Guidelines update
52
HCV is just a matter of time Last guidelines updates July 2016 By Mohammed Aboelmagd (MD) Endemic & Infectious diseases Department
-
Upload
mohammed-abo-elmagd -
Category
Health & Medicine
-
view
116 -
download
0
Transcript of Guidelines update
HCV is just a matter of timeLast guidelines updates
July 2016
ByMohammed Aboelmagd (MD)Endemic & Infectious diseases Department

HCV Timeline
• 5000 years ago Jaundice at the dawn of medicine .
• For centuries, hepatitis was a mystery and understanding came in waves until its origin was finally unraveled.

At 4th millennium BC
• The word icterus was first found in the Hippocratic corpus as early as 460 BC.
• Hippocrates described the first clinical features of epidemic jaundice.
• A fulminant course in patients who died within 11 days. The recommended treatment was a diet of honey and water.

At 3th millennium BC
• early description of jaundice was found in Sumeria clay tablets(The first handbook of medicine )
Description of the etiology of jaundice was a devil name “Ahhazu” who attacked the liver which in those days was the home of the soul.
At 6th century
• As early as 752, Pope Zacharias wrote about “jaundice of a contagious nature” where those affected would have to be segregated.
• Pope Zackary clearly recommended isolation as the best approach in dealing with an epidemic of jaundice.
• Patients were considered ‘impure’ and were therefore to be ‘avoided’ and isolated.

FROM 17TH ~ 18TH CENTURY
Outbreaks of epidemic jaundice have been recorded in military
during the war timeNapoleon-time

THE 19TH CENTURY (1801-1900)BRITAIN AND THE INDUSTRIAL REVOLUTION
• Lurman (1883): reported outbreaks of serum hepatitis
following vaccinationTHE 1ST HALF OF THE 20TH CENTURY
(1901-1950)……WORLD WAR)
• McDonald (1908): postulated that the infectious jaundice is
caused by virus.

1947, Mac Callum suggested the first historical distinction between two forms of
hepatitis in : 1- epidemic hepatitis .2- serum hepatitis .
1988 ,Harvey & Alter discover non A non B virus

Identification of non-A non-B hepatitis
1973 HAV
1977 HDV
1983 HEV
1988 HCV
Life cycle fully understood in 2005


Road map

Specific Targets for HCV Treatment:Protease and Polymerase Inhibition
C E1 E2 p7 NS2 NS3 NS4A NS4B NS5A NS5B
PolymeraseProtease
Kwong A, et al. Beyond interferon and ribavirin: Antiviral therapies for hepatitis C virus. Drug Discovery Today: Therapeutic Strategies. 2006;3:211-220.
NS5A Inhibitors
M.Mekky March.2016

buvir Asvir Previrsofosbuvir Daclatasvir
Ombitasiverledipasvir
-Simprevir- Asunaprevir- Faldaprevir


AASLD-IDSA JULY 2016
Recommendations for Testing,Managing, and Treating Hepatitis C

Rating System Used to Rate the Level of the Evidence and Strength of the
Recommendation for Each Recommendation

Summary of Recommendations for HCV Testing and Linkage to Care

Recommendations for HCV Testing and Linkage to Care
3. Other considerations• HIV infection• Sexually active persons about to start pre-exposure prophylaxis
(PreP) for HIV• Unexplained chronic liver disease and/or chronic hepatitis including
elevated alanine aminotransferase levels• Solid organ donors (deceased and living)Rating: Class I, Level B
*Regardless of country of birth

Recommendation for HCV Testing Those with Ongoing Risk Factors
• Annual HCV testing is recommended for persons who inject drugs and for HIV-seropositive men who have unprotected sex with men. Periodic testing should be offered to other persons with ongoing risk factors for exposure to HCV.
Rating: Class IIA, Level C

Recommendations for Follow-up of Initial Testing

Recommendations for Counseling Those with Current (Active) HCV Infection
1. Abstinence from alcohol and, when appropriate, interventions to facilitate cessation of alcohol consumption should be advised for all persons with HCV infection.Rating: Class IIa, Level B2. Evaluation for other conditions that may accelerate liver fibrosis, including HBV and HIV infections, is recommended for all persons with HCV infection. Rating: Class IIb, Level B3. Evaluation for advanced fibrosis using liver biopsy, imaging, and/or noninvasive markers is recommended for all persons with HCV infection, to facilitate an appropriate decision regarding HCV treatment strategy and to determine the need for initiating additional measures for the management of cirrhosis (eg, hepatocellular carcinoma screening). Rating: Class I, Level A
Recommendations for Counseling Those with Current (Active) HCV Infection
4. Vaccination against hepatitis A and hepatitis B is recommended for all susceptible persons with HCVinfection. Rating: Class IIa, Level C5. Vaccination against pneumococcal infection is recommended to all patients with cirrhosis. : Class IIa, Level C6. All persons with HCV infection should be provided education on how to avoid HCV transmission toothers. Rating: Class I, Level C
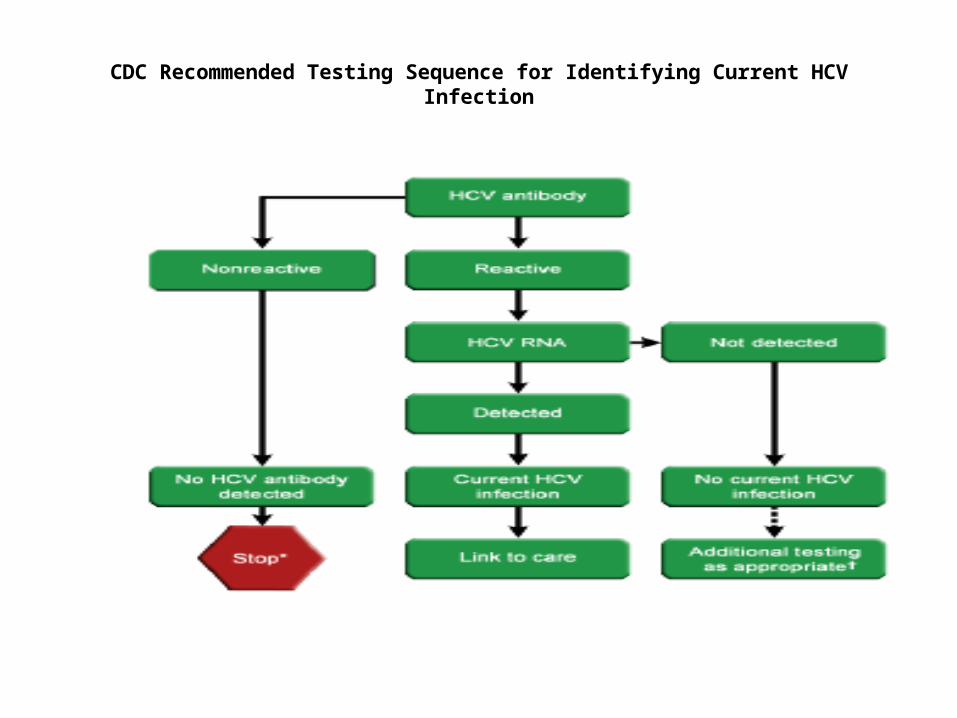
CDC Recommended Testing Sequence for Identifying Current HCV Infection

Summary of Recommendations for When and in Whom to Initiate HCV Therapy

Recommendations for When and in Whom to Initiate Treatment
• Treatment is recommended for all patients with chronic HCV infection, except those with short life expectancies that cannot be remediated by treating HCV, by transplantation, or by other directed therapy.
• Patients with short life expectancies owing to liver disease should be managed in consultation with an expert.
Rating: Class I, Level A

Recommendations for Pretreatment Assessment
• Evaluation for advanced fibrosis using liver biopsy, imaging, and/or noninvasive markers is recommended for all persons with HCV infection, to facilitate an appropriate decision regarding HCV treatment strategy and to determine the need for initiating additional measures for the management of cirrhosis (eg , hepatocellular carcinoma screening).
Rating: Class I, Level A

INITIAL TREATMENT OF HCV INFECTION
• A. Genotype 1a




B. Genotype 1b


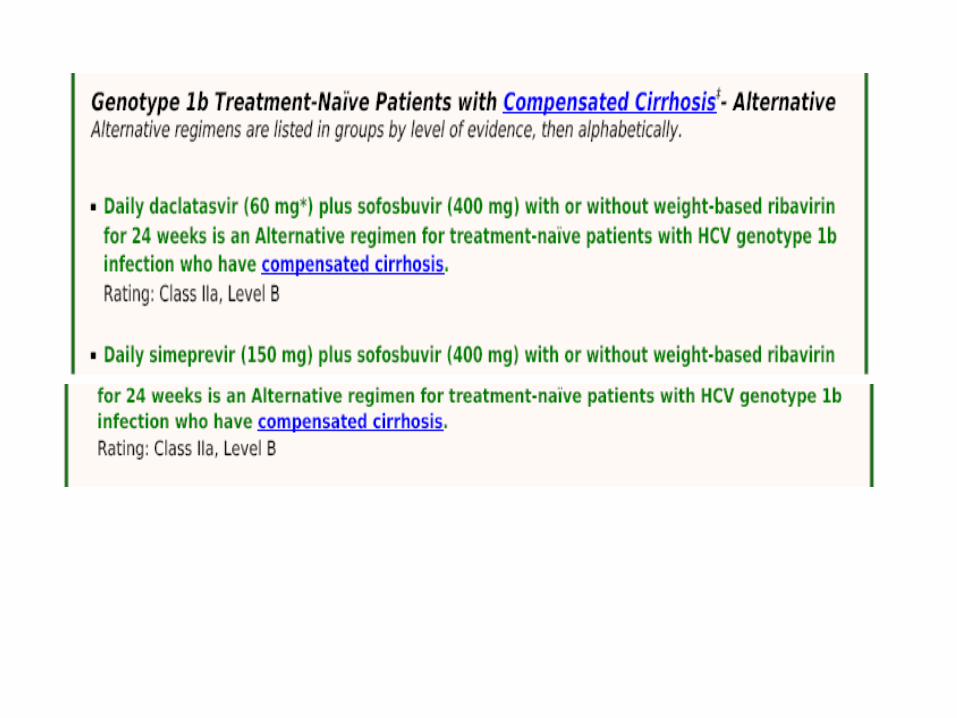

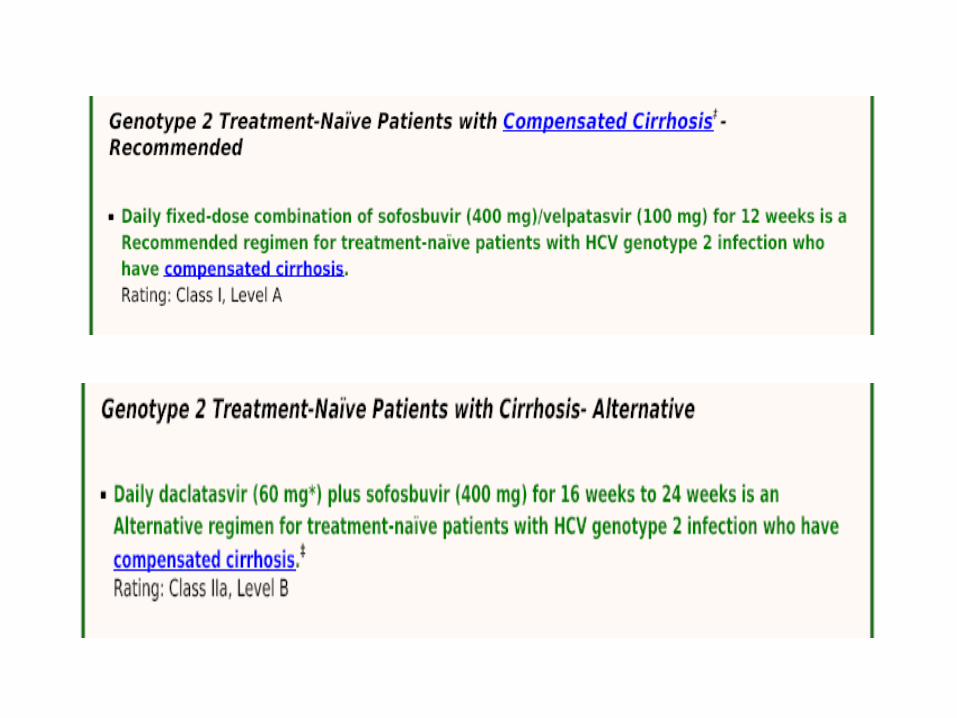
II. Genotype 2

III. Genotype 3


IV. Genotype 4


V. Genotype 5 or 6
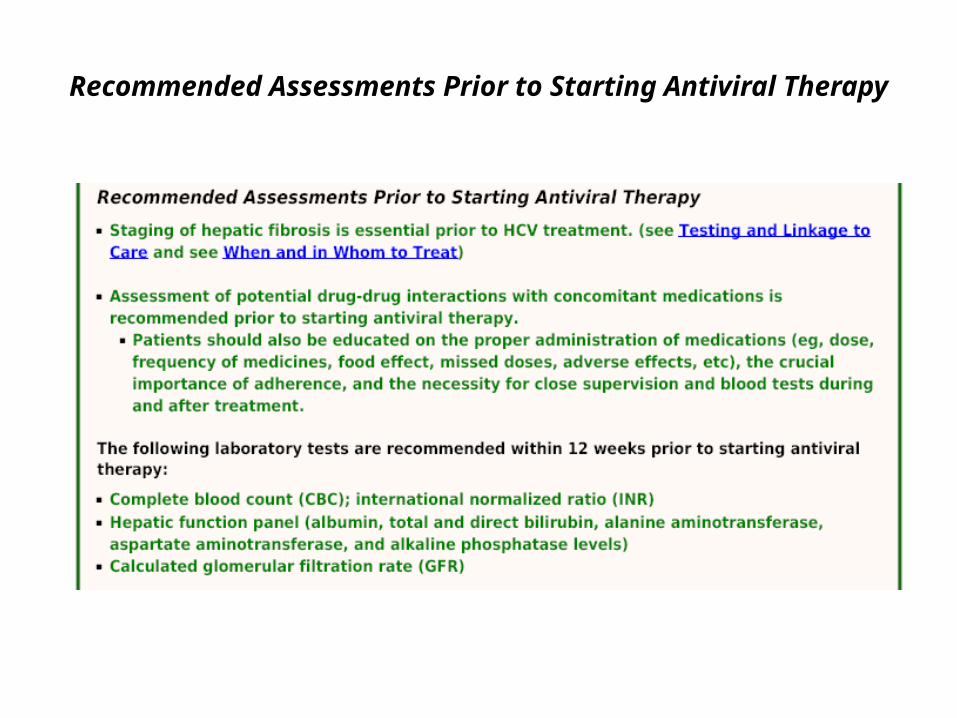
Recommended Assessments Prior to Starting Antiviral Therapy