GUIDELINES FOR USING PANTOPRAZOLE HUSM flow chart... · GUIDELINES FOR USING PANTOPRAZOLE HUSM...
58
GUIDELINES FOR USING PANTOPRAZOLE HUSM Upper GIT bleed Mucosal break lesion Treatment Prophylatic/suspected Upper GIT bleed confirm IV Pantoprazole 40 mg BD Chronic Acute T. Pantoprazole 40 mg BD –6/52 IV Pantoprazole 80 mg stat then IV Pantoprazole 80 mg/hour for 72 hour then IV Pantoprazole 40 mg BD for 7/7 then T. Pantoprazole 40 mg BD –6/52 OGDS Maintenance T. Pantoprazole 40 mg OD - 3-6/12 therapy If not properly heal 1
Transcript of GUIDELINES FOR USING PANTOPRAZOLE HUSM flow chart... · GUIDELINES FOR USING PANTOPRAZOLE HUSM...

GUIDELINES FOR USING PANTOPRAZOLE HUSM
Upper GIT bleed
Mucosal break lesion
Treatment
Prophylatic/suspected
Upper GIT bleed confirm
IV Pantoprazole 40 mg BD
Chronic Acute
T. Pantoprazole 40 mg BD –6/52 IV Pantoprazole 80 mg stat then IV Pantoprazole 80 mg/hour for 72 hour then IV Pantoprazole 40 mg BD for 7/7 then T. Pantoprazole 40 mg BD –6/52
OGDS
Maintenance T. Pantoprazole 40 mg OD - 3-6/12 therapy
If not properly heal
1

FLOW CHART USAGE OF PPI IN HUSM ENDOSCOPY MEETING ON 4/10/07
Bleeding cases (Non variceal bleed) 1st Endoscopic procedure, then 2nd Proton pump inhibitor, then 3rd Mucosal protective therapy, then 4th I/V Somatostatin analog 25 mg/hr 1 kg, then 5th Surgival intervention PPI 1st line I/V Pantoprazole 80 mg stat, then I/V Pantoprazole 8 mg/hr for 3 – 5/7, then I/V Pantoprazole 40 mg BD Follow-up by t.Pantoprazole 40 mg BD – 8 – 12/52 and to repeat endoscopy if rebleed or after complete treatment. I/V Esomeprazole can be used as second choice. Mucosal break lesion (Prophylaxis) 1st line I/V Esomeprazole 40 mg BD or 2nd line I/V Pantoprazole 40 mg BD or 3rd line I/V Ranitidine or Tablet 4th line Mucosal protection agent (Sulcalfate) Peptic Ulser disease (PUD) 1st line Tab. Lansoprazole 30 mg OD/BD, then 2nd line Tab. Esomeprazole 40 mg OD/BD, then 3rd line Tab. Pantoprazole 40 mg OD/BD, then 4th line Tab. Rabeprazole 20 mg OD/BD, then 5th line Tab. Omeprazole 40 mg OD/BD, then 6th line Tab. Ranitidine 150 mg OD/BD, then 7th line Tab. Cimetidine 300 g OD
2

In cases of PUD (No. OGDS) (No. PPI test)
with T. Ganaton 50 mg BD/TDS 1st line T. Lansoprazole 30 mg OD/BD 2nd line T. Esomeprazole 40 mg OD/BD If not improve after 2/52 refer results endoscopy investigation (Gastro/Surgical) In cases of no OGDS for PPI test 1st line T. Lansoprazole 30 mg BD – 2/52 then decision OR 2nd line T. Esomeprazole 40 mg BD – 2/52 then decision. In Cases of Biliary gastritis/recurrent GERD/GERD (Gastrooesophageal disease)
1) T. Ganaton 50 mg BD/TDS with } 1st line T. Esomeprazole 40 mg BD/TDS }
2) T. Ganaton 50 mg BD/TDS with } 2 nd line T. Rabeprazole 20 mg BD }
In Cases of PUD with normal OGDS/NERD (non erosive gastritis) T. Ganaton 50 mg BD/TDS WITH 1st line Esomeprazole 40 mg OD/BD 2 nd line T. Lansoprazole 30 mg OD/BDs 3 rd line T. Pantoprazole 40 mg OD/BD 4th line T. Rabeprazole 20 mg OD/BD
3

LIPID LOWERING THERAPY USM GUIDELINES
Indications for use
1. Coronary heart disease (CHD) 2. CHD disease equivalent
a) Diabetes Mellitus b) Carotid artery disease c) Peripheral artery disease d) Abdominal aortic aneurysm
3. Familial hyperlipidaemia (or total chol > 8, LDL chol > 6) 4. CHD high risk individuals
a) Individuals with 2 or more risk factors 5. CHD low risk
a) Individuals with less than 2 risk factors 6. If asymptomatic but total cholesterol ≥ 5.0 mmol/l, LDL cholesterol ≥ 3.0
mmol/l and total CVD risk of projected CVD risk at 60 years of age is ≥ 5%. 7. Others
a) Individuals with chronic renal disease (Creatinine > 133 umol/L or GFR < 60 ml/min/1.73 m2)
b) Metabolic syndrome Drug Dose range LDL reduction Cost for 1/12 rx
( mg ) RM Pravastatin 10 - 40 19 – 40 % Simvastatin 10 - 80 28 - 48 % Lovastatin 20 - 80 29 – 48 % Atorvastatin 10 - 80 38 – 54 % Rosuvastatin 10 - 40 52 – 63 %
4

Indications 1-4
• Aggressive lipid lowering therapy required • High dose and high potency drug required • Suggestion
1. Coronary heart disease (CHD) 2. CHD disease equivalent i) Diabetes Mellitus ii) Carotid artery disease iii) Peripheral artery disease iv) Abdominal aortic aneurysm 3. Familial hyperlipidaemia (or total chol > 8, LDL, chol >6) 4. CHD high risk individuals- Individuals with 2 or more
Check FLP Start atorvastatin
10 – 20 mg od TLC
Check FLP after 3/12
Total C > 4.5 or Total C < 4.5 or LDL > 2.5 LDL < 2.5
Intensification of Rx Continue medication or consider de-escalation of Rx ie change to Simvastatin or Pravastatin as per indicated
Increase dose of Atovarstatin or change to Rosuvastatin
TLC
TLC = Therapeutic lifestyle changes
5
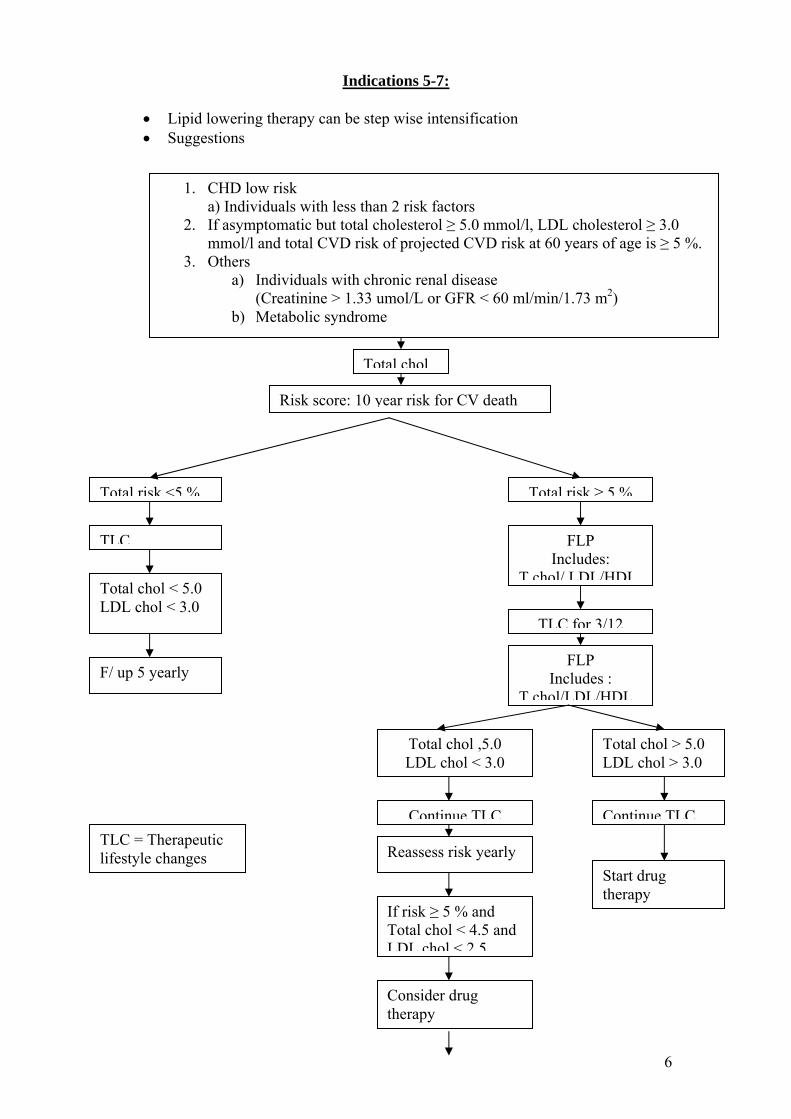
Indications 5-7:
• Lipid lowering therapy can be step wise intensification • Suggestions
6
1. CHD low risk a) Individuals with less than 2 risk factors
2. If asymptomatic but total cholesterol ≥ 5.0 mmol/l, LDL cholesterol ≥ 3.0 mmol/l and total CVD risk of projected CVD risk at 60 years of age is ≥ 5 %.
3. Others a) Individuals with chronic renal disease
(Creatinine > 1.33 umol/L or GFR < 60 ml/min/1.73 m2) b) Metabolic syndrome
Total chol
Risk score: 10 year risk for CV death
Total risk <5 % Total risk ≥ 5 %
TLC FLP Includes:
T chol/ LDL/HDLTotal chol < 5.0 LDL chol < 3.0
F/ up 5 yearly
TLC for 3/12
FLP Includes :
T chol/LDL/HDL
Total chol ,5.0 LDL chol < 3.0
Total chol > 5.0 LDL chol > 3.0
Continue TLC Continue TLC
Reassess risk yearly Start drug therapy
If risk ≥ 5 % and Total chol < 4.5 and LDL chol < 2 5
TLC = Therapeutic lifestyle changes
Consider drug therapy

Drug therapy indicated
Total chol 5.0 – 5.9 Total chol 6.0 – 6.9 Total chol 7.0 LDL chol 2.5 – 3.5 LDL chol 3.5- 4.5 LDL chol 4.5
Pravastatin or Simvastatin or Atorvatatin or
rosuvastatin simvastatin atorvastatin If targets not achieved : Total chol > 4.5 or LDL > 2.5 CHECK COMPLIANCE TO TLC AND DRUG THERAPY
Consider intensifying treatment
Combination therapy Simvastatin Ezetimide Atorvastatin
Or Or Atorvastatin Rosuvastatin
Or And or Rosuvastatin Ezetimibe
And or Fibrates etc
Prepared by Dr Tee Meng Hun & AP Dr Zulkurnai Yusof, Med Dept
7

Indication of Using Amlodipine (and ± Felodipine) in HUSM (suggestion) 1. Introduction Calcium channel blockers work by blocking the initial calcium influx into myocytes and vascular smooth muscle cells. Amlodipine and felodipine are long acting second generation dihydropyridine that have vascular smooth muscle relaxing activity with no or minimal negative inotropic effects. They have a greater selectivity for vascular smooth muscle compared to the myocardium. They vasodilate coronary arteries reduce coronary resistance, increase coronary blood flow and may enhance the development of coronary collaterals. 2.Indication of using calcium channel blocker (CCB) 2a. The use of CCB as anti-ischemic agent -calcium channel blocker has been shown to exert anti-angina properties in various ways such as reduction in heart rate, reduction in contractility, reduction in afterload and direct vasodilatation. -calcium channel blocker should be considered if there are contraindications or adverse reactions to either beta blockers of nitrates or if symptoms are not well controlled with a combination of these agents. 2b.The use in acute coronary syndrome (ACS) patients. - The potential benefits of either amlodipine or felodipine in acute MI has not been examined directly. - Amlodipine is often used in patients with acute MI when hypertension is not adequately controlled by other therapy of proven benefit (beta blockers and ACE inhibitors ). - Study in stable coronary heart disease (PREVENT trial) found no or little benefit of amlodipine but also has no harm. - Therefore amlodipine is not indicated as first line therapy on ACS patients unlike ACE inhibitors and beta blockers. 2c. The use of CCB in patients with heart failure - The potential benefit of either amlodipine or felodipine in acute MI has not been examined directly. However, clinical trial that have evaluated these drugs in heart failure (V- HeFT III and the PRAISE trials) found no or little benefit but also no harm. - In patient with heart failure, amlodipine in at a drug choice as compared to ACE inhibitors, beta blockers and aldosterone antagonist.
8

2d.The use of CCB in hypertension patients. - Although recommendations for initiating medical therapy in essential hypertension have been proposed, there is no uniform agreement on which antihypertensive agent should be given as initial therapy. A variety of different classes of drugs can be used in this setting. These include the thiazide diuretics, beta blockers, angiotensin converting enzyme (ACE) inhibitors, angiotensin II receptor blockers and calcium channel blockers. - There have been limited data as to whether different antihypertensive drugs have variable effects upon patient outcomes, particularly cardiovascular morbidity and mortality. However, an increasing number of trials have provided evidence that at the same level of blood pressure control, most antihypertensive drugs provide the same degree of cardiovascular protection provided there are no other compelling indications. - The choice of drug should be based on the patient’s individual risk profile and the tolerability of the drugs. - “First-line” drugs should have the following properties : 1. reduce long-term morbidity and mortality 2. high efficacy of once-daily administration 3. no adverse effects on concomitant risk factor 4. good tolerability - based on JNC VII guidelines, hypertensive naïve patient should receive diuretics as first line drug. 2e. The use of CCB in anti-arrythmic agents -the use of amlodipine as anti- arrythmic agents therapy was not well studied unlike verapamil and diltiazem, therefore it is not recommended as anti-arrythmic therapy. 2f. The use of CCB in patients with renal disease/nephropathy - Hypertension is common in chronic renal disease and is risk factor for progression of renal damage, and reduction of blood pressure (BP) is an efficient way of preventing or slowing the progression of this damage. BP – lowering effects are common to all antihypertensive drugs, but intra-renal effects differ between classes and between individual drugs within certain classes. Angiotensin – converting enzyme (ACE) inhibitors and angiotensin receptors blockers (ARB) have beneficial effects on proteinuria and declining renal function that appear to be mediated by factors additional to their effects on BP. These RAS inhibitors are recommended as first-line antihypertensive approach in patients with chronic kidney disease. - Calcium channel antagonist are highly a heterogenous class of compounds, and it appears that some agents are more suitable for use in patients with chronic renal disease than others. Most common calcium channel blockers are nondihydropyridine group like verapamil and diltiazem. - Dihydropyridine calcium channel blockers (eg nifedipine and amlodipine) may worsen proteinuria and accelerate the progression of disease in patients with nondiabetic or diabetic nephropathy.
9

2g. The use of CCB in peripheral vascular disease (PVD) patient.
- Unlike verapamil, the use of amlodipine and felodipine in treating peripheral vascular disease patients are not well studied. Therefore, it is not recommended to use these drugs to treat PVD patients.
2h. The use of CCB in Pulmonary Artery Hypertension patients.
- The oral vasodilators of choice are the calcium channel blockers nifedipine and diltiazem. Verapamil is not recommended, since it tends to posses significant negative inotropic properties.
- Amlodipine has been a useful alternative for patients who are intolerant of the other agents (eg. Because of edema, bradycardia, tachycardia, or hypotension)
- The use of Felodipine in pulmonary artery hypertension is not well studied. 3. Advantages of Amlodipine (and felodipine) above other antihypertensive. 3a.Single daily dose, therefore this will improve patient compliance. 3b. No need for renal function monitoring. 3c. Among the least side effects compared to other anti-hypertensive. 3d. In comparison between amlodipine and felodipine, on of the retrospective study has shown that amlodipine has better patient’s adherence compared to felodipine. 4. Disadvantages of CCB above other antihypertensive. 4a. The potential benefit of either amlodipine or felodipine in ACS has not been examined directly in ACS patients. A systematic analysis of all randomized calcium blocker trials in unstable angina suggests calcium channel blockers that as a class do not prevent the development of acute myocardial infarction or reduce mortality, and it also has no harm to these group of patients. 4b. Short-acting CCB (i.e. Nifedipine) has a relatively high incidence of adverse side effects, including peripheral edema (not related to heart failure), flushing, headaches, and lightheadedness, which is due to peripheral vasodilatation. 4c. There was a study (cross sectional) showed that there was a higher rate of depression among hypertensive patients who were on calcium channel blocker as compared to other anti-hypertensive. 4d. Both amlodipine and felodipine are long acting calcium channel blockers, therefore it is not recommended as first line therapy for hypertensive urgency.
10

List of Tables Table 1 Comparative pharmacokinetics of selected dihydropyridine calcium channel antagonists
Nifedipine Nisoldipine Felodipine Amlodipine Diodipine >90 Oral absorption >90 >90 >90 >90
Oral bioavailability
30-50 5-15 10-25 60-65 5-15
Elimination half-life
3-5 4-10 2-8 35-50 3-15
Table-Dosing and costs of the Calcium Channel Blockers Drug Initial Dose Usual Dosage Range Cost x 30 days Verapamil - regular (Isoptia® generic) 80mg TID 80-160 mg TID $37.33-$68.15 - long acting (Isoptin SR®) 180 mg
daily 120 mg daily-240mg BID
$37.52-$99.94 (Varelan®) $32.87-$85.92
180 mg daily
120-480 mg daily
Diltiazem - regular (Cardizem®
generic) 30mg TID 30mg TID-90 mg QID $28.51- $83.61 60 mg BID 60-80 mg BID $51.63- $126.31**
- long acting (Cardizem SR
120 mg daily
120 mg-300mg daily $47.12- $95.89 ®)**
(Cardizem CD®) Felodipine (Plendil®, Renedil
5mg daily 2.5-20 mg daily $23.13-$83.61 ®)
Nifedipine - regular capsules
(Adalat10mg TID 10mg TID-30 mg QID $27.25-$89.52
®generic) 10 mg BID 10-40mg BID $37.90-$104.72** - long acting (Adalat PA®)** 30 mg daily 30-120 mg daily $37.81-$104.72
® (Adalt XL ) 5 mg daily 5-10 mg daily $46.14-$65.34 Amlodipine (Norvasc®) 10mg TID 20-40 mg TID $62.04-$117.58
®Nicardipine (Cardene ) **Base on wholesale acquisition cost Feb. 1995 of least expensive product and professional fee of $6.50 as April 1, 1995. Pharmcare no longer covers Cardizem SR and Adalat PA
11

5. References
1. Antiischemic Agents in the Management of Unstable Angina and Acute Non-ST Elevation (Non-Q Wave) Myocardial Infarction. Michael Simons, MD. Up to date version 13.3
2. Calcium Channel Blockers in Acute Myocardial Infarction. Robert S
Rosenson, MD Harold L Keneddy, MD, MPH. Up to date version 13.3.
3. Calcium Channel Blockers in the Management of Stable Angina Pectoris. Joseph P. Kannam, MD. Julian M Aroesty, MD. Bernard J Gersh, MB, ChB, DPhil, FRCP. UpToDate version 13.3.
4. Choice of Therapy in Essential Hypertension: Clinical Trials. Norman M
Kaplan, MD, Burton D Rose, MD. UpToDate version 13.3.
5. Wenzel, Rene R. Renal Protection in Hypertensive Patients: Selection of Antihypertensive Therapy. (Review). Dugs. 65 (Suppl 2):29-39, 2005.
6. JNC VII guidelines. 7. Medical Management of Claudication. UpToDate version 13.3.
8. Non Diabetic Kidney Disease (Andrew S) N Engl J Med. VOl 347. No 19.
November 7, 2002. 9. Nephropathy in Patient with Type 2 Diabetes. Remuzzi et al. N Engl J Med.
Vol. 346, No. 15 April 11, 2002.
10. Adherence to Calcium Channel Blocker Therapy in Older Adults: A Comparison of Amlodipine and Felodipine. Menzin J et al. J Int Med Res. 2004 May-June; 32(3) :233-9.
12

13
FLOW CHART
Diagnosis of hypertension
Initiate lifestyle modification
If still not achieve BP target (<140/90 mmHg or <130/80 mmHg for those with diabetes or chronic kidney disease)
Initiate drug of choice
Without compelling indication With compelling indication
Stage I Hypertension BP(140-159/90-99) Thiazide is a first choice. May consider ACEI/ARB/BB/CCB or combination. If CCB is used amlodipine is preferred due to good blood pressure control compared to felodipine. If cost is an issue, felodipine can be used instead of amlodipine. If patient has side-effects to amlodipine such as headache, postural hypotension, changed to felodipine is justified.
Stage 2 hypertension (SBP > 160 or DBP >100mmHg) –consider 2 drugs
Use appropriate anti-hypertensive agent

PROPOSAL
GUIDELINES ON PLAVIX PRESCRIPTION FOR CARDIOLOGY PATIENTS HUSM
ACUTE CORONARY SYNDROME
PERCUTANEOUS CORONARY INTERVENTION
(PCI)
INTRACEPT ASD CLOSURE DEVICE
CABG
• NSTEMI/UA = 9 months • Bare metal stent = 3-4 weeks
• Plavix x 3 months • No indication • STEMI = 8 days
• Drug eluting stent (DES) = 6-12 months
* Contraindication for aspirin, ticlopidine is a substitution
14

PROTOCOL NOVOSEVEN OR RECOMBINANT FACTOR 7 FOR JABATAN NEUROSAINS HUSM. Level for recommendations:
1. recommended (by experts) – better than other measures (evidence based and expert opinion) 2. optional – other measures can be as good as novoseven/lacking solid evidence.
Drug name Indication Dose Amount stored Criteria
1. Polytrauma/Trauma patient in severe DIVC or coagulopathy, requires urgent/emergency life saving surgery.
1. NOVOSEVEN -1 vial (1.2 mg) but if severely deranged coagulopathy or obese, 2 or 3 vials can be given initially.
3 vials per session of use.
Non standard and require specialist approval.
Level of recommendation (0.2-0.9 mg/kg) Recommended (1) -Paediatrics also can be
given. (0.2-0.9 mg/kg) -can be repeated after
2-5 hours.(the INR and APTT should be repeated after those 2-5 hours of therapy).
2. Coagulopathy is resistant to other
therapeutic measures and requires urgent/emergency or life saving surgery.
Same
Level of recommendation Recommended (1)
15

3. Patients known to suffer from
coagulopathy disorders (eg Haemophilia) who requires urgent/emergency life saving surgery which can or can not cause post operative DIVC.( if patient developed severe coagulopathy prior to surgery, please refer to indication 1)
Same/Novoseven made available
Level of recommendation Recommended (1) Note: alternative is the haemophilic factor (8/9)
4. Warfarin/Liver diseases induced intracranial haematoma (abnormal INR) that causing neurological deficits/neurological deterioration which is supported by radiological findings.
Same
Level of recommendation Optional (2) Note 1: FFP, Vitamin K are the alternatives. Note 2: Patient who is candidate for emergency
life saving surgery, the Novoseven is the choice made available intraoperatively because of fast effect (FFPs are the alternatives intraoperatively)
16

5. Patient who has within 4 hours of
intracranial haematoma causing neurological deficits/deterioration but is not a candidate for surgery yet.
Same
Level of recommendation Optional (2) Note 1: the BP-controlled management and correction of coagulopathy if presence with other measures are the alternatives.
Note 2: routine use of Novoseven for post surgical evacuation of intracranial clots for patient with persistent post operative abnormal clotting parameters is not recommended, the FFP and/or cryoprecipitate are the primary alternatives.
Note: Clinical management among cases may differ, depending on some other clinical scenarios/factors.
17

FLOW CHART
(POLY) TRAUMA PATIENT 1.
IN SEVERE DIVC OR COAGULOPATHY, PLANS FOR URGENT/EMERGENCY LIFE-SAVING SURGERY (NEUROSURGERY)
GIVE NOVOSEVEN DIVC CORRECTED
SURGERY
Level of recommendation: Recommended (1)
18

2. (POLY) TRAUMA OR NON TRAUMA PATIENT
IN SEVERE DIVC OR COAGULOPATHY, DIVC
IS NOT CORRECTED BY OTHER MEANS AND REQUIRED URGENT/EMERGENCY OR LIFE SAVING SURGERY.
GIVE NOVOSEVEN DIVC OR COAGULOPATHY CORRECTED SURGERY Level of recommendation: Recommended (1)
19

3. KNOWN COAGULOPATHY (Eg Haemophiliac) PATIENT
WITH/WITHOUT TRAUMA
PLAN FOR EMERGENCY LIFE SAVING SURGERY (CRANIOTOMY/CRANIECTOMY)
NOVOSEVEN MADE AVAILABLE
SURGERY NOVOSEVEN GIVEN IF COAGULOPATHY WORSENING. - novoseven should be given earlier, if severe coagulopathy occurs prior to
surgery and patient requires life saving surgery (see flow chart 1) Level of recommendation: Recommended (1)
Note: alternatives is the haemophiliac factor (8/9)
20

4. WARFARIN/LIVER DISEASES INDUCES INTRACRANIAL HAEMATOMAS (ABNORMAL INR) THAT CAUSING NEUROLOGICAL DEFICITS/DETERIORATION
IMAGING BRAIN: SIGNIFICANT HAEMATOMA/S WITH RADIOLOGICAL FEATURES OF RAISED INTRACRANIAL PRESSURE AND/OR CLINICAL EVIDENCE OF RAISED INTRACRANIAL PRESSURE.
GIVE NOVOSEVEN 5.
Level of recommendation: Optional (2) Note 1: FFP, Vitamin K are the alternatives. Note 2: Patient who is a candidate for emergency life saving surgery, the Novoseven is the choice made available intraoperatively because of fast effect (FFPs are the alternatives)
21

5. PATIENTS WITHIN 4 HOURS OF DEVELOPING INTRACRANIAL HAEMATOMA/S WITH NEUROLOGICAL DEFICITS/DETERIORATION.
IMAGING BRAIN: SIGNIFICANT HAEMATOMA/S WITH VOLUME 30 MLS OR ABOVE BELIEVES CAUSING NEUROLOGICAL
DEFICITS/DETERIORATION
NOVOSEVEN CAN BE GIVEN TO HALT THE PROGRESSION OF DEFICITS/DETERIORATION IN CONSERVATIVELY TREATED PATIENT WHO IS NOT YET A SURGICAL CANDIDATE.
-ROUTINE USE IS NOT RECOMMENDED.
Level of recommendation: Optional (2) Note 1: the BP-controlled managemant and correction of coagulopathy if presence with other measures are the alternatives. Note 2: routine use of Novoseven for post surgical evacuation of intracranial clots for patient with persistent post operative abnormal clotting parameters are not recommended, the FFP, Cryoprecipitate are the primary alternatives.
22

ABSOLUTE CONTRAINDICATION
1. Known allergy to Novoseven. 2. Allergy to mouse, hamster and bovine proteins.
RELATIVE CONTRAINDICATIONS 1. Known thrombotic tendencies. 2. Prosthetic heart valves requiring warfarin. 3. Recent angioplasty, stent insertion, MI thrombotic CVA, PE or DVT. COMPLICATIONS 1. Thromboembolic events 2. Anaphylaxis
23

24
References:
1. Malaysian Society of Anaesthesiologist : Novoseven recommendations 2006. 2. Mayer FA, Rincon F: Ultra-early hemostatic therapy for acute intracerebral haemorrhage. Semin Hematol.2006 Jan; 43 (1 Supp): S70-6. 3. Neurosurgery : Coagulopathy in Neurosurgery and recombinant Factor 7: series articles: Jun 2006 4. DeLoughery T.G : Management of bleeding emergencies : when use recombinant activated Factor VII: Expert Opinion ; a
review article.Pharmacotherapy 7(1): 2006.
5. Novoseven Product cataloge 2006. THIS PROTOCOL MEANT TO CLINICAL DOCTORS IN NEUROSCIENCES OR ALLIED NEUROSCIENCES. ACCURATE INTERPRETATION /UNDERSTANDING MAY REQUIRE EXPERT EXPLAINATIONS. Prepared by Dr Zamzuri Idris Date: 29/10/2006

GUIDELINES FOR OUTPATIENT TREATMENT OF CHRONIC ASTHMA DEPARTMENT OF MEDICINE HOSPITAL USM
CLASSIFICATION BY SEVERITY1
CLASSIFY SEVERITY Clinical Feature Before Treatment
Symptoms Nocturnal
Symptoms FEV or PEF 1
STEP 4 Continuous Limited physical activity
Frequent ≤ 60% predicted Variability > 30% Severe
Persistent STEP 3 Daily > 1 time a week 60-80% predicted
Moderate Persistent
attack affect activity Variability > 30%
STEP 2 > 1 time a week > 2 times a month ≥ 80% predicted Mild Persistent but < 1 time a day Variability 20-30%
STEP 1 < 1 time a week Asymptomatic
≤ 2 times a month ≥ 80% predicted Intermittent Variability < 20%
and normal PEF between attacks
TREATMENT
STEP 1- Salbutamol Inhaler as required STEP 2- Move to step 2 if symptoms as above or failure of step 1 T. Montelukast 10 mg daily2
Does the patient has: Yes Salbutamol inhaler as required
STEP 3- Move to step 3 if symptoms as above or failure of step 2 STEP 4 – move to step 4 if step 3 fails
Allergic rhinitis? Definite aspirin allergy?
No Exercise induced asthma? Budesonide MDI/Turbuhaler 100-800ug BD Beclomethasone MDI 50-500 ug BD/TDS Ciclesonide MDI 160 ug OD/BD Salbutamol MDI as required Start steroid at high dose, taper down later1
Treatment options: Formoterol/ Budesonide 4.5/160Turbuhaler (Symbicort®) 1 inh BD or Salmeterol/ Fluticasone 50/250 Accuhaler (Seretide®) 1 inhalation BD Salbutamol inhaler as required
Consider Symbicort® if patient is educated because
• the dose can be adjusted according to the patients need i.e. 1 inhalation BD when symptomatic and 1 inhalation daily if stable3
• Symbicort® may be used as rescue medication
25

STEP 4 – Move to step 4 if step 3 fails
Treatment options: Plus Formoterol/ Budesonide
Montelukast 10 mg daily 4.5/160Turbuhaler (Symbicort®) 1 inh BD or
KIV Salmeterol/ Fluticasone 50/250 Accuhaler (Seretide®) 1 inhalation BD Theophyline SR 250 mg BDSalbutamol inhaler as required
Still symptomatic Add Prednisolone 5-10 mg OD Please note:
• Do reversibility test if diagnosis of asthma is questionable • Do spirometry as baseline before starting any treatment • Do spirometry before any change of treatment regime • Discuss with chest physician before starting daily prednisolone
References:
1. Global Initiative For Asthma 2002. www.ginaasthma.com 2. Mastalertz L, et al. Clin Exp Allergyu 2002 Sep;32(9):1360-5 3. Aalbers R, et al. Curr Med Res Opin 2004;20:225-240
Prepared by: Dr. Che Wan Aminud-din Hashim Respiratory Physician Department of Medicine
Version 1 Nov 2006
26

GUIDELINES FOR USING INFLUENZA VACCINE Indication: Patients with the following criteria:-
1. Moderate to severe Chronic Obstructive Pulmonary Disease (Defined by GOLD guideline, HUSM guideline)
2. Asthma with recurrent exacerbation due to flu / URTI 3. Moderate to severe bronchiectasis with recurrent exacerbation 4. Any other chronic lung disease eg. Post-tuberculosis infection, insterstitial
lung disease, etc with recurrent secondary infection. Management Plan: Influenza vaccine will be administered as yearly basis. Prepared by: Dr. Che Wan Aminud-din b Hashim Repiratory Physician HUSM
27

FLOW CHART PENGGUNAAN DRUG UNTUK RAWATAN ATTENTION DEFICIT HYPERACTIVITY DISORDER (ADHD)
• METHYLPHENIDATE IR (IMMEDIATE RELEASE) • METHYLPHENIDATE SR (SLOW RELEASE) • METHYLPHENIDATE LA (LONG ACTING) • METHYLPHENIDATE (EXTENDED RELEASE) OR CONCERTA • ATOMOXETINE (STRATERA)
Pesakit dirujuk ke klinik
Diagnosa ADHD ‘Pure ADHD’ ‘ADHD with comorbidities’
Adult ADHD Disediakan oleh: Dr Mohd Jamil Yaacob, Klinik Psikiatri Kanak-kanak & Remaja.
Umur di atas 6 tahun Umur di bawah 6 tahun
IR Methylphenidate (dly-tds) Methyphenidate (dly-bd)
Methyphenidate LA (single dose) Concerta (single dose)
Behavior modification
Epilepsy
Tics
Gilles de la Tourette
Complicated Pervasive SR Development Disorders
Severe untoward events due to methyllphenidate
Atomoxetine (Stratera)
28

Lampiran A DEPARTMENTAL POLICY ON THE USE OF ANTIPSYCHOTIC DRUGS AND REQUEST FOR NON-STANDARD DRUGS
1. The typical or conventional antipsychotics are encouraged as the first line, especially for unproductive and chronic patients who had not benefited much from their improvement. However, if patients developed side-effect with the conventional drugs, changing to atypical antipsychotic is recommended.
2. The use of atypical antipsychotic drugs in Malaysia and throughout the world is increasing from year to year. In order to cut the cost, risperidone the cheapest atypical antipsychotic is recommended as the first line. However, exception to the rule is when patients clinical features are more favors for other available antipsychotics. In dealing with psychogeriatric cases that are sensitive to drug side-effect, Quatiapine may be considered as first line.
3. The used of atypical antipsychotic in poor compliance patients is discouraged: typical antipsychotics or depot preparation of typical group such Fluphenazine Decanoate and Flupentixol Decanoate should be strongly considered.
4. All the available drugs in the formulary must be tried with adequate dose (at a lower dose if patients developed side-effects) and duration before considering for non-standard drug. The request (LP) will be rejected if it does not follow the standard procedure.
5. Not all the non-standard antipsychotics could be requested through L.P, the list of non-standard drugs approved by the department will be circulated from time to time. If patients need non-standard drug which is not approved by the department, drug company should supplied to the patients or they should bought by their own.
6. An additional form which contained information such as the detail of drugs used (dose, duration and side-effect), benefit from the patient improvement and socioeconomic background of the patients family must be attached to the standard LP form when applying for non-standard drug.
7. The staffs from pharmacy department may counter-check patients folder when they are doubtful about the accurateness of the information given in the LP form. The request could not be processed if the information given was misleading.
8. The pharmacy department will give the feedback to the treating doctor whether the application for the non-standard drug is approved or not.
29

Lampiran B
FLOW CHART OF USING ATYPICAL ANTIPSYCHOTICS FOR GENERAL
PSYCHIATRIC PATIENTS
Risperidone No side-effect Developed intolerated Required dosage >4 mg daily Side-effect <4 mg daily Continued Olanzapine/ Olanzapine/ Continued the drug Aripiprazole Aripiprazole the drug Side-effect Poor response LP Quatiapine Clozapine/ drug combinations Note: try to keep maintaining dose of olanzapine and aripiprazole not exceeding 15 mg daily; otherwise review the diagnosis and medication to minimize the dose.
30

GUIDELINE ON THE USE OF ANTIPSYCHOTICS
A. SCHIZOPHRENIA AND RELATED DISORDERS (NON-EFFECTIVE PSYCHOSES)
1. UNPRODUCTIVE PATIENTS
Used typical antipsychotics as a first line
Developed moderate to severe side-effect
Developed mild side-effects
Continued the drug
Change to risperidone
* Unproductive means the patients could not contribute to the socio-economic development of the family, community or nation even after they improved; e.g, jobless patients. It is not cost-effectiveness of giving expensive drugs to these groups of patients.
31

2. PRODUCTIVE PATIENTS
Used risperidone as first line
No side-effect Developed intolerable side-effect in the dose < 3 mg daily
Required dosage >3 mg daily
Continued the drug Changed to olanzapine or other atypical antipsychotics
Change to olanzapine or increased the dose
* Examples of productive patients are students, government servants, self-employer and active house-wives.
32

B. AFFECTIVE DISORDERS Used olanzapine as first line for new cases Poor compliance or
developed side-effect Good compliance or
responding well
Change to other drug Continued the drug
OLD CASES
1. unproductive patients on atypical antipsychortics, especially involved olanzapine, try to change to typical drugs if it does not compromise with efficacy of the treatment and side-effects.
2. Any patient, who has evidence of poor drug compliance regardless of the diagnosis, should change to a cheaper drug, e.g conventional antipsychotics.
33

ALZHIMER’S DISEASE TREATMENT STRATEGY
Mild to moderate cases a) F.D.A. Approval drugs (cholinestherase inhibitors) 1) Donepezil 5-10mg/day
2) Rivastigmine 6-12mg/day 3) Galantamine 16-24mg/day b) Use Supported by Clinical Trials
1) Seligeline 5mg BD. 2) Vit. E 2000I.U./day
Moderate to severe cases a) NMDA. Antagonist- Memantine 10-20mg/day
b) Combination of cholinestherase inhibitors + N.M.D.A. Antagonist
34

PARKINSON DISEASE 1 Defer use of Levodopa if age below
60 2 Seligeline
Early stage with minimal symptoms-sign
3 Amantadine 4 Dopamine Receptor Agonists Ropinerol Pramipexol Peribedil 5 Anti-cholinergics
1 Add small titrating dose of Levodopa- dopa de carboxylase
Moderate motor symptoms interfering with activities
Inhibitor Combination (L-Dopa-Carbidopa) – Madopar (L-Dopa-Benzeraside)-Sinement
1 Add on Dopamine Receptor agonist and reduce dose of
Levodopa 2 Add on COMT Inhibitor Ento
Severe Symptoms-Motor Capone (COMTAN) Complications of L. Dopa 3 Starton STALLEVO a
combination of Levodopa- carbidopa Entocaps
4 Adjunctivies – Amantadine Anti- Cholinergics
Very advanced motor 1 Consider Surgical Treatment Complications of Levodopa Therapy Deep Brain Stimulation
35

FLOW CHART FOR TREATMENT HEPATITIS B IN TREATMENT NAÏVE PATIENTS
HBSAg positive
HBeAg status
Positive HBeAg Negative HBeAg Is ALT Elevated Is ALT Elevated
NO YES YES NO
ALT more than 2x normal
ALT less 2x normal
No treatment. ALT less 2x normal
ALT more than 2x normal Monitor ALT
every 1-3 months.
HBVDNA (PCR) Quantitative >log
HBVDNA (PCR) Quantitative >log
105 104
Liver Biopsy Ishak Score >2.0 Liver Biopsy
Ishak Score >2.0
Oral therapy 18 months (minimum) Oral therapy Minimum duration 2 years
First choice: 1. Entecavir 0.5 mg OD 2. Adefovir 10 mg OD 3. Telbivudine 600 mg OD
American/Europian/Asia Pasific Guidelines no longer use lamivudine as first line due to high viral resistance of 25% at 1 year, 45% at 2 years and 65% resistance at 3 years treatment duration.
Second choice: 1. Lamivudine 100mg Od
2. Interferon Alpha (injection)
End points of treatment 1. ALT Normalisation 2. HBeAg Seroconversion/ HBeAntibody 3. HBVDNA (PCR) supression
36

FLOW CHART OF CHRONIC VIRAL HEPATITIS B PRE CORE MUTANT HBEAG NEGATIVE
HBSAg POSITIVE MORE THAN 6 MONTHS
LIVER ENZYME ALT > 2 × NORMAL
HBVDNA (PCR) QUANTITATIVE
HBVDNA > 10,000 COPIES/ML
LIVER BIOPSY HPE BIOPSY SCORE > 2 ISHAR SCORE
THERAPY FOR MINIMUM 18 MONTHS
1. LAMIVUDINE 100 MG OD 2. TELBIVUDINE 600 MG OD
HBVDNA (PCR) QUANTITATIVE
MONITORED AT 24, 48, 72 WEEKS
THERAPY STOPPED AFTER MINIMUM 18 MONTHS IF HBVDNA (PCR) UNDETECTABLE
Prepared by: Dr. Amry A. Rahim Physician / Clinical Specialist Gastroenterology / Hepatology HUSM
37

FLOW CHART FOR GENITAL ULCER SYNDROME Patient complains of GENITAL ULCER or SORE
Take history and examine INVESTIGATIONS NEEDED:-
1. Dark ground microscopy for syphilis (IF AVAILABLE) 2. Gramstain for haemophilus ducreyi 3. Tzanck’s smear 4. VDRL, TPHA
5. HIV Ab. Multiple superficial erosions or vesicular lesions
Ulser present? PRESENT?
• Treat for SYPHILIS and CHANCROID • Health Education • Educate for behaviour change • Educate for behaviour change • Partner management YES • TCA x 2 weeks and review
results of inv. • Follow-up regime
For confirmed syphilis √ 2 weeks for results √ monthly x 3 visits √ 3 monthly x 3 visits √ 3 monthly x 2 visits • Genitial herpes management
• 3 months repeat HIV Ab. And • Educate for behaviour change VDRL/TPHA if initial results were negative • TCA x 2 weeks and review results
Treatment Protocol For Genital Ulcer Syndrome
TREATMENT FOR SYPHILIS AND CHANCROID
1ST FIRST CHOICE: IM BenzathinePenicillin 2.4 million units weekly x 2 (once a week x 2 weeks) PLUS Azythromycin 1.0 gm single oral dose
2nd SECOND CHOICE: IM Benzathine Penicilin 2.4 million units weekly x 2 (once a week x 2 weeks) PLUS Cotrimoxazole 2 tablets orally twice daily x 7 days
3rd THIRD CHOICE: IM Benzathine Penicillin 2.4 million units weekly x 2 (once a week x 2 weeks) PLUS IM Ceftriaxone 250mg single dose
Note: If patient develops allergic reaction to the 1st dose of IM Benzathine Penicillin, DO NOT give the second dose. If patient is allergic to Penicillin, use EITHER Doxycycline 100mg orally bd x 15 days OR Erythromycin ES 800 mg bd x 15 days.
38

FLOW CHART FOR VAGINAL DISCHARGE SYNDROME
Patient complains of VAGINAL DISCHARGE
Take history and do physical examination
INVESTIGATION NEEDED:- • Vaginal swab √ Wet mount for trichomonas vaginalis
√ Gram stain for candidia albicans and clue cells • Cervical swab
√ Gram stain for gonococci and pus cells √ Culture for gonococci ( using Amies charcoal transport media ) • VDRL, TPHA, and HIV ab.
YES Patient has LOWER ABDOMINAL PAIN?
NO
Refer to NEAREST Hospital
• Treat for VAGINITIS
Treatment Protocol For Vaginal Discharge Syndrome (Cervicitis And Vaginitis) 1st FIRST CHOICE: Azithromycin 1 gm single oral dose 2nd SECOND CHOICE: IM Ceftriaxone 250 mg single dose
+ Doxycycline 100 mg bd x 10 –14 days
3rd THIRD CHOICE: IM Ceftriaxone 250 mg single dose +
Erythromycin ES 800 mg bd x 10 – 14 days PLUS Metronidazole 2 gm STAT PLUS Nystatin pessaries 100,000 units daily x 14 days On follow-up: If no improvement or not effective to continue Metronidazole 400 mg bd x 7 days OR TREATMENT FOR VAGINITIS ONLY
RISK FACTORS NO • Educate for behaviour change 1. Less than 21 years old RISK ASSESSMENT
2. Single • Partner has symptoms OR • Follow up for 2 weeks for results
3. Recent partner ( less than 3 monts) • Risk factor positive
4. Multiple partners YES
• Treat for CERVICITIS and Vaginitis • Educate for behaviour change • Partner management • Follow- up ---2 weeks for result
3 months to repeat VDRL, TPHA & HIV Ab, IF INITIAL TEST WERE NEGATIVE
Treatment for Vaginal Discharge Syndrome ( Cervicitis)
Treatment for Vaginal Discharge Syndrome ( Cervicitis)
39

40
Discharge PRESENT?
Traetment for CHLAMYDIA
FLOW CHART FOR URETHRAL DISCHARGE SYNDROME IN MEN Treatment Protocol for Urethral Discharge Syndrome 1st CHOICE: Azithromycin 1gm orally single dose 2nd CHOICE: IM Ceftriaxone 250mg single dose + Erythromycin ES800mg orally bd x 10-14 days 3rd CHOICE: IM Ceftriaxone 250mg single dose + Erythromycin ES 800mg orally bd x 10-14 days IM Spectinomycin 2gm STAT + Doxycycline 100mg orally bd x 10-14 days OR IM Spectinomycin 2gm STAT + Erythromycin ES 800 mg orally bd x 10-14 days
Patient complains of Urethal Discharge/Dysuria or irritation
Take history and examine (milk URETHRA if necessary)
INVESTIGATIONS NEEDED:- - Urethral smear
√ Gram stain for gonococci & pus cells √ Culture for gonococci (use AMIE’S charcoal transport media)
- 2 glass urine test - VDRL,TPHA & HIV Ab
1. Do 2 glass test 2. result POSITIVE? ULCER PRESENT?
• Treat for GONORRHEA and CHLAMYDIA
• Educate for behaviour change • Partner management • Follow-up
If Patient is allergic to penicillin and azithromycin is not available
Treatment for Gonorhea and Chlamvdia
√ Two weeks for result √ Three months to repeat VDRL, TPHA & HIV Ab.
REFER TO Appropriate flow chart
Health Education Follow-up for 2 weeks
Yes
No
Yes
No
No
Yes

TREATMENT PLAN
OUTPATIENT TREATMENT OF CAP
YES
YES
DIAGNOSIS
NO
PRIMARY CARE OF EMERGENCY DEPT VISIT
Patient presents w/ symptoms suggestive of community-acquired pneumonia (CAP)
Does history, physical Exam & chest x-ray
confirm CAP ?
SITE OF CARE DECISION Does patient have any of the
core adverse prognistic factors?
ALTERNATIVE DIAGNOSIS
Treat patient appropriately
NO
Yes, 2 core adverse prognostic factors are present
No core adverse prognostic factors are present
EVALUATION Does patient have
preexisting adverse prognostic factors?
CLINICAL DECISION Should patient be admitted to
hospital? Base decision on clinical judgement, additional adverse
prognostic factors, the patient’s social circumstances & patient
preferences
OUTPATIENT TREATMENT Non-pharmacological
• Patient education Avoid smoking Adequate hydration &
nutrition Pharmacotherapy
• Symptomatic therapy Analgesics for pleuritic
pain • Antibiotics therapy
NO
Yes, 1 core adverse prognostic factors are present
HOSPITAL ADMISSION
YES
41

42
TREATMENT PLAN (CONT’D)
EMPIRIC OUTPATIENT CAP ANTIBIOTIC THERAPY
EMPIRIC ORAL ANTIBIOTICS Local epidemiologic patterns need to be considered to target the antimicrobial therapy against the likely pathogens Previously healthy individual Any one of the following :
• High-dose Amoxycillin • Doxycycline • Macrolide – Erythromycin
Preferred agent in many guidelines Comorbidity is present (DM, renal insufficiency, CHF, alcohol abuse, COPD) Any one of the following :
• Advanced macrolide - Azithromycin • Beta-lactam or beta lactam-beta-lactamase inhibitor • Quinolone
Patient has multiple medical condirions , has COPD & received antibiotics or oral steriods in the last 3 months or any other risk factors for Gram –ve organisms • Macrolide (Azithromycin) + beta lactam or beta-lactam (beta – lactamase inhibitor) • Quinolone (alone)
Suspected aspiration pneumonia Any one of the following :
• Beta-lactam, beta-lactamase inhibitor w/ or w/o macrolide (Azithromycin) • (Clindamycin or metronidazole w/ quinolone)
FOLLOW UP • Follow up will depend on initial severity assessment • Recommended follow up in 48-72 hr • If patient fails to improve consider the following :
Chest X-ray Hospital admission
• Possible reasons for failure to improve Host factors associated w/ a delayed response Inadequate antimicrobial selection (eg. Resistant organism or bacteria not covered by initial antibiotic therapy) Metastatic infections (eg. Meningitis, endocarditis, empysema etc) Noninfections illness

FLOW CHART OF USING SULPERAZONE IN ICU
ICU Patient
Ventilated/NonVentilated Nosocomial Infection
Non Acinetobacter Acinetobacter
Non-Drug Multi Resistance
Multi-Drug Resistance (MDR) Quinolones or
3rd Generation or
4th Generation or
Carbapename Sulperazone Unasyn
±Aminoglycoside ±Aminoglycoside
Responding Non-Responding Within 24-48 Hr or Suspicious of MDR
Continue Treatment
43

GUIDELINES FOR USING NOVOMIX 30 FLEXPEN HOSPITAL UNIVERSITI SAINS MALAYSIA
PRE-MIXED INSULIN
NovoMix 30 Mixtard 30 Penfill FlexPen
OAD’s failures
Patients on Mixtard (switch to)
OAD’s failure 1. elderly 2. hypoglycaemic prone 1. frequent hypoglycaemia 3. fasting (ramadhan) or puasa sunat)
2. poor control 3. post prandial hyperglyacemic 4 fasting (ramadhan) or puasa
44

FLOWCHART FOR USE OF GLUCOPHAGE XR
Type 2 Diabetes Mellitus
Metformin (immediate release) BID/TID
Poor compliance or Gastro-intestinal side-effects
Metformin (extended release) (Glucophage XR) once daily
45

FLOWCHART FOR USE OF INSULIN DETEMIR
Insulin requiring diabetes mellitus
NPH insulin
Hypoglycemia
Insulin Detemir/Glargine
46

ALGORITHM FOR THE MANAGEMENT OF POSTMENOPAUSAL OSTEOPOROSIS
Clinical Assessment
Patients with risk General measures: Patients with prior factor but no - Calcium intake (B) incidental low
fracture - Physical activity (B) trauma fracture In the elderly: - Vitamin D + calcium (A) - Prevention of falls (B) BMD measurement
T score: T score: T score:
≥ -1 <-1 to > -2.5 ≤ -2.5
NORMAL OSTEOPENIA* OSTEOPOROSIS OSTEOPOROSIS (BMD if available)
Monitor If multiple risk factor present (C) Treatment options: Treatment options:
-Strontium ranelate -Strontium ranelate -SERMs/ - Bishosphonate (A) -Bishosphonates (A) -SERMs (A) -Activated vitamin D (A) -Activated vitamin D (A) -Calcitonin (A)
-rPTH**(A) Reassess with BMD after 2 years (A) NO YES
Follow up with BMD if available If BMD
deteriorates Reassess Treatment options: BMD yearly (C) - Strontium ranelate - SERMs (A) - Alendronate (A) - HRT (A)
47

ZOLENDRONIC ACID PRESCRIPTION FLOW CHART
Bone Metastasis –Confirmed By Bone Scan Primary By:
1) Breast Carcinoma 2) Nasopharyngeal Carcinoma 3) Lung Carcinoma (NSCLC) 4) Prostate Carcinoma
Symptoms of Pain
Severe Hypercalcaemia Mild To Moderate Pain Severe pain. Scale > 7/10
1st
1st Line IV Zolendronic Acid 4 mg over 15 minutes every 4 weeks for 6 months.
Palliative Intension. To stop and reduce bone metastases/damage especially when bone involvement is wide spread
+/- Hypercalcaemia
2nd Line IV Zolendronic Acid 4 mg over 15 minutes every 4 weeks for 6 months
Further pain +/- Hypercalcaemia
Line IV Pamidronate 90 mg Over 2 hours every 4/52 For 6 months
48
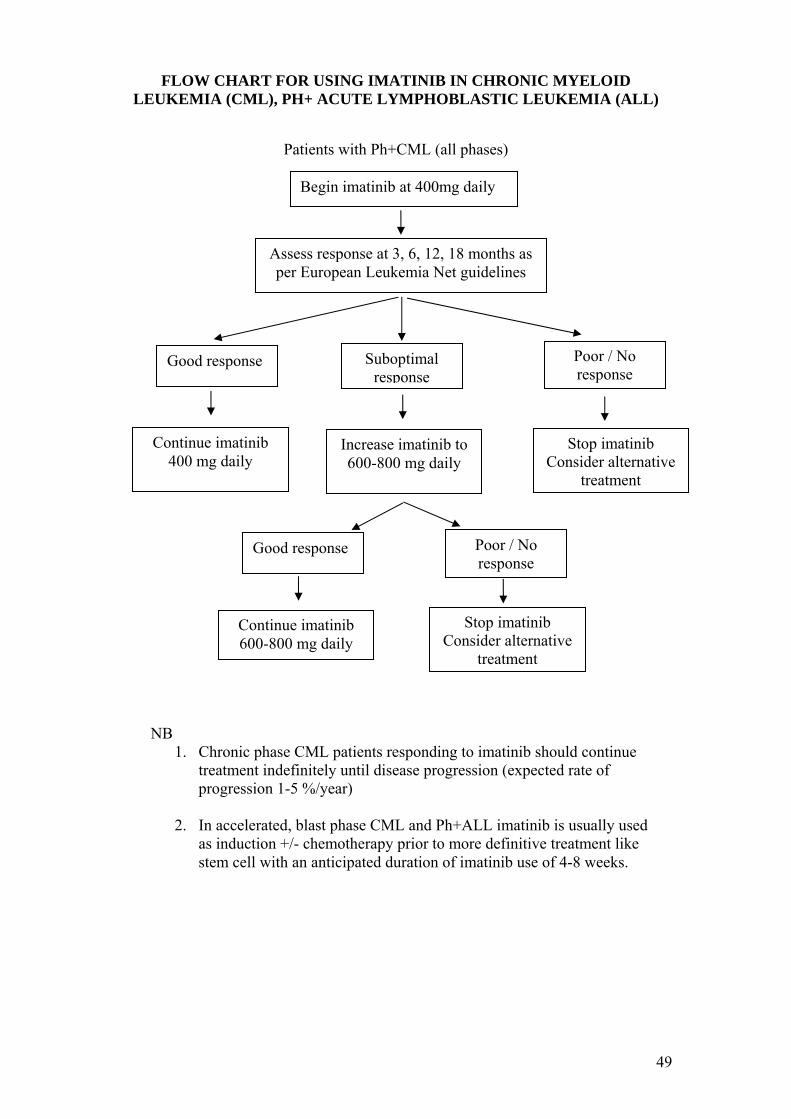
FLOW CHART FOR USING IMATINIB IN CHRONIC MYELOID LEUKEMIA (CML), PH+ ACUTE LYMPHOBLASTIC LEUKEMIA (ALL)
Patients with Ph+CML (all phases)
Begin imatinib at 400mg daily
Assess response at 3, 6, 12, 18 months as per European Leukemia Net guidelines
Poor / No response
Suboptimal response
Good response
Continue imatinib 400 mg daily
Stop imatinib Increase imatinib to 600-800 mg daily Consider alternative
treatment
Poor / No response
Good response
Stop imatinib Continue imatinib 600-800 mg daily Consider alternative
treatment
NB 1. Chronic phase CML patients responding to imatinib should continue
treatment indefinitely until disease progression (expected rate of progression 1-5 %/year)
2. In accelerated, blast phase CML and Ph+ALL imatinib is usually used
as induction +/- chemotherapy prior to more definitive treatment like stem cell with an anticipated duration of imatinib use of 4-8 weeks.
49

Lampiran1 Dr. Shamsul Kamaruljan
ARCOXIA PRESCRIPTION FLOW CHART
*Prescription: Maximum only for 3/52 Dose: 60mg, 90mg and 120mg (Depends on severity of the pain and condition of the pain)
1st line: T. Celebrex 200-400mg dly T. Meloxicam 7.5mg bd T. Tramadol 50-100mg tds Oral opiods e.g. T. DF118, Oral morphine
1st line: NSAIDS e.g Voltaren, Mefenamic acid, Ibuprofen
History of Gastritis
Acute/chronic pain
YesNo
Pain not relieved
Pain not relieved
2nd line: 2nd
T. Celebrex 200-400mg dly T. Meloxicam 7.5mg bd Oral opiods e.g. T.DF118, Oral morphine
line: T. Arcoxia 60-120mg dly T. Oxycontin 10-40mg bd
Pain not relieved
3rd line: T. Arcoxia 60-120mg dly T. Oxycontin 10-40mg bd
50

Lampiran 2 Setelah diubahsuai oleh Jabatan Ortopedik
OUTPATIENT PAIN PRESCRIPTION FLOW CHART
Acute/chronic pain History of Gastritis *COX2 Prescription for acute pain: Maximun only for 3/52 Arcoxia Dose: 60mg (OA), 90mg (RA) and 120mg (Acute pain e.g. gouty arthritis) (Depends on severity of the pain and condition of the pain) 3rd line is same in both pathways
1st line: AC: T. Celebrex 200-400mg dly AC Gouty arthritis : T Arcoxia 120mg daily CHR: T. Meloxicam 7.5mg dly T Celebrex 200mg dly
1st line: AC: Voltaren, Mefenamic acid, Ibuprofen CHR: Feldene, Neprosyn
YesNo
Pain not relieved
Pain not relieved
2nd line: 2nd
AC: Oral opiods e.g. T.DF118, T. Arcoxia 120mg dly CHR: T. Celebrex 200 dly T. Meloxicam 7.5mg dly
line: Oral opiods e.g. T.DF118, T. Arcoxia 60-120mg dly
Pain not relieved
3rd
3rd line: Oral morphine T. Oxycontin 10-40mg bd
line: Oral morphine T. Oxycontin 10-40mg bd
AC – acute CHR - chronic
51

FLOWCHART OF PATIENTS DIAGNOSED WITH BACTERIAL CONJUNCTIVITIS
Bacterial Conjunctivitis
1st line:
Gutt. Chloramphenicol
Perform Culture and Sensitivity test Not resolved
2nd line:
Gutt. Ciprofloxacin (Ciloxan)
Not resolved
3rd line:
Gutt. Moxifloxacin (Vigamox)
52

FLOWCHART OF PATIENTS DIAGNOSED WITH BACTERIAL KERATITIS
Bacterial Keratitis
1st line:
Gutt. Ciprofloxacin (Ciloxan)
Perform Cornea Scrapping/ Culture Not resolved and Sensitivity test
2nd line: Gutt. Moxifloxacin
(Vigamox)
53

FLOWCHART OF PATIENTS REQUIRING PRE AND POST CATARACT SURGERY ANTIBIOTIC PROPHYLAXIS
Cataract Surgery
Prophylaxis
Pre–op prophylaxis: • Gutt. Moxifloxacin 0.5 % (Vigamox) 1 drop every 15 minutes 1
hour prior to surgery. • 5 % Povidone – iodine ( 1 drop ) on the ocular surface.
Intra-cameral injection:
• 1mg in 0.1 mL cefuroxime* or • 0.1 mL Gutt. Moxifloxacin 0.5% (Vigamox)1 - at the end of surgery *Dilution is required as standard ceruroxime injection is 100 mg/mL.
Post–op prophylaxis:
• Gutt. Moxifloxacin 0.5% (Vigamox) 3-4 times daily for 1 month.
Reference: 1) CRG Espiritu et. al. Safety of Prophylactic Intracameral Moxifloxacin 0.5%
Opthalmic Solution in Cataract Surgery Patients. J Cataract Refract Surg 2007: 33: 63-68
54

FLOW CHART FOR USING OLOPATADINE 0.1% AND SODIUM
CROMOGLYCATE
i. Kegunan ubat tersebut adalah untuk rawatan kes “Allergic conjunctivitis” terutama “Vernal Allergic conjunctivitis” di kalangan kanak-kanak dan remaja.
ii. Kerana mempunyai kesan kedua-dua iaitu “mast cell stabilizer” dan “anti histamines”
iii. Ubat titis sodium cromoglycate yang dahulu digunakan untuk kes di atas, akan dikurangkan kegunaannya.
“Flow chart” penggunaan kedua-dua drug bagi membezakan kes-kes tersebut seperti berikut; Pesakit
Pesakit “Allergic conjunctivitis” terutama “Vernal Allergic
conjunctivitis”
Selainnya
Ubat titis Sodium Cromoglycate 2%
Ubat titis Olopatadine
55
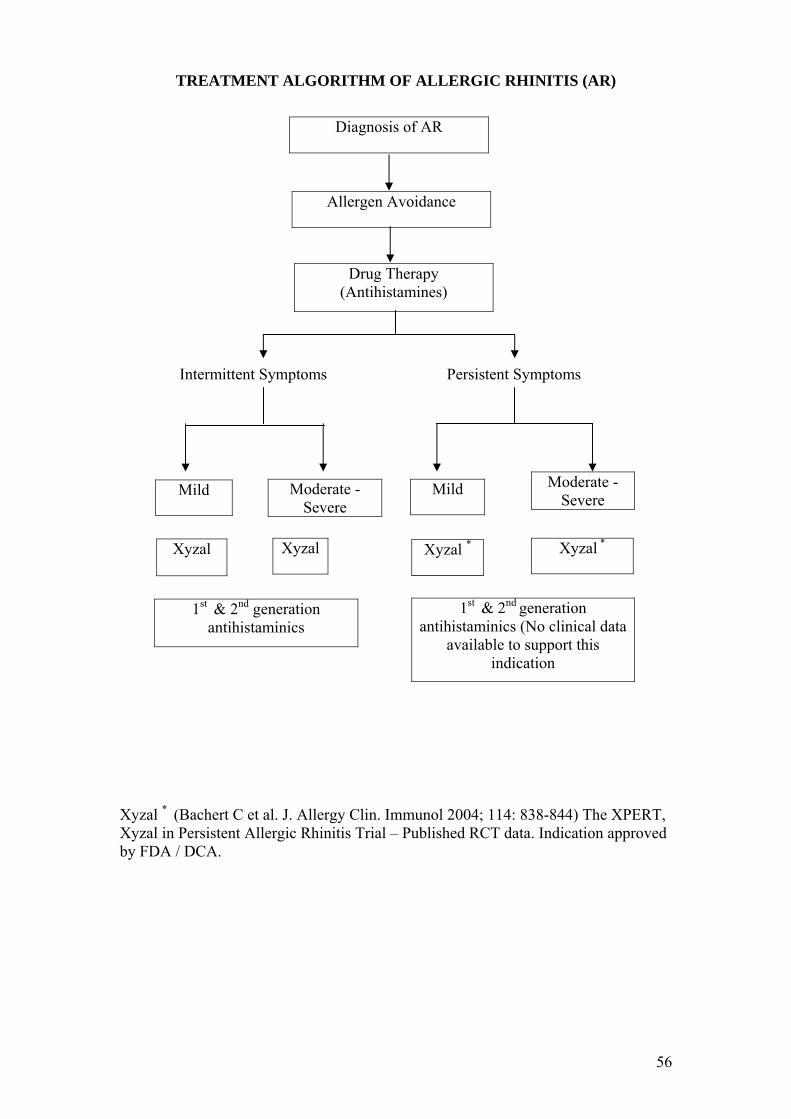
TREATMENT ALGORITHM OF ALLERGIC RHINITIS (AR)
Diagnosis of AR
Allergen Avoidance Drug Therapy (Antihistamines) Intermittent Symptoms Persistent Symptoms
Moderate - Severe
Moderate - Severe
Mild Mild
*
Xyzal * (Bachert C et al. J. Allergy Clin. Immunol 2004; 114: 838-844) The XPERT, Xyzal in Persistent Allergic Rhinitis Trial – Published RCT data. Indication approved by FDA / DCA.
Xyzal Xyzal *Xyzal Xyzal
1st & 2nd generation antihistaminics
1st & 2nd generation antihistaminics (No clinical data
available to support this indication
56

FLOW CHART OF THALASSAEMIA PATIENT WITH IRON OVERLOAD
DIAGNOSIS OF THALASSAEMIA ON REGULAR BLOOD TRANSFUSION
REGULAR 3-4 MONTHLY FOLLOW-UP IN PAEDIATRIC HAEMATOLOGY
CLINIC
REGULAR 3-4 WEEKLY FOLLOW-UP IN THALASSAEMIA DAY CARE UNIT
FOR BLOOD TRANSFUSION
3 MONTHLY MONITORING SERUM FERRITIN LEVEL
EVIDENCE OF IRON OVERLOAD, SERUM FERRITIN > 1000 MCG/L
INTRODUCE TO SUBCUTANEOUS DESFERAL (deferoxamine) WITH
TRAINING AND MONITORING
ASSESSMENT OF COMPLIANCE TO DESFERAL (Growth, Se Ferritin, yearly
echo of heart)
POOR COMPLIANCE GOOD COMPLIANCE TO DESFERAL TO DESFERAL Se Ferritin Se Ferritin < 2500mcg/L > 2500mcg/L CONTINUE DESFERAL
DEFERASIROX DEFERIPRONE
57

INTERFERON BETA-1B FLOWCHART
Multiple Sclerosis
1) Remitting and Relapsing type.
2) Clinically Isolated syndrome with MRI evidence of multiple
plaques.
DIAGNOSIS ESTABLISHED AS PER Mc DONALD CRITERIA
TREAT THE ACUTE EPISODE WITH I.V METHYL PREDNISOLONE
THEN CONSIDER THE THERAPEUTIC OPTION OF STARTING BETA-
INTERFERON THERAPY.
(Beta interferon is the only evidence based treatment for the above condition, to reduce the risk of relapses and slow down the disease progression).
58