Oppression of Minority Shareholders- Protecting Minority Rights
Upload
erick-henryCategory
view
215download
1
Haemoglobinopathy , a challenge in service design
Prevalence very variableMinority communities
Little political “ muscle “ English not first language
Often low socio-economic status Asylum seekers
Seen as “ not our problem “
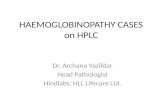
Sickle cell disease is the most common genetic condition in England, with higher prevalence than cystic fibrosis
Highest prevalence of SCD occurring in people of African and Afro-Caribbean origin, with birth prevalence as high as 1 in 300 in some areas whilst Thal more common in Asian and Southern European (recessive)
Affects an estimated ~10,000 individuals (audit 2008)
Reported in more than 1 in 2,000 live births
Most common inherited disease of Caucasians (recessively inherited)
Affects an estimated ~8,400 individuals
Reported in more than 1 in 2,500 live births
Sickle Cell Disease & Thalassemia1
Cystic Fibrosis2
In the UK, sickle cell disease is as prevalent as cystic fibrosis – the only difference is in the ethnic group most likely to be impacted
1. Source: Development of transcranial Doppler screening services in England, Dianne Addei, Nov 20072. Source: Specialist Services National Definitions Set (2nd Edition)
The Process
• Define population at risk demographics, numbers and disease
• what exists at present • what do we aspire to ,define standards • what is the gap • how to move from existing services to
new clinical units• how to maintain /continually improve
services

Haemoglobinopathy Forum survey of existing resources
• 65% see 5 or less Sickle per year
• 88% see 5 or less Thal per year
• Of 21 units seeing greater than 20 children with Sickle 17 in London
• Response from 88%

??
?
?
UK Thalassaemia Register
1999:807 patients / 164
doctors
71 only 1 attending77 2 – 9
patients12 10 – 304 > 50
11 doctors @ 9 sites saw 20 or more
patients

Survey ( cont)
• of smaller units < 20 per year 76% would treat painful crises but only 40% would treat Acute chest or Priapism
• Of larger units 14 would refer on for neurologic episode needing MRI and for ICU facilities
• Only 6 units have facility for TCD

Conclusions
• Services best described as “patchy”
• Little organisation about who does what
• Particular concern is links or not of small units
• Urgent need for standards and agreed networks of care

Drivers for change
• Screening programme • Standards for adults and children • Treatment/care for long term conditions • NCEPOD report into Haemoglobinopathy
mortality • Haemoglobinopathy coming under SSA
remit • Patient expectations
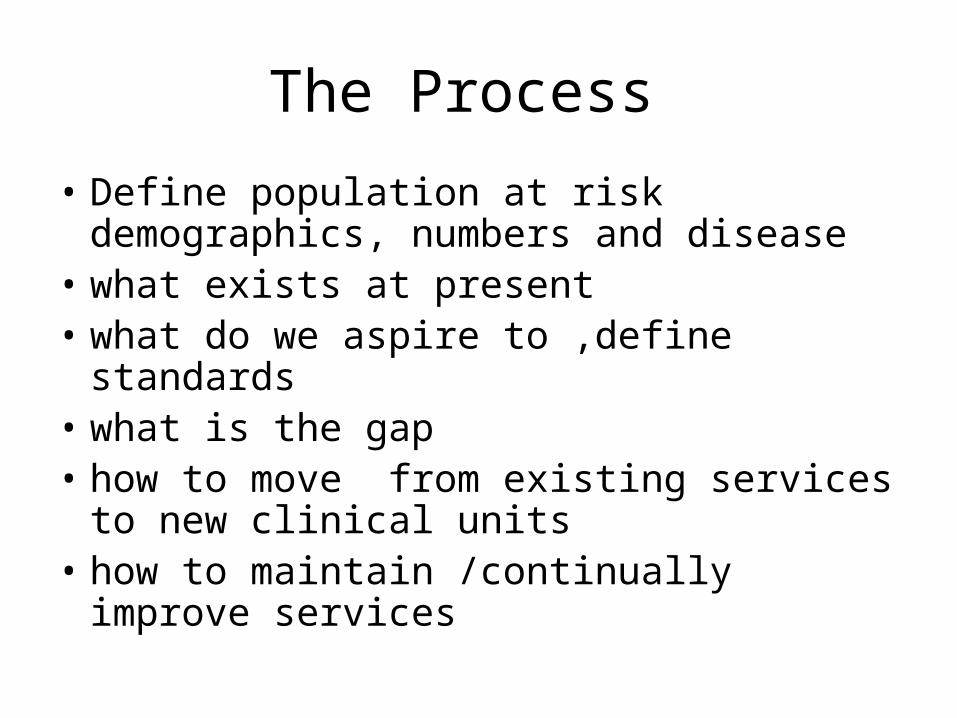
Super-specialist services eg specifically experienced
BMT, fertility clinic
Clinic
Clinic
Centre
Specialist Team
Annual Review
Special investigations
New treatment options
Liaiases with Clinic / GP
Clinic undertakes: regular transfusions and pre-transfusion review, offers ready access, prescribes chelation, regular tests.
Refers / liaises with Centre
Primary care, outreach and community
services
WORK
All need informedfront line / A&E staff

What is missing
• Any infrastructure , need agreement on core components
• Detailed data
• Tariffs fairly basic
• Understanding of how they will be supported long term
• An overview of training and education needs of the networks .
Standards
• Thalassaemia major completed three years ago
• sponsored by Thalassaemia society
• multidisciplinary group
• backing of DH
• main theme is promoting the development of a patient and family centred service .

Sickle Standards
• Again produced by multidisciplinary group including patient representative group Sickle cell society
• Themes very similar to Thal
• Define specialist units and relationship to smaller units
• Defines good /best practice

What exists at present
• Clinical standards • Specialist definition • Some very well developed formal and
informal groups • Commissioner engagement • Some excellent practise • Registry • Goodwill

The national strategy for Haemoglobinopathy services would drive
improvements in care and services
• Develop best practice care pathways
From: Screening and diagnosis
To: Treatment and prevention of major illnesses
Involving: health and social care
Resulting in : Reduced A&E burden– Support for patients living with HbO
• Improve service delivery
– Design best practice service delivery model to improve consistency and equity of service provision (hospital and community)
– Roll out hub and spoke model of service centres to enhance provision
– Enhance commissioning
– Review funding
– Improve training and education (NCEPOD)
– Collect and analyse data (NCEPOD)
• Make available the right care, advice and treatment• Tackle inequities • Build for the future
• Design Sickle services for the future– Review workforce requirement (specialist services)– Support national leadership
1
2
3

In order to address the unmet needs of sickle cell patients, a comprehensive national strategy is urgently required
A national strategy for managing sickle cell disease would deliver
multiple benefits …
Raise the profile of sickle cell disease
across England
Drive improvements in care and services
With policy makers
With clinicians and care providers
With commissioners(at both PCT and SCG level
Involving patients and the Sickle cell society
Design Sickle services for the future
Develop best practice care pathways
Improve service delivery
1
2
3

Objectives
• Gathering information about individual units on behalf of DH ,up to date picture of secondary and tertiary services
• Performance in key areas against standards • Nature of existing clinical networks • Nature of present commissioning arrangements • Perceived gaps in services and how to improve • Inform DH strategy
What is in process
• Peer review
• Expansion of Registry to include adverse event reporting and annual review
• Specialist commissioning overview

Some themes
• Inequality both within individual networks and between networks .
• Access
• Community/specialist nursing support
• manpower ,psychology particularly poor .
• Second string to cancer
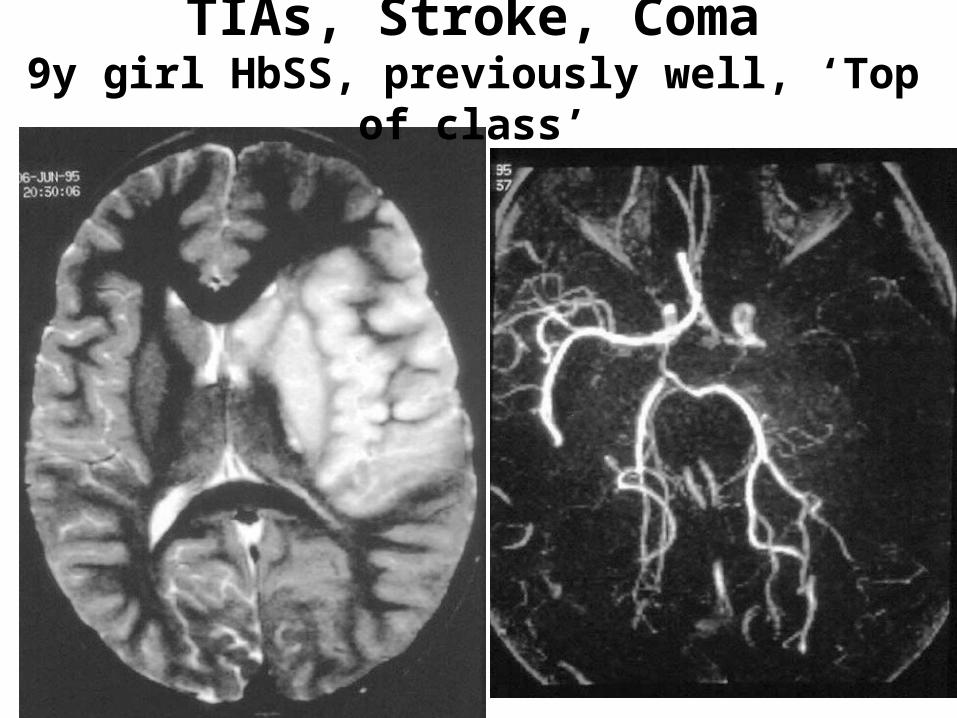
TIAs, Stroke, Coma9y girl HbSS, previously well, ‘Top of class’

Moyamoya
Severe stenosis or occlusion of the terminalinternal carotid artery / proximal middlecerebral artery with collateral vessels Yoon 2000

TCD
• Great change from 4 years ago
• Theoretical coverage now good only a couple of areas without firm plans to get in place this year .
• Challenge now to increase uptake , use of one stop clinics , outreach combined with annual review
• Training programme tenders now out .
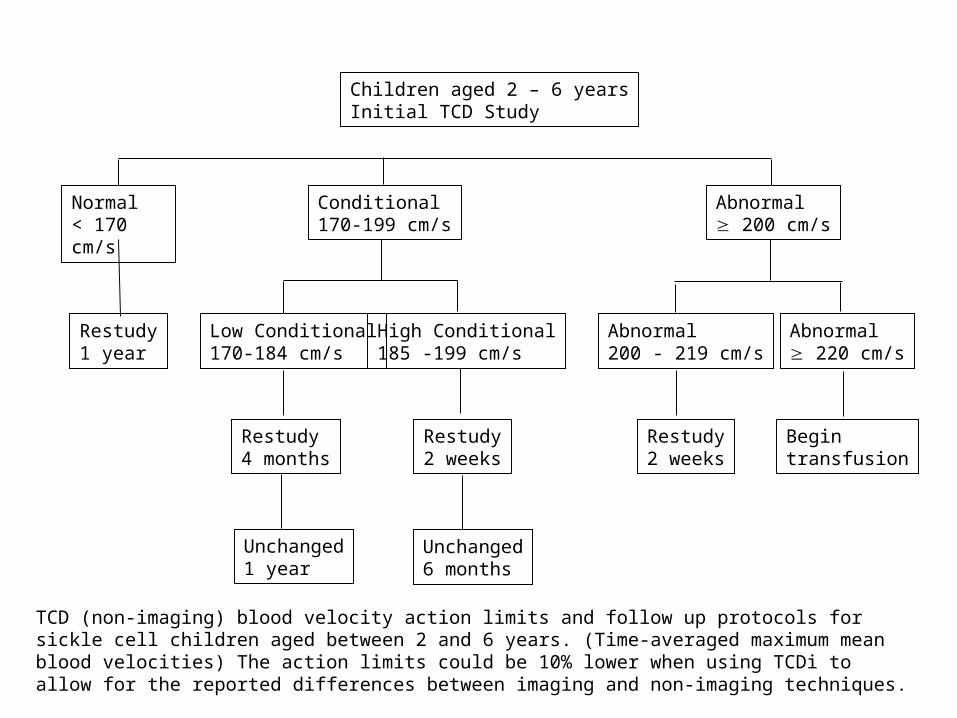
Children aged 2 – 6 yearsInitial TCD Study
Normal< 170 cm/s
Conditional170-199 cm/s
Abnormal 200 cm/s
Restudy1 year
Low Conditional170-184 cm/s
High Conditional185 -199 cm/s
Restudy4 months
Restudy2 weeks
Unchanged6 months
Abnormal200 - 219 cm/s
Abnormal 220 cm/s
Restudy2 weeks
Begin transfusion
Unchanged1 year
TCD (non-imaging) blood velocity action limits and follow up protocols for sickle cell children aged between 2 and 6 years. (Time-averaged maximum mean blood velocities) The action limits could be 10% lower when using TCDi to allow for the reported differences between imaging and non-imaging techniques.

Specialist nursing
• Probably biggest area of unmet need
• Need for flexibility in low prevalence areas
• suggestion that screening has possibly reduced time available from community side .

Community support
• Vast range of arrangements , some excellent ,some not !
• Good ones typified by leadership and clarity of roles between Acute Trust and community work
• Little use of new recommendations about planned care packages in long term conditions . .

Specialist nursing/community
• Many trusts need to go back and look at what is needed –ask the patients
• Define existing resource , formalise agreement about who does what
• Look for resource if not available ,
• Must be seen as a whole package
Specialist/community
• Too often service artificially limited by PCT boundaries .
• Too often operating as separate teams
• Need to include patient groups more in design , monitoring problem solving in this area .
Access
• Huge variation , again some very good arrangements in low prevalence Trusts ,more easily able to individualise treatment
• sometimes second string to cancer
• Many continue to be less than satisfied that A and E performance often based on audit data . .
Access
• Open access and use of either dedicated day case or Haematology day case areas seemed to give high level of satisfaction
• Use of A and E with some for of alert , fast track , patient held care plan , next
• Lowest level of perceived satisfaction (mainly among providers ) was A and E with no special arrangements .

High/Low prevalence
• Challenges very different
• How to keep up interest/expertise /training
• Can often be more flexible
• Innovative use of components of other services
• Again leadership key factor .

Transition
• All had arrangements in place
• Works most easily when adult/Paed service on same site
• Surprisingly little use of compatible protocols
• Widespread anxiety/dissatisfaction at services available for the young adult .

Neonatal screening
• All had clear pathways from result to getting result to clinician/family
• Not an automatic link to larger centre
• Not always clear whose responsibility to ensure patient actually has been seen .

Thalassaemia
• Distribution very different from Sickle
• All comfortable with concept of regular review at a larger centre even if already had high Sickle expertise
• Tendency sometimes to get lost in Sickle numbers
Transfusion
• • Little flexibility
• Minimal use of patient/family orientated transfusion
• Exchange programmes not readily available
• Smaller units often able to be more flexible than larger ones

MRI T2*MRI T2*Lack of Correlation: Liver and Cardiac IronLack of Correlation: Liver and Cardiac Iron
LiverLiverLiverLiver

Procurement
• A variety of different arrangements
• Chelation drugs outside tariff from April 09 so likely that individual application to PCT unless your network negotiates a different arrangement .

Comparison of Currently Available Iron Chelators
Approved in US, Switzerland, and
30 countries
Licensed outside US/Canada
(approved in 46 countries)
LicensedStatus
FaecalUrinaryUrinary, faecalExcretion
12-16 hr3-4 hr20-30 minHalf-life
Oral
(Once daily)
Oral
(3 times daily)
SC, IV
(8-12 hr, 5 d/wk)Route
20-307525-60Usual dose(mg/kg/d)
DeferasiroxDeferiproneDesferrioxamineProperty

Networks
• What should they have in place --• Regular meetings , morbidity/mortality • Network audits ,performance in key areas • Discussion development of at least compatible
policies /protocols • Defined referral pathways • Defined governance responsibilities • A forum for patient engagement • Data collection

Networks
• Dissemination /development of good/innovative practice
• Key link with local commissioners
• ? Investigation of adverse events /incidents
• Links with a national group
• Client group involvement
What do commissioners want
• To be offered sensible proposals for all aspects of care in Haemoglobinopathy that are affordable !
• To deal with a small number of key groups • Not to see a proliferation of “ specialist “
arrangements . • They will be looking critically at London , they
want a pan London implementation group to develop services in conjunction with professional leads .
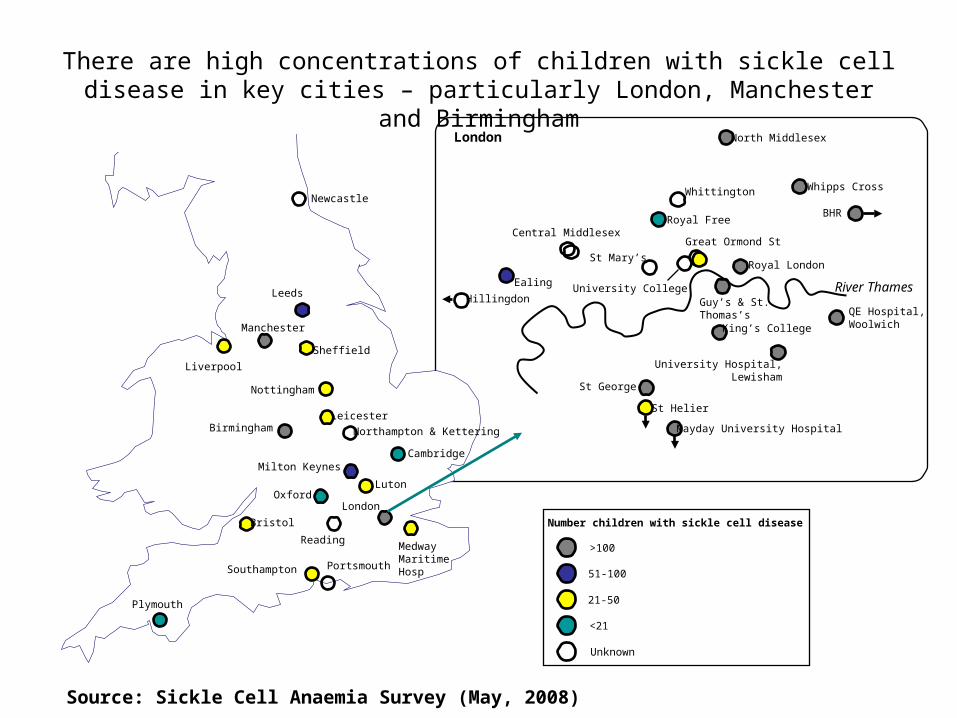
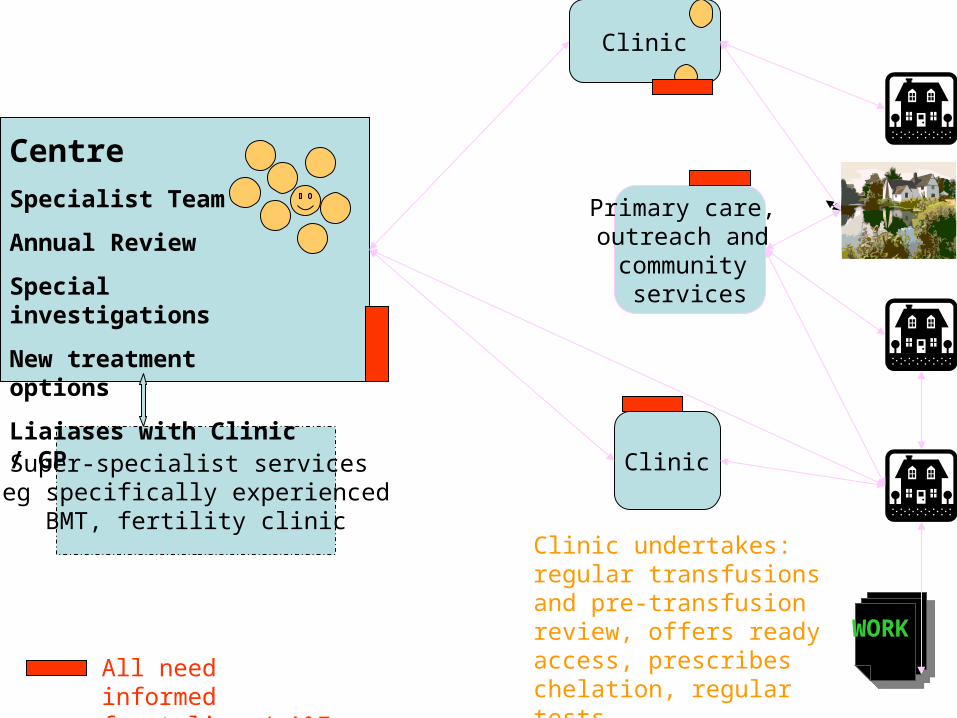
There are high concentrations of children with sickle cell disease in key cities – particularly London, Manchester and Birmingham
Milton KeynesCambridge
Luton
London
Sheffield
Nottingham
Leicester
Northampton & Kettering
Newcastle
Leeds
Manchester
Liverpool
Oxford
Portsmouth
Bristol
Birmingham
Reading
Southampton
Plymouth
Royal London
Great Ormond St
Whipps Cross
Central Middlesex
Whittington
University College
Royal Free
North Middlesex
St Mary’s
Ealing
Hillingdon
King’s College
Guy’s & St. Thomas’s
University Hospital, Lewisham
QE Hospital, Woolwich
St George
St Helier
River Thames
London
51-100
21-50
<21
>100
Number children with sickle cell disease
Unknown
BHR
Medway Maritime Hosp
Mayday University Hospital
Source: Sickle Cell Anaemia Survey (May, 2008)
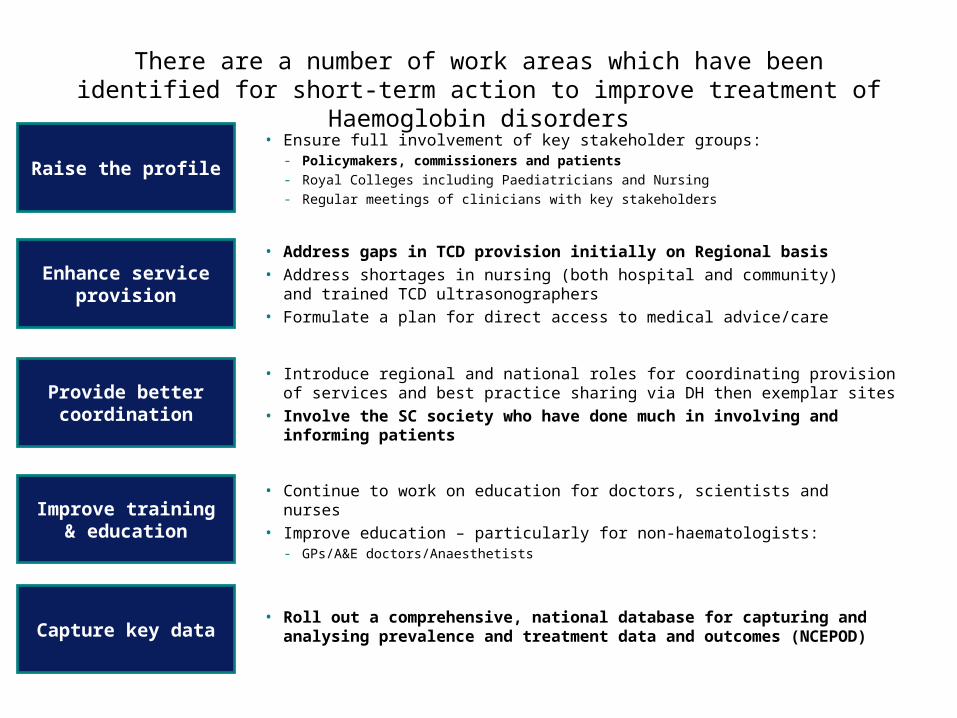
There are a number of work areas which have been identified for short-term action to improve treatment of Haemoglobin disorders
Enhance service provision
Improve training & education
Raise the profile
• Address gaps in TCD provision initially on Regional basis• Address shortages in nursing (both hospital and community) and trained
TCD ultrasonographers• Formulate a plan for direct access to medical advice/care
• Continue to work on education for doctors, scientists and nurses • Improve education – particularly for non-haematologists:
- GPs/A&E doctors/Anaesthetists
• Roll out a comprehensive, national database for capturing and analysing prevalence and treatment data and outcomes (NCEPOD)Capture key data
Provide better coordination
• Ensure full involvement of key stakeholder groups:- Policymakers, commissioners and patients- Royal Colleges including Paediatricians and Nursing - Regular meetings of clinicians with key stakeholders
• Introduce regional and national roles for coordinating provision of services and best practice sharing via DH then exemplar sites
• Involve the SC society who have done much in involving and informing patients