H1N1 in Scotland: Epidemiology and Surveillance
34
H1N1 in Scotland: Epidemiology and Surveillance Chris Robertson, Kim Kavanagh, Adam Wagner Jim McMenamin, Heather Murdoch, Arlene Reynolds, Eisin Shakir, Martin Donaghy Strathclyde University Health Protection Scotland
description
H1N1 in Scotland: Epidemiology and Surveillance. Chris Robertson, Kim Kavanagh, Adam Wagner Jim McMenamin, Heather Murdoch, Arlene Reynolds, Eisin Shakir, Martin Donaghy Strathclyde University Health Protection Scotland. Initial Cases Containment phase up to 5 th July - PowerPoint PPT Presentation
Transcript of H1N1 in Scotland: Epidemiology and Surveillance

H1N1 in Scotland:Epidemiology and Surveillance
Chris Robertson, Kim Kavanagh, Adam Wagner
Jim McMenamin, Heather Murdoch, Arlene Reynolds, Eisin Shakir, Martin Donaghy
Strathclyde University Health Protection Scotland

• Initial Cases– Containment phase up to 5th July
• Surveillance in Scotland– GP Consultation Rates– NHS24 telephone– Mortality– AntiViral Prescriptions

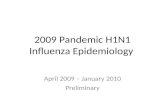
Epidemic Curve during Containment Phases
Date of symptom onset
Count of Cases
temporary change in the implementation of the containment policy led to a cessation of universal swabbing in South Glasgow (the then “hotspot” for transmission)
Schools closing

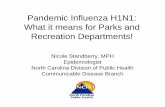
Geographical location of initial cases

Geographical location of initial cases

Deprivation

Summary• Initial outbreak• Predominantly located in Glasgow area
– But evidence of spread throughout central Scotland• Mainly those aged 0-25 affected
– But not heavily weighted among school age children• Mainly those in high deprivation groups affected • Serial interval median of 3 days, range 0-10• R0 – average number of new infections• 1.31 (95% CI 1.30-1.32) Exponential Method• 1.25 (95% CI 1.23 – 1.27) Wallinga Teunis (AJE, 2006)
Colleagues at Health Protection Agency, Colindale:
Ben Cooper, Marc Baguelin, Stefan Flasche, Nick Andrews

Surveillance
• GP Consultation Rates– Sample of nasal swabs from patients
presenting at GPs with acute respiratory symptoms
• NHS24 telephone• Mortality• AntiViral Prescriptions• Hospitalisations
Weekly HPS Situation Report Influenza A H1N1v
http://www.hps.scot.nhs.uk/resp/swineinfluenza.aspx

General Practitioners• There are 1031 Scottish GP practices• 14 Health Boards
– 3 very small (Western Isles, Orkney, Shetland)– 1 has over 25% of population (Greater Glasgow and
Clyde) • Four main software systems for recording their patient
consultation information. – GPASS (67% of practices)– EMIS (8%)– INPS (Vision) (24%)– Ascribe (1%)
• Furthermore, 58 practices within Scotland are part of the PTI network.

Pandemic Influenza Primary care Reporting (PIPeR)
This system has been designed from the outset to meet the surveillance needs in the event of a pandemic of influenza developing.
The scheme is drawn from GP practices which participate in the Practice Team Information (PTI) scheme (formerly the Continuous Morbidity Recording – CMR – team) coordinated by NSS ISD.
This is a network of GP’s who receive an annual financial incentive to record all of their practice data electronically.
The clinical component presents both ILI and Acute Respiratory Infections (ARI) in recognition of the previous finding that many individuals (particularly children) have their influenza recorded under an ARI rather than an ILI category.
All ILI and ARI Read Codes are extracted daily

Location of PTI Practices
PiperGpassEMISVision
• 37 of the 58 practices– All 37 run GPASS
• 211542 Patients – 4% Scottish
Population– Not a total
geographic coverage

020
4060
8010
012
014
0All Patients
ILIARI excluding Asthma - PIPER LEVEL 4
2003-10-01 to 2009-09-07
Dai
ly C
onsu
ltatio
n R
ate
per 1
0000
0
2004 2005 2006 2007 2008 2009

020
4060
8010
012
0
2008-10-01 to 2009-10-26
Dai
ly C
onsu
ltatio
n R
ate
per 1
0000
0
2009 2010
Data2008/09 Trend99% Confidence Limits
2007/08 Trend
Consultation Rates PIPeR Practices

Model
i
iiii mwds log
iiii yVarODPy ),(~
idsiw
Expected Count on Day iSpline trend for Day (time) knots every week
= 1 of Day i is a weekend or holiday,
=0 otherwise
Observed Count on Day i
ih = 1 of Day i is a Monday,
=0 otherwise
Library mgcv in R

050
100
150
2008-10-01 to 2009-10-26
Dai
ly C
onsu
ltatio
n R
ate
per 1
0000
0
2009 2010
Data2008/09 Trend99% Confidence Limits
2007/08 Trend
Consultation Rates PIPeR Practices Age 5-14

020
4060
80
2008-10-01 to 2009-10-26
Dai
ly C
onsu
ltatio
n R
ate
per 1
0000
0
2009 2010
Data2008/09 Trend99% Confidence Limits
2007/08 Trend
Consultation Rates PIPeR Practices Age 15-64

NHS24• Confidential health advice and information
service for people in Scotland • NHS 24 works in partnership with local NHS
Boards out-of-hours services to provide patients with health advice and help when GP practices are closed.
• About 25,000 – 40,000 total calls per week• Surveillance system running since Jan 2004
monitoring 12 syndromes in 14 health boards

Modeli iii wd log
iiii yVarODPy ),(~
j j
jjj ypn
21,1maxˆ
2161
32
32
21
1ˆ
ˆˆ2
3
jjj
jjj
h
yr
Farrington CP, et al. A Statistical Algorithm for Early Detection of Outbreaks of Infectious Disease. Journal of the Royal Statistical Society Series A 1996; 159:547-563
id
iw
Expected Count on Day iDay
= 1 of Day I is a weekend
or holiday, =0 otherwiseObserved Count on Day i
2,1max jj r

Date, beginning in 2008
Cou
nt
01/10 30/11 29/01 30/03 29/05 28/07 26/09
050
010
0015
00
ObsExpUL
Scotland.CR ColdsFlu99% Exceedance - Created 2009-10-28
28 Days Centred - Linear

Mortality
• Daily Extract of all registered deaths in Scotland supplied by GRO Scotland
• Age, • Gender, • Partial Postcode• Date of Death and,• Date of Registration

Models
i
ias
iasasias
dsd
log
)(~ ii Poissony
idsiw
Expected Count on Day iSpline trend for Day (time) knots every week
= 1 of Day i is a holiday,
=0 otherwise
Observed Count on Day i
im factor denoting separate working days Monday to Friday
Library mgcv in R
iasiasi
iasasi
mhdsd
log
Date of Death Date of Registration of Death
i – Indexes daysa – Age Groups - Gender

Date of Death (2008-10-01 to 2009-10-27)
Dea
ths
Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov
120
140
160
180
200
220
All DeathsSmoothed Previous Years + 99% Prediction Interval
DataFitted TrendPredicted Range
Under ReportingCorrection

Date of Registration of Death (2008-10-01 to 2009-10-27)
Dea
ths
Oct Nov Dec Jan Feb Mar Apr May Jun Jul Aug Sep Oct Nov
010
020
030
040
050
060
070
0
All DeathsSmoothed Previous Years + 99% Prediction Interval
DataFitted TrendPredicted Range


Scottish GP Surveillance System• Expansion of the GP Surveillance system
to cover daily consultations by 1031 GPs in Scotland– GPASS (67% of practices)– EMIS (8%)– INPS (Vision) (24%)– Ascribe (1%)– 58 practices in PTI network
• A similar system worked well last year for winter flu vaccine uptake
• Currently 89% of practices participating

Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
100
150
Ayrshire & Arran
Date
Rat
e pe
r 100
000
17/08 10/09 05/100
5010
015
0
Borders
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
100
150
Dumfries & Galloway
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
100
150
Fife
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
100
150
Forth Valley
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
100
150
Greater Glasgow & Clyde
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
100
150
Grampian
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
100
150
Highland
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
100
150
Lanarkshire
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
100
150
Lothian
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
100
150
Orkney
Date
Rat
e pe
r 100
000
20/08 14/09 08/10
050
100
150
Shetland
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
100
150
Tayside
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
100
150
Western Isles
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
150
250
Scotland
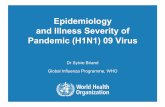
Raw unadjusted consultation rates

Issues
• 4 GP recording systems– Systematic differences between then
• 58 PTI practices – enhanced training for recording consultations
• Health Boards cannot be compared as each health board predominantly used one system– E.g.Greater Glasgow and Clyde GPASS

Model
ijk
kkkkkijijk
ijk HBPTISystemPTISystemP
:log
ijkijkijkijk yVarODPy ),(~
Expected Count in Practice k, for age group i and gender j
Observed Count on a Day
ijkP Population in Practice k, for age group i and gender j

Modelling
• Trying to get a reasonably robust model• which captures the essential features and• which can then be used to adjust the data
to provide an ‘all Scotland’ picture• within hours of receiving the completed
data

Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
150
250
Ayrshire & Arran
Date
Rat
e pe
r 100
000
17/08 10/09 05/100
5015
025
0
Borders
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
150
250
Dumfries & Galloway
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
150
250
Fife
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
150
250
Forth Valley
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
150
250
Greater Glasgow & Clyde
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
150
250
Grampian
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
150
250
Highland
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
150
250
Lanarkshire
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
150
250
Lothian
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
150
250
Orkney
Date
Rat
e pe
r 100
000
20/08 14/09 08/10
050
150
250
Shetland
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
150
250
Tayside
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
150
250
Western Isles
Date
Rat
e pe
r 100
000
17/08 10/09 05/10
050
100
150
Scotland
Adjusted consultation rates

Statistical Issues
• Relatively large amount of daily data• Summarised and modelled for reporting that day • Models need to take into account
– Known biases in data collection– Systematic trend– Reporting delays– Holidays
• Mostly automatic and it is difficult to foresee all the data checks that are required

Statistical Issues• Reporting is all based upon modelling using
historic data to predict expected patterns this year• Flexible models using splines for the trend plus
parameters for known systematic effects• Systems are brought in very quickly with limited
time for testing and investigation• Need to be very aware of data quality and the
mechanisms for data capture to interpret the data correctly
• Need to be open about the models and method of analysis used

Position in Scotland• Daily consultation rates (age/gender)• Daily NHS call data (age)• Daily Hospitalisations (Individual records)• Daily deaths (age/gender)• Daily antiviral prescriptions
– All electronic data capture and reporting• Weekly Laboratory testing of a planned 500
swabs from symptomatic patients per week (80 - 100 achieved over summer)
• Using excellent data capture systems to increase the size of the surveillance to provide local level information

Position in Scotland
• Great effort by a large number of people in government and health service organisations, laboratories and registrars offices to provide valuable data on a daily basis
• Individual and GP level data which is anonymised but can be linked.
• Will systems be robust in the event of a huge increase in the number of cases?