Guidelines on Prescribing Specialist Infant Formulas in ... · AAf top ups can be maintained if no...
25
Oxfordshire Clinical Commissioning Group Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019. Guidelines on Prescribing Specialist Infant Formulas in primary care Contents 1. Introduction 2. Prescribing Guidance 2.1 Quantities to Prescribe 2.2 Prescription Management 3. Cow’s Milk Protein Allergy (CMPA) 3.1 Background Information 3.2 Diagnosis and Initial Management of CMPA 3.2.1 IgE mediated CMPA 3.2.2 Non-IgE mediated CMPA and Home Reintroduction 3.3 Ongoing Management of Confirmed Mild to Moderate CMPA 3.4 Product choices 3.4.1 Extensively Hydrolysed Formula (EHf) 3.4.2 Amino Acid Formula (AAf) 3.4.3 Products Not Suitable for Prescribing in CMPA 3.5 Prescription Management 3.6 Reintroducing Cow’s Milk 3.7 Weaning 4. Gastro-oesophageal Reflux Disease (GORD) 5. Secondary Lactose Intolerance 6. Faltering Growth 7. Preterm Infants 8. Metabolic Products 9. References and Acknowledgements 10. Appendices 10.1 Appendix 1 – Suspected Cow’s Milk Allergy (CMA) in the 1 st Year of Life (iMAP) 10.2 Appendix 2 – Primary Care Management of Mild to Moderate Non-IgE CMA (iMAP) 10.3 Appendix 3 – Parent leaflet: The iMAP Milk Allergy Guideline– Initial Fact Sheet 10.4 Appendix 4 – Parent leaflet: The Early Home Reintroduction to confirm the diagnosis of cow’s milk allergy 10.5 Appendix 5 – The iMAP Milk Ladder 10.6 Appendix 6 - Infant Formula products – quick reference guide 10.7 Appendix 7 – Summary of Guidelines on prescribing specialist infant formula in primary care
Transcript of Guidelines on Prescribing Specialist Infant Formulas in ... · AAf top ups can be maintained if no...
Oxfordshire Clinical Commissioning Group
Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
Guidelines on Prescribing Specialist
Infant Formulas in primary care
Contents
1. Introduction
2. Prescribing Guidance 2.1 Quantities to Prescribe 2.2 Prescription Management
3. Cow’s Milk Protein Allergy (CMPA)
3.1 Background Information 3.2 Diagnosis and Initial Management of CMPA
3.2.1 IgE mediated CMPA
3.2.2 Non-IgE mediated CMPA and Home Reintroduction
3.3 Ongoing Management of Confirmed Mild to Moderate CMPA 3.4 Product choices
3.4.1 Extensively Hydrolysed Formula (EHf) 3.4.2 Amino Acid Formula (AAf) 3.4.3 Products Not Suitable for Prescribing in CMPA
3.5 Prescription Management 3.6 Reintroducing Cow’s Milk 3.7 Weaning
4. Gastro-oesophageal Reflux Disease (GORD)
5. Secondary Lactose Intolerance
6. Faltering Growth
7. Preterm Infants
8. Metabolic Products
9. References and Acknowledgements
10. Appendices
10.1 Appendix 1 – Suspected Cow’s Milk Allergy (CMA) in the 1st Year of Life (iMAP) 10.2 Appendix 2 – Primary Care Management of Mild to Moderate Non-IgE CMA (iMAP) 10.3 Appendix 3 – Parent leaflet: The iMAP Milk Allergy Guideline– Initial Fact Sheet 10.4 Appendix 4 – Parent leaflet: The Early Home Reintroduction to confirm the diagnosis of cow’s milk
allergy 10.5 Appendix 5 – The iMAP Milk Ladder 10.6 Appendix 6 - Infant Formula products – quick reference guide 10.7 Appendix 7 – Summary of Guidelines on prescribing specialist infant formula in primary care

2 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
1. Introduction
These guidelines outline recommendations for the safe, appropriate and cost-effective prescribing of specialist infant formula for children up to the age of 18 months in the Oxfordshire area. It covers:
Over-the-counter (OTC) products available wherever appropriate
Quantities to prescribe
Which products to use for different clinical conditions
Initiating, reviewing and discontinuing prescriptions
When to refer to dietitians and/ or secondary or specialist care
For allergy related queries please contact consultant-led paediatric allergy advice service via [email protected].
Breast milk remains the optimal nutrition for infants and should be promoted, supported and encouraged where it is clinically safe.
2. Prescribing Guidance
2.1 Quantity of Powdered Formula to Prescribe
When prescribing powdered infant formulas please refer to the table below for suggested quantity to
prescribe per month:
Age of child Suggested quantity of powdered formula to prescribe per month
400g tin 900g tin
< 6 months Highest requirement at 4-6 months prior to weaning
Up to 12 tins Up to 5 tins
6 – 12 months 6 – 12 tins 3 – 5 tins
> 12 months Up to 6 tins Up to 3 tins
2.2 Prescription Management
1. Only prescribe 1-2 tins initially as “acute” prescription to assess tolerance and to avoid waste.
Review recent correspondence from the paediatrician or paediatric dietitian.
2. Add formula to repeat prescribing template only if tolerance and diagnosis are confirmed, and a
regular, robust review process is established to ensure that the formula and quantity prescribed are
appropriate for the child’s age and nutritional requirements.
3. Prescribing specialist formula for children over 18 months will be low priority unless specifically
requested from a specialist (paediatrician or dietitian) and reason for continued use is provided, in
line with Clinical Commissioning Policy 250.
4. DO NOT prescribe the following on NHS prescriptions. Parents should be advised to purchase these
as their costs are similar to that of cow’s milk formula, in line with Clinical Commissioning Policy 88
and 250:
Soya formula - Wysoy®

3 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
Lactose free formula - Aptamil® LF, SMA® LF, Enfamil® O-Lac
Pre-thickened formula - Cow and Gate® Anti-reflux, Aptamil® Anti-reflux, SMA® PRO Anti-
reflux
Thickening formula - SMA® Staydown (replaced by SMA® PRO Anti-reflux), Enfamil® AR
5. DO NOT prescribe ready-to-feed liquids as they have no clinical advantage and are usually
substantially more expensive. These should only be prescribed on specialist’s request when there is
a clinical need e.g. if the patient is tube or PEG (percutaneous endoscopic gastrostomy) fed.
6. Prescriptions must be endorsed ‘ACBS’.
3. Cow’s Milk Protein Allergy (CMPA)
3.1 Background Information
CMPA is the commonest food allergy in the first year of life with a prevalence of 2-3 %. Most infants
with CMPA develop symptoms within one week of introduction of a cow’s milk protein (CMP) - based
formula and improve within 1-2 weeks of a CMP elimination diet. However, this can take up to 6 weeks.
Most children with a diagnosis of CMPA have mild to moderate symptoms which can be managed in
primary care. Severe CMPA should be managed in conjunction with a paediatrician with an interest in
allergy. For detailed assessment of severity of CMPA refer to iMAP CMPA algorithm for symptoms
presentation (see appendix 1) and algorithm for diagnosis and management (see appendix 2).
3.2 Diagnosis and Initial Management of CMPA
There are two main types of cow’s milk allergy: acute Immunoglobulin E (IgE) mediated reactions
(symptom onset within minutes up to 2 hours) and the delayed non-IgE mediated reactions (2-72hrs
onset). The table below depicts recognised clinical features of CMPA. For detailed guidance on
obtaining an allergy focused history, see NICE CG116: Food Allergy in Children and iMAP allergy
focused clinical history for suspected CMPA in infancy.
Download the iMAP Milk Allergy Guideline– Initial Fact Sheet (see Appendix 3) for parents whose
infants are showing mild to moderate symptoms of delayed non Ig-E mediated reaction to CMP.
Acute IgE-mediated Delayed non-IgE-mediated
The skin
Pruritus Pruritus
Erythema Erythema
Acute urticaria – localised or generalised Atopic dermatitis Acute angioedema of lips, face and around the eyes
The gastrointestinal
system
Oral pruritus Gastro-oesophageal reflux
disease Colicky abdominal pain Loose or frequent stools
Vomiting Blood and/or mucus in stools
Diarrhoea Abdominal pain
Infantile colic Food refusal or aversion
Constipation Perianal redness

4 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
The respiratory
system (usually in
combination with
one or more of skin
and GI symptoms)
Upper respiratory tract symptoms (nasal itching, sneezing, rhinorrhoea or congestion
(with or without conjunctivitis), signs or symptoms of anaphylaxis e.g. laryngeal
oedema with drooling and hoarse voice and tongue swelling.
Lower respiratory tract symptoms (cough, chest tightness, wheezing or shortness of
breath)
Note: this list is not exhaustive. The absence of these symptoms does not exclude food allergy.
3.2.1 IgE mediated CMPA (symptom onset within minutes up to 2 hours)
AAf = amino acid formula; EHf = extensively hydrolysed formula
Yes
Severe
Immediate reactions with severe respiratory +/- CVS
(cardiovascular system) signs and symptoms.
Anaphylaxis -> A&E. Allergy referral and commence on
AAf and dairy free weaning with dietetic support.
Mild to moderate
More than one of the following symptoms: acute pruritus,
erythema, urticaria, angioedema, acute flaring of atopic
dermatitis, vomiting, diarrhoea, acute rhinitis
Acute Onset symptoms: IgE mediated
Any immediate symptoms on EHf feeds?
Recurrence of
immediate symptoms
despite maternal dairy
free diet*?
Refer to specialist for allergy
testing to confirm CMPA and
plan for reintroduction, AAf
may be needed. Do not
perform Home
Reintroduction. Refer to
dietitians for weaning support.
Continue EHf.
Refer for allergy
testing and
Reintroduction
plan. Refer to
dietitian for
weaning support.
**Note: if no delayed symptoms prior to a mild/moderate acute reaction there is no need for maternal dairy exclusion. Rarely
there may be minor immediate symptoms such as redness, hives after breast feeds. Maternal dairy free diet will be required in
these cases.
Mixed/ formula feeding: Urgent referral
to paediatric allergy service.
Formula feeding: Specialist to recommend/
commence AAf exclusively;
Mixed feeding: AAf as top-ups if required.
Maternal dairy free diet* if persistent GI
symptoms and atopic dermatitis. Specialist
follow up and Reintroduction plan.
Exclusively formula feeding: Trial EHf;
Mixed feeding**: EHf top-ups if needed
+ maternal dairy free diet* if persistent GI
symptoms or active atopic dermatitis with
breast feeding** (see notes below).
Refer for allergy testing
to confirm CMPA. Do
not Perform Home
Reintroduction. Refer
to dietitians for weaning
support.
Continue maternal dairy free diet*.
Refer for allergy testing and
Reintroduction plan. If top-up
formula required refer to paediatric
allergy service for AAf. Refer to
dietitians for weaning support.
* Breastfeeding mothers on a milk free diet may require supplementation with 1000mg calcium and 10mcg Vitamin D per day.
No
No
Exclusively breastfed:
Maternal dairy free diet*
for 2 - 4 weeks.
Yes
5 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
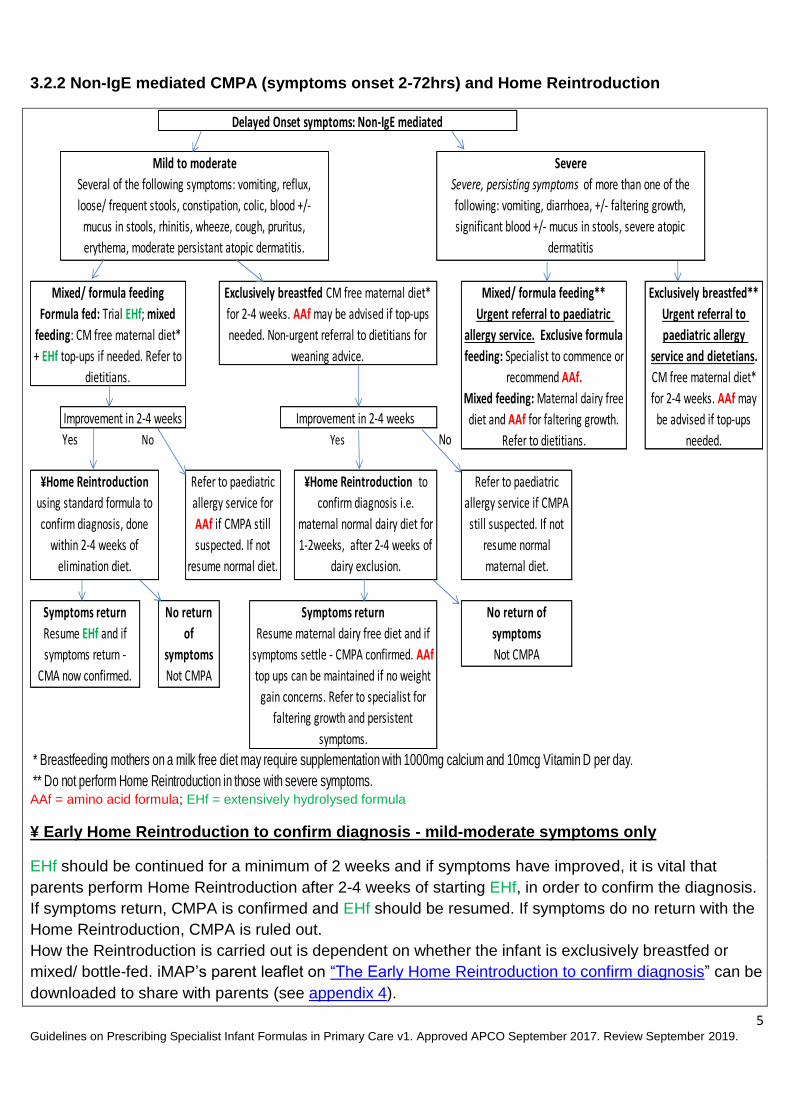
3.2.2 Non-IgE mediated CMPA (symptoms onset 2-72hrs) and Home Reintroduction
AAf = amino acid formula; EHf = extensively hydrolysed formula
¥ Early Home Reintroduction to confirm diagnosis - mild-moderate symptoms only
EHf should be continued for a minimum of 2 weeks and if symptoms have improved, it is vital that
parents perform Home Reintroduction after 2-4 weeks of starting EHf, in order to confirm the diagnosis.
If symptoms return, CMPA is confirmed and EHf should be resumed. If symptoms do no return with the
Home Reintroduction, CMPA is ruled out.
How the Reintroduction is carried out is dependent on whether the infant is exclusively breastfed or
mixed/ bottle-fed. iMAP’s parent leaflet on “The Early Home Reintroduction to confirm diagnosis” can be
downloaded to share with parents (see appendix 4).
Improvement in 2-4 weeks
Yes No Yes No
* Breastfeeding mothers on a milk free diet may require supplementation with 1000mg calcium and 10mcg Vitamin D per day.
** Do not perform Home Reintroduction in those with severe symptoms.
Symptoms return
Resume maternal dairy free diet and if
symptoms settle - CMPA confirmed. AAf
top ups can be maintained if no weight
gain concerns. Refer to specialist for
faltering growth and persistent
symptoms.
Mixed/ formula feeding**
Urgent referral to paediatric
allergy service. Exclusive formula
feeding: Specialist to commence or
recommend AAf.
Mixed feeding: Maternal dairy free
diet and AAf for faltering growth.
Refer to dietitians.
Improvement in 2-4 weeks
Symptoms return
Resume EHf and if
symptoms return -
CMA now confirmed.
No return of
symptoms
Not CMPA
¥Home Reintroduction
using standard formula to
confirm diagnosis, done
within 2-4 weeks of
elimination diet.
No return
of
symptoms
Not CMPA
Exclusively breastfed**
Urgent referral to
paediatric allergy
service and dietetians.
CM free maternal diet*
for 2-4 weeks. AAf may
be advised if top-ups
needed.
Mixed/ formula feeding
Formula fed: Trial EHf; mixed
feeding: CM free maternal diet*
+ EHf top-ups if needed. Refer to
dietitians.
Refer to paediatric
allergy service if CMPA
still suspected. If not
resume normal
maternal diet.
Refer to paediatric
allergy service for
AAf if CMPA still
suspected. If not
resume normal diet.
Delayed Onset symptoms: Non-IgE mediated
Severe
Severe, persisting symptoms of more than one of the
following: vomiting, diarrhoea, +/- faltering growth,
significant blood +/- mucus in stools, severe atopic
dermatitis
¥Home Reintroduction to
confirm diagnosis i.e.
maternal normal dairy diet for
1-2weeks, after 2-4 weeks of
dairy exclusion.
Exclusively breastfed CM free maternal diet*
for 2-4 weeks. AAf may be advised if top-ups
needed. Non-urgent referral to dietitians for
weaning advice.
Mild to moderate
Several of the following symptoms: vomiting, reflux,
loose/ frequent stools, constipation, colic, blood +/-
mucus in stools, rhinitis, wheeze, cough, pruritus,
erythema, moderate persistant atopic dermatitis.
6 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
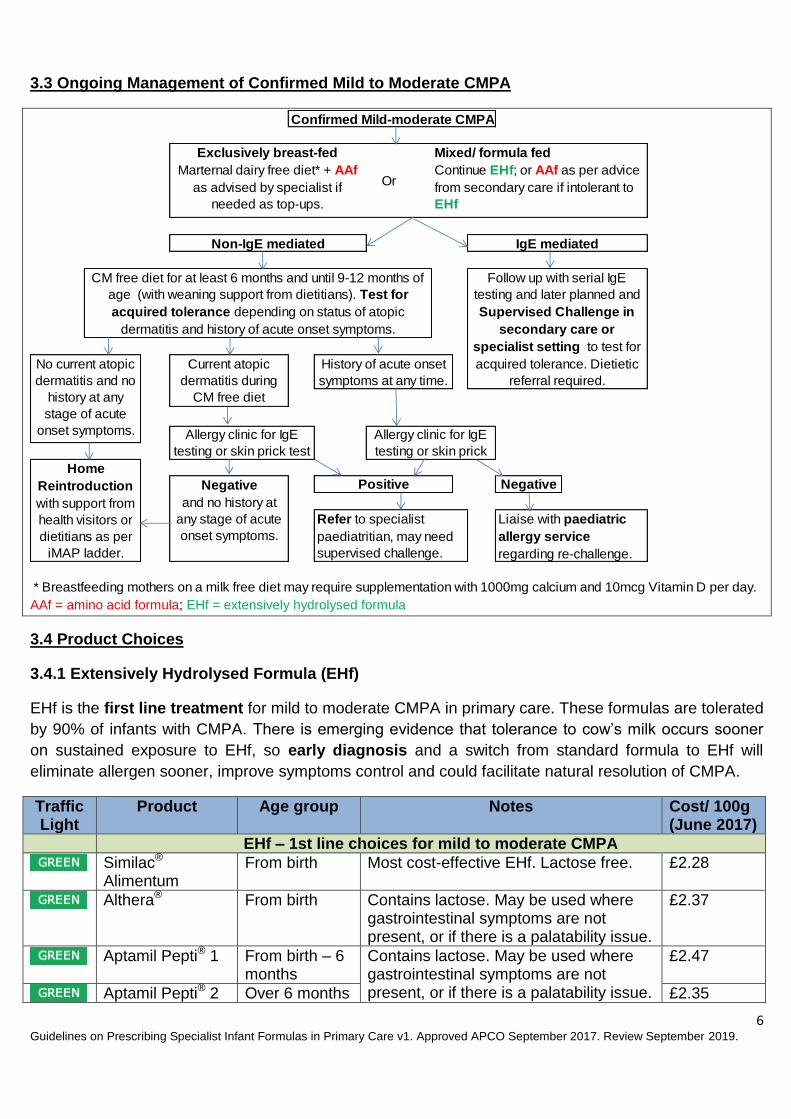
3.3 Ongoing Management of Confirmed Mild to Moderate CMPA
AAf = amino acid formula; EHf = extensively hydrolysed formula
3.4 Product Choices
3.4.1 Extensively Hydrolysed Formula (EHf)
EHf is the first line treatment for mild to moderate CMPA in primary care. These formulas are tolerated
by 90% of infants with CMPA. There is emerging evidence that tolerance to cow’s milk occurs sooner
on sustained exposure to EHf, so early diagnosis and a switch from standard formula to EHf will
eliminate allergen sooner, improve symptoms control and could facilitate natural resolution of CMPA.
Traffic Light
Product Age group Notes Cost/ 100g (June 2017)
EHf – 1st line choices for mild to moderate CMPA
Similac® Alimentum
From birth Most cost-effective EHf. Lactose free. £2.28
Althera® From birth Contains lactose. May be used where gastrointestinal symptoms are not present, or if there is a palatability issue.
£2.37
Aptamil Pepti® 1 From birth – 6 months
Contains lactose. May be used where gastrointestinal symptoms are not present, or if there is a palatability issue.
£2.47
Aptamil Pepti® 2 Over 6 months £2.35
Confirmed Mild-moderate CMPA
Negative
* Breastfeeding mothers on a milk free diet may require supplementation with 1000mg calcium and 10mcg Vitamin D per day.
Allergy clinic for IgE
testing or skin prick test
Allergy clinic for IgE
testing or skin prick
Current atopic
dermatitis during
CM free diet
No current atopic
dermatitis and no
history at any
stage of acute
onset symptoms.
Home
Reintroduction
with support from
health visitors or
dietitians as per
iMAP ladder.
Negative
and no history at
any stage of acute
onset symptoms.
Mixed/ formula fed
Continue EHf; or AAf as per advice
from secondary care if intolerant to
EHf
Or
Exclusively breast-fed
Marternal dairy free diet* + AAf
as advised by specialist if
needed as top-ups.
Liaise with paediatric
allergy service
regarding re-challenge.
History of acute onset
symptoms at any time.
Positive
IgE mediated Non-IgE mediated
Refer to specialist
paediatritian, may need
supervised challenge.
CM free diet for at least 6 months and until 9-12 months of
age (with weaning support from dietitians). Test for
acquired tolerance depending on status of atopic
dermatitis and history of acute onset symptoms.
Follow up with serial IgE
testing and later planned and
Supervised Challenge in
secondary care or
specialist setting to test for
acquired tolerance. Dietietic
referral required.

7 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
Traffic Light
Product Age group Notes Cost/ 100g (June 2017)
Nutramigen 1 with LGG®
From birth – 6 months
Lactose free. Contains a unique probiotic Lactobacillus rhamnosus GG (LGG®).
£2.75
Nutramigen 2 with LGG®
Over 6 months £2.75
EHf with MCT (medium chain triglycerides)– Initiated by secondary Care only
Pregestimil Lipil® From birth Suitable only when CMPA is also accompanied by fat malabsorption.
£3.05
Pepti Junior® From birth £2.90
NB: Infatrini® Peptisorb is a high calorie EHf for mild to moderate CMPA with poor intake and poor
weight gain but no significant growth faltering. See also section 6.
3.4.2 Amino Acid Formula (AAf)
In AAf, the milk protein is broken down into individual amino acids. AAf is suitable only if at least one of the following criteria is met:
Persistent symptoms after 4 weeks on EHf;
Severe CMPA such as faltering growth and severe GI symptoms;
A history of anaphylactic reaction to cow’s milk formula;
Persistent symptoms in breast fed infants unresponsive to maternal dairy free diet for 4 weeks, or mother does not wish to continue breastfeeding.
AAf should only be prescribed on advice or recommendation of a Paediatric Consultant. GPs can
contact the consultant-led paediatric allergy advice service via [email protected] for
specialist advice on appropriateness of AAf before starting it in new patients.
Traffic Light
Product Age group Notes Cost/ 100g (June 2017)
AAf – Secondary Care Recommendation/ Initiation only
Alfamino® From birth up to 18 months old, or when able to tolerate OTC products
Most cost-effective AAf. Has higher vitamin A content.
£5.75
Nutramigen® PurAmino
Gluten and lactose free. Previously known as Nutramigen® AA.
£6.77
Neocate LCP®
From birth - 1 year Can be used as a sole source of nutrition up to the age of 1 year.
£7.18
Other AAf
Neocate® Junior
From 1 year – 10 years
Neocate® Junior will replace Neocate® Active and Neocate® Advance over a period of 12 months, from April 2017 to April 2018. These are high calorie formulas and will not be required automatically by all infants over 1 year. Suitable as a sole source of nutrition or as a supplement.
£ 7.18 (unflavoured/ vanilla/ strawberry)

8 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
3.4.3 Products Not Suitable for Prescribing in CMPA
1. Soya products: Wysoy®
Soya products should NOT be routinely prescribed for infants with CMPA, in particularly those under 6 months due to high phytoestrogen content. It may be used in infants over 6 months who do not tolerate first line EHf due to issues with palatability. There is a risk of co-sensitisation to soya in infants with predominantly GI symptoms of CMPA. It is more likely that children will tolerate soya formula from 1 year, and parents should be advised to purchase soya formula or Alpro Soya Growing Up Drink (1+ Years) from 1 year of age as these are similar costs to cow’s milk formula, in line with Clinical Commissioning Policy 88 and 250.
2. Lactose free formula: Aptamil® LF, SMA® LF and Enfamil® O-Lac.
Lactose intolerance is not the same as CMPA and these formulas are cow’s milk based. EHf or AAf
should not be prescribed for transient lactose intolerance.
3. Rice milk: Unsuitable under age of 5yrs due to arsenic content.
4. Other mammalians milk e.g. Goat’ milk, Sheep milk products have similar protein composition to
cow’s milk so are not suitable for treating CMPA.
3.5 Prescription Management
1. Try a formula for a minimum of two weeks and maintain for at least four weeks before further
changes.
2. Specialist formulas may be prescribed for infants with CMPA usually for no longer than 6 – 12
months. All children on EHf should be reviewed by GPs at 12 months and then 18 months as
appropriate. For those who are on AAf, GPs should review latest correspondence from the specialist or
dietitian as there may be changes in formula or quantity.
3. Parents of all children with non-IgE CMPA should be advised on graded dairy introduction using the iMAP milk ladder (see appendix 5) after 6 months of exclusion. This is a test for acquired tolerance and helps resolution if certain dairy products are well tolerated. The iMAP milk ladder (see appendix 5) should be shared with parents as it contains useful practical pointers to support parents at home. iMAP milk ladder recipes can be downloaded here. 4. Review prescriptions regularly and refer to latest correspondence from specialist for any change in
formula or quantity. Review and consider stopping prescription if the patient meets one or more of the
following criteria:
On the formula for more than a year
The quantity of formula prescribed is higher than recommended above (see section 2.1)
Patient can eat cow’s milk containing foods such as cow’s milk, cheese, yogurt, ice-cream,
custard, cakes, chocolate, cream, ghee and etc.
Over 18 months old. Please note children with multiple or severe allergies may require
prescriptions beyond 18 months old. This should always be on the recommendation of the
paediatric dietitian or consultant.

9 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
Please send a new referral or liaise with appropriate services if the child is already under the care of a
paediatric dietitian or paediatric allergist.
3.6 Reintroducing Cow’s Milk Products
1. Note that this is different from the Early Home Reintroduction usually performed 2 – 4 weeks after
introducing EHf, which is aimed at confirming CMPA diagnosis (see section 3.2.2).
2. Children on long-term EHf or AAf should be reintroduced to dairy on a graded approach, to establish
if they have acquired tolerance to CMP. About 60 – 75% of children outgrow CMPA by 2 years of age,
rising to 85-90% at 3 years of age.
3. For exclusively breastfed infants who have been symptom-free for at least 6 months:
- Re-introduce dairy products to maternal diet from 9-12 months and if tolerated, use the iMAP
milk ladder (see appendix 5) for graded dairy re-introduction. iMAP milk ladder recipes can be
downloaded here.
4. For formula only and mixed formula/ breast-fed children who have been symptom-free for at least
6 months:
- Re-introduce cow’s milk products using the the iMAP milk ladder (see appendix 5) around 9-12
months old and every 2 months thereafter until tolerated. iMAP milk ladder recipes can be
downloaded here.
5. All children with IgE CMPA should have a plan of dairy reintroduction from Paediatric allergist when
safe. No Home Reintroductions should be performed in these patients.
3.7 Weaning
When an infant with CMPA reaches 6 months and starts to be weaned, it is important that an adequate
calcium intake is achieved, particularly whilst remaining on a CM-free weaning diet. Refer to community
or paediatric dietitian for support at this stage.

10 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
4. Gastro-oesophageal Reflux Disease (GORD)
GORD is the passage of gastric contents into the oesophagus causing troublesome symptoms and/ or complications. About 50% of infants have some degree of reflux at some time. In most infants it is physiological and with minimal effect so most parents can be reassured. Regurgitation of feeds is worse with higher volumes of feed but improves with thickened feeds.
Traffic Light
Product Age group
Notes Cost/ 100g (June 2017)
Cow & Gate® Anti-reflux
From birth
Readily available to purchase OTC in most pharmacies and major supermarkets. *N/B: SMA® Staydown will be available for a further few months (replaced by SMA® PRO Anti-reflux).
£1.28 (R*)
Aptamil® Anti-reflux £1.44 (R)
SMA® Staydown* £1.22 (R)
SMA® PRO Anti-reflux
£1.25 (R)
Enfamil® AR This may need to be ordered in specially at the pharmacy
£1.73 (R)
R* = Retail price
Refer to specialist paediatric
No
Bottlefed
Breastfed
No improvement
Review
Trial with Infant Gaviscon® offered on a spoon for 1-
2 weeks, up to max 6 times a day
Refer to specialist
paediatrician care
Cow and Gate® Anti-reflux,
Aptamil® Anti-reflux,
SMA Staydown®,
SMA® PRO Anti-reflux,
Enfamil AR®.
If symptoms persist, STOP the thickening
formula and trial Infant Gaviscon® for 1 -2
weeks. DO NOT prescribe separate
thickeners, antacids, PPIs or ranitidine
with thickening formula.
Trial using Carobel® to thicken standard
formula or one of the following for 1 - 2
weeks. These are available OTC and
should be purchased by parents:
Continue with treatment and review regularly to check growth
and symptoms. Trial stopping treatment at intervals and by 12
months as 90% of children usually outgrow GORD by then.
Once vomiting resolves return to standard formula.
Symptoms: effortless vomiting after feeding (not projectile) usually in the first 6 months e.g. regurgitation
of a significant volume of feed, reluctance to feed, distress/ crying at feed times, small volumes of feed
being taken
Rule out over feeding: check volume and frequency
of feeds - average requirement in babies <6 months is
150ml/kg/day and should be spread over 6-7 feeds.
Advise on feeding position and activity following a feed.
Does the infant have faltering growth?
The infant is thriving
and NOT distressed
The infant is thriving BUT distressedReassure and monitor, symptoms are likely
to improve over time, usually by 12 months.
Provide advice on avoidance of
overfeeding, positioning during and after
feeding, and activity after feeding.
If infant is clearly overfed, advise
restriction of volumes of feed
Yes
Yes
Improvement

11 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
5. Secondary Lactose Intolerance
Primary lactose intolerance is rare and is caused by an inherited deficiency of lactase which breaks
down lactose. Primary lactase deficiency usually develops after the age of two years, when
breastfeeding or bottle-feeding has stopped. The symptoms may not be noticeable until adulthood.
Secondary lactose intolerance is due to impaired lactase activity in the intestinal brush border and it is
neither immune mediated nor a feature of atopy. Secondary lactose intolerance in children occurs post
gastroenteritis and rarely following other gut insults such as prolonged courses of antibiotics. Symptoms
are usually self-limiting.
Parents of breastfed babies with lactose intolerance should be advised to purchase lactase enzyme
drops (e.g. Colief®). This should not be prescribed on the NHS. Exclusion of lactose from the maternal
diet is unnecessary as lactose is present in breast milk independent of diet. More severe or persistent
symptoms suggestive of lactose intolerance will need paediatric assessment if lactase is ineffective.
Alternative diagnosis such as CMPA will need to be considered for persistent gastrointestinal
symptoms.
Parents qualifying for Healthy Start vouchers can use these to purchase lactose free formula where the
packaging states that the milk is based on cow’s milk and can be used from birth, e.g. SMA® LF and
Enfamil® O-Lac.
Traffic Light
Product Age group Notes Cost/ 100g (June 2017)
Enfamil® O-Lac
From birth to 1 year
Lactose, sucrose and fructose free cow’s milk formula. May need to be ordered in specially at the pharmacy.
£2.30 (R*)
SMA® LF From birth up to 1 year
Not suitable for those who are allergic to cows' milk protein. Available to purchase OTC in pharmacies and major supermarkets.
£1.40 (R)
Aptamil® LF From birth to 1 year
£1.50 (R)
Lactofree® From 1 year £0.14/ 100ml (R)
R* = Retail price
Symptoms: abdominal bloating, increased (explosive) wind, loose green stools for > 2 weeks.
Diagnosis is confirmed if symptoms resolved within 48 hours of withdrawing lactose from diet.
Trial OTC lactose-free formula for 2 weeks. These can be bought at a similar cost to standard
formula: <12 months: Aptamil LF®, SMA LF®, Enfamil O-Lac® (may need to pre-order from
pharmacies) >12 months: LF full fat milk (e.g. Lactofree® brand) can be bought in supermarkets
Not lactose Intolerance
Consider alternative
diagnosis e.g. CMPA.
Refer to specialist care.
Note: Rarely symptoms may
last up to 3 months
Continue LF formula for up to 8 weeks gradually then re-
introduce standard formula/milk into diet. If symptoms return
restart LF formula until normal dairy tolerated.
There is a need to await natural resolution. Referral needed
if symptoms do not improve on LF formula.
Lactose Intolerance confirmed
Symptoms improved Symptoms not improved

12 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
6. Faltering Growth
Faltering growth is when an infant falls below the 0.4th centile or crosses 2 centiles downwards from
initial centile on a growth chart. Refer to paediatric services without delay. Specialist formula for
children with faltering growth should only be prescribed in primary care following assessment and
recommendations from a Consultant Paediatrician or Paediatric Dietitian.
GPs can access specialist advice via [email protected].
Traffic Light
Product Age group Notes Cost/ 100ml (June 2017)
SMA® PRO High Energy
From birth up to 18 months or 8kg.
Refer to paediatric services without delay. All infants will need growth monitoring to ensure catch up growth is achieved. Discontinue when on an appropriate diet as per dietitian advice.
£0.99
Similac® High Energy
£1.07
Infatrini® £1.16
Infatrini® Peptisorb
From birth up to 18 months or 9kg. Suitable for infants with faltering growth and intolerance to whole protein feeds, e.g. short bowel syndrome, intractable malabsorption, inflammatory bowel disease, bowel fistulae
£1.77
7. Preterm Infants
Pre-term infants will have been commenced on a pre-term formula (eg Nutriprem®) in hospital prior to
discharge. Pre-term formula should not be commenced in primary care unless recommended by a
specialist. The GP can continue prescribing the pre-term formula, until the baby is 6 months corrected
age i.e. Expected Delivery Date (EDD) + 26 weeks. At this stage the GP should review the prescription
and switch to a standard term formula which should be purchased by parents.
If there is a concern about growth, the baby should be referred back to the neonatal unit for advice. Not all babies require pre-term formula for the full 26 weeks from EDD. If there is excessive weight gain at any stage up to 6 months corrected age, the pre-term formula may be discontinued and a change made to a standard formula. Ready to feed liquids are substantially more expensive than the powder and should not be prescribed in primary care unless there is a clinical need e.g. the baby is immunocompromised, tube fed or there has been a specific request by secondary care.
Traffic Light
Product Age group Notes Cost/ 100 kcals (June 2017)
Nutriprem® 2
powder From birth to 6 months (corrected age)
GP to review and stop prescription at 6 months corrected age or if excessive weight gain.
£0.26
SMA® PRO Gold Prem 2 powder
£0.23

13 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
Traffic Light
Product Age group Notes Cost/ 100 kcals (June 2017)
Nutriprem® 2 liquid Only prescribe if the infant is immune-compromised, tube fed or as directed by secondary care.
£1.16
SMA® PRO Gold Prem 2 liquid
£1.12
8. Metabolic Products
Children under Dietetic Care may need to have other specialist formulas for reasons other than CMPA. Two examples of these could include formulas or products for metabolic patients and hydrolysed or amino acid based formulas for gastroenterology symptoms or treatment.
9. References and Acknowledgement
References: Bernie Canani R et al. (2013) Formula selection for management of children with cow’s milk allergy influences the rate of acquisition of tolerance: a prospective multicentre study. J Pediatr, 163 (3):771-7. Buller HA, Rings EH, Montgomery RK,Grand RJ. (1991) Clinical aspects of lactose intolerance in children and adults. Sc and J Gastroenterolgy Suppl,188:73-80.
Food Standard Agency statement on arsenic levels in rice milk (2009) http://webarchive.nationalarchives.gov.uk/20120403220542/http://www.food.gov.uk/multimedia/pdfs/fsis0209arsenicinrice.pdf Milk Allergy in Primary Care (MAP) Guidelines: Venter C, Brown T, Shah N, Walsh J Fox AT. (2013) Diagnosis and management of non-IgE-mediated cow's milk allergy in infancy - a UK primary care practical guide, Clinical and Translational Allergy, 3:23. www.cowsmilkallergyguidelines.co.uk/the-map-guideline/
Venter et al. (2017) Better recognition, diagnosis and management of non-IgE-mediated cow’s milk allergy in infancy: iMAP—an international interpretation of the MAP (Milk Allergy in Primary Care) guideline, Clinical Translational Allergy, 7:26. https://ctajournal.biomedcentral.com/articles/10.1186/s13601-017-0162-y NICE (2011) Food Allergy in Children and Young People. https://www.nice.org.uk/guidance/cg116. NICE (2015) Gastro-oesophageal reflux disease in children and young people. NG1 www.nice.org.uk Acknowledgement: This guideline has been produced by the Medicines Optimisation Team, Oxfordshire Clinical Commissioning Group in consultation with: Dr Felicitas Obetoh, Paediatrician with Interest in Allergy, Paediatric Allergy Clinic, Oxford University Hospitals NHS Trust

14 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
Dr Kenny McCormick, Neonatal consultant, Oxford Newborn Care Unit, Oxford University Hospitals NHS Trust Katheryn Clarke and colleagues, Community Paediatric Dietetics Team, Oxford University Hospitals NHS Foundation Trust Suzanne Bradshaw, Prescribing Support Dietitian, Oxfordshire Clinical Commissioning Group This guideline has been based on the following documents: PrescQIPP Bulletin 146, November 2016: Appropriate prescribing of specialist infant formulae (foods for special medical purposes) Central London Community Healthcare, Paediatric Dietetics Service, August 2015: Primary Care Specialist Infant Formulae Prescribing Guidance Pan Mersey Area Prescribing Committee, November 2014: Pan-Mersey Prescribing Guidelines for Specialist Infant Formula Feeds in lactose Intolerance and Cow’s Milk Protein Allergy. Ipswich and East Suffolk Clinical Commissioning Group, September 2015: Recommendations for Prescribing Specialist Infant Formula 2015/16.

15 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
Appendix 1: Suspected Cow’s Milk Allergy (CMA) in the 1st Year of Life

16 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
Appendix 2: Primary Care Management of Mild to Moderate Non-IgE CMA

17 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
Appendix 3: Initial factsheet for parents

18 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.

19 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
Appendix 4: The Early Home Reintroduction to Confirm Diagnosis – leaflet for parents

20 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.

21 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
Appendix 5: The iMAP Milk Ladder

22 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.

23 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
Appendix 6: Infant Formula products – quick reference guide
ALL CONDITIONS - Suggested Prescribing Quantities of Powdered Formula per month
< 6months 6 -12 months >12 months
13 x 400g tin OR 6 x 900g tins 7-13 x 400g tins OR 3-6 x 900g tins 7 x 400g tins OR 3 x 900g tins
Milk Type Proprietary Brand Suitable for Cost / Original pack (T = Trade; R = Retail)
Cost / 100g or 100ml
Supply Route
Cow’s Milk Protein Allergy (CMPA)
Extensively Hydrolysed Formula (EHf)
Nutramigen LGG1 < 6m £10.99 (400g)T £2.75 FP10
Nutramigen LGG2 > 6m £10.99 (400g) T £2.75 FP10
Aptamil Pepti 1 < 6m £19.70 (800g) T £2.47 FP10
Aptamil Pepti 2 > 6m £9.35 (400g) T £2.35 FP10
Similac Alimentum 0 – 18m £9.10 (400g) T £2.28 FP10
Althera 0 – 18m £10.68 (450g) T £2.37 FP10
Pregestimil Lipil From birth £12.19 (400g) T £3.05 FP10
Pepti Junior From birth £13.06 (450g) T £2.90 FP10
Amino Acid Formulas (AAf)
SMA Alfamino From birth £23.00 (400g) T £5.75 FP10
Nutramigen PurAmino From birth £27.09 (400g) T £6.77 FP10
Neocate LCP From birth £28.70 (400g) T £7.18 FP10
Neocate Junior From 1 year to 10 years
£28.70 (400g) T £7.18 FP10
Review need if child is 18 months, has been prescribed for >1 year, able to eat cheese, yoghurt, chocolate, or butter
Gastro-oesophageal Reflux Disease
Anti-Reflux Cow & Gate Anti-reflux From birth £11.21 (900g) R £1.28 OTC
Aptamil Anti-reflux From birth £13.49 (900g) R £1.44 OTC
*SMA Staydown From birth £10.99 (900g) R £1.22 OTC
SMA PRO Anti-reflux From birth £10.00 (800g) R £1.25 OTC
**Enfamil AR From birth £6.90 (400g) R £1.73 OTC
* Being replaced by SMA PRO Anti-reflux and is available for further few months. ** may have to be specially ordered at the pharmacy
Secondary Lactose intolerance
Lactose-free SMA LF < 12m £6.00 (430g) R £1.40 OTC
Enfamil O-Lac < 12m £9.21 (400g) R £2.30 OTC
Aptamil LF < 12m £5.99 (400g) R £1.50 OTC
Lactofree >12m £1.35 (1000ml) R £0.14 Shops
Symptoms usually resolve within 8 weeks. Lactose free milk is available in supermarkets for infants > 12 months
Faltering Growth
High energy SMA PRO High Energy Birth – 18m/ 8kg £1.97 (200ml) T £0.99 FP10
Similac High Energy Birth – 18m/ 8kg £2.13 (200ml) T £1.07 FP10
Infatrini Birth – 18m/ 8kg £2.23 (200ml) T £1.11 FP10
Infatrini Peptisorb Birth – 18m/ 9kg £3.54 (200ml) T £1.77 FP10
Ensure that there is a clear goal and discontinuation point
Pre-term
Initiated in secondary care
Nutriprem 2 powder Birth – 6m (corrected age)
£11.67 (900g) T £0.26 FP10
SMA PRO Gold Prem 2 powder
Birth – 6m (corrected age)
£4.92 (400g) T £0.23 FP10
Nutriprem 2 liquid Birth – 6m (corrected age)
£1.74 (200ml) T £1.12 FP10
SMA PRO Gold Prem 2 liquid
Birth – 6m (corrected age)
£2.05 (250ml) T £1.16 FP10
These milks are not suitable for infants > 6months (corrected age). Do not prescribe ready to use liquid unless essential

Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
Appendix 7: Summary of guidelines (NOT TO BE USED FOR DIAGNOSIS)
Summary of Guidelines on prescribing specialist infant formula in primary care (NOT TO BE USED FOR DIAGNOSIS) For diagnosis and prescribing please see the full OCCG guidelines.
Some children may require more, e.g. those with faltering growth. Review recent correspondence from the paediatrician or paediatric dietitian.
All conditions: How much powdered infant formula should I prescribe monthly?
Under 6 months 6 – 12 months Over 12 months
400g tin 900g tin 400g tin 900g tin 400g tin 900g tin
Up to 12 tins Up to 5 tins 6 – 12 tins 3 – 5 tins Up to 6 tins Up to 3 tins
Cow’s Milk Protein Allergy
(CMPA):
IgE symptoms (<2hrs onset) [See page 4 of the full guidelines for diagnosis algorithm] – Skin symptoms: urticaria, pruritus, angioedema; respiratory: difficulty in breathing and swallowing, hoarse cry, acute wheeze or anaphylaxis.
Non-IgE symptoms (2-72hrs onset) [See page 5 of the full guidelines for diagnosis algorithm] - Skin symptoms: pruritus, erythema, urticaria, atopic dermatitis; GI symptoms: diarrhoea, bloody stools, vomiting, abdominal distention, colicky pain, constipation, GORD; Respiratory symptoms: recurrent wheeze/ cough, nasal itching, sneezing or congestion and rhinorrhoea. Growth faltering.
Most infants with CMPA develop symptoms within 1- 2 weeks of introduction. Mild – moderate non-IgE CMPA can be managed in primary care. Early diagnosis and treatment is very important. Download The iMAP Milk Allergy Guideline– Initial Fact Sheet for parents whose infants fall under this group.
Breast milk is the best choice for most infants with CMPA. Breastfeeding mothers may require a dairy free diet and daily 1000mg calcium and 10 mcg Vitamin D supplementation.
Refer to paediatric community or paediatric dietitians for weaning advice before infant is 6 months of age. Always review the latest clinic correspondence before issuing each prescription to ensure any recommended changes are implemented.
First line: Extensively Hydrolysed formula (EHf) Soya milk, lactose-free (LF) formula, rice milk or other mammalians milk are not suitable in CMPA
Most cost-effective: Similac Alimentum
Other options: Althera, Aptamil Pepti 1&2, Nutramigen 1&2 with LGG
To confirm diagnosis, perform Early Home Reintroduction in infants with mild-moderate non-IgE CMPA (2 – 72 hours). Not safe for immediate symptoms of IgE CMPA. At diagnosis EHf should be continued for at least 2 -4 weeks and if symptoms improve, Home Reintroduction should be performed after 2-4 weeks of starting EHf to confirm the diagnosis of CMPA. Download iMAP’s parent leaflet on The Early Home Reintroduction to confirm diagnosis to support parents at home.
Second line: Amino Acid formula (AAf) Secondary care initiation or recommendation only. Consultant-led email advice: [email protected].
Most cost-effective: Alfamino
Other options: Nutramigen PurAmino, Neocate LCP, Neocate Junior
Reintroduction: Patients should be evaluated after at least six months of exclusion of dairy products to assess acquired tolerance to CMP. Download iMAP milk ladder and recipes to support parents reintroduce CM at home, provided there is no history of immediate allergic reactions or other indications for referral to secondary care.
Review the need for specialised formula prescription regularly and consider STOPPING if any of the following applies: Can the patient tolerate any dairy foods? Is the patient over 18 months old (continue treatment if specifically indicated by specialists)? Has the formula been prescribed for more than one year? Is the quantity prescribed more than the recommended amount?
Refer infants with anaphylaxis or faltering growth to secondary care
urgently.

25 Guidelines on Prescribing Specialist Infant Formulas in Primary Care v1. Approved APCO September 2017. Review September 2019.
Gastro-oesophageal
Reflux Disease (GORD)
GORD presents with a history of effortless vomiting after feeding (up to two hours), usually in the first six months of life. [See page 10 of the full guidelines for more details]
Over feeding should be ruled out by establishing the volume and frequency of feeds.
Give reassurance and advice on positioning post-feeds.
Infant Gaviscon can be given up to a maximum of six times per day.
Initially recommend adding Carobel (available from pharmacies) to current standard formula, or trial anti-reflux formula (available from pharmacies/ supermarkets) for 1-2 weeks and review symptoms.
Cow and Gate Anti-reflux, Aptamil Anti-reflux, SMA PRO Anti-Reflux, Enfamil AR
Secondary Lactose
Intolerance
Secondary lactose intolerance usually occurs following an infectious GI illness (but can occur alongside new or undiagnosed coeliac disease) and is usually self-limiting. [See page 11 of the full guidelines for more details]
Symptoms include abdominal bloating, increased explosive wind and loose green stools.
Resolution of symptoms within 48 hours of withdrawal of lactose from the diet confirms diagnosis.
Initially recommend over-the-counter lactose-free (LF) formula for two weeks. Continue LF formula for up to eight weeks if symptoms improved. Symptoms usually resolve within this time but in rare cases may take up to three months.
0 – 12 months: Enfamil O-Lac, SMA® LF, Aptamil LF
Over 12 months: Lactofree
Faltering Growth
Faltering growth cannot be detected without using a growth chart. Diagnosis is usually made when an infant falls below the 0.4th centile or crosses 2 centiles downwards on a weight or height centile. [See page 12 of the full guidelines for more details] Consultant-led email advice: [email protected].
First line: High-energy formula Secondary care initiation or recommendation only. Discontinue when on an appropriate diet as per dietitian advice.
Most cost-effective: SMA PRO High Energy
Other options: Similac High Energy, Infatrini, Infatrini Peptisorb (high calorie EHf)
Pre-term
These infants will have had their pre-term formula commenced on discharge from the neonatal unit and will be under regular review by the paediatricians. Pre-term formula should not be commenced in primary care unless recommended by a specialist. GPs should discontinue these formulas after the infants are six months corrected age or if there is excessive weight gain. [See page 12 of the full guidelines for more details]
Started in secondary care: Pre-term formula DO NOT prescribe liquid formula unless immune-compromised, tube fed or clinically indicated by secondary care.
Nutriprem 2 powder, SMA PRO Gold Prem 2 powder
Nutriprem 2 liquid, SMA PRO Gold Prem 2 liquid
This quick reference guide has been adapted from PrescQipp B146: Specialist infant feeds quick reference guide.
Refer to secondary care without delay.
Refer infants with faltering growth to secondary care without delay.