
Hand Terapy & TeMulti-disciplinaryeam (MD)No single treatment modality
seems to be effective for the
treatment of FHD. When
treating musicians an MDapproach can be very helpfuland necessary. Tis team will
frequently include: the musician,neurologist, hand therapist,music teacher, instrument maker
and psychologist.MD treatments can include
traditional hand therapymodalities, encouraging
rest, psychological support,modifications to the instrument,Alexander technique or
Feldenkrais therapy, mirrortreatment techniques andretraining the whole body and
associated movement patterns. Abrief outline of each of the abovetreatments will follow.
raditional hand therapymodalities include splinting(Figure 4a, b and c), adaptive
devices, heat, ice, exercise,strengthening, rehabilitation andpreventative measures against
the development of FHD. Soft-
tissue massage may be requiredto decrease muscular tension.Education and liaison with the
teachers and other members ofthe MD are integral.
Dystonic movements occur
predominately while performingperceptual motor tasks involvingemotion. Tere is difficulty
changing emotional andmotor traces that have becomeassociated, and this may lead
to preservation of dystonicsymptoms. Emotional support orreferral for professional help may
be necessary for some patients.Modifications to the
instrument may assist in
decreasing symptoms through
eliminating postural triggers(Fig 5). Modications could
include: changing to a smallerinstrument, altering location ofthumb on neck of instrument
or altering tension or type ofstrings. Playing positions canalso be changed, ie standing up,
kneeling or lying down to play.Feldenkrais and Alexander
techniques can help patients gain
awareness of control, with simplemovements being practised andthen more complex patterns beingintroduced once muscle activity
and relaxation have been learnt.28
Chamagne29particularlyfocuses on increasing shoulder
control. I use arm-swinging
Figs 4b and c. Splints can assist in retraining movement patterns and can block movements or act as a sensory trick.27
Fig 4a. Blocking splints made ofplastic.
b) c)
-
8/13/2019 Hand Injuries DPS L L v2
3/322 ACOUSTIC MAGAZINE OCTOBER 2011
FEATURE PREVENTING INJURIES IN GUITARISTS
exercises in the clinical settingfrequently and integrate them
into the patients home exerciseprogramme, and many peoplereport these as being veryeffective and helpful.
Mirror treatment techniqueswere first used with patientssuffering from phantom limb.30When using this technique withdystonic patients, instant visual
feedback with mirrors can helppatients recognise dystonicand non-dystonic movements.
Te mirror is positioned so themusician can see the uninjuredhand looking like the injuredone. Te illusion is created and
the brain thinks there is activityin the injured hand.31It is very
useful to use this techniquewith pianists in particular, asboth hands are performing
similar motions. Tis techniqueis not so easily translated toinstruments such as the guitar
as the hands perform suchdierent movements. However,this technique can be useful
in retraining basic movementpatterns in guitarists and isused frequently within the clinic
setting to assist guitarists in
Fig 5: Instrument modifications can include using supports that alter theposition of the guitar, and this can lead to a change in arm and hand positionsthat may assist in decreasing postural triggers.
retraining hand movements awayfrom the instrument.
Prevention Is BetterTan Cure!Animal studies show that highlyrepetitive motor movementscontribute to disorganisation in
the area of the brain that controlsthe hand.
Protect yourself:
Vary the speed and force ofrepetitive movements.
Maintain your instrument in
top playing condition to reduceexcessive energy outlay.
Intersperse practice with
other activities. Control stress and anxiety
before a performance andpractice sessions.
Conclusionse mechanisms by which FDdevelops in musicians need to
be identified. reatment mustassist in re-establishing the linkbetween sensory and movement
control and commands. Acomprehensive therapy andhome exercise programme
with sensory re-education as
a focus can improve sensoryprocessing and motor controlof the hand. SMR, slow-down
exercise therapy, and handtherapy techniques are of valuewhen treating FD in guitarists.A whole-body approach must
be adopted when treating thispatient group and regular reviewand assessment of the musician
playing their instrument is
essential. Scientic researchinvestigating preventativemeasures and appropriate
treatments for FHD is essential.Collaboration and an MDapproach to prevention,
treatment and research areimperative and will benefit all.Katherine Butler
1.Fahn, S (1998). Concept and classication of dystoniaClinical Neuropharmacology 9(2): S37S48
2.Fahn S, Bressman SB and Marsden CD (1998).Classification of dystonia Advances in Neurology 78:110
3.Fahn S, Marsden CD and Calne DB (1987).Classification and investigation of dystonia In CDMarsden and S Fahn (Eds.) Movement Disorders 2,London: Butterworths.
4. Berardelli A, Rothwell JC, Hallett M et al. (1998).Te pathophysiology of primary dystonia Brain121:11951121
5. Deuschl G and Hallett M (1998). Focal dystonias:from occupational cramp to sensorimotor disease thatcan be treated Aktuelle Neurologie 25: 320328
6. Jankovic J and Shale H (1989). Dystonia in musiciansSeminars in Neurology 9: 131135
7.Hallett M (1995). Is dystonia a sensory disorder?Annals of Neurology 38(2): 139140
8. Lederman RJ (1991). Focal dystonia ininstrumentalists: Clinical features Medical Problems ofPerforming Artists 6: 132136
9.Jabusch HC (2006). Epidemiology, phenomenologyand therapy of musicians cramp In: Altenmller E, ed.Music, Motor Control and the Brain. Oxford UniversityPress: Oxford
10.Brandfonbrener AG (1995). Musicians with focaldystonia: A report of 58 cases seen during a ten-yearperiod at a performing arts medicine clinic MedicalProblems of Performing Artists 10(4): 121127
11. Lim VK, Altenmller E and Bradshaw JL (2001).Focal dystonia: Current theories Human MovementScience 20: 875-914 Clinical lecture on certainconditions of the hand and arm which interfere withthe performances of professional acts, especially piano-playing British Medical Journal 1: 441444
12.Nutt JG, Muenter MD and Melton IJ (1988).
Epidemiology of dystonia in Rochester, MinnesotaAdvances in Neurology 50: 361365
13.Butler K and Rosenkranz K (2006) Focal HandDystonia affecting musicians. Part I: An overview ofepidemiology, pathophysiology and medical treatmentse British Journal of Hand erapy 11(3): 7278
14.Butler K and Rosenkranz K (2006) Focal handdystonia affecting musicians. Part II: An overview ofcurrent rehabilitative treatment techniques Te BritishJournal of Hand erapy 11(3): 7987
15. Byl N, Merzenich MM and Jenkins WM (1996a). Aprimate genesis model of focal dystonia and repetitivestrain injury: Learning-induced dedifferentiationof the representation of the hand in the primarysomatosensory cortex in adult monkeys Neurology47(2): 508520
16.Byl N, Wilson F, Merzenich M, Melnick M, Scott P,Oakes A and McKenzie A (1996b). Sensory dysfunctionassociated with repetitive strain injuries of tendonitisand focal hand dystonia: A comparative study Journalof Orthopaedic and Sports Physical erapy 23(4):234244
17.Byl NN and McKenzie A (2000). Treatmenteffectiveness for patients with a history of repetitivehand use and focal hand dystonia: A planned,prospective follow-up study Journal of Hand erapy13(4): 289299
18.Byl NN, McKenzie A, Nagarajan SS (2000).Differences in somatosensory hand organization in ahealthy flutist and a flutist with focal hand dystonia: acase report Journal of Hand erapy. 13(4):3029.
19.Byl N and Topp KS (1998). Focal hand dystoniaPhysical Terapy Case Reports 1(1): 3952
20. Zeuner KE, Bara-Jimenez W, Noguchi PS, GoldsteinSR, Dambrosia JM, Hallett M (2002). Sensory trainingfor patients with focal hand dystonia Annals ofNeurology. 51(5):5938
21.Zeuner KE, Hallett M (2003). Sensory training as
treatment for focal hand dystonia: a 1-year follow-upMovement Disorders. 18(9):10447
22. Rosenkranz, K, Butler, K, Cordivari, C, Lees, A,Williamon, A and Rothwell JC (2008). Behavioural andneurophysiological effects of proprioceptive training inmusicians dystonia Movement Distorders 23: S165
23. Candia, V., Elbert, T., Altenmller, E., Rau, H.,Schafer, T. and Taub, E. (1999). Constraint-inducedmovement therapy for focal hand dystonia in musi-cians. Lancet 353: 42.
24.Candia, V., Wienbruch, C., Elbert, T., Rockstroh, B.and Ray, W. (2003). Eective behavioral treatment offocal hand dystonia in musicians alters somatosensorycortical organisation. Proc Natl Acad Sci USA 100:79427946.
25. Candia, V., Schafer, T., Taub, E., Rau, H.,Altenmller, E., Rockstroh, B. and Elbert, T. (2002).Sensory motor retuning: A behavioural treatment forfocal hand dystonia of pianists and guitarists. Arch PhysMed Rehabil 83: 13421348.
26. Sakai N (2006). Slow-down exercise for thetreatment of focal hand dystonia in Pianists MedicalProblems of Performing Artists March: 2528
27. Butler K and Svens B (2005) A Functional umbMetacarpal Extension Blocking Splint Journal of HandTerapy, (18:3) 375377
28.Jabusch HC, Muller SV and Altenmller E (2004).Anxiety in musicians with focal dystonia and those withchronic pain Movement Disorders 19(10): 116975
29.Chamagne P (2003). Functional dystonia inmusicians: rehabilitation Hand Clinics 19(2): 30916
30.Ramachandran VS and Hirstein W (1998). eperception of phantom limbs e D.O. Hebb lecture.Brain 121: 160330
31.Rosen B Lundborg G (2005). Training with a mirrorin rehabilitation of the hand Scandinavian Journal ofPlastic Reconstructive Hand Surgery 39(2): 1048
References