Guidelines on Maternal-Nutrition in Uganda · ACRONYMS AED Academy for Education Development ANC...
37
MINISTRY OF HEALTH Guidelines on Maternal - Nutrition in Uganda - 1 st EDITION DECEMBER 2010 1
Transcript of Guidelines on Maternal-Nutrition in Uganda · ACRONYMS AED Academy for Education Development ANC...

MINISTRY OF HEALTH
Guidelines on MaternalNutrition in Uganda
1st EDITION DECEMBER 2010
1

ACKNOWLEDGEMENTS
The Ministry of Health would like to acknowledge the valuable contribution of partners, groups, and individuals at various stages of the development of these guidelines.
Ministry of Health is indebted to A2Z: The USAID Micronutrient and Child Blindness Project/AED and UNICEF for technical and financial support that made the development and finalization process of the guidelines possible.
Ministry of Health is grateful to the technical working group: Dr. Alfred Boyo (A2Z/AED), Annet Kyarimpa Mugabe (A2Z/AED), Dr. E. Madraa (MOH), Tim Mateeba (MOH), Rebecca Mirembe (MOH), Dr. Jacinta Sabiiti (MOH), Sheila Katurebe (MOH), Dr. G. Bisomborwa (WHO), Dr. Miriam Mutabazi (MSH-Strides).
Special thanks and appreciation is extended to Dr. Alfred Boyo, Annet Kyarimpa Mugabe and Tim Mateeba for coordinating the entire process.
Dr. Anthony. K. Mbonye Commissioner Community Health Ministry of Health
2

TABLE OF CONTENTS
ACRONYMS .............................................................................................................................................. 5
FOREWARD............................................................................................... Error! Bookmark not defined.
1. INTRODUCTION................................................................................................................................ 9
1.1. Overview............................................................................................................................................ 9
1.2. Situation analysis .............................................................................................................................. 11
1.3. Justification ....................................................................................................................................... 11
1.4. Purpose of the guidelines ................................................................................................................. 12
1.5. Goal and objectives of the guidelines .............................................................................................. 12
1.6. Target audience................................................................................................................................ 12
2. MATERNAL NUTRITION INTERVENTIONS........................................................................... 13
2.1. Maternal nutrition interventions during preconception .................................................................. 13
2.1.1. Nutritional assessment during preconception .......................................................................... 13
2.1.2. Micronutrient deficiencies prevention and control through diet and supplementation........... 14
2.1.3 Nutrition education/counseling during preconception.............................................................. 16
2.2. Maternal nutrition interventions during antenatal care ................................................................... 17
2.2.1. Nutritional assessment .............................................................................................................. 17
2.2.2. Nutritional requirements of pregnant women.......................................................................... 22
2.2.3. Nutrition education/counseling during antenatal care .............................................................. 23
2.2.4. Common physiological disturbances during pregnancy ............................................................ 23
2.3. Maternal nutrition interventions during postnatal care................................................................... 24
2.3.1. Nutritional assessment of lactating women .............................................................................. 24
2.3.3. Nutritional requirements during lactation ................................................................................ 25
3. MATERNAL NUTRITION UNDER SPECIAL CIRCUMSTANCES ...................................... 26
3.1 Diseases ............................................................................................................................................ 26
3

3.2. Social factors, local practices, and environmental issues affecting maternal nutrition .................... 27
3.2.1. Child spacing.............................................................................................................................. 27
3.2.2. Myths, local practices, and gender issues that affect maternal nutrition ................................. 28
3.2.3. Substance abuse ........................................................................................................................ 28
3.2.4. Maternal nutrition in emergencies ............................................................................................ 29
3.2.5. Nutritional care for adolescent pregnancy ............................................................................... 29
3.2.6. Community support for maternal nutrition.............................................................................. 29
3.2.7. Water, sanitation, and hygiene.................................................................................................. 30
4. IMPLEMENTATION ........................................................................................................................ 31
5. MONITORING AND EVALUATION ......................................................................................... 34
ANNEX I: Counseling Job aid for Health Workers on Prevention and Control of Anemia .................. 35 ANNEX 2: Protocols for Interventions to Prevent and/or Treat Maternal Anemia............................... 36
4

ACRONYMS
AED Academy for Education Development ANC Antenatal Care BFHI Baby-friendly hospital initiative BMI Body Mass Index DHT District Health Team DOT Direct observed Therapy FP Family planning HIMS Health Information Management Service IDD Iodine deficiency disorders IEC Information Education and Communication IFA Iron and Folic Acid IPT Intermittent Presumptive treatment ITNs Insecticide Treated Nets LBW Low birth weight baby MDG Millennium Development Goals MOH Ministry of Health MUAC Mid-Upper Arm Circumference NDP National Development Plan NGO Non-Governmental Organization NTD Neglected Tropical Diseases PEM Protein energy malnutrition PMTCT Prevention of mother-to-child transmission PNC Prenatal care RCT Routine Counseling and Testing TB Tuberculosis UDHS Uganda Demographic Health Survey VAD Vitamin A deficiency VHT Village health teams WHO World Health Organization YCC Young Child Clinic
5

FOREWARD
Maternal nutrition plays a critical role in the reduction of maternal morbidity and mortality. This document provides guidance on nutrition for women of reproductive age. During periods of pregnancy and lactation, women’s nutrition becomes particularly vulnerable. Maternal malnutrition in Uganda is cyclical: mothers give birth to low birth-weight babies who were undernourished in utero, and these children are then stunted during childhood, pregnant during adolescence, underfed and overworked during pregnancy and lactation, and ultimately give birth to low birth weight babies of their own. This report provides guidance on how to break this intergeneration cycle of maternal malnutrition by outlining special nutritional interventions at preconception, pregnancy, and lactation that enable safer and more optimal birth outcomes. These guidelines should be implemented in conjunction with the existing Infant and Young Child Feeding policy guidelines to improve the health of babies, which will ultimately result in healthier adolescents and adults.
It is important that all maternal health stakeholders in Uganda utilize these guidelines by integrating the recommendations for implementation into their programs and supporting and/or funding the interventions, thus contributing to a reduction of maternal malnutrition as well as the associated morbidity and mortality.
These maternal nutrition guidelines have been developed to improve the knowledge and skills necessary for service providers at all levels to adequately respond to maternal and child nutritional needs; improve provision of quality maternal and child nutritional services at the community and health facility level; to provide a basis for advocacy efforts that garner support for maternal nutrition interventions at all levels, to facilitate workshops for health care providers and other stakeholders on interpersonal nutrition education and counseling, community dialogue, development of IEC materials, and health education for improved maternal nutrition; and to strengthen integration of nutrition interventions for adolescent, pregnant, and lactating women within existing health services.
These recommendations set forth by the Ministry of Health aim to ensure the provision of optimal maternal nutrition services. MOH will continue to coordinate and monitor the implementation of the guidelines.
The following recommendations can be followed to improve the provision of maternal health and nutrition services in Uganda:
Recommendation 1: Folic acid at preconception Folic acid should be provided as a supplement, in addition to adequate intake of foods rich in folic acid, to women prior to conception to prevent neural tube defects in newborns.
Recommendation 2: Proper weight gain during pregnancy i. Based on BMI results, women who are underweight, overweight, or obese should
receive counseling regarding appropriate diet for adequate weight gain during pregnancy. ii. A woman at preconception is considered to be underweight when her MUAC reading is
less than 21.0cm.
6

iii.� A pregnant or lactating woman is considered to be underweight when her MUAC reading is less than 23.5cm.
Recommendation 3: Antenatal care and iron and folic acid supplementation i. All pregnant women should be screened for anemia and corrective action taken. ii. All pregnant women should be encouraged to attend at least four ANC sessions at
health facilities during which they receive iron and folic acid supplementation according to nationally accepted protocols to prevent anemia.
iii. Pregnant women should be counseled to ensure compliance with the recommended iron and folic acid supplementation intake of at least 90+ tablets.
Recommendation 4: Malaria and worm control to prevent anemia i.� All expectant mothers should be given preventive doses of fansidar and dewormers
during the second and third trimesters. ii.� Women should be advised to sleep under ITNs and practice adequate personal and
environmental hygiene.
Recommendation 5: Diet during pregnancy and lactation In addition to the regular three meals, women should be counseled to eat at least one extra meal (snack) per day while pregnant and two extra meals per day while lactating, to meet the daily energy requirements of pregnancy and lactation respectively.
Recommendation 6: Vitamin A supplementation i.� Women should be counseled and given a one-time dose of 200,000IU of vitamin A
within eight weeks of giving birth. ii.� For mothers who have opted NOT to breast feed their infants, a one-time, low dose of
50,000IU should be given to the infant to help boost immunity.
Recommendation 7: Postnatal care and iron and folic acid supplementation All postnatal w omen should be given routine iron and folic acid supplementation within six weeks of delivery and be counseled to ensure compliance with the recommended dosage of one tablet per day for three months.
Recommendation 8: Iodine supplementation All women of reproductive age should be counseled on the daily intake of iodine by using iodized salt.
Recommendation 9: Nutrition counseling and education All women of reproductive age should be given sufficient nutritional counseling and education to promote improved nutritional status on the following topics:
i.� Intake of foods rich in iron, folate, vitamin A, and iodine. ii.� Intake of variety of foods that includes protein, energy, vitamin and mineral rich foods. i.� Clean and safe drinking water and personal and environmental hygiene.
7

Recommendation 10: Breastfeeding and family planning Women should be counseled on the role of, and conditions for, exclusive breastfeeding as a method of family planning in addition to other family planning methods.
Recommendation 11: Education regarding local practices that negatively affect maternal nutrition Health care providers should educate and counsel mothers and family members regarding all forms of myths, taboos, or local practices that affect the nutritional status of women before, during, and after pregnancy.
Recommendation 12: Nutrition during emergencies During emergency situations, humanitarian aid programs should prioritize vulnerable groups that include children, pregnant women, and lactating mothers in their nutrition outreach to meet their energy and other nutrient needs.
Dr. Nathan Kenya-Mugisha For Director General of Health Services
8

1. INTRODUCTION
1.1. Overview
The term maternal nutrition refers to nutrition of a woman during any stage of her reproductive age, which eventually affects the health of the fetus and/or infant, as well as herself.
There are heightened nutrient needs during pregnancy and lactation. Without an increase in energy and other nutrient intake to meet the increased needs during this time, the woman’s body uses its own reserves, leaving her weakened and vulnerable to pregnancy-related complications.
Many women are undernourished at birth, stunted during childhood, become pregnant during adolescence, are underfed as well as overworked during pregnancy and lactation, and, consequently, give birth to low birth weight babies. It is these children who eventually become stunted women, perpetuating the intergeneration cycle of malnutrition among women. Undernutrition weakens a woman’s ability to survive childbirth and give birth to a healthy baby, translating into increased morbidity and mortality of mothers and their infants.
The impact of poor maternal nutrition begins before a woman conceives, and continues through pregnancy, delivery, and finally, lactation, where the cycle may resume.
In Uganda, as in many developing countries, most pregnancies are not planned. In such circumstances, health service providers should emphasize the importance of good nutrition for women during contact with communities, adolescents, when pregnancy is confirmed, and during Young Child Clinic visits.
The main forms of maternal malnutrition include: Macronutrient deficiencies (Protein Energy Malnutrition - PEM):
o PEM is managed by ensuring: (a) adequate frequency of food intake (b) adequate amounts of food (c) adequate variety of foods to include the 3 major groups, and (d) proper personal and environmental hygiene.
Micronutrient deficiencies, such as iron deficiency anemia, vitamin A deficiency (VAD), and iodine deficiency disorders (IDD): These conditions result in increased risk of maternal mortality, low birth weight, and neonatal and infant mortality. Anemia is observed to contribute to about 20% of maternal deaths. It increases the risk of hemorrhage and prolonged labor, which can lead to sepsis.
Micronutrient deficiencies can be managed by (a) adequate intake of foods rich in micronutrients such as fruits and dark-green and brightly colored vegetables, (b)�supplementation with fortified foods and mineral/vitamin formulations.�
9

Underlying Causes
Inadequate maternal
care.
Household food
insecurity.
Unhealthy
environment,
insufficient health
services, and poor hygiene and
sanitation.
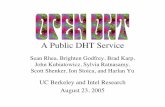
Causes and consequences of maternal malnutrition in Uganda There are many factors contributing to maternal malnutrition as summarized in Table I below:
Figure I: Summary Causes of Maternal Malnutrtion
Immediate Causes Consequences
Women’s Poor Health • Infections and diseases
• Poor access to basic health
services (e.g. inadequate iron and folic acid
supplementation).
• Frequent parasites and infections.
Inadequate Food Intake Due to diet characterized by
Low, highly variable over
seasons, and often of low
nutrient density.
Basic Causes
Political structure
Resources and their control
Heavy workloads
Frequent births
Harmful local practices and food taboos.
Intrahousehold food distribution does not favor women.
Maternal Health Increased risk of maternal
death. Increased infections. Anemia Compromised immune
functions. Lethargy and weakness. Lower productivity.
Infant/Child Health Increased risk of fetal and
neonatal death. Intrauterine growth
retardation, low birth weight, preterm birth.
Compromised immune functions.
Birth defects. Cretinism and reduced IQ.
10

1.2. Situation analysis The current maternal mortality ratio in Uganda is estimated at 435/100,000 live births,1
translating to 6,000 women dying annually. Twenty percent of these deaths (1,200 women) are attributable to maternal malnutrition (Lancet Series, 2008)2
Demographic and Health Surveys data from 2006 indicate that maternal malnutrition is highly prevalent in Uganda as shown below: 12% of women (neither pregnant nor lactating) between the ages of 15–49 years are
undernourished or “thin” (BMI less than 18.5). Anemia prevalence: 49% of women in reproductive age, 64% of pregnant women, and
53% of lactating women. VAD prevalence: 18.6% of pregnant women and 17.3% of lactating mothers.
Although known interventions that address maternal malnutrition exist, the majority of mothers in Uganda do not have access to this information or services.
For example: 1 in 3 mothers receive postpartum vitamin A supplementation. 47% of mothers attend four or more ANC visits. Less than 1% of mothers followed the recommended dose of 90+ IFA supplementation. 60% of pregnant women took iron supplements for 60 days or less. 16% of pregnant women received IPT2. 24% of women reported sleeping under mosquito nets. 26.8% deworming coverage of pregnant women.
1.3. Justification In Uganda, one of the obstacles to the provision of improved maternal nutrition health services is lack of comprehensive reference nutrition recommendations for health service providers to use in providing nutrition counseling to women on how to meet their nutritional requirements through dietary and behavioral changes.
This document aims to: Highlight the plight of maternal malnutrition and the attention it deserves in the
minimum health care package and nutrition programs.� Provide information to, and increase knowledge amongst, health service providers on
how to counsel women to meet their increased nutritional requirements through dietary and behavioral changes and health care-based services.
Provide a comprehensive reference material for maternal nutrition.
1 Uganda Demographic and Health Survey (UDHS), 2006. 2 Lancet Series, 2008. 3UDHS, 2006.
11
3

The adequate implementation of the recommendations outlined in this document will contribute significantly to provision of improved and adequate maternal nutrition services in Uganda. It will contribute information that will, together with other maternal health improvement programs, support the reduction of maternal morbidity and mortality, and help Uganda move towards attainment of Millennium Development Goal (MDG) 5 of reducing the maternal mortality ratio by 3/4.
1.4. Purpose of the guidelines The main purpose of these guidelines is to support health care providers in the provision of maternal nutrition care and support services. The guidelines can also be used by health training institutions, schools, and other organizations, as well as other line ministries implementing maternal nutrition interventions.
1.5. Goal and objectives of the guidelines To contribute to the reduction of maternal and child morbidity and mortality through improved maternal nutrition in Uganda and with specific focus:
To improve the knowledge and skills of service providers at all levels to respond to maternal and child nutritional needs.
To improve provision of quality maternal and child nutritional services at community and health facility level.
To advocate for support of appropriate interventions that address maternal nutrition at all levels.
To facilitate health care providers and other stakeholders in interpersonal nutrition education and counseling, community dialogue, development of IEC materials and health education for improved maternal nutrition.
To strengthen integration of nutrition interventions for adolescent, pregnant, and lactating women within existing health services.
1.6. Target audience Primary target: This includes health care providers such as midwives, nurses, clinical officers, doctors, nutritionists, dieticians, counselors, health promoters and educators, nutrition teachers, and institutions and organizations implementing maternal nutrition interventions.
Secondary target: This includes, health training institutions, schools, non-governmental organizations (NGOs) and community-based organizations implementing maternal nutrition interventions.
Additional target: Other line ministries - such as education, agriculture, animal industry and fisheries, gender, labor and community development, local government, and water and sanitation can use these guidelines.
12

2. MATERNAL NUTRITION INTERVENTIONS
2.1. Maternal nutrition interventions during preconception The nutritional status of a woman before conception is a key determinant of the pregnancy outcome and the health of the newborn. Adolescent girls and women need to attain appropriate nutritional status in order to prepare them to meet the future needs of pregnancy -for both the mother and unborn child.
The objectives of nutritional care in the pre-conception period are to encourage women to achieve appropriate weight for height and healthful dietary habits.
The interventions during preconception are: Macro-nutrient assessment Micro –nutrient deficiency prevention and control through supplementation Nutrition education/counseling
2.1.1. Nutritional assessment during preconception To offer proper nutrition services for macro-nutrients, health workers need to establish the nutritional status of women 15-49 years using BMI and MUAC. Suggested contact points for this activity include family planning visits, community outreaches for maternal health care, immunization/young child clinic visits.
Body mass index (BMI) BMI is one of the measures used to determine a woman’s nutritional status., It is a measure of thinness or obesity. Measuring BMI prior to pregnancy is important because it allows a health worker to determine the weight that should be gained during pregnancy.
Assessment using BMI: Below 18.5 – Underweight (chronic energy deficiency) 19 – 24.9 - Normal 25 – 30 - Overweight More than 30 - Severe overweight (obese)
How to calculate BMI: BMI = Weight in kilograms / [(Height in meters) x (height in meters)]�
There is a strong relationship/association between low pre-pregnant weight and height, and intra uterine growth retardation of the fetus.�
Mid upper arm circumference (MUAC) MUAC directly assesses the amount of soft tissue in the arm and is a measure of thinness or fatness. It is the easiest index to use in the community for screening and identifying women in need of further nutrition assessment and/or treatment
13

Assessment using MUAC: A woman at pre-conception is considered underweight when the MUAC reading is
less than 21cm. A pregnant or lactating woman whose MUAC is less than 23.5cm is considered to
be underweight.
How to measure MUAC: 1.� Locate tip of shoulder bone with your fingertips. 2.� Bend the woman’s elbow to make a right angle and find the tip of the elbow. 3.� Place the beginning of the measuring tape at the tip of the shoulder and pull the
tape straight down past the tip of the elbow. 4.� Read the number at the tip of the elbow to the nearest centimeter. 5.� Divide the reading in step number four to get the midpoint of the upper arm. Mark
midpoint (or as an alternative, bend the tape in two from the elbow to the shoulder to estimate the mid-point and mark it).
6.� Straighten the arm and let it hang loose. Measure around the upper arm at the midpoint, making sure that the tape is flat around the skin and the numbers are right side up.
7.� Make sure the tape has the proper tension i.e. it should not be too tight or too loose around the mid-upper arm.
8.� Once the tape is in the correct position, with the correct tension, r ead the measurement in centimeters (cm) to the nearest 0.1cm.
9.� Record the reading accurately.
2.1.2. Micronutrient deficiencies prevention and control through diet and supplementation
The relevant micronutrients at preconception include: Folic acid� Iron� Iodine Calcium
Folic acid The role of folic acid at preconception is to reduce the risk of birth defects of the brain and spine, called neural tube defect (NTD) in the newborn.
The neural tube closes during the 4th week of pregnancy - a time when most women may not even know they are pregnant. Because most pregnancies in Uganda are unplanned, it is especially crucial for all women of childbearing age (15 – 49 years) to have an adequate intake of folic acid through food diets and/or supplementation.
Those women at high risk of neural tube defect outcomes include: - Those previously affected by folic acid deficiency - Those with a family history of NTD or diabetes, who have sickle cell anemia, or who
are on anti-epileptic medication.
14

Recommended actions Folic acid should be taken in through appropriate diets and supplementation by women
prior to conception to prevent NTD in the newborn. Counsel women on the consumption of foods rich in folic acid such as dark green leafy vegetables (i.e. spinach), citrus fruits, nuts, legumes, whole grains, and fortified breads and cereals.
Supplement dosage 400 micrograms a day for one month for pre-pregnancy care.
Iron The intake of iron before conception helps to provide adequate reserves that help to prevent anemia later during pregnancy.
Recommended actions Women should be counseled on intake of iron rich foods such as liver, red meat,
kidney, fish, chicken, millet, ground nuts, and green leafy vegetables. Women should be counseled to avoid foods containing iron absorption inhibitors (tea/
coffee) just before, during and shortly after meals, and to consume foods containing caffeine two or more hours before or after iron containing foods or iron supplements.
Women should be counseled on intake of foods containing iron absorption enhancers just before, during and after meals (e.g. foods rich in vitamin C like oranges, tangerines, mangoes, meat and fish products, tomatoes, green peppers etc.).
Weekly iron supplementation of 60mg (200mg of iron sulphate) as is recommended for women for three months prior to conception, per the WHO guidelines, 2009.
Iodine Role of iodine in maternal nutrition: Iodine helps to prevent IDD
Symptoms of iodine deficiency Enlargement of thyroid gland (goiter) is the first sign of iodine deficiency, and presents
as a swelling on the forward lower part of the neck.
Recommended actions All women should be counseled on intake of iodine through use of iodized salt.
Calcium Calcium is needed for building bones and teeth, for blood clotting, for regulating nerve and muscle activity and for absorption of iron. Women’s bone density diminishes in the first three months of pregnancy as a result of increased calcium uptake by the developing fetus. It is advisable to ensure sufficient calcium intake during preconception to build up calcium reserves in preparation for pregnancy.
15

Recommended action Women should be counseled to consume foods rich in calcium such as dairy products (yoghurt, milk, and cheese), eggs, fish, beans, soybeans, beef and cereals like whole millet and rice.
2.1.3 Nutrition education/counseling during preconception
Health workers should provide nutrition education and counseling prior to pregnancy in order to promote maternal health and good pregnancy outcomes. Nutrition education should be conducted for individuals, communities, schools, in outreaches and at health facilities. The counseling should include: Variety of foods Frequency of foods Hygiene Focus on locally available foods Importance of the adequate nutrition before pregnancy. Folic acid supplementation Prevention of anemia
Advise on nutritional requirements during preconception No single food contains all the nutrients the body needs. A variety of foods should be consumed at every meal. These include: Energy giving foods, such as cereals like maize meals, rice, millet, sorghum, roots and
tubers e.g. potatoes, cassava, and plantains like bananas etc Protein giving foods include animal products such as meat, milk, eggs, and fish, and plant
products such as legumes like beans, peas, soya, and groundnuts. Minerals and vitamin rich foods such as fruits and vegetables
Key nutrition messages during preconception Prevention of worm infestations through regular de-worming at least twice a year and
wearing of footwear. Regular exercise. Adequate consumption of water (at least 2 liters per day). Regular consumption of fiber rich foods which are essential for movements of the
gastrointestinal tract (whole grains, fruits, vegetables). Encourage consumption of a variety of locally available foods. Provide guidance on appropriate food preparation methods to preserve the nutritional
value and safety. Counsel on iron/zinc/calcium absorption inhibitors. Examples of foods containing
inhibitors include tea, coffee, spinach and soya bean. Intake of these foods that contain the inhibitors should be avoided when consuming other iron-rich foods. It is advisable to consume foods containing caffeine two or more hours before or after iron-rich foods or iron supplements have been taken.
Counsel on nutrient absorption enhancers. Encourage intake of foods rich in absorption enhancers just before, during, and after meals, such as vitamin C-rich foods like oranges, tangerines, mangoes, meat and fish products, tomatoes, green peppers etc.
16

Counsel on obtaining the optimal weight for height as indicated by a BMI value that is at or higher than 18.5, but lower than 25.
2.2. Maternal nutrition interventions during antenatal care
Antenatal care offers an opportunity for assessment of the nutritional status of a pregnant woman as well as the assessment of essential nutritional actions and continuous monitoring throughout pregnancy. There are heightened nutrient needs during pregnancy. Without a corresponding increase in energy and other nutrient intakes, the body’s own reserves are used, leaving a pregnant woman weakened and vulnerable to maternal and fetal complications, and, at worst, death.
The interventions during antenatal care are categorised as: Nutritional status assessment Micronutrient supplementation Nutrition education/counseling during antenatal care Managing common nutrition related physiological disturbances during pregnancy
2.2.1. Nutritional assessment
The relevance of nutrition assessment during pregnancy is for monitoring progress of pregnancy and detecting risk factors for the mother, the fetus and/or the infant associated with nutritional deficiencies. A pregnant woman who is underweight or micronutrient deficient is more likely to have poor birth outcomes affecting both mother and baby. On the other hand, a pregnant woman who is overweight has an increased risk of coronary heart disease, high blood pressure, high blood cholesterol, and diabetes that can complicate a pregnancy.
Comprehensive nutrition assessment This should commence on the woman’s first contact with the health worker, and should include aspects shown in Table I on the following page.
17

Table I. Nutrition Assessment during Pregnancy Assessment What to Ask or Measure Nutrition History
Dietary intake (frequency, quantity and diversity) Eating habits (dieting, craving, food myths & taboos) Food intolerance and dislikes Fatigue and physical activity Nausea, vomiting Heartburn Substance abuse during pregnancy (alcohol, smoking) Availability of clean, and safe water Sanitation and hygiene practices in food preparation and handling
(personal hygiene, food preparation and handling, Daily intake of iron and folic acid supplements Use of iodized salt
Physical Anthropometric measurements: Assessment Height
Pre-pregnancy weight Weight gain during pregnancy MUAC
Other physical features Oedema Pallor (palm, tongue, conjunctiva) Goitre
Medical History
History of constipation, diarrhea, previous births with NTD Concurrent medical problems (e.g., diabetes, hypertension,
coronary heart disease, asthma) Outcome of previous pregnancy/pregnancies (e.g. LBW, difficult
deliveries, prematurity) Laboratory Investigations
Heamoglobin level
Medication Profile
Medications used for concurrent medical problems (e.g., diabetes, hypertension, ischemic heart disease, malaria, HIV/AIDS, TB)
Psychosocial Profile
Living environment and functional status (income, housing, amenities for cooking, access to food, attitudes to nutrition and food preparation)
Age Family or support system Educational level
Source: Regional Centre for Quality of Health CARE, FANTA, and LINKAGES. 2003.�
18

Following the assessments detailed in Table I above, women at risk of malnutrition and its complications will be identified. At-risk groups may include the following:
Women who were obese at the time of conception. Women who gain too little or too much weight (see 2.2.2.1 below). Women whose height is less than 145cm. Women with MUAC less than 23.5 cm. Pregnant adolescents (younger than 18 years of age). Women with short birth intervals (less than 1 year). Women with too-early pregnancies below 18 years of age. Women with too-late pregnancies above 40 years of age. Women with a history of low birth weight infants (less than 2500gm). Women who are HIV positive/ have AIDS. Women living in poor socio-economic situations. Women in emergency situations like famine, wars, civil strife and other hazards –
manmade and natural.
Recommended action Women identified as at-risk of malnutrition need closer nutritional and medical attention and should be advised to have more frequent visits to the health service providers in order to receive appropriate care and support.
Weight gain during pregnancy It is important to measure the BMI of a woman prior to pregnancy in order to determine the weight that should be gained during pregnancy. Recommended weight gain under normal BMI during pregnancy is: 0.5kg per month for the first trimester A minimum of 1kg to 1.5kg per month in the second and third trimester.
Potential problems with too much or too little weight gain during pregnancy. Women who gain too little weight are at increased risk of having anemia, premature
rupture of membranes, and a low birth weight baby. Women who gain too much weight are at increased risk of premature labor, larger
babies, gestational diabetes, and high blood pressure. It is best to aim for something near the recommended gain shown in the table below.
If the pre-pregnancy weight is known, the ideal increase in weight during pregnancy is as summarized in Table 2:
19

TABLE 2: Recommended Weight Gain for Pregnant Women Based on BMI (kg/m2)
Pre Pregnancy BMI Recommended Gain during Pregnancy Based on Pre-Pregnancy BMI (kg)
Normal (BMI > 18.5 - <25.0) 11.5 – 16.0 Underweight (BMI<18.5) 12.5 – 18.0 Overweight (BMI> 26-27) 7.0 – 11.5 Twin pregnancy 16.0 – 20.5 Obese (BMI ≥ -30.0 ≥6.0 (Adapted from the Institute of Medicine's Nutrition during Pregnancy)
Micronutrient assessment For purposes of this document, micronutrient assessment will focus on iron and folic acid due to the role they play in control of anemia as a major public health concern among women (49% women anemic). Aside from malaria and worm infestation, much of the anemia in Uganda is associated with iron and folate deficiency besides the effects of malaria and worm infestation. The severity of anemia is assessed through amount of hemoglobin levels in the blood, and this will be taken as a proxy indicator of iron and folic acid deficiency besides malaria infection and worm infestation.
Health care providers should counsel women on intake of other of other micronutrients such as iodine and calcium vitamin B12 even without the assessment.
Iron and folic acid Inadequate level of iron in the blood is a major contributor of anemia. The body needs folic acid to make red blood cells (RBC), new genetic material (DNA) in cells and normal development of a fetus. Therefore iron and folic acid deficiency during pregnancy contributes to anemia.
Recommended actions All pregnant women attending ANC should be assessed for anemia using physical, clinical, and/or laboratory tests.
Clinical assessment of anemia Signs and symptoms of anemia to look for in a clinical assessment include: Pallor of mucus membranes Body weakness Easy fatigability Palpitations on exertion
Biochemical assessment of anemia The severity of anemia is determined by Heamoglobin concentration (Table 3).
20

Table 3. Recommended Cut-Offs for Categorizing Anemia in Pregnancy and actions. Category of Anemia
Heamoglobin Levels
Action
Normal >11g/dl Dietary diversification and supplementation Mild 10 - 10.9g/dl Dietary diversification and supplementation Moderate 7 – 9.9g/dl Dietary diversification and supplementation Severe <7g/dl Dietary diversification and treatment for anemia
which may include blood transfusion Source: WHO standards categorizing anemia in pregnancy 2001
Vitamin A Vitamin A is important during pregnancy (embryonic development, mucous membranes, infection resistance, bone growth, fat metabolism). Dietary intake of foods containing vitamin A is preferably recommended. For example carrots, pumpkins, green leafy vegetables, pawpaws, foods fortified with vitamin A like cooking oil and margarines.
Supplementation with vitamin A is NOT recommended because it provides high doses that lead to birth defects and liver toxicity.
Iodine Role of Iodine during pregnancy: Cretinism in children born to mothers with iodine deficiency while pregnant. This
condition is characterized by mental deficiency, stunted growth, hearing, and sight defects.
Enlargement of thyroid gland (goiter) In Uganda the coverage of iodized salt is over 95%. It is therefore recommended that women be counseled to consume iodized salt.
Recommended actions on prevention and control of micronutrient deficiency: To prevent and correct micronutrient deficiency in pregnancy, the Ministry of Health recommends: Supplementation: implementing a supplementation program for iron and folic acid to
prevent anemia. (see annex 2) Nutrition counseling and education: on consumption of iron, folic acid, and vitamin
A rich foods so as to control related deficiencies. Prevention of IDD: Use of iodized salt. Malaria control: this is vital in preventing anemia during pregnancy. Pregnant women
should sleep under ITNs and receive IPT with fansidar (three tablets of fansidar during the 2nd trimester, and three tablets during the 3rd trimester) as directly observed therapy (DOT.)
Deworming: pregnant women should also be given deworming tablets in the second and third trimesters (400mg of albendazole during the 2nd trimester, and 400mg during the 3rd trimester).
21

Consumption of fortified foods: examples include cooking oil fortified with Vitamin A; wheat flour fortified with iron, margarine with Vitamin A and D.
2.2.2. Nutritional requirements of pregnant women
Pregnant women should be encouraged to eat a variety of foods, according to local availability and accessibility, in adequate amounts in order to meet their nutritional requirements. It is particularly important that underweight women increase their energy intake to gain the required weight during pregnancy as recommended in 2.2.1.1 above.
Energy and protein requirements To meet the extra demands needed for growth of the fetus, placenta, and other maternal tissues, extra energy and protein intake during pregnancy is required - especially in the second and third trimesters. In addition to the regular three meals, women should be counseled to eat at least one extra meal (snack) per day to meet the daily energy requirements of pregnancy.
Micronutrient requirements during pregnancy There is increased demand for micronutrients during pregnancy. Their deficiencies increase the risk of maternal morbidity and mortality during the pregnancy, delivery, and postpartum periods. For example, anemia increases the risk of death from postpartum hemorrhage, prolonged labor and sepsis (infections). Addressing maternal micronutrient malnutrition is therefore an important intervention for reducing maternal mortality. Micronutrient status of pregnant women can be improved through diet diversification, micronutrient supplementation, and food fortification.
Table 4. Micronutrient Requirement during Pregnancy and Postpartum Period
NUTRIENT DAILY REQUIREMENTS FOR PREGNANCY/POST
NATAL CARE CONSEQUENCES OF DEFICIENCY
Iron 60mg of elemental iron (200mg of ferrous sulphate) for pregnant women.
(12mg for non-Pregnant
19mg for lactating women)
Increased peri-natal and maternal mortality
Increased risk of pre-term birth and/or low birth weight
Impaired cognitive development Reduced work productivity
Folic Acid 400ųg for pregnant women (180 for non-pregnant and 280 for lactating women)
Risk of infants having neural tube defect. Higher risk of abnormal pregnancy
outcome, including eclampsia, and premature delivery, and birth defects such as Clubfoot and cleft palate.
Iodine 175ųg Goiter
22

(150 for non pregnant and 200 for lactating women)
Cretinism (mental deficiency, deafness, dwarfism.)
Calcium 1200 mg risks of pre-eclampsia Depletes bone stores, rendering the bones
weak and prone to fracture.
2.2.3. Nutrition education/counseling during antenatal care
Pregnant women should be educated to achieve optimal nutritional status during pregnancy. Key nutrition information should be provided on the following issues: Importance of adequate nutrition during pregnancy. Relevancy of appropriate weight gain during pregnancy. Increased nutrient requirements. Nutrient rich dietary sources. Importance of micronutrient supplementation during pregnancy. Guidelines for healthy eating habits. Appropriate food preparation methods. Food safety and hygiene. Avoidance of substance abuse (e.g. alcohol, drugs, smoking). Nutrition precautions in special circumstances such as chronic diseases, medications,
etc.
2.2.4. Common physiological disturbances during pregnancy
Table 5. Common Physical Symptoms during Pregnancy Physiological disturbance
Description Essential Actions
1. Nausea and Vomiting
Associated with hormonal changes Usually occurs during first Trimester, but could continue into second trimester or throughout the pregnancy. Usually more severe in the morning.
Advise on the following: o Counsel mother that nausea will wear
off as pregnancy progresses o Do not take medication unless
prescribed by health worker o Avoid foods that trigger nausea, such as
fried and heavily-spiced foods o Eat small frequent meals o Chew food adequately and eat slowly NB: Encourage women not to avoid eating because adequate nutrition during this period is important for her own health and that of the development of the fetus.
2. Heart-burn This is a burning feeling, which rises from the upper abdomen or lower chest up towards the throat region. Common in the later stages of
Assess the diet of the pregnant women so as to exclude the foods that may be causing the heartburn and advise on the following: o Avoiding, for a while, foods and drinks
that are known to cause heartburn, so 23

pregnancy, due to pressure of the enlarged uterus on the stomach in combination with the relaxed oesophageal sphincter, resulting in occasional regurgitation of stomach contents into the Oesophagus.
as to see if symptoms improve. These include spiced foods, fried foods, alcohol, etc.
o Eating small frequent meals instead of three large meals per day.
o Attention should be given to adequate chewing and eating slowly.
o Eating at least three hours before going to bed to allow for digestion
3. Constipation o Advise pregnant women to take a diet containing plenty of fluid, fruit juice and fiber
o Encourage regular exercises as this can be helpful
o Discourage the use of laxatives o Advise pregnant women on
constipation resulting from use of iron supplementation.
4. Oedema Oedema is the retention of body fluids and usually manifests as swelling of lower limbs.
o Advise pregnant women to rest with legs elevated
o Encourage them to lie on their side while sleeping so that blood flows from the legs back to the heart
o Discourage the use of diuretics in pregnancy
o Advice pregnant women not to reduce salt intake, unless medically recommended.
o Consult with the health worker to rule out other causes of oedema
NB. The body needs enough salt to maintain the balance of fluid.
2.3. Maternal nutrition interventions during postnatal care
Nutritional requirements during postnatal period are greater than during pregnancy due to: The need to produce breast milk The need to promote recovery and sustain the mother’s health Increased physical activity compared to pregnancy
2.3.1. Nutritional assessment of lactating women
The six-week Postnatal Care visit presents an opportunity for assessing nutritional status of these women. Macro nutrient assessment
24

MUAC (Refer to assessment during pregnancy)
Assessment and control of micronutrient deficiencies
Vitamin A Vitamin A supplementation is given to mothers postnatally to increase Vitamin A in breast milk to a level adequate to meet the infant’s requirements, as well as to improve the mother’s immunity.
Night blindness is the first symptom of vitamin A deficiency. Individuals should be asked whether they have difficulty seeing in dim light. Look out for signs of severe vitamin A deficiency like corneal opacity, clouding, Bitot’s spots, and xeropthalmia.
Iron This is to prevent anemia in mothers during lactation/breast feeding. Supplementation with 1 tablet/day (60mg) for 3 months after delivery is recommended in addition to the intake of iron rich foods. (See annex 2)
2.3.3. Nutritional requirements during lactation
Every breastfeeding woman should:
Eat at least 4 meals a day (approximately 650 additional calories), to meet the energy needs of lactation ensuring variety of the 3 food groups: o Body-building foods: beef, fish, eggs, meat, liver, lean beef, pork, fish and legumes o Energy giving foods: mainly cereal foods, tubers, o Micronutrient-rich foods: fruits such as passion fruits, paw-paws, pineapples,
guava, avocado, mango, pumpkin and vegetables like spinach, dodo, nakati, buga, sukuma wiki, tomatoes, etc. Fortified foods to improve micronutrient intake (oil e.g. fortified with Vitamin A,
Take a dose of (200,000 IU) of Vitamin A immediately after delivery or within the 1 st
eight weeks after delivery. Take iron (60mg) and folic acid 400µg daily for 3months. Take iodized salt Be counseled on:
o Uptake of family planning services and timing and spacing of pregnancies o Importance of exclusive breastfeeding o Appropriate infant and young child feeding, growth monitoring and promotion.
25

3. MATERNAL NUTRITION UNDER SPECIAL CIRCUMSTANCES
3.1 Diseases
The nutritional status of pregnant women is undermined by the presence of communicable and non-communicable diseases. The common diseases affecting pregnant women and pregnancy outcomes are outlined in the table below:
Table 6: Common Diseases Affecting Pregnant Women and Pregnancy Outcomes Illness Risk Factors Essential Actions Hypertension Family history (genetic
factors) Obesity Lack of regular physical
activity Poor nutrition especially
low calcium intake. Stress
Monitor the condition regularly. Encourage women to maintain a healthy
diet during pregnancy Advise on increasing exercise Advise on reducing intake of table salt Advice on increasing calcium intake. Discourage the use of alcohol
Diabetes Family history Eating small, regular meals helps control Mellitus (DM) Obesity weight and glucose levels. In some cases, Sedentary life style Eating a variety of foods will help maintain diabetes develops May be drug induced adequate nutrition. during pregnancy Moderate exercise for 30 minutes or (pregnancy induced more on most days of the week. diabetes) and is as a Eat low fat foods. result of glucose Encourage consumption of carbohydrate intolerance. foods that contain dietary fiber (e.g. fruits,
vegetables, whole wheat bread, cereals, brown rice, legumes).
Avoid smoking. Avoid alcohol intake.
Sickle cell Anemia Family history of sickle cell disease
Appropriate care and nutrition education for sickle cell patients should be ensured i.e. a healthy diet (providing zinc, vitamin E, vitamin C, vitamin A, vitamin B6, and vitamin B12, folic acid supplements and prevention of dehydration.
All sicklers should receive preventive doses of anti-malarials.
More frequent prenatal visits allow for close monitoring of the mother and of fetal well-being.
Counsel on using family planning.
26

Caution should be taken in prescribing iron, and refer for appropriate management.
Give appropriate dose of folic acid.
Malaria Stagnant polluted water and large mosquito population near living environment
Lack of ITN
All pregnant women should be given a preventive doze of anti-malarials and when diagnosed with malaria managed according to the current national malaria protocols.
Sleep under a long-lasting, insecticide treated nets.
Increase fluid intake including water. Small frequent meals of wide variety in
case of low appetite and vomiting. Continued intake of iron and folic acid
supplements. HIV/AIDS HIV/AIDS puts extra demands for energy and nutrients and adds to those already imposed by pregnancy and lactation
Unprotected sex with infected partners/a person of unknown sero-status
Multiple sexual partners Transfusion with
unscreened blood Use of unsterilized
equipment Sharing of syringes and
needles and razor blades
To preserve their health and nutritional status HIV positive pregnant and lactating women should eat at least 2 nutritious snacks in addition to the regular 3 meals to meet their energy and nutrient needs.
Support pregnant women and lactating mothers to seek, early treatment of HIV.
Regularly monitor the nutritional status of pregnant and lactating mothers.
Prevent and treat all opportunistic infections/illness that may affect their nutritional status or their ability to eat.
Encourage good food safety and hygiene practices to avoid food and water-borne diseases.
Source: Guidelines for service providers on Nutritional care and support for People Living with HIV and AIDS, in Uganda (May, 2006).
3.2. Social factors, local practices, and environmental issues affecting maternal nutrition
3.2.1. Child spacing
Encourage the use of family planning to ensure healthy timing and spacing of pregnancies.
Recommended actions Support mothers to initiate breastfeeding within the first hour after birth and exclusively
breastfeed for six months, as this constitutes a form of natural contraception. 27

Counsel on the need for birth spacing through promotion of other appropriate family planning methods in order to allow the body to regain nutrient stores4 .
Promote safe sex practices Counsel on inter-pregnancy interval of 3-5 years
3.2.2. Myths, local practices, and gender issues that affect maternal nutrition
Myths and local practices and gender issues influence food habits and may negatively impact on the nutrition status of women because most of them prohibited foods are usually protein-rich.
Recommended actions Health care providers should be able to overcome myths by using the following suggested actions: Be conversant about local practices pertaining to nutrition that have a negative impact
on women’s nutrition in the areas where they work. Counsel both men and women on how to adapt local practices so that women receive
adequate nutrition Raise the awareness of communities on appropriate nutritional interventions for women
during pregnancy and lactation, and as to the influence of local practices on nutrition. Health care providers should counsel families to involve men, within the cultural context, to support nutritional interventions.
Educate communities on the need for reduced workload and enough rest for pregnant and lactating women
Health workers should dispel myths about food taboos that affect women from�accessing highly nutritious foods like fish, meat, eggs, etc.�
Educate families and counsel adolescents on the physical and emotional dangers of early marriages and childbearing.
3.2.3. Substance abuse
Substance abuse is the excessive use of a potentially addictive substance such as alcohol, tobacco, and drugs (marijuana, qat, cannabis, cocaine, etc) that may modify body functions.
Substance abuse has the following effects on maternal nutrition: o Suppressing the woman’s appetite, leading to reduced food intake which is one
of the major immediate causes of malnutrition. o In the case of lactating mothers, the substances can pass through breast milk and
affect the baby’s health. o Drugs can have a direct effect on the mother’s health when they cause illnesses
eg lung and liver cancer from tobacco and alcohol respectively. Illnesses negatively affect maternal nutrition.
4 Consider breastfeeding status when prescribing contraception.
28

Recommended actions All forms of substance abuse should be avoided and discouraged in pregnancy and
lactation.
3.2.4. Maternal nutrition in emergencies
Hunger and malnutrition are rampant in incidences of emergencies. Women of reproductive age, and pregnant and lactating mothers in particular, are more vulnerable to malnutrition in these settings. Besides wasting, deficiencies of iodine, vitamin A and iron are common in emergency-affected populations. In Uganda humanitarian agencies support government in general provision of food aid.
Recommended actions In cases of emergency, humanitarian aid programs should prioritize vulnerable groups
like pregnant and lactating women and meet their energy and other nutrient needs through the rations that are usually served.
Routine iron and folic acid supplementation should still remain priority to pregnant and lactating mothers despite the emergence situations.
3.2.5. Nutritional care for adolescent pregnancy
The proportion of adolescent pregnancies in Uganda stands at 25% of the age bracket 10 – 19 years. The nutritional needs of pregnant adolescents are similar to those of other mothers. However, because their bodies are still developing, younger adolescents compete with the fetus for nourishment, exha usting iron and other nutrient reserves. As a result, nutritional deficiencies such as iron deficiency anemia are more common in pregnant adolescents.
Recommended actions Health workers should ensure that they; Assess the nutritional status of these adolescents. Counsel and provide appropriate advice/information to the supporting families on
adequate nutrition and eating behaviors of the adolescent. Counsel on compliance and intake of micronutrient supplements according to national
protocols.
3.2.6. Community support for maternal nutrition
In order to establish a social environment conducive to optimal maternal nutrition, the following actions are recommended: Utilize the referral system using of the Village Health Teams (VHTs) linking to the
established health care system. Supportive social networks through the VHTs (e.g. family support groups, women
groups for improved nutrition). Effective referrals with other agencies that can help to improve household food security
and uptake of preventive health services (e.g. antenatal care, adolescent-friendly health services, nutritional information, micronutrient supplementation, etc.).
Provision of nutrition education and counseling to ensure proper utilization, preparation and storage of foods.
29

3.2.7. Water, sanitation, and hygiene
One of the major causes of malnutrition in an individual is the presence of disease. Poor sanitation and the use or consumption of unsafe or contaminated water is usually the primary source of diseases related to environmental hygiene. Food and water should be handled in a hygienic manner in order to avoid food and water-borne illnesses. Pregnant women’s immune systems are weaker, and thus they are susceptible to infection.
Recommended actions Always wash hands with soap before and after touching food. Wash fruits and vegetables thoroughly before eating. Make sure that food preparation and eating areas are perfectly clean. Cover food that is not eaten to avoid contamination. Serve cooked foods when hot. Serve foods using clean utensils. Water meant for drinking should be brought to a rolling (bubbling) boil and boiled for 3
minutes to kill germs. Avoid consuming expired processed food products by checking on the “best before”
dates.
30

4. IMPLEMENTATION
Implementation should be effected at all levels and the strategies should be integrated in the existing maternal health care services such as Goal-oriented ANC, maternity, postnatal care (PNC), baby-friendly health facility initiative (BFHI), prevention of maternal to child transmission (PMTCT) of HIV, FP, YCC, etc.
Table 7: Implementation of the Maternal Nutrition Interventions. Intervention Activities Level Responsibilit
y Target
Macronutrient deficiency control
Education and counseling on diet diversification, amounts and frequencies of meals
Health facility and community
Health care providers at facility and community.
All women of reproductive age.
Micronutrient deficiency control
Supplementation with iron and folic acid during pre pregnancy, pregnancy and lactation.
Vitamin A within 8 weeks after delivery.
Education and counseling on diet diversification
Health facility and community, including schools
Health care providers.
Adolescent girls Pregnant and lactating women.
Deworming. Malaria control using
ITN and IPT2.
Health facility, community
Health care providers, VHTs
Pregnant and lactating women.
Promote availability and use of Fortified foods:
All levels MOH, DHT, Community leaders
Women of reproductive age.
Nutritional assessments
Anthropometry Clinical and
biochemical assessments
Health facility and community.
Health care providers
Women of reproductive age.
Nutrition promotion and education
Production and dissemination of IEC materials, Job Aids and Protocols.
National and District
MOH, partners and DHT
Health care providers
Nutrition counseling
Health education talks All levels MOH and DHT
Women of reproductive age.
31

Intervention Activities Level Responsibilit y
Target
Community Home visits Districts and DHT Women of mobilization and Community meetings Community VHT reproductive sensitization Media programs
Linkages to social support groups.eg to health facilities, income generating activities and women support groups.
age.
Partnerships/ Review and report District and MOH Partner Inter-sectoral sharing meetings National organizations collaboration Joint implementation partners and Networking of prioritized
activities Capacity building Provide adequate
Staffing Orientation of service providers.
Introduce Maternal nutrition as part of the pre-service training for teachers and health workers
National and District
MOH and DHT
Health care providers
Provision of adequate equipment and tools.
National and District
MOH and DHT
Service delivery points.
Logistics and Accurate and reliable National, MOH, DHT Service supplies Quantification district and and health delivery management Procurement
Storage and distribution system developed.
health facility facility. points.
Policy aspects Maternal nutrition be integrated in RCT, Goal oriented ANC, PMTCT, and Family planning services
National, district and health facility
MOH, DHT and health facility.
Service delivery points.
Monitoring and Review data collection, National MOH Districts and Evaluation support supervision and
reporting tools for maternal nutrition
health facilities
32

Intervention Activities Level Responsibilit y
Target
Provide data collection and reporting tools
National Districts
MOH, DHT Districts and health facilities
Support quality data collection, analysis and timely reporting and use.
National Districts
MOH, DHT Districts and health facilities
Advocacy Resource mobilization, Publicity and awareness creation for maternal nutrition
National and district
MOH, DHT Leaders at all levels.
33

5. MONITORING AND EVALUATION
Monitoring and evaluation should be done for both process and outcome indicators to ensure that the implementation of the guidelines is being followed to achieve the desired result. The District Health Team Leader will be responsible for collection, compilation and report making using the existing data management structures of the health system. Indicators to be monitored:
Number of pregnant women receiving 30+ iron supplements per visit through facility Number of lactating women receiving 30+ iron supplements per visit through facility Proportion of women consuming at 90+ IFA tablets in the course of pregnancy through
special surveys and DHS Number of pregnant women weighed at fourth visit (approximately at 32 weeks of
gestation) through health facility.
Channels of collection Channels of data collection will be through established structures like health information
management service (HIMS) data collecting registers and reports, and special surveys and UDHS.
Integrated Registers for ANC, Maternity, PNC, family planning (FP) and PMTCT
34

ANNEX I: Counseling Job aid for Health Workers on Prevention and Control of Anemia
Health worker’s expected actions (In all these actions, health worker listens, builds confidence in the woman, respects, and is courteous so that pregnant woman will feel comfortable in returning for another visit)
Use “GATHER” method to counsel women (Greet, Ask, Tell, Help, Explain, and Reassure) Greet: Greets the pregnant woman and praises woman and family members for coming. Ask: Asks pregnant woman if she has any difficulties or concerns and Tell: Responds to her based on the identified problems or concerns. Help: (offer practical help) o If mother presents with danger signs, refers to health facility immediately o If mother presents with malaria, provides treatment o Assesses for anemia (pallor), ot her illnesses, HIV and Immunization status, and
infant feeding options. o If anemic (pallor) provides higher dose of iron (ferrous sulphate)/folate (folic acid)
and refers to a well equipped health facility for further management. o If not anemic, provides 30 tablets of Iron/Folic Acid and counsels on benefits,
compliance, managing side-effects and safety (see protocols behind): o Provide a dose of Fansidar IPT for malaria by DOT (see protocols) o Provide a single dose of Albendazole/Mebendazole by DOT (see protocols) o Advises on foods rich in iron, importance of future antenatal visits, any treatment
needed and 2-week follow- up if anemic o Advises on sleeping under a treated mosquito net to protect her and her unborn
child o Advise on nutrition for pregnant mother and on successful breastfeeding. o Offer other services such as family planning counseling.
Explain: Discusses with mother the effects of anemia and need for compliance i.e. - Effects of anemia on the mother – increased risk of maternal death during
pregnancy and delivery - Effects of anemia on the unborn baby – permanent brain damage, very weak and
danger of death (low bi rth weight) Reassure: Makes an appointment and counsels for follow-up visit to ensure that
unborn child and mother are safe & collect medicines.
35

AN
NE
X 2
: Pro
toco
ls f
or
Inte
rven
tio
ns
to P
reve
nt a
nd/
or
Tre
at M
ater
nal
An
emia
Med
icin
e/S
upp
lem
ent
Do
sage
S
ide
Eff
ects
M
anag
emen
t F
erro
us
sulp
hat
e p
lus
Fo
lic a
cid
(T
o bo
ost
bloo
d fo
rmat
ion)
Pr
ophy
laxi
s: Fe
rrou
s su
lpha
te 2
00m
g or
ele
men
tal i
ron
60m
g an
d fo
lic a
cid
400µ
gdai
ly fo
r 6
mon
ths
of p
regn
ancy
(1
80 t
able
ts) a
nd 3
mon
ths
(90
tabl
ets)
afte
r de
liver
y O
r
Com
bine
d Ir
on 1
50m
g w
ith F
olic
aci
d 0.
5mg
daily
for
6 m
onth
s of
pre
gnan
cy (
180
tabl
ets)
and
3 m
onth
s (9
0 ta
blet
s) a
fter
deliv
ery.
Tre
atm
ent:
Mod
erat
e an
emia
(H
b 7
– 10
.9g/
dl)
Iron
60m
g tw
ice
daily
for
two
wee
ks a
nd r
ever
t to
no
rmal
pro
phyl
axis
dos
e.
Folic
aci
d 40
0µg
twic
e da
ily fo
r 2w
eeks
.
Tre
atm
ent
for
seve
re a
nem
ia:
o
60m
g ir
on
tw
ice
dai
ly f
or
3mo
nth
s an
d
folic
aci
d 8
00 µ
g da
ily fo
r 3
mon
ths.
The
n re
vert
to
norm
al p
roph
ylax
is d
osag
e.
Blac
k st
ools,
con
stip
atio
n,
abdo
min
al p
ain
and
naus
ea. T
hese
are
not
da
nger
ous.
The
y ar
e te
mpo
rary
.
Cou
nsel
mot
her
on im
port
ance
of
com
plia
nce
with
full
trea
tmen
t.
How
to
min
imiz
e sid
e ef
fect
s: by
ta
king
bef
ore
bed,
afte
r m
eals,
ea
t m
ore
frui
ts a
nd v
eget
able
s, w
hole
gra
ins.
Con
sum
e vi
tam
in
C r
ich
frui
ts a
nd v
eget
able
s, an
d no
tea
or
coffe
e w
ithin
1 h
our
befo
re o
r af
ter
mea
ls
Fan
sid
ar/S
P
(IPT
for
Mal
aria
)
3 ta
blet
s sin
gle
dose
dur
ing
2nd
trim
este
r (4
-6m
onth
s)
and
3rd
trim
este
r (7
-9m
onth
s) b
y D
irec
tly O
bser
ved
The
rapy
(DO
T) a
t le
ast
one
mon
th a
part
. N
ote
D
elay
inta
ke o
f fol
ic a
cid
or c
ombi
ned
Iron
/folic
aci
d ta
blet
s fo
r 1
wee
k af
ter
adm
inist
ratio
n of
fans
idar
be
caus
e fo
lic a
cid
inte
rfer
es w
ith t
he e
ffect
of f
ansid
ar
Do
not
give
fans
idar
in t
he fi
rst
trim
este
r (fi
rst
3 m
onth
s).
Nau
sea
and
vom
iting
A
bdom
inal
pai
n T
hese
are
not
dan
gero
us.
Cou
nsel
mot
her
on c
ompl
ianc
e w
ith t
he t
reat
men
t. G
ive
it by
DO
T
Alb
end
azo
le/M
eben
daz
o
le
(Pre
vent
ive
trea
tmen
t fo
r w
orm
infe
stat
ions
)
A
lben
dazo
le 4
00 m
g as
a s
ingl
e do
se (a
t 1s
t co
ntac
t bu
t no
t in
the
1st
tri
mes
ter)
O
r
Meb
enda
zole
500
mg
as a
sin
gle
dose
(at
1st
cont
act
but
not
in t
he 1
st t
rim
este
r)
Nau
sea
and
vom
iting
T
hese
are
not
dan
gero
us.
Cou
nsel
mot
her
on c
ompl
ianc
e w
ith t
he t
reat
men
t. G
ive
it by
DO
T
36

- - -
These guidelines are made possible by the generous support of the American people through the United States Agency for International Development (USAID) under the terms of Cooperative Agreement No. GHS A 00-05-00012 00. The contents of this guidelines document are however, the responsibility of the Ministry of Health of the Government of Uganda.
37